
Abstract
Objective
To systematically evaluate clinical evidence concerning the efficacy and safety of superficial radiotherapy in the treatment of cutaneous warts.
Methods
Eight major international clinical literature databases were queried according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for superficial radiotherapy studies published prior to 9 August 2025. Randomized controlled trials, prospective/retrospective controlled studies, and case series with sample sizes ≥10 were included. The primary outcome was the cure rate, whereas secondary outcomes included recurrence rate and adverse reactions. Risk or odds ratio with 95% confidence interval were pooled using random-effects or fixed-effects models as appropriate. Heterogeneity was assessed using the I2 statistic. Subgroup analysis was performed based on monotherapy versus combination therapy. Publication bias was evaluated using funnel plots and Egger’s test, and the Grading of Recommendations Assessment, Development and Evaluation system was applied to assess the quality of evidence.
Results
The overall cure rate for cutaneous warts using superficial radiotherapy was 81% (95% confidence interval: 0.76–0.85, p < 0.05), whereas the recurrence rate was 14% (95% confidence interval: 0.10–0.18, p < 0.05). For superficial radiotherapy monotherapy, the cure rate was 76% (95% confidence interval: 0.69–0.83, p < 0.05), and recurrence rate was 21% (95% confidence interval: 0.04–0.38, p < 0.05). Compared with superficial radiotherapy monotherapy, combination therapy was associated with a higher cure rate (odds ratio = 4.08, 95% C confidence interval: 2.43–6.83, p < 0.05) and lower recurrence rate (odds ratio = 0.23, 95% confidence interval: 0.08–0.65, p < 0.05).
Conclusions
Superficial radiotherapy monotherapy is an effective treatment for cutaneous warts, associated with low recurrence rates and infrequent adverse reactions. Combination therapy is associated with a higher cure rate and a lower recurrence rate than superficial radiotherapy monotherapy. Further studies comparing combination and superficial radiotherapy monotherapy are necessary for a more rigorous evaluation of the long-term recurrence rates associated with these therapies. The study was retrospectively registered with the International Platform of Registered Systematic Review and Meta-analysis Protocols (Registration Number: INPLASY202650102).
Introduction
Cutaneous warts are common benign disorders of epidermal cell hyperproliferation caused by human papillomavirus (HPV) infection. Affected patients present with diverse clinical manifestations, including common, plantar, flat warts, and condylomata acuminata, among other lesions. 1 Although benign, these lesions are often visible, may cause friction-related discomfort, and can even impair limb function or appearance. Therefore, they can impose a substantial psychological burden and reduce the quality of life which motivates patients to actively seek treatment. 2 Current clinical management encompasses a variety of approaches. Physical therapies include cryotherapy using liquid nitrogen and ablative therapy using carbon dioxide or pulsed dye lasers. Pharmacotherapies include keratolytic topical agents (e.g. salicylic acid and trichloroacetic acid), antimicrobial modulators (e.g. fluorouracil), or immune modulators (e.g. imiquimod). Additional options include photodynamic therapy and systemic immunomodulatory treatment. 3 Although effective, these conventional treatments have several limitations. Cryotherapy and laser therapy produce rapid results; however, they are associated with significant procedural pain and may lead to post-treatment pigmentation changes, scarring, functional impairment, and high recurrence rates. Topical medications usually require long-term application and are associated with variable efficacy and poor patient adherence. Furthermore, although immune-based therapies may theoretically reduce recurrence, they are slow-acting and can cause local or systemic adverse reactions. 4
Superficial radiotherapy (SRT) has regained attention as a noninvasive treatment modality in recent years. This technique employs low-energy X-rays (50–100 kV) to deliver precise irradiation to the target skin area. Due to its limited tissue penetration, the energy is concentrated primarily in the epidermis and upper dermis, minimizing damage to the deep tissue. 5 SRT is associated with minimal discomfort during treatment, does not require anesthesia, and generally results in no open wounds, bleeding, or significant scarring. Therefore, it is well-suited for the treatment of warts that are resistant to conventional treatments, recurrent, or located in anatomically sensitive regions (e.g. periungual areas, face, and feet soles). Mechanisms of action include destruction of HPV-infected keratinocytes, inhibition of viral DNA replication, and modulation of the local immune microenvironment. Although clinical reports on SRT have demonstrated favorable short-term efficacy and tolerability, there is a paucity of large randomized controlled trials (RCTs) and studies with long-term follow-up assessing the therapeutic performance of SRT. Consequently, there is a lack of consensus regarding the overall effectiveness and safety of SRT. To address these gaps, we performed this systematic meta-analysis of the clinical literature on SRT, providing insights into the effectiveness of SRT monotherapy compared with combination therapies.
Material and methods
Search strategy
Major clinical literature databases, including PubMed, Embase, Web of Science, Cochrane Library, China National Knowledge Infrastructure (CNKI), WanFang, Chinese Science and Technology Journal Database (VIP), and SinoMed were queried to identify RCTs and prospective/retrospective studies related to SRT for the treatment of cutaneous warts. A combination of subject headings and free-text terms was employed in the search. Key search terms included “pi fu you,” “zhi liao,” “qian ceng X xian fang she,” “cutaneous wart,” “treatment,” and “superficial radiation therapy,” among other relevant Chinese and English keywords.
Inclusion and exclusion criteria
Our analysis included RCTs, prospective/retrospective controlled studies, and case series on SRT therapy. Study populations included patients of any age or sex diagnosed with cutaneous warts (including common, plantar, periungual, and flat warts as well as condylomata acuminata). Outcome measures included overall cure rate, recurrence rate, and adverse reactions. Our analysis excluded published conference proceedings, reviews, systematic reviews, duplicate publications, poorly designed studies, and studies with crude data unsuitable for secondary consolidation, conversion, or analysis. Additionally, studies involving patients with comorbid systemic diseases or skin lesions complicated by dermatological conditions such as eczema or tinea were excluded.
Literature quality assessment
Studies were categorized based on their design into cohort studies, case series, and RCTs. The Newcastle–Ottawa Scale (NOS) was used for cohort studies, and the Joanna Briggs Institute (JBI) Critical Appraisal Tool for Case Series was applied for case series and RCTs. Each included study was assigned a quality score. The study quality was independently assessed by two researchers, and discrepancies were resolved through discussion or consultation with a third researcher.
Data extraction
Two researchers independently reviewed the articles and extracted relevant data into a standardized table. Details regarding each study’s first author, year of publication, patient characteristics, sample size, treatment protocols, and quality assessment scores were recorded. Discrepancies and conflicting records were resolved through discussion or consultation with a third researcher.
Statistical analyses
Data were analyzed using the Stata software, and main findings were represented using forest plots. For dichotomous outcomes (efficacy and recurrence rates), odds ratios (ORs) with 95% confidence intervals (CIs) were used as effect measures. A p-value <0.05 was considered statistically significant. Heterogeneity was assessed using the Cochrane Q test. If the p-value was >0.1 and I2 was <50%, a fixed-effects model was applied; if the p-value was <0.1 and I2 was ≥50%, a random-effects model was used. Sources of heterogeneity were explored through subgroup analysis. Funnel plots were generated to assess potential publication bias. This study was registered retrospectively with the International Platform of Registered Systematic Review and Meta-analysis Protocols (INPLASY) (Registration Number: INPLASY202650102).
Results
Literature search
In total, 171 publications were initially identified, and 133 articles were excluded after cursory review due to the following reasons: (a) irrelevance (n = 119); (b) review articles (n = 2); (c) experiential summary (n = 1); and (d) case analyses (n = 11). After more comprehensive assessment, four additional articles were excluded. Ultimately, seven studies were included in our analysis,6–12 comprising five Chinese8–12 and two English studies.6,7 The literature screening algorithm has been detailed in Figure 1, and the characteristics of the included studies are presented in Table 1.6–12
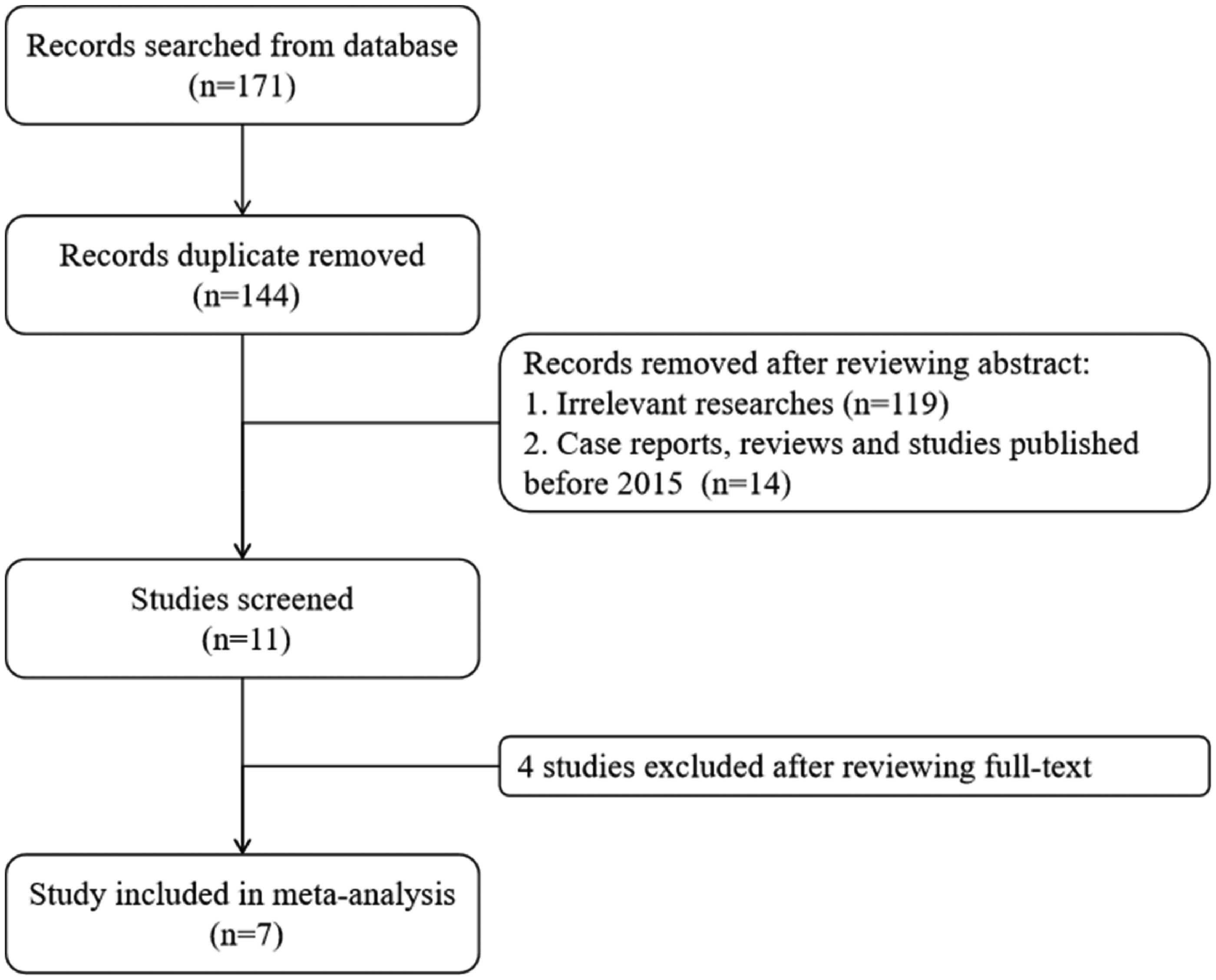
Flowchart of the literature screening process.
Characteristics of the studies included in our meta-analysis.

SRT: superficial radiotherapy; CO2: carbon dioxide.
Quality assessment of included studies
Among the seven included studies, three were RCTs, three were case series, and one was a retrospective cohort study. Overall, the methodological quality of the studies was moderate. Radiation doses for SRT or laser-based interventions, when reported in the original studies, have been presented in Table 1. Specific quality assessment scores are shown in Table 1.
Meta-analysis
Overall cure rate
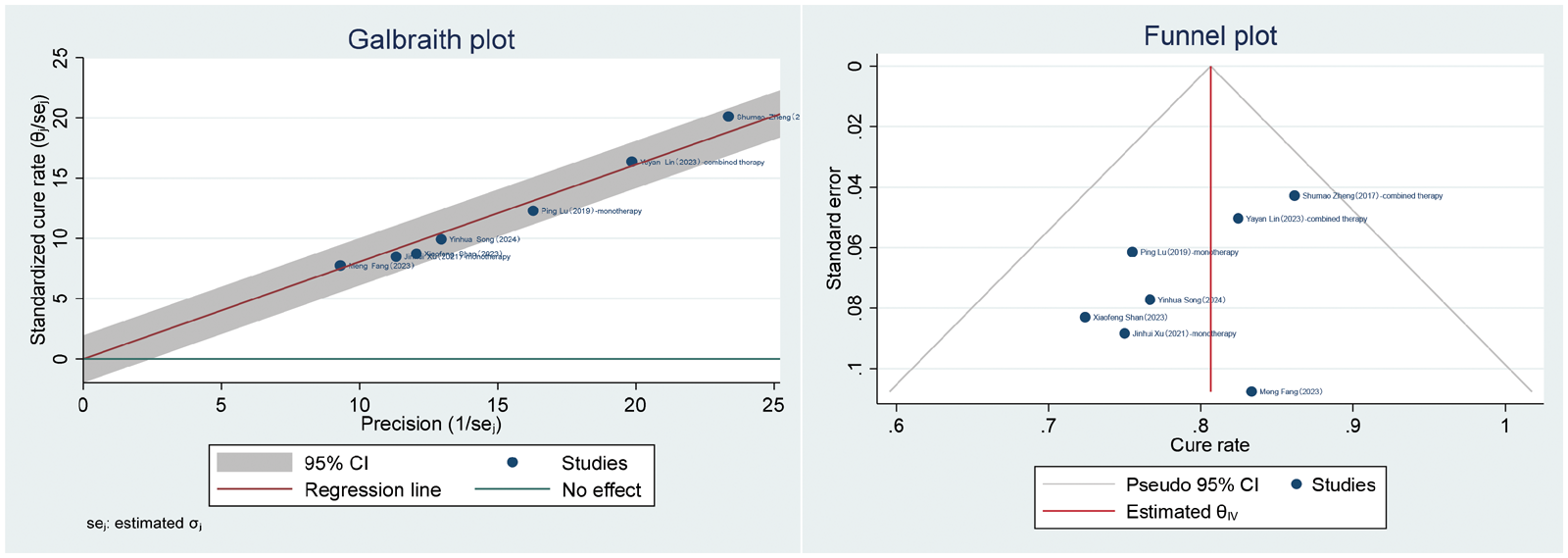
All seven studies6–12 reported cure rates. The random-effects model indicated significant statistical heterogeneity in the cure rates (overall mean =0.78, 95% CI: 0.71–0.86, I2 = 80.54%, p < 0.05) (Figure 2). Galbraith plot and funnel plot analyses identified the study by Lu et al. 12 as a major source of heterogeneity (Figure 3). After excluding this study, the remaining studies were analyzed using a fixed-effects model which showed no significant heterogeneity (I2 = 0.00%, p = 0.65). The pooled effect size was 0.81 (95% CI: 0.76–0.85, p < 0.05), indicating an overall cure rate of 81% (95% CI: 0.76–0.85) (Figures 4 and 5).
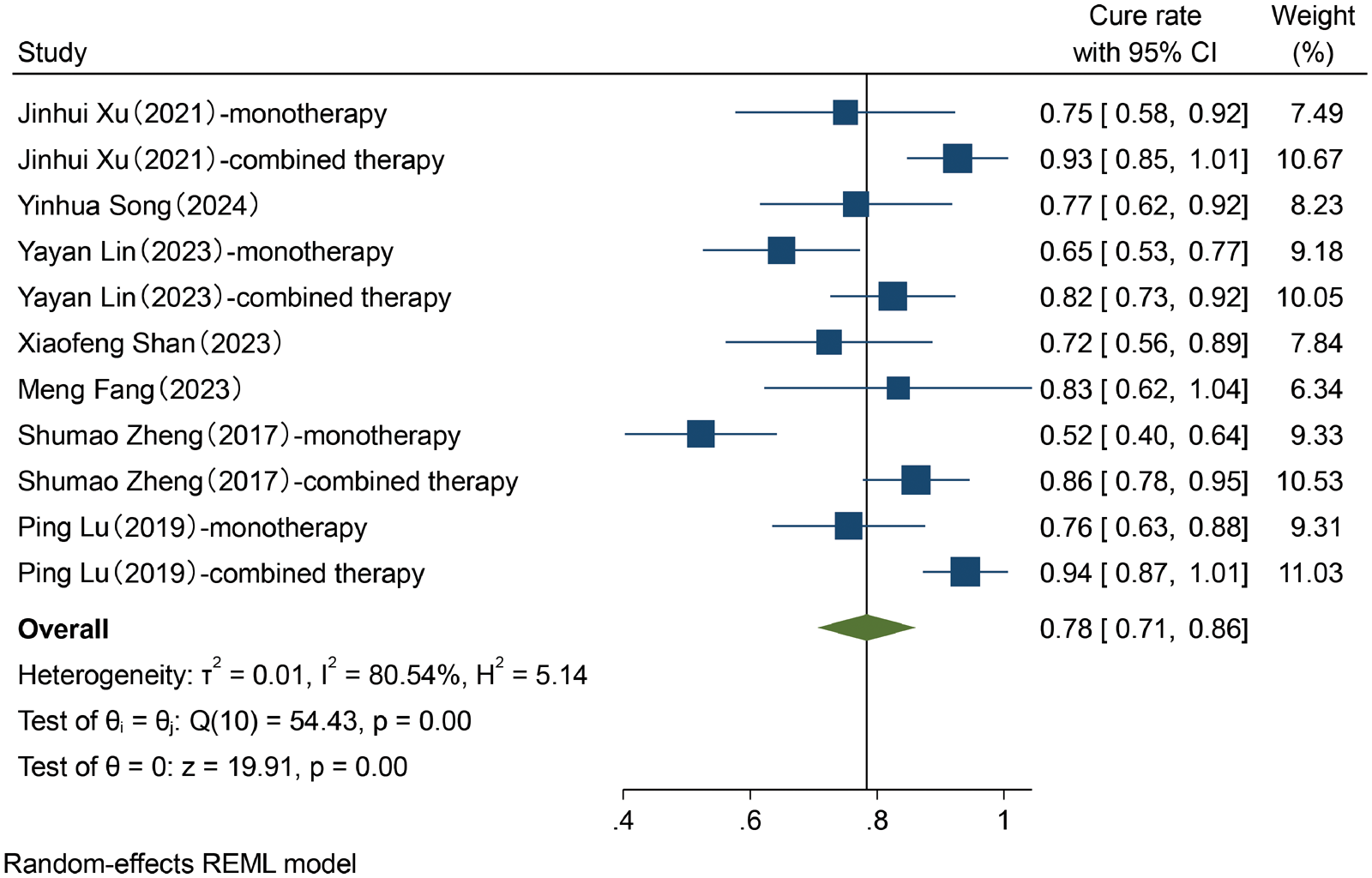
Forest plot of random-effects meta-analysis of the overall cure rate.
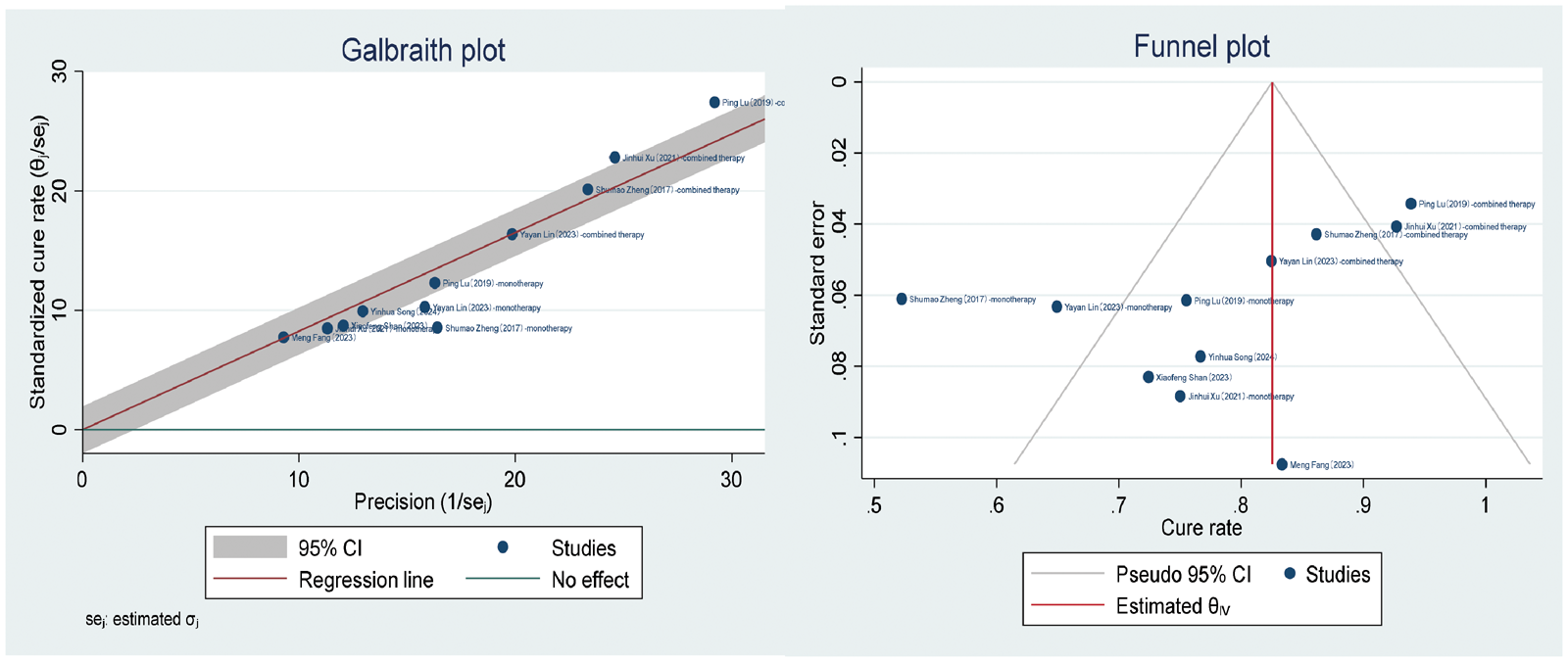
Galbraith and funnel plots of the overall cure rate.
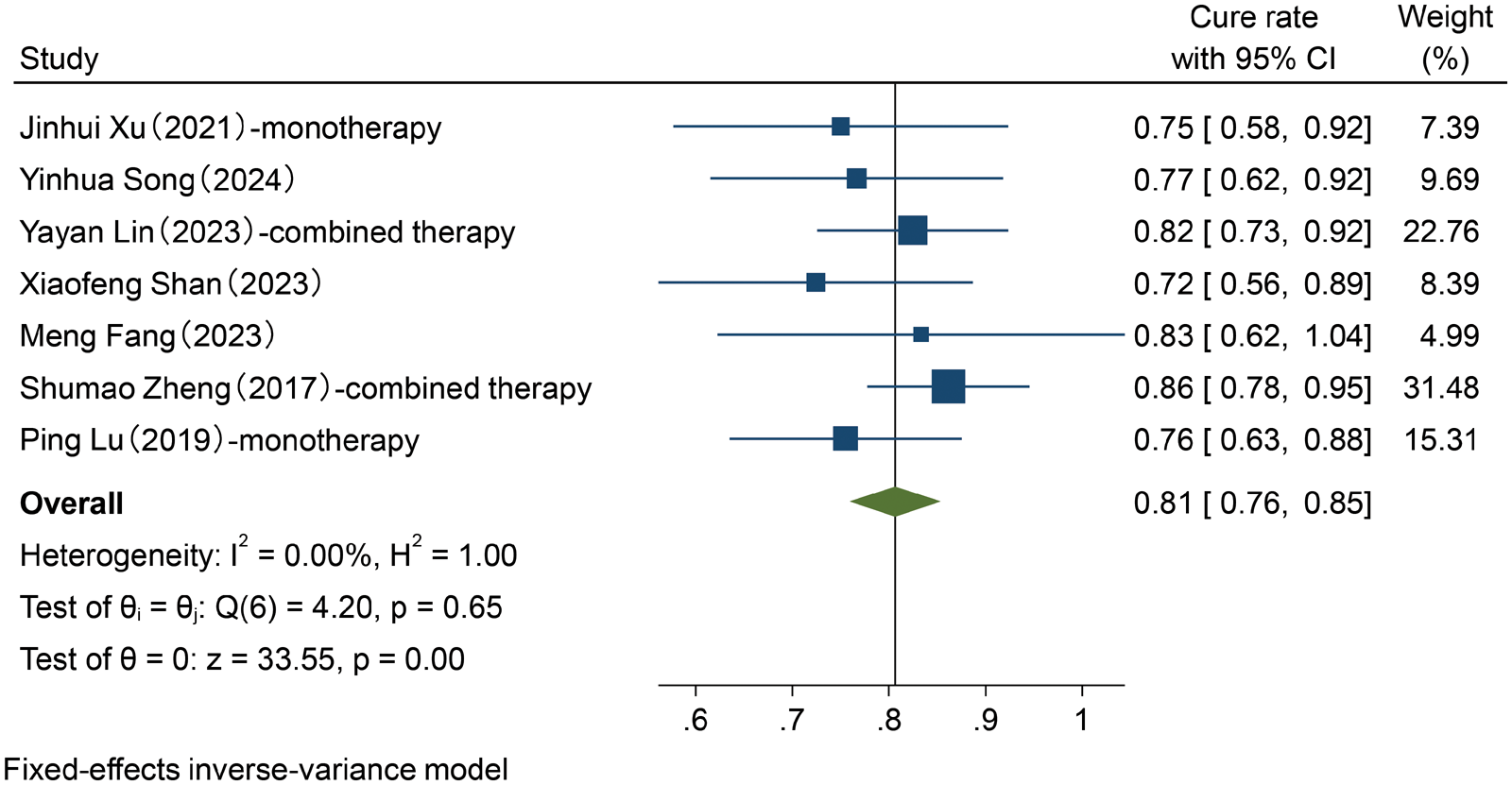
Forest plot of fixed-effect meta-analysis of the overall cure rate.
Galbraith and funnel plots of the overall cure rate after removing the source of heterogeneity.
Overall recurrence rate
Six studies6–8,10–12 reported recurrence rates. Significant heterogeneity was observed in the recurrence rate using the random-effects model (recurrence rate = 0.23, 95% CI: 0.13–0.33, I2 = 86.78%, p < 0.05) (Figure 6). Galbraith and funnel plots (Figure 7) again identified the study by Lu et al. 12 as an outlier. After its exclusion, the fixed-effects model was applied to the remaining six studies and showed no significant heterogeneity (I2 = 0.00%, p = 0.83). The pooled effect size was 0.14 (95% CI: 0.10–0.18, p < 0.05), indicating an overall recurrence rate of 14% (95% CI: 0.10–0.18) (Figures 8 and 9).
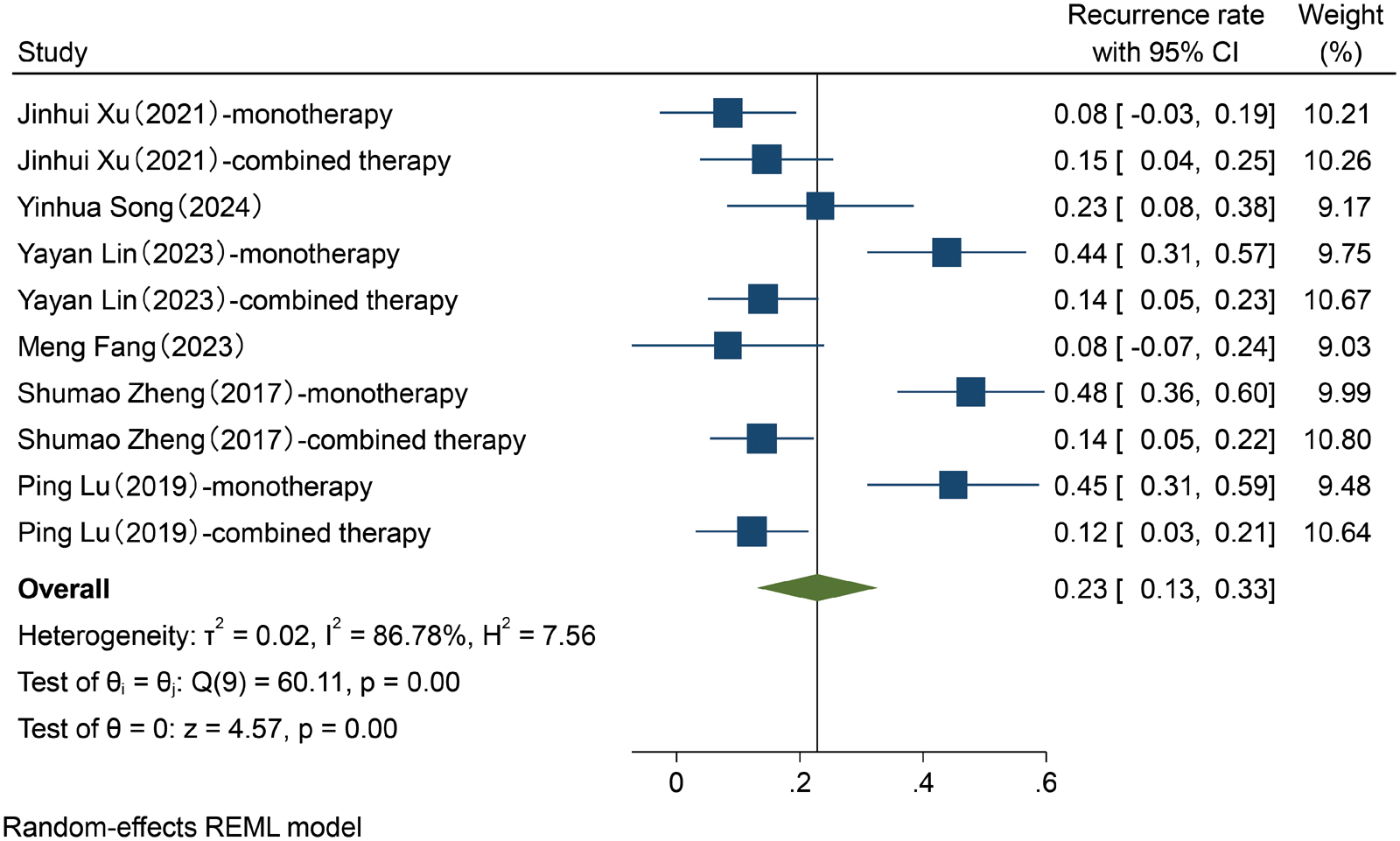
Forest plot of the random-effects meta-analysis of the overall recurrence rate.
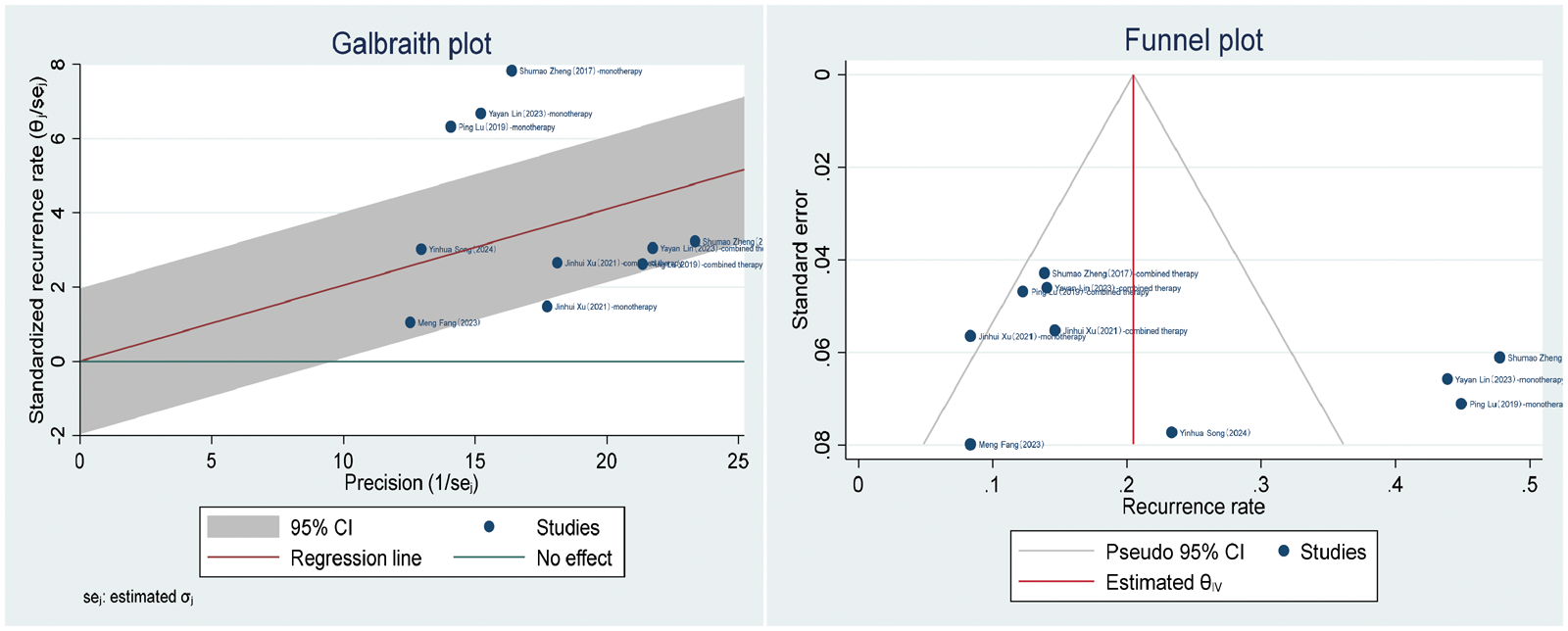
Galbraith and funnel plots of the overall recurrence rate.
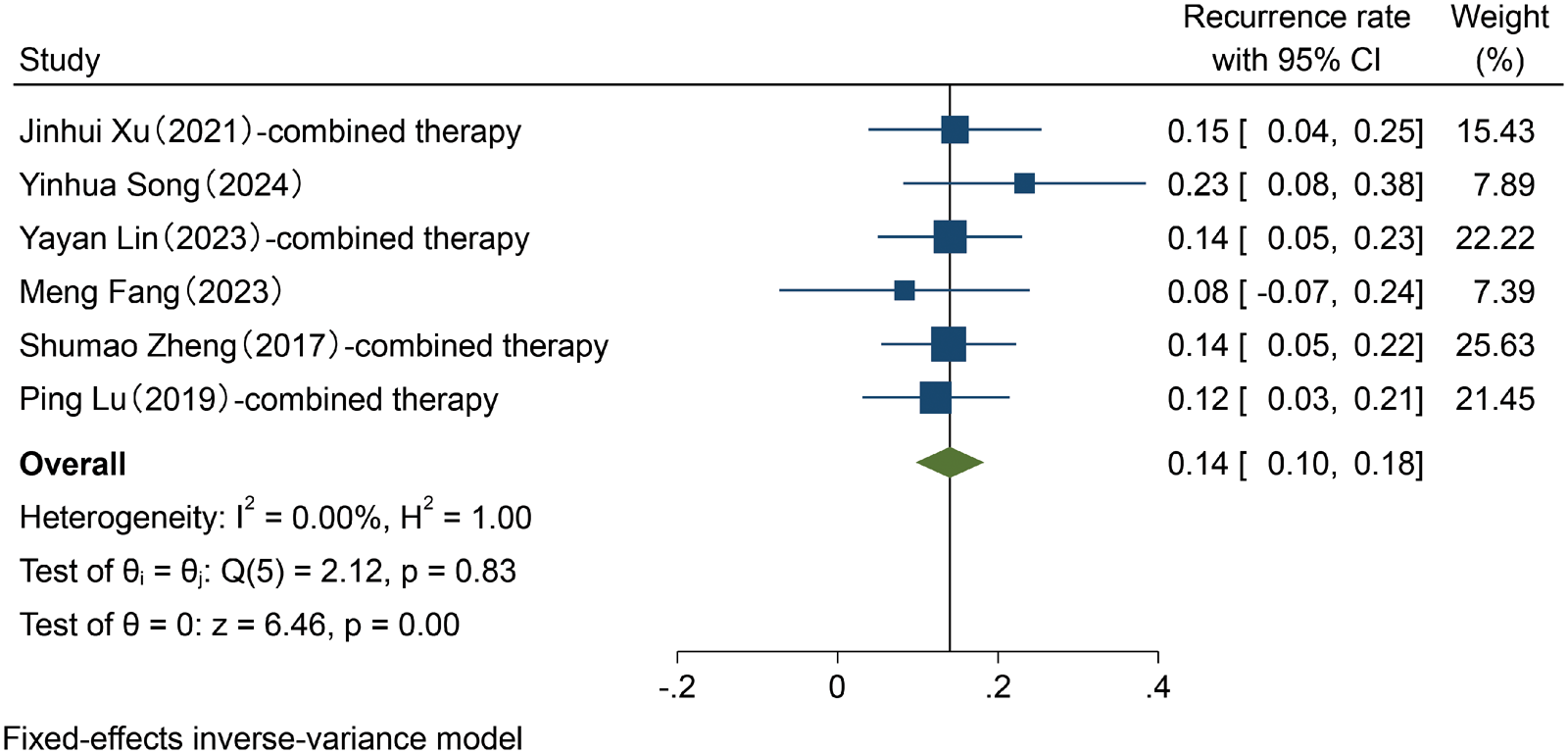
Forest plot of the fixed-effect meta-analysis of the overall recurrence rate.

Galbraith and funnel plots of the overall recurrence rate after removing the source of heterogeneity.
Cure rate of SRT monotherapy
Five studies6,7,9,10,12 reported the cure rates for SRT monotherapy. The fixed-effects model showed no significant heterogeneity (I2 = 0.00%, p = 0.95). The pooled effect size was 0.76 (95% CI: 0.69–0.83, p < 0.05), indicating a cure rate of 76% (95% CI: 0.69–0.83) for SRT monotherapy (Figure 10). The corresponding funnel plot is shown in Figure 11.

Forest plot of the fixed-effect meta-analysis of the cure rate for SRT monotherapy. SRT: superficial radiotherapy.

Funnel plot of the cure rate for SRT monotherapy. SRT: superficial radiotherapy.
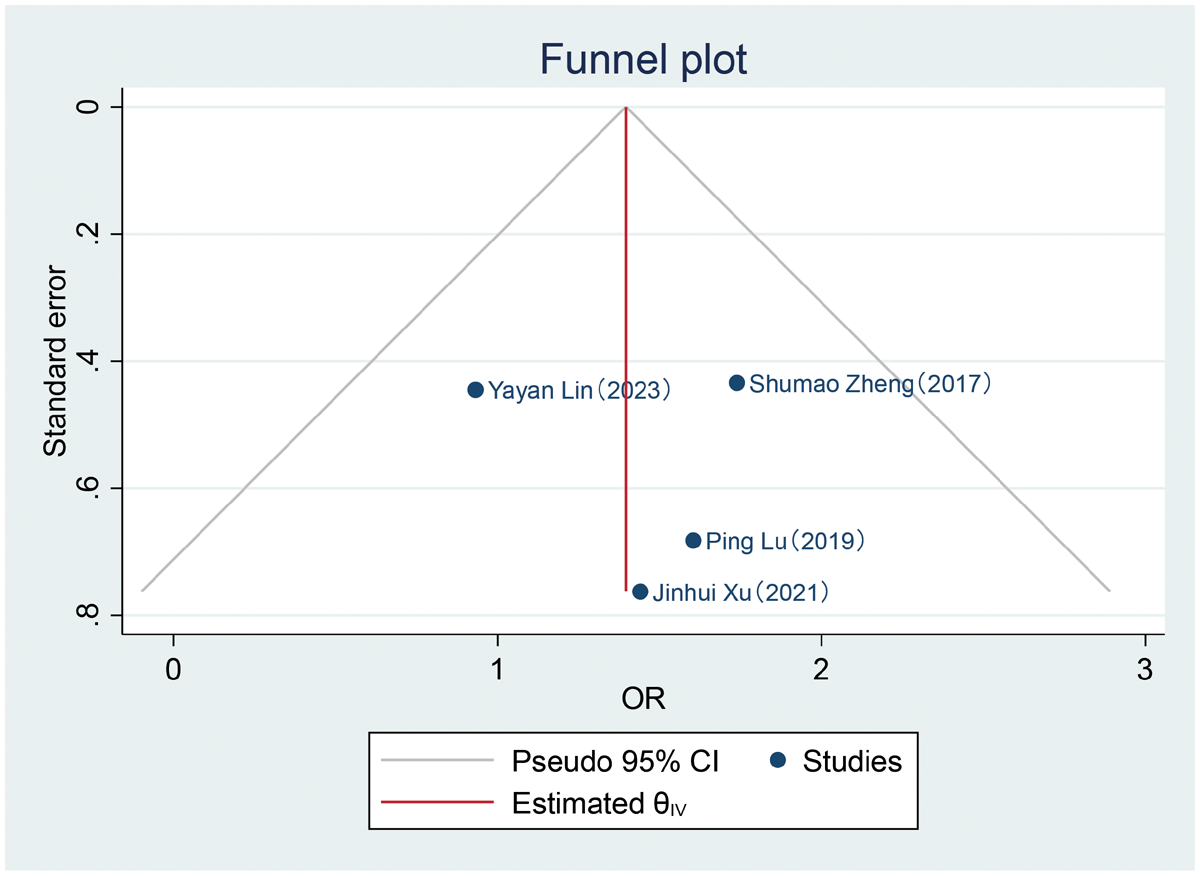
Recurrence rate after SRT monotherapy
Four studies6,7,10,12 reported recurrence rates after SRT monotherapy. The random-effects model indicated significant heterogeneity (I2 = 83.65%, p < 0.05). The pooled effect size was 0.21 (95% CI: 0.04–0.38, p < 0.05), indicating a recurrence rate of 21% (95% CI: 0.04–0.38) after SRT monotherapy (Figure 12). The corresponding funnel plot is shown in Figure 13.
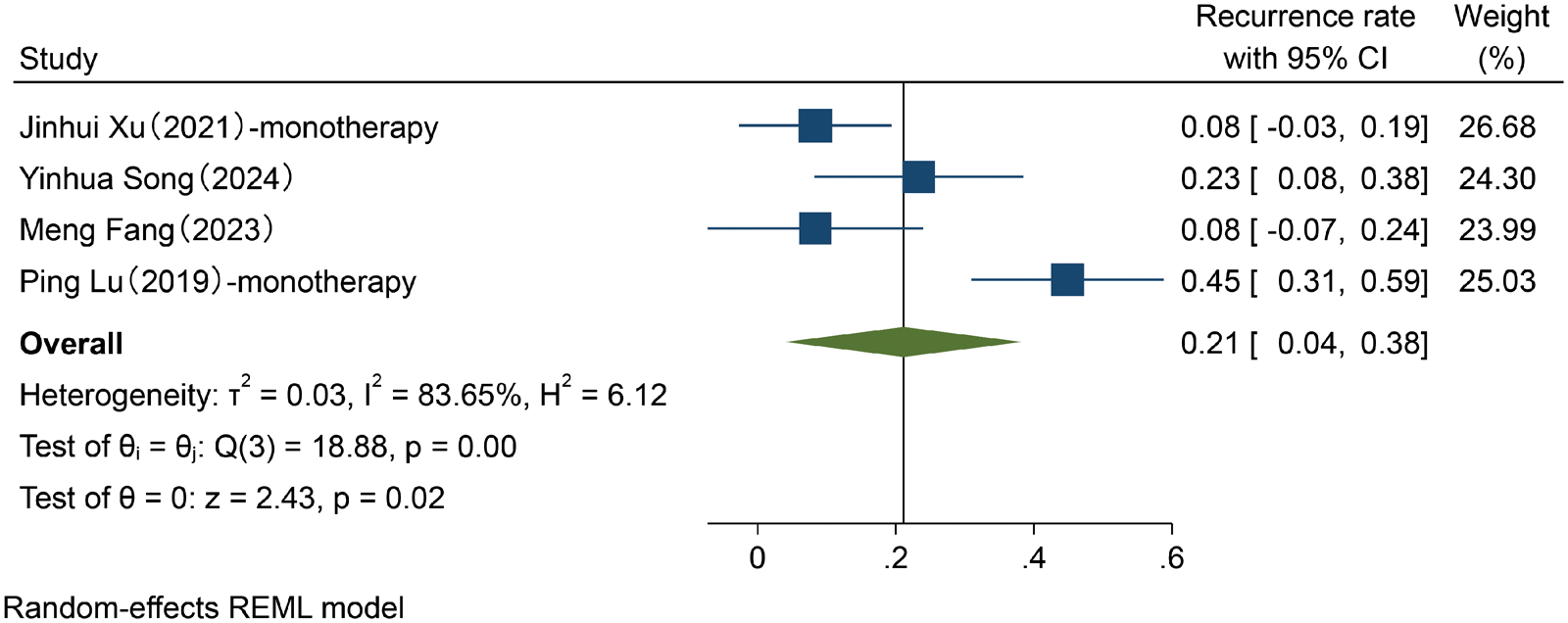
Forest plot of the random-effects meta-analysis of the recurrence rate with SRT monotherapy.

Funnel plot of the recurrence rate for SRT monotherapy. SRT: superficial radiotherapy.
Comparison of the cure rates of SRT monotherapy versus combination therapy
Four studies6,8,11,12 compared the cure rates between SRT monotherapy and combination therapy that included SRT. The fixed-effects model showed no significant heterogeneity (I2 = 0.00%, p = 0.61). The pooled odds ratio was 4.08 (95% CI: 2.43–6.83, p < 0.05), indicating that the cure rate in the combination therapy group was 4.08-fold higher than that in the monotherapy group (Figure 14). The corresponding funnel plot is shown in Figure 15.

Forest plot of the meta-analysis comparing the cure rates between SRT monotherapy and combination therapy. SRT: superficial radiotherapy.
Funnel plot comparing the cure rates between SRT monotherapy and combination therapy.
Comparison of the recurrence rates of SRT monotherapy versus combination therapy
Four studies6,8,11,12 compared the recurrence rates between SRT monotherapy and combination therapy. The random-effects model indicated significant heterogeneity (I2 = 73.64%, p = 0.03). The pooled odds ratio was 0.23 (95% CI: 0.08–0.65, p < 0.05), indicating that the recurrence rate in the combination therapy group was 0.23-fold lower than that in the monotherapy group (Figure 16). The corresponding funnel plot is shown in Figure 17.

Forest plot of the meta-analysis comparing the recurrence rates between SRT monotherapy and combination therapy. SRT: superficial radiotherapy.

Funnel plot comparing the recurrence rates between SRT monotherapy and combination therapy. SRT: superficial radiotherapy.
Cure and recurrence rates across wart type subgroups
A random-effects model was applied to analyze the cure and recurrence rates among the different subgroups of wart types across the seven studies. The pooled cure rates for verruca vulgaris, condyloma acuminatum, palmoplantar warts, and periungual warts were 0.74, 0.77, 0.79, and 0.86, respectively (Figure 18).

Forest plot of the meta-analysis of cure rates with SRT across different wart types. SRT: superficial radiotherapy.
The pooled recurrence rates of verruca vulgaris, condyloma acuminatum, palmoplantar warts, and periungual warts were 0.29, 0.29, 0.16, and 0.12, respectively (Figure 19).

Forest plot of the meta-analysis of recurrence rates after SRT across different wart types.
Discussion
SRT has re-emerged in recent years as a safe and viable therapeutic strategy for various dermatological conditions owing to its use of low-energy radiation, favorable safety profile, and controllable treatment delivery. It has been shown to be effective in the treatment of keloids, nonmelanoma skin cancers, viral warts, and infantile hemangiomas. 13
This meta-analysis demonstrated that SRT is highly effective in treating cutaneous warts, with an overall cure rate of 81% (95% CI: 0.76–0.85). Both SRT monotherapy and combination therapies that include SRT are associated with low recurrence rates, suggesting that SRT can serve as an effective treatment option for refractory warts, recurrent warts, or warts located in specific anatomical sites. The underlying mechanisms via which SRT exerts therapeutic effects in patients with cutaneous warts are multifactorial and involve the following:7,14
Direct cytotoxicity in abnormally keratinized and HPV-infected basal layer cells induced by low-energy X-rays, leading to wart regression and shedding; Radiation-mediated viral DNA damage, which reduces the proliferative capacity and potential for persistent HPV infection; Stimulation of mild inflammatory responses in the affected tissues, which enhances the host’s immune recognition and clearance of the HPV.
With respect to safety, multiple studies have reported that adverse reactions associated with SRT are mostly mild and self-limiting (e.g. transient erythema, pigmentation changes, and slight desquamation), with severe complications being extremely rare.8–10,15 Furthermore, the low long-term recurrence rates observed in nonmelanoma skin cancer patients treated using SRT indirectly support its favorable safety profile.16,17 A longitudinal study spanning 24 years that reported on the treatment of 531 wart cases reported no significant adverse effects, 18 further confirming the reliability of SRT when performed under standardized protocols. Nevertheless, potential long-term risks associated with repeated or large-area irradiation, such as skin aging, pigmentary changes, and potential carcinogenicity, warrant vigilance and systematic evaluation through long-term follow-up studies. Despite its favorable safety record, SRT remains an ionizing modality, and potential long‑term risks should be considered. The low penetration depth of 50–100 kV X‑rays restricts most of the absorbed dose to the epidermis and superficial dermis,16,18 thereby reducing systemic exposure. Nevertheless, repeated treatments or use over large anatomical areas may lead to chronic skin atrophy, telangiectasia, pigmentary changes, or (in theory) radiation‑induced neoplasia. 19 Importantly, none of the seven included studies documented any malignant transformation, and prior longitudinal studies reporting the treatment of >500 wart cases have also not recorded any case of radiation‑related cancer over more than two decades. However, most available studies provide only short-term follow‑up data and lack systematic late‑toxicity assessment data. Thus, prolonged follow‑up periods and standardized safety monitoring are essential in future clinical studies to quantify the risk of malignant induction more precisely.
It is noteworthy that the indication and response rates of SRT for cutaneous warts vary by subtype. For instance, flat warts, commonly appearing on the faces of adolescents, can be numerous; however, they are often self-resolving. Gentle approaches such as topical retinoid application or photodynamic therapy are usually recommended as evidence supporting the use of SRT for this type of warts remains limited. In contrast, SRT is clearly indicated for plantar warts, characterized by thick hyperkeratosis and significant pressure because these warts respond poorly to conventional cryotherapy. Both SRT and carbon dioxide (CO2) laser therapy have demonstrated efficacy in the treatment of refractory plantar warts.7,19 Periungual warts are challenging to treat, and traditional methods involve risk of damage to the nail matrix. SRT offers a noninvasive alternative, with a reported efficacy rate of approximately 75%, and can often be combined with other therapies to enhance outcomes. 10 Additionally, studies suggest that the patient’s immune status significantly influences treatment efficacy. Immunocompromised individuals are prone to the development of multiple warts and have a higher recurrence risk. Thus, combining local or systemic immunomodulatory treatments (e.g. interferon injections and adjuvant vaccines) may improve viral clearance and reduce recurrence in this patient population. 20
Based on the present study and existing literature, the following patient groups may be particularly suitable for SRT:
Those with refractory or recurrent warts that have not responded to conventional therapies such as cryotherapy, laser, and topical medications; Those with warts located in challenging anatomic locations or hyperkeratotic areas such as the palms, soles, and periungual regions; Patients with multiple lesions or functional-area involvement in whom SRT allows simultaneous treatment of multiple sites, thereby reducing discomfort and treatment burden.
This study also found that combination strategies outperformed monotherapy in improving cure rates and reducing recurrence, suggesting that SRT acts synergistically with other treatments and should be further promoted in personalized therapeutics.
The present study has certain limitations. First, most of the included studies were retrospective studies or case series, not RCTs, introducing potential selection and information biases. The total sample size was relatively limited, particularly in the context of subgroup analyses involving combination therapies. Significant heterogeneity existed across studies in terms of patient baseline characteristics, wart types, radiation doses, and treatment courses, which may have reduced the reliability of the pooled results. Finally, in most studies, the follow-up duration was <6 months, a time-frame insufficient for evaluating long-term safety and recurrence rates.
Future research on SRT therapy for cutaneous warts should employ multicenter RCTs with large sample sizes and long-term follow-up to systematically compare the efficacy and safety of SRT with those of conventional treatments. Such studies could also evaluate the impact of treatment optimization by exploring different doses, fractionation regimens, and device types on outcomes. Additional research on the effectiveness of combining SRT with pharmacological, physical, or immunotherapeutic approaches is warranted to clarify synergistic mechanisms and identify suitable populations. Future studies should emphasize the inclusion of special populations (e.g. children, pregnant women, and immunocompromised patients) as existing data on these populations are insufficient to evaluate the efficacy and safety of SRT. Finally, long-term follow-up observational mechanisms should be established to comprehensively assess recurrence rates, cosmetic outcomes, functional recovery, and rare late complications (e.g. radiation-induced malignancies).
Thus, SRT represents an effective and safe treatment for cutaneous warts, particularly those that are refractory or located in unique and/or challenging areas. Combining SRT with other therapeutic strategies may further improve prognosis and lower recurrence rates. Although current evidence supports SRT as an alternative or adjuvant treatment, more clinical studies are clearly needed to strengthen the evidence base and inform clinical guidelines. Retrospective study registration may have introduced bias in our results and represents a study limitation.
Footnotes
Acknowledgments
None.
Author contributions
Yu-Yu Deng contributed to the conception and design of the study, literature search, data extraction, data analysis, manuscript drafting, and revision.
Chang-xia Li contributed to literature screening, data extraction, and manuscript revision.
Guo-lan Li contributed to statistical analysis and interpretation of the results.
Xiao-hua Tao contributed to manuscript review, editing, and supervision.
All authors have read and approved the final version of the manuscript and agree to be accountable for all aspects of the work.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declare no potential conflict of interest.
Funding statement
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.