
Abstract
Background
Kimura disease presents considerable diagnostic and therapeutic challenges because of its rarity, polymorphic early manifestations, recalcitrant clinical course, high recurrence rate, and potential for multiorgan involvement.
Case presentation
A Chinese woman in her late 40s presented with a 3-year history of foreign body sensation in the pharynx and a 6-month history of dysarthria. Laryngoscopy revealed a smooth mass on the epiglottis. Laboratory investigations demonstrated elevated peripheral blood eosinophil counts and serum immunoglobulin E levels. The mass, together with the epiglottic cartilage, was surgically resected. Histopathological examination of paraffin-embedded specimens confirmed the diagnosis of Kimura disease. Postoperatively, low-dose corticosteroid therapy was administered. No recurrence was observed during follow-up.
Conclusion
This case provides novel insights into Kimura disease and underscores the importance of including this condition in the differential diagnosis of epiglottic masses. Systemic glucocorticoids represent a valuable therapeutic option. Importantly, close long-term follow-up is essential for optimal patient management.
Introduction
Kimura disease (KD), also known as eosinophilic hyperplastic lymphogranuloma, is a rare chronic inflammatory disorder of unknown etiology. It predominantly affects young to middle-aged Asian males and typically presents as painless masses in the head and neck region (e.g. the parotid, submandibular, postauricular, and periorbital areas), with a reported global incidence of approximately 200 histopathologically confirmed cases and a male-to-female ratio of 3:1. 1 Regional lymphadenopathy is common. Laboratory findings frequently include elevated serum immunoglobulin E (IgE) levels and peripheral blood eosinophilia. Histopathologically, KD is characterized by dense lymphoid infiltrates with prominent follicular hyperplasia; interfollicular sheets of eosinophils, lymphocytes, and mast cells; postcapillary venule proliferation; and varying degrees of fibrosis. It is often misdiagnosed as a malignancy (e.g. lymphoma), hemangioma, or other inflammatory conditions. We recently encountered a case of KD manifesting as an epiglottic mass in a patient presenting with pharyngeal discomfort. A review of the literature indicated that epiglottic involvement is exceedingly rare, with only 13 previously reported cases,2,3 including one case with concurrent lip and epiglottic involvement. 4 Such atypical localization of KD can pose significant diagnostic challenges both clinically and histologically and, if untreated, may lead to serious complications. Herein, we report this case, detailing its clinical presentation, diagnostic workup (with emphasis on pathological features), therapeutic strategy, and follow-up outcomes, with the aim of enhancing awareness of this rare entity and highlighting the importance of an accurate differential diagnosis.
Case report
A Chinese woman in her late 40s presented to the Bethune International Peace Hospital (Shijiazhuang, Hebei, China) in December 2024 with a 3-year history of progressive pharyngeal foreign body sensation and a 6-month history of dysarthria. She reported occasional acid reflux and heartburn. Her medical history included allergies to “fungi, animal hair, and egg yolk,” with no history of renal disease.
Otolaryngological examination revealed a smooth, bulging mass posterior to the tongue base, with its pedicle not visible. Flexible fiberoptic laryngoscopy demonstrated a smooth submucosal mass obscuring the epiglottis (Figure 1).

Flexible fiberoptic laryngoscopy showing a smooth, bulging masses in the oropharynx, obscuring the epiglottis. The lesion did not involve the laryngeal surface of the epiglottis or the vocal cords.
Laboratory tests demonstrated significantly elevated serum IgE levels (1810 IU/mL; normal <100 IU/mL) and peripheral blood eosinophilia (absolute count, 2.24 × 109/L; percentage, 26.8%; normal ranges: 0.02–0.52 × 109/L and 0.4%–8%, respectively). Routine urinalysis, fecal examinations, and liver/kidney function tests were normal.
Contrast-enhanced computed tomography (CT) revealed two well-defined, homogeneously enhancing oval soft-tissue density lesions involving the epiglottis, as well as multiple enlarged lymph nodes in the neck and thoracic inlet (Figure 2). Magnetic resonance imaging (MRI) showed that the lesions were isointense on T1-weighted images and slightly hyperintense on T2-weighted images, with homogeneous enhancement. Coronal T2 fat-saturated sequences confirmed the epiglottic lesions and associated lymphadenopathy (Figure 3). Ultrasonography identified a thyroid nodule (Thyroid Imaging Reporting and Data System, Category 3 (TI-RADS 3)) and several enlarged left cervical lymph nodes.

Axial contrast-enhanced CT scan demonstrating two well-defined oval soft-tissue lesions involving the epiglottis (arrows) and multiple enlarged lymph nodes in the neck.
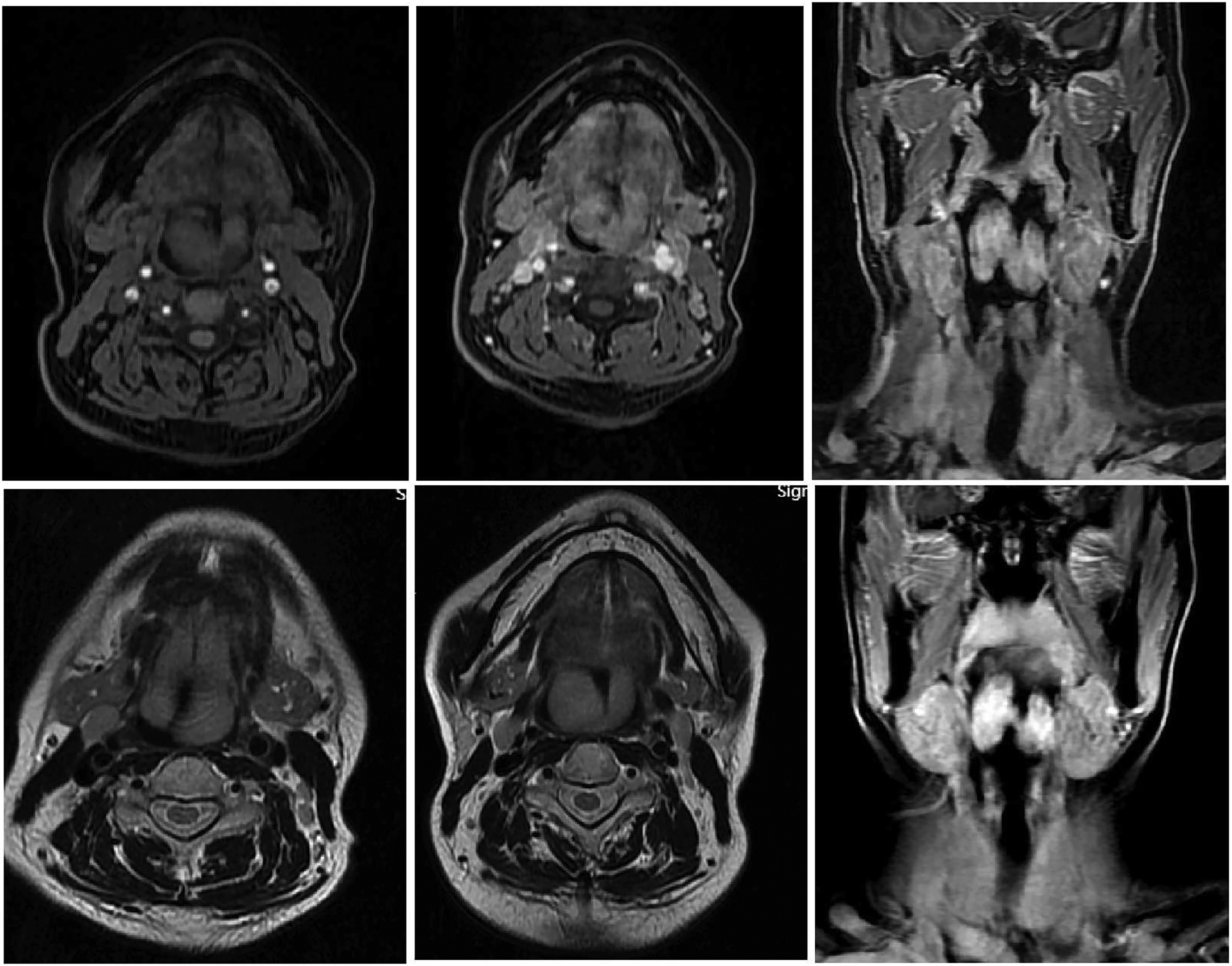
Magnetic resonance imaging (MRI) demonstrating two well-circumscribed ovoid masses arising from the epiglottis. The lesions exhibited isointense signal intensity on T1-weighted images and slightly hyperintense signal intensity on T2-weighted images, with homogeneous internal signal characteristics. Postcontrast images revealed marked progressive enhancement of the epiglottic lesions.
Under general anesthesia with fiberoptic bronchoscope-guided intubation, surgical exploration via a transhyoid approach revealed two large, lobulated, solid masses (3 × 1.6 × 2 cm and 2.5 × 1.6 × 1.5 cm) located between the tongue base and epiglottis and inseparable from the epiglottic cartilage. The masses were resected en bloc with the involved epiglottic cartilage. Intraoperative frozen-section examination suggested lymphoid hyperplasia. Owing to concerns regarding potential postoperative airway compromise, a temporary tracheostomy was performed.
Definitive histopathological examination of paraffin-embedded sections showed dense submucosal lymphoid follicular hyperplasia with germinal center formation, extensive interfollicular eosinophilic infiltration, thin-walled capillary proliferation, and focal fibrosis, consistent with KD (Figure 4). Immunohistochemistry was positive for cluster of differentiation (CD) 3 (CD3) (interfollicular), CD20 (follicular), CD21 (organized network), Ki-67 (>50%), kappa, lambda, CD38 (partial), and CD138 (partial) and negative for CD30 and CD15.
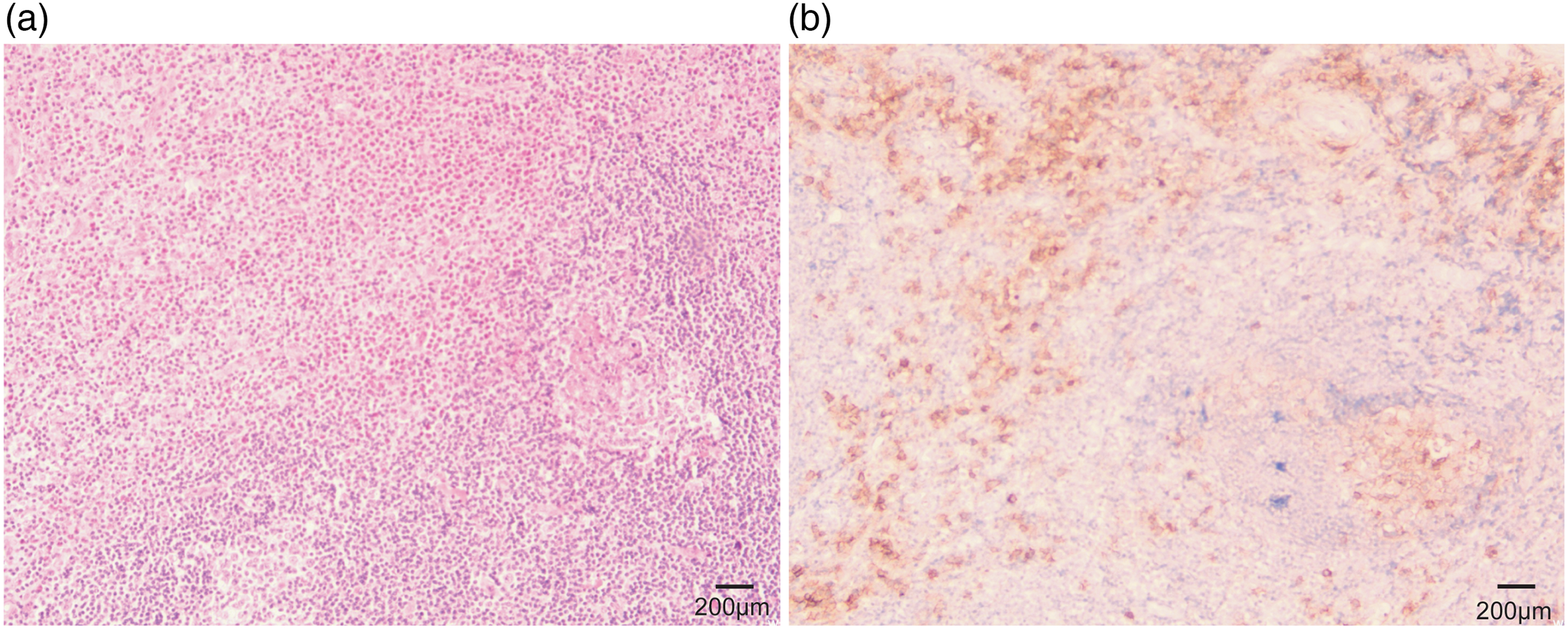
(a) Hematoxylin and eosin (H&E) staining revealed prominent lymphoid follicular hyperplasia within the submucosa. The interfollicular regions were expanded by dense eosinophilic infiltrates accompanied by proliferation of thin-walled blood vessels. Focal areas showed variable degrees of fibrotic proliferation. (b) Immunohistochemical staining for CD38. Plasma cells were partially positive for CD38. Original magnification: 10×; scale bar = 200 μm.
On postoperative day (POD) 2, laboratory testing revealed a peripheral blood eosinophil count of 0 × 109/L (normal range: 0.02–0.52 × 109/L) and an eosinophil percentage of 0% (normal range: 0.4%–8%). Follow-up measurements showed eosinophil counts of 1.13 × 109/L on POD 6, 1.23 × 109/L on POD 10, 1 × 109/L on POD18, and 0.95 × 109/L on POD 25. By postoperative day 25, the serum IgE level had decreased to 1180 IU/L (normal <100 IU/L) (Figure 5)
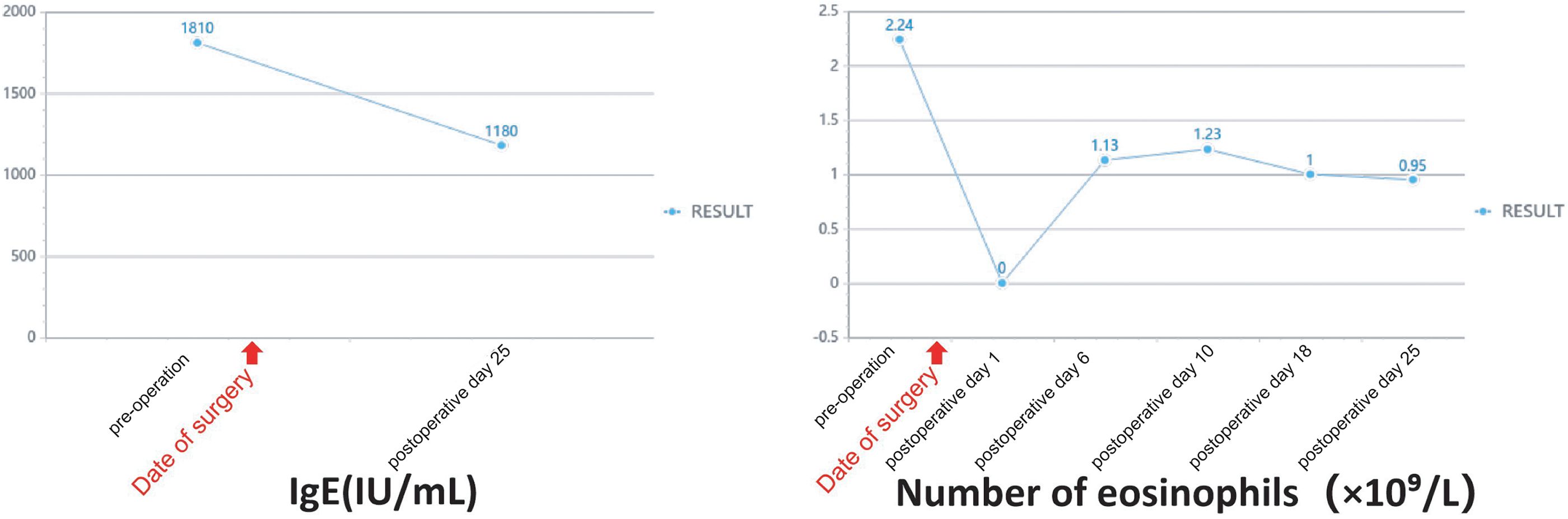
Laboratory findings after laryngectomy for Kimura disease. On postoperative day (POD) 2, the peripheral blood eosinophil count was 0 × 109/L. Subsequent follow-up measurements revealed eosinophil counts of 1.13 × 109/L on POD 6, 1.23 × 109/L on POD 10, 1 × 109/L on POD 18, and 0.95 × 109/L on POD 25. By POD 25, the serum IgE level had declined.
The tracheostomy tube was successfully removed 2 months postoperatively following an uneventful 48-h capping trial. The patient has remained asymptomatic.
Follow-up includes periodic clinical and endoscopic evaluations for recurrence, monitoring of peripheral eosinophil counts and serum IgE levels, and imaging when indicated. To date, the patient has shown no evidence of recurrence or complications and reports a good quality of life. The reporting of this case conforms to the CARE guidelines. 5
Discussion
KD is a rare chronic inflammatory disorder that typically presents with painless head and neck masses, marked eosinophilia, and elevated serum IgE levels. A review of the literature identified only 13 previously reported cases involving the epiglottis, including one with concomitant lip involvement. 4 In our case, the diagnosis was established based on characteristic imaging, histopathological, and laboratory findings. Management consisted of wide local excision followed by low-dose corticosteroid therapy, with no recurrence observed at the 1-year follow-up. Peripheral eosinophil counts and serum IgE levels decreased following treatment.
The classic clinical triad of KD comprises painless head/neck masses (commonly involving the salivary glands or lymph nodes), peripheral blood eosinophilia, and elevated serum IgE levels. Pathological diagnosis relies on characteristic features, including reactive lymphoid follicular hyperplasia, dense eosinophilic infiltrates (sometimes forming microabscesses), postcapillary venule proliferation, and fibrosis. Immunohistochemistry (e.g. CD3, CD20, and CD21) helps confirm the benign reactive nature of the lesion and exclude mimics such as lymphoma or angiolymphoid hyperplasia with eosinophilia (ALHE). KD is characterized by prominent lymphoid follicles, marked eosinophilia with elevated IgE levels, and non-epithelioid endothelial cells; ALHE is distinguished by epithelioid endothelial cells, mild eosinophilia, and MYC/FOSB alterations in some cases. Lymphoma typically presents with atypical lymphoid infiltrates showing clonal T-cell receptor or immunoglobulin gene rearrangements, often accompanied by lymphadenopathy and B symptoms (Table 1).
A 2022 meta-analysis 6 indicated lower recurrence rates with surgical excision than with conservative management for localized disease. Prognosis may be more favorable in patients with smaller tumors (<3 cm), shorter symptom duration (<5 years), lower peripheral eosinophil percentages (<20%), or lower serum IgE levels (<10,000 IU/mL). Adjuvant therapies, 7 including corticosteroids, immunomodulators (e.g. cyclosporine and cyclophosphamide), low-dose radiotherapy, and targeted biologics such as omalizumab (anti-IgE) and dupilumab,8,9 may be combined with surgery for optimal disease control. However, recurrence rates remain high (up to 62%), 10 and no standardized treatment protocol has been established.
Distinguishing features between Kimura disease (KD) , angiolymphoid hyperplasia with eosinophilia (ALHE) and Lymphoma.
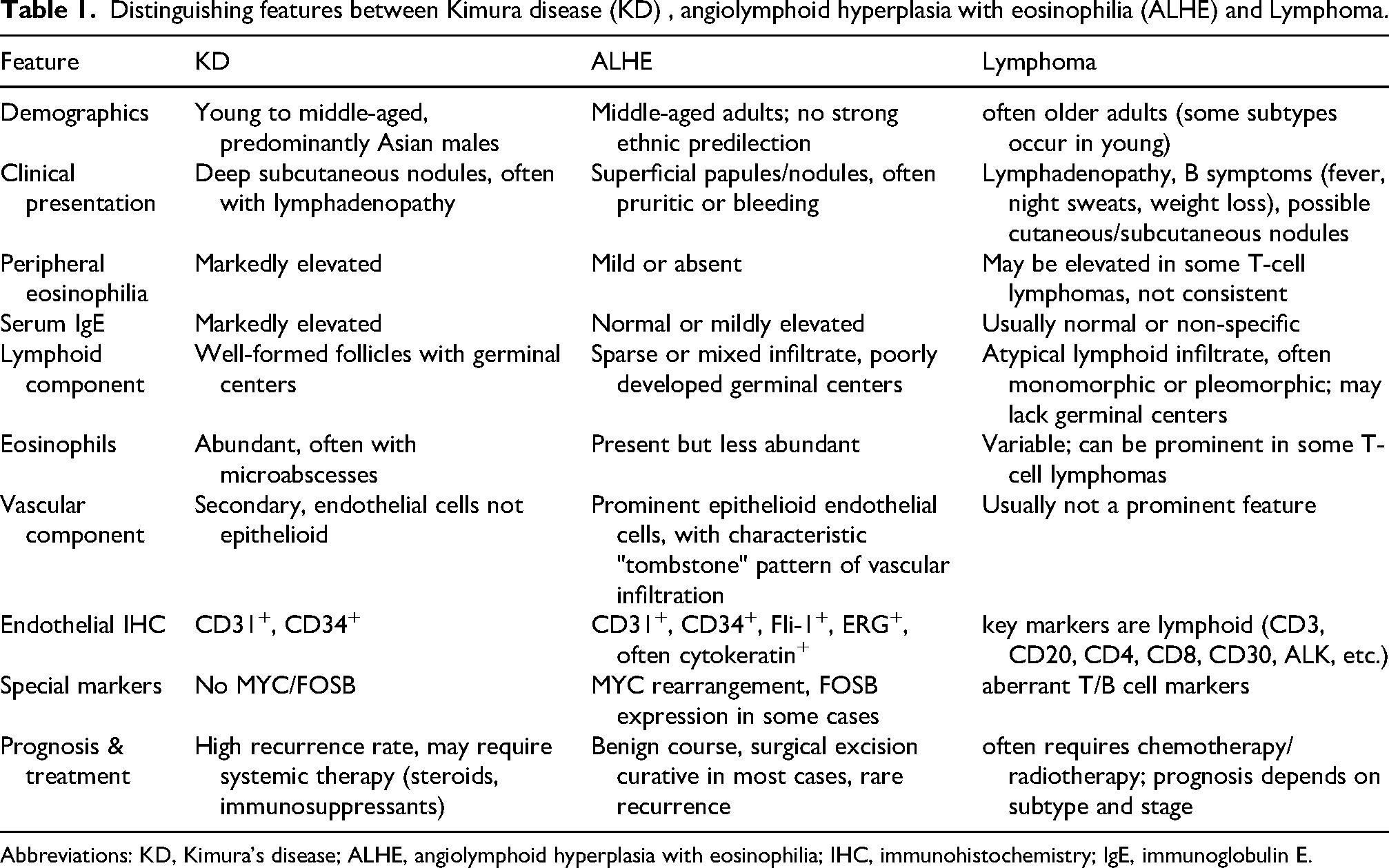
Abbreviations: KD, Kimura's disease; ALHE, angiolymphoid hyperplasia with eosinophilia; IHC, immunohistochemistry; IgE, immunoglobulin E.
Given the high potential for recurrence and the frequent association with renal disease (incidence, 10%–60%), 11 long-term follow-up is imperative. Follow-up should include clinical examinations, monitoring of eosinophil counts and serum IgE levels, and periodic assessment of renal function.
This case underscores that KD should be considered in the differential diagnosis of painless epiglottic masses and carefully distinguished from ALHE, lymphoma, and other entities. Treatment should be individualized. Surgery is effective for local disease control but is associated with a risk of recurrence. Systemic corticosteroids are beneficial; however, prolonged therapy may be required. Long-term surveillance is essential for detecting recurrence and complications such as nephrotic syndrome.
Conclusion
We present a rare case of epiglottic KD in a middle-aged woman, successfully managed with wide local excision and postoperative low-dose oral methylprednisolone. The patient remained recurrence-free at 1 year, with resolution of eosinophilia and elevated IgE levels, supporting the effectiveness of this combined approach for epiglottic KD.
Footnotes
Acknowledgments
This work was supported by the Medical Science Research Project of the Hebei Provincial Health Commission (Grant No. 20220255).
Ethics approval
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Medical Ethics Committee of Bethune International Peace Hospital (Ethics Approval No.: 2025-KY-243). Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Copyright transfer statement
The authors have signed the Copyright Transfer Agreement.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
All data generated or analyzed during this study are included in this article. Further details are available from the corresponding authors upon reasonable request.