
Abstract
Objective
To characterize interspecialty variation and areas of consensus in the understanding and clinical management of functional hypothalamic amenorrhea among physicians from different clinical specialties in China.
Methods
We conducted a nationwide, cross-sectional questionnaire survey of licensed physicians practicing in reproductive endocrinology, obstetrics and gynecology, and related specialties involved in functional hypothalamic amenorrhea care. The survey was administered anonymously via a national continuing medical education platform affiliated with the Peking Union Medical College Hospital Alliance between 1 November and 30 November 2025.
Results
A total of 2026 questionnaires were included in the final analysis, comprising 112 reproductive endocrinologists (5.5%), 1516 obstetricians–gynecologists (74.8%), and 398 physicians from other specialties (19.6%). Overall, only 62.7% of respondents recognized genetic susceptibility as a contributing factor to functional hypothalamic amenorrhea, and only 43.9% of respondents perceived that functional hypothalamic amenorrhea was generally diagnosed appropriately. Compared with physicians from other specialties, reproductive endocrinologists and obstetricians–gynecologists were significantly more likely to prioritize sex hormone evaluation, pelvic ultrasonography, and assessment of the thyroid and adrenal axes (all p < 0.01), whereas physicians from other specialties more frequently reported emphasizing assessments of energy metabolism (p < 0.01). Among women without fertility intentions, reproductive endocrinologists were more likely to report prioritizing elimination of precipitating factors (p < 0.05) and recommending hormone replacement and bone-targeted therapies (both p < 0.01). For women desiring pregnancy, reproductive endocrinologists were more likely to report recommending ovulation induction (p < 0.01), whereas physicians from other specialties reported greater support for the use of pulsatile gonadotropin-releasing hormone pumps (p < 0.01).
Conclusions
Variations were observed in physicians’ self-reported diagnostic and management approaches to functional hypothalamic amenorrhea across clinical specialties in China. These findings suggest the importance of promoting multidisciplinary consensus, developing standardized clinical pathways, and strengthening interdisciplinary collaboration to improve the quality of care for women with functional hypothalamic amenorrhea.
Keywords
Introduction
Functional hypothalamic amenorrhea (FHA) is a form of chronic anovulation caused by nonorganic, reversible suppression of the hypothalamic–pituitary–ovarian axis. In recent years, the prevalence of FHA among women of reproductive age has risen, accounting for 25%–35% of secondary amenorrhea cases and affecting approximately 17.4 million women worldwide.1,2 The etiology of FHA is complex, involving multiple factors such as psychosocial stress, disordered/restrictive eating, excessive exercise, and genetics.3,4 Psychological stress may disrupt hypothalamic regulation of reproduction via activation of the hypothalamic–pituitary–adrenal (HPA) axis, 5 whereas inadequate energy availability resulting from restrictive eating or excessive physical activity can suppress pulsatile gonadotropin-releasing hormone (GnRH) secretion through metabolic mediators (particularly leptin, insulin, and ghrelin). 6 In addition, recent evidence has highlighted a genetic susceptibility to FHA that could explain interindividual variability in stress response. 7
Although amenorrhea and hypogonadotropic hypoestrogenism are the hallmark clinical features of FHA, reproductive dysfunction, including infertility, as well as neuropsychiatric abnormalities, bone loss, and increased cardiovascular disease incidence may also represent a significant burden for many patients with FHA. In clinical practice, FHA is commonly defined as amenorrhea ≥3 consecutive months, estradiol (E2) < 50 pg/mL, follicle-stimulating hormone (FSH) and luteinizing hormone (LH) < 10 mIU/L, and an LH/FSH ratio <1 after exclusion of other etiologies. 8 Current clinical guidelines emphasize that FHA is a diagnosis of exclusion and recommend a multidisciplinary approach to management whenever feasible. 9 Accordingly, clinicians should be prepared to recognize this condition and understand its pathophysiology to make a timely diagnosis and manage the disorder in affected women.
Despite these recommendations, data on clinicians’ knowledge and self-reported diagnostic and management approaches to FHA remain limited. In particular, little is known about whether and how diagnostic and therapeutic approaches may vary across clinical specialties. To address this gap, we conducted a large-scale, nationwide cross-sectional survey to evaluate specialty-specific differences in the understanding, diagnosis, and management of FHA among physicians in China.
Methods
Study setting and design
This nationwide, cross-sectional questionnaire study was conducted and reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 10 The study protocol was approved by the Ethics Committee of Peking Union Medical College Hospital, Chinese Academy of Medical Sciences (Beijing, China) on 13 October 2025 (Approval No. 1–25PJ2617), and complied with the Declaration of Helsinki (revised in 2024).
Participants and data collection
Licensed physicians, including residents, attending physicians, and specialists practicing in obstetrics and gynecology, reproductive endocrinology, and related fields across China, were invited to participate. Participants were recruited using a convenience sampling approach through the official communication platform of the Peking Union Medical College Hospital (PUMCH) Alliance, which comprises 123 regional and specialty-specific online collaboration groups. The questionnaires were administered via the online survey platform Wenjuanxing between 1 November and 30 November 2025. Electronic informed consent was obtained from all participants prior to participation. Participants were required to actively check a confirmation box after reading the study information page, which served as an electronic signature. All data were collected anonymously, and no personally identifiable information was recorded. All data were de-identified prior to analysis to ensure participant confidentiality.
Questionnaire content
The questionnaire used in this study was specifically developed for this nationwide survey. Item generation was informed by current international guidelines and relevant literature on FHA. An initial draft of the questionnaire was reviewed and refined through expert consultation involving four senior clinicians from PUMCH, each with more than 20 years of clinical experience.
The questionnaire collected information on demographic and professional characteristics, including sex, age, hospital level, specialty, years of clinical practice, and experience in managing FHA. In addition, respondents were asked to estimate their perceived adequacy of FHA diagnosis in their own clinical practice, with response options including “generally appropriate diagnosis,” “underestimated diagnosis,” “overestimated diagnosis,” and “uncertain.” These responses reflected physicians’ self-reported perceptions rather than objectively measured diagnostic accuracy. Knowledge-based multiple-choice questions assessed respondents’ understanding of FHA etiology, clinical presentation, diagnostic evaluation, and treatment strategies for patients with and without fertility intentions. The full English version of the questionnaire is provided as Supplementary File S1.
Before dissemination, the questionnaire was piloted among 30 practicing clinicians to ensure clarity and content validity. Feedback from the pilot phase was incorporated into the final version of the survey.
Statistical analysis
Statistical analyses were performed using SPSS version 27.0 (IBM Corp., Armonk, NY, USA). Categorical variables are presented as frequencies and percentages. Comparisons among specialty groups were primarily conducted using Pearson's chi-square test. Fisher's exact test was used when expected cell counts were less than 5. All statistical tests were two-sided, and a p value < 0.05 was considered statistically significant.
Results
General characteristics of the participants
A total of 2073 questionnaires were initially collected. Questionnaires completed in less than 85 s (predefined as insufficient response time) or with substantial missing responses were excluded to ensure data quality. Specifically, 16 questionnaires (0.77%) were excluded due to insufficient completion time and 31 questionnaires (1.50%) due to substantial missing data, resulting in 2026 valid questionnaires included in the final analysis. The respondents comprised 112 reproductive endocrinologists (5.5%), 1516 obstetricians–gynecologists (74.8%), and 398 physicians from other related specialties (19.6%), including internal medicine, general practice, and nutrition. Most participants were female (93.5%), older than 35 years (79.7%), and had more than 10 years of clinical experience (75.8%). Overall, 88.8% were employed at secondary or tertiary hospitals. Detailed participant characteristics are summarized in Table 1.
General characteristics of participants.
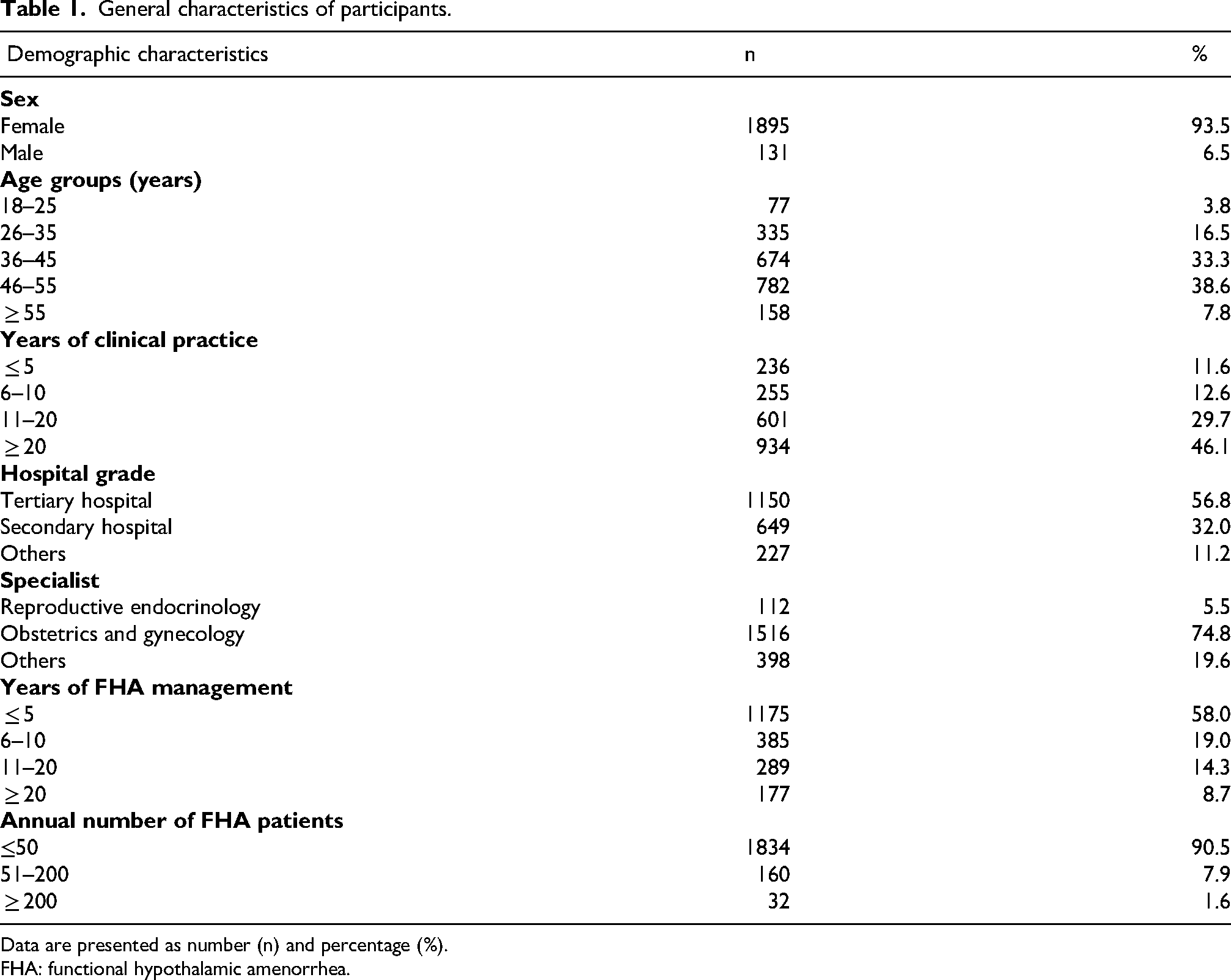
Data are presented as number (n) and percentage (%).
FHA: functional hypothalamic amenorrhea.
Awareness and understanding of FHA
The results show that rapid weight loss was the most commonly perceived cause of FHA (97.8%), followed by excessive psychological stress (95.0%) and high-intensity exercise/overwork (89.2%). In contrast, only 62.7% of respondents identified genetic susceptibility as a contributing factor. In addition, respondents reported that the most common presenting complaint was irregular menstruation (93.3%). Infertility (66.3%), neuropsychiatric symptoms (53.7%), genitourinary symptoms (37.5%), vasomotor symptoms (33.5%), and musculoskeletal symptoms (27.9%) were also reported as common reasons for consultation. Additionally, the key diagnostic considerations for FHA include the minimum duration of amenorrhea (≥3 consecutive months) and the exclusion of other causes of amenorrhea, which have been included in guidelines for many years and were recognized by most respondents (approximately 80%). Although most respondents correctly identified prolonged amenorrhea and exclusion of other causes as key diagnostic criteria, only 43.9% of respondents perceived that FHA was generally diagnosed appropriately in their clinical practice (Table 2).
Awareness and understanding of FHA.

Data are presented as number (n) and percentage (%). Multiple responses were allowed where applicable.
FHA: functional hypothalamic amenorrhea.
Diagnosis and evaluation of FHA
Compared with physicians from other specialties, reproductive endocrinologists and obstetricians–gynecologists were significantly more likely to report performing sex hormone testing, pelvic ultrasonography, and thyroid and adrenal axis evaluations (all p < 0.01). In contrast, physicians from other specialties were significantly more likely to report prioritizing assessments of energy metabolism (p < 0.01). No significant differences were observed among groups in the reported use of gonadotropin-releasing hormone stimulation testing or bone mineral density assessment (Figure 1).

Diagnosis and evaluation of FHA. (a) Sex hormone evaluation was more frequently performed by reproductive endocrinologists and obstetricians-gynecologists compared with other specialties (P < 0.01). (b) Pelvic ultrasound examination was also more frequently performed by reproductive endocrinologists and obstetricians-gynecologists (P < 0.01). (c) Hypothalamic-pituitary-adrenal (HPA) and hypothalamic-pituitary-thyroid (HPT) axis assessments were more commonly selected by reproductive endocrinologists and obstetricians-gynecologists (P < 0.01). (d) No significant differences were observed among specialties in the use of gonadotropin-releasing hormone (GnRH) stimulation testing (P > 0.05). (e) Energy metabolism assessments were more frequently selected by physicians from other specialties compared with reproductive endocrinologists and obstetricians-gynecologists (P <0.01). (f) Bone density evaluation did not differ significantly across specialty groups (P > 0.05). Data are presented as percentages (%).
Treatment and management of FHA patients with or without fertility needs
For patients without fertility intentions, most respondents favored elimination of precipitating factors and hormone replacement therapy. Specifically, reproductive endocrinologists were significantly more likely than physicians from other specialties to report recommending removal of causative factors (p < 0.05). In addition, reproductive endocrinologists and obstetricians–gynecologists were more likely than physicians from other specialties to recommend hormone replacement and bone-targeted therapies (both p < 0.01). In contrast, physicians from other specialties reported greater support for the use of pulsatile gonadotropin-releasing hormone pumps (p < 0.01).
For patients desiring pregnancy, addressing underlying causes was widely endorsed. Reproductive endocrinologists were significantly more likely to report recommending ovulation induction compared with other groups (p < 0.01). Obstetricians–gynecologists and reproductive endocrinologists more frequently reported supporting the use of traditional Chinese medicine than physicians from other specialties (p < 0.05 and p < 0.01, respectively). However, no significant intergroup differences were observed with respect to causative factor removal or bone-targeted therapy. In contrast, physicians from other specialties reported greater support for the use of pulsatile gonadotropin-releasing hormone pumps (p < 0.01). (Figure 2).

Treatment and management of FHA patients with or without fertility needs. (a) Treatments recommended for patients without fertility needs. (b) Treatments recommended for patients with fertility needs.
Discussion
To our knowledge, this is one of the first nationwide studies to systematically evaluate interspecialty variation in physicians’ self-reported diagnostic and management approaches to FHA in China. Although most respondents demonstrated adequate awareness of the core etiology, typical clinical manifestations, and key diagnostic principles of FHA, substantial differences were observed in both self-reported diagnostic evaluation and therapeutic decision-making across specialties. These findings are broadly consistent with existing guideline recommendations that emphasize the complexity and multisystem nature of FHA, while also suggesting potential gaps between guideline-based principles and reported clinical practice patterns. 9
Regarding diagnostic approaches, reproductive endocrinologists and obstetricians–gynecologists were significantly more likely to report prioritizing sex hormone testing, pelvic ultrasonography, and assessment of the thyroid and adrenal axes. This diagnostic emphasis is consistent with current evidence demonstrating that FHA is frequently accompanied by adaptive neuroendocrine alterations, including activation of the HPA axis and suppression of the hypothalamic-pituitary-thyroid axis, reflecting chronic stress and energy deficiency states. 11 As outlined in Endocrine Society clinical practice guidelines, evaluation of these endocrine axes is recommended not only to exclude alternative causes of amenorrhea, such as thyroid dysfunction or Cushing syndrome, but also to provide objective markers of the underlying pathophysiological milieu in FHA. 9 In contrast, physicians from other specialties more frequently emphasized assessments of energy metabolism, which is consistent with evidence that menstrual function is highly sensitive to energy availability and body composition. Classic work by Loucks et al. 12 demonstrated that luteinizing hormone pulsatility is disrupted when energy availability falls below approximately 30 kcal/kg fat-free mass, while subsequent studies have suggested that restoration of menses may require a minimum body fat percentage exceeding 22%. 13 These findings underscore the complementary value of metabolic and nutritional assessment in FHA and may help explain specialty-specific diagnostic priorities observed in this survey.
Notably, fewer than half of respondents (43.9%) reported confidence in their ability to appropriately assess patients with suspected FHA. This finding suggests a potential gap between theoretical knowledge and self-reported clinical confidence. Several factors may contribute to this observation. First, FHA remains a diagnosis of exclusion with nonspecific clinical manifestations, requiring clinicians to integrate endocrine, metabolic, and psychosocial information, which may increase diagnostic complexity. Previous studies have suggested that FHA may remain underrecognized with misdiagnosis being relatively common. For instance, a retrospective study found that between 1.7% and 36.9% of women referred for suspected polycystic ovary syndrome were subsequently diagnosed with FHA, highlighting the potential for misclassification in clinical settings. 14 In addition, this finding may reflect possible gaps in current medical education and training. FHA is often not systematically emphasized in residency or continuing medical education programs, and structured interdisciplinary training remains limited. Given the multifactorial nature of FHA, insufficient integration of knowledge across specialties may hinder clinicians’ ability to develop a comprehensive diagnostic approach. Moreover, there is limited published literature directly addressing these educational and training gaps, suggesting a clear need for further investigation into standardized curricula and targeted educational interventions.
Substantial variation was also observed in therapeutic strategies, which may reflect differences in clinical focus and thresholds for treatment escalation. Consistent with guideline recommendations, lifestyle modification and elimination of precipitating factors were widely endorsed as first-line interventions across all specialties. 9 Existing evidence supports the central role of nutritional rehabilitation in FHA management, with systematic reviews demonstrating that restoration of adequate energy intake can lead to menstrual recovery within 1–12 months in many patients. 15 In addition, cognitive behavioral therapy has been shown in randomized controlled trials to facilitate recovery of ovarian function and normalization of hypothalamic-pituitary signaling, suggesting the importance of addressing psychological stressors alongside nutritional factors. 16
Beyond lifestyle-based interventions, reproductive endocrinologists and obstetricians–gynecologists were more likely to report recommending hormone replacement therapy and bone-targeted treatments for patients without fertility intentions. 17 This pattern is consistent with evidence indicating that prolonged hypoestrogenism, energy deficiency, and inadequate calcium and vitamin D intake contribute to reduced bone mineral density in patients with FHA. 18 Prior studies have demonstrated associations between longer duration of amenorrhea, earlier age at onset, and more severe bone loss, while weight restoration remains the most effective intervention for improving skeletal health. 19 Pharmacological approaches, including estrogen replacement and bisphosphonates, may be considered in selected patients with significant bone loss, although their use requires careful consideration of age, reproductive plans, and potential adverse effects.20,21
For patients desiring pregnancy, reproductive endocrinologists were more likely to report recommending ovulation induction, which is consistent with guideline-based fertility management strategies. 9 Importantly, current recommendations caution against ovulation induction in women with a body mass index below 18.5 kg/m2 due to increased risks of adverse pregnancy outcomes, emphasizing the importance of careful patient selection and preconception optimization. 22 Physicians from other specialties, however, reported greater support for pulsatile gonadotropin-releasing hormone therapy. Evidence from a meta-analysis of 35 studies involving over 1000 patients with hypothalamic amenorrhea indicates that pulsatile gonadotropin-releasing hormone therapy achieves high ovulation, pregnancy, and live birth rates with relatively low risks of ovarian hyperstimulation and multiple gestation. 23 Long-term cohort data further support its efficacy and safety in appropriately selected patients. 24 Nevertheless, the limited availability, high cost, and technical demands of this therapy may constrain its widespread use in routine clinical practice, potentially contributing to differing perceptions across specialties.
Complementary and adjunctive therapies also featured prominently in clinical decision-making. Approximately half of respondents reported using traditional Chinese medicine in the management of FHA, reflecting its widespread use in China. Prior clinical studies have reported favorable outcomes with kidney-tonifying herbal formulations and acupuncture-based interventions, including improved ovulation rates and reduced recurrence, although the quality and consistency of evidence remain variable.25,26 Emerging therapies such as leptin and kisspeptin have shown promise in small-scale studies by targeting upstream regulators of the hypothalamic-pituitary-gonadal axis, but their safety, efficacy, and long-term outcomes require further evaluation before widespread clinical application.27,28
Clinical implications
Taken together, these findings suggest that observed variation in physicians’ self-reported approaches may be related to differences in training background, clinical priorities, and perceived scope of responsibility across specialties, rather than fundamental disagreement over core principles of FHA management. Given the multifactorial pathophysiology of FHA, standardized diagnostic pathways that integrate endocrine, metabolic, nutritional, and psychosocial assessments may help bridge potential gaps between specialties. In addition, structured referral algorithms and targeted cross-specialty education may facilitate more consistent, patient-centered care, particularly for women with complex presentations or fertility goals.
Strengths and limitations
The strengths of this study include its large sample size and broad national representation of physicians involved in FHA care, enhancing the generalizability of the findings within China. Several limitations should be acknowledged. The online, self-reported survey design may not fully reflect actual clinical practices, and participants may have consulted reference materials when responding. Additionally, the anonymous nature of the survey precluded assessment of nonparticipation and response bias. Furthermore, participants were recruited using a convenience sampling strategy, which may have resulted in a higher proportion of respondents from obstetrics and gynecology. Physicians from primary care, internal medicine, or rural healthcare settings may therefore be underrepresented, and the findings should be interpreted with caution when generalizing to all clinicians involved in the management of amenorrhea. In addition, although differences across specialties were the primary focus of this study, variations in years of clinical experience and FHA case volume may have influenced physicians’ responses. Finally, while our survey identified physicians’ self-reported tendencies to prioritize energy metabolism assessments, recommend removal of causative factors, and consider bone-targeted therapies, it did not collect detailed information on the specific metrics, factors, or pharmacological agents used. This limits the ability to draw conclusions about the exact clinical methods or interventions that may be applied in these domains. Future research exploring the specific assessment methods, therapeutic strategies, and decision-making processes in greater detail may help further inform clinical practice and optimize care for patients with FHA.
Conclusion
Our survey identified variation and potential knowledge gaps in physicians’ self-reported approaches to the diagnosis and management of FHA across medical specialties. These findings suggest that differences in training background and clinical priorities may be associated with variation in diagnostic and management approaches. Strengthening continuing medical education, promoting standardized clinical pathways, and encouraging interdisciplinary collaboration may help improve the consistency of FHA management and enhance the quality of care for affected patients.
Footnotes
Acknowledgments
The authors are grateful to all Chinese physicians who participated in our survey.
Author contributions
YZ: research plan implementation, questionnaire design, formal analysis, conceptualization, and manuscript writing; YYG, YCW: questionnaire collection, formal analysis, and conceptualization; YL, YD: questionnaire distribution, completion, and collection, and manuscript review; WX, XYS, WQL, YW: questionnaire distribution, completion, and collection; AJS: research plan implementation, questionnaire design, and organization and coordination of the national survey.
Funding
This work was supported by the National Key R&D Program of China (Grant No. 2025YFC3508000; Project No. 2025YFC3508004).
Declaration of conflicting interests
No potential conflict of interest was reported by the authors.
Data availability statement
The datasets used in this article would be shared on reasonable request to the corresponding author.
Supplemental material
Supplemental material for this article is available online.