
Abstract
Objective
To evaluate the association between a prehospital-to-in-hospital integrated transfusion workflow and transfusion timeliness, coagulation-related indices, and short-term clinical outcomes in patients with severe trauma requiring emergency transfusion.
Methods
This single-center observational before-and-after study included 120 consecutive patients with severe trauma requiring emergency transfusion (60 per group). The conventional workflow group included patients treated between January 2022 and August 2023, and the integrated workflow group included patients treated between January 2024 and March 2025. The integrated workflow comprised prehospital assessment, real-time pre-arrival communication, early activation of emergency and transfusion resources, electronic transfusion ordering, and dedicated blood product delivery. The primary outcome was time to first transfusion, interpreted as a process-efficiency measure. Secondary outcomes included coagulation-related indices before transfusion and at 24 h, 24-h blood product utilization, intensive care unit length of stay, and in-hospital mortality. Univariable and multivariable analyses were performed to evaluate the association between workflow group and key outcomes.
Results
Baseline demographic, clinical, and pretransfusion laboratory characteristics were generally comparable between groups. The integrated workflow group had a shorter time to first transfusion than the conventional workflow group (25.1 ± 6.4 vs. 56.3 ± 8.2 min, p < 0.001). Fresh frozen plasma transfused within 24 h was higher in the integrated workflow group (1776 ± 348 vs. 1395 ± 317 mL, p < 0.001), whereas 24-h packed red blood cell use was similar (14.2 ± 5.4 vs. 14.7 ± 5.7 U, p = 0.645). At 24 h after transfusion, international normalized ratio and activated partial thromboplastin time were lower in the integrated workflow group (1.24 ± 0.29 vs. 1.37 ± 0.33, p = 0.022; 35.1 ± 6.6 vs. 42.1 ± 8.1 s, p < 0.001). Intensive care unit length of stay was shorter (7.3 ± 2.3 vs. 8.7 ± 3.8 days, p = 0.013). In-hospital mortality was numerically lower but did not differ significantly between groups (13.3% vs. 21.7%, p = 0.337).
Conclusions
In this single-center observational before-and-after study, a prehospital-to-in-hospital integrated transfusion workflow was associated with shorter time to first transfusion, greater early plasma administration, more favorable coagulation-related indices at 24 h, and shorter intensive care unit length of stay in patients with severe trauma requiring emergency transfusion. These findings should be interpreted primarily as evidence of improved workflow efficiency and hypothesis-generating associations with intermediate physiologic and short-term clinical outcomes. Further multicenter studies using standardized workflow timestamps, protocol-adherence assessment, and more rigorous adjustment for confounding are needed to determine whether this approach improves patient-centered outcomes across different trauma systems.
Keywords
Introduction
Severe trauma remains a major cause of preventable death worldwide, particularly among younger adults, and uncontrolled hemorrhage is one of the leading causes of early post-injury mortality.1–3 In patients with major bleeding, timely hemostatic resuscitation is essential because delayed blood product delivery can aggravate shock, acidosis, tissue hypoperfusion, and trauma-induced coagulopathy.1,2,4 Contemporary trauma care therefore emphasizes rapid activation of transfusion pathways, early balanced component therapy, and close coordination between resuscitation teams and transfusion services.1,4,5
Trauma-induced coagulopathy may develop early after injury, sometimes even before hospital arrival, and is strongly associated with adverse outcomes. 6 Evidence from observational and randomized studies, including the PROMMTT (Prospective, Observational, Multicenter, Major Trauma Transfusion) and PROPPR (Pragmatic, Randomized, Optimal Platelet and Plasma Ratios) studies, has established balanced transfusion and damage-control resuscitation as central principles in modern trauma management.4,7 Current guidelines for major bleeding similarly emphasize the need to minimize avoidable delays in blood product availability and administration.1,2
Despite these advances, workflow-related delays remain common in routine practice. In many hospitals, emergency transfusion is initiated only after patient arrival and depends on a sequence of time-consuming steps, including recognition of transfusion need, order completion, sample transport, blood typing, crossmatching, and physical delivery of blood products to the emergency department. These vulnerabilities may be more pronounced in settings where trauma systems are still evolving and prehospital-to-in-hospital coordination remains incomplete. 8
Previous workflow-focused studies have shown that optimization of in-hospital emergency transfusion processes can shorten time to first transfusion, increase early plasma administration, improve coagulation parameters, and reduce intensive care unit (ICU) length of stay in patients with severe trauma. 9 However, in many of these models, key preparatory actions still begin only after hospital arrival. For patients with life-threatening hemorrhage, this approach may leave the earliest therapeutic window underused. Evidence regarding the clinical impact of a prehospital-to-in-hospital integrated transfusion workflow remains limited.
A prehospital-to-in-hospital integrated transfusion workflow may address this limitation by moving recognition, communication, team activation, and blood preparation upstream. By initiating these steps before arrival, such a model may reduce sequential delays, facilitate earlier component preparation, and improve the timeliness of hemostatic resuscitation. We hypothesized that this integrated workflow would shorten time to first transfusion and be associated with more favorable coagulation-related and short-term clinical outcomes in patients with severe trauma requiring emergency transfusion. To test this hypothesis, we conducted a single-center observational before-and-after study comparing a conventional transfusion workflow with an integrated prehospital-to-in-hospital workflow.
Methods
Study design and setting
This single-center observational before-and-after study was conducted in the emergency department of the Linhai Second People’s Hospital, Taizhou, Zhejiang, China. A before-and-after design was used because the integrated transfusion workflow was implemented as a system-level quality improvement and clinical process intervention and could not be randomized at the individual patient level during routine emergency trauma care. The conventional workflow group comprised consecutive patients with severe trauma requiring emergency transfusion who were treated between January 2022 and August 2023. The integrated workflow group comprised consecutive patients treated between January 2024 and March 2025 after formal implementation of the prehospital-to-in-hospital integrated transfusion workflow. All eligible patients during the two study periods were screened consecutively. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guideline. 10
Ethics
This study was conducted in accordance with the Declaration of Helsinki of 1975, as revised in 2024. The study protocol was reviewed and approved by the Institutional Review Board of Linhai Second People’s Hospital, Taizhou, Zhejiang, China (approval no. 2024052101; approval date: January 2024). The requirement for informed consent was waived by the Institutional Review Board because of the observational nature of the study and the use of routinely collected clinical data. All patient data were de-identified before analysis, and no information that could identify individual patients is presented in this manuscript.
Study population
Patients were eligible if they had severe trauma, suspected or confirmed active bleeding, hemodynamic instability, and activation of emergency transfusion by the attending emergency physician or trauma team leader. Severe trauma was defined as trauma requiring emergency resuscitation and urgent evaluation for major hemorrhage based on injury severity and physiologic instability at presentation. Injury severity was assessed using the Injury Severity Score (ISS). 11 Hemodynamic instability was defined as systolic blood pressure <90 mmHg, persistent circulatory instability after initial fluid resuscitation, or clinical signs of ongoing hypoperfusion. Emergency transfusion activation was defined as formal initiation of urgent blood product preparation and administration by the emergency team because of suspected life-threatening traumatic hemorrhage. Active bleeding was identified by focused assessment with sonography for trauma (FAST), computed tomography (CT), or clinical evaluation. Supporting clinical features included pallor or diaphoresis, impaired responsiveness, a weak or rapid pulse, persistent hypotension, and imaging or clinical findings suggestive of ongoing hemorrhage.
Exclusion criteria were (a) pregnancy; (b) death within 2 h of emergency department arrival; (c) major pre-existing cardiopulmonary disease; (d) known coagulation disorders; (e) malignancy; (f) chronic hepatic or renal insufficiency; (g) or insufficient data for assessment of the primary outcome. These conditions were excluded because they could substantially affect coagulation status, transfusion requirement, or short-term outcomes independent of workflow exposure. Patients who died within 2 h of emergency department arrival were excluded because they usually could not complete the predefined workflow exposure assessment, 24-h laboratory reassessment, or ICU outcome evaluation. This exclusion was applied consistently to both study groups. However, because these patients may represent the most severely injured subgroup with early exsanguination or irreversible shock, the potential for survivor bias was recognized and is addressed in the Discussion.
Workflow definitions
Conventional workflow
Under the conventional workflow, transfusion-related procedures were initiated only after patient arrival in the emergency resuscitation area. Emergency physicians assessed the patient, determined the need for emergency transfusion, ordered laboratory tests, completed transfusion-related documentation, and sent blood samples for blood typing and crossmatching. Blood products were then prepared by the transfusion service and retrieved by emergency department personnel for administration.
Integrated workflow
Under the integrated workflow, severe trauma was identified in the prehospital setting, and key preparatory steps were moved upstream to reduce sequential delays. First, after initial on-site assessment and stabilization, prehospital emergency physicians transmitted real-time video images, vital sign monitoring data, and structured pre-arrival clinical information from the ambulance to the in-hospital emergency command system. Real-time prehospital-to-hospital communication was performed through the hospital emergency information platform using the ambulance-mounted mobile communication terminal connected to the hospital emergency network. The transmitted information included mechanism of injury, estimated bleeding risk, blood pressure, heart rate, oxygen saturation, mental status, suspected bleeding site, and preliminary prehospital interventions. When video transmission was unavailable or unstable, voice communication and structured electronic pre-arrival notification were used as backup communication methods. Transmission failure or instability was defined as failure of the in-hospital emergency team to receive real-time video or monitoring data before patient arrival. Formal transmission failure rates were not prospectively recorded during the study period; this limitation is addressed in the Discussion.
Second, hospital-based emergency physicians used the online emergency platform to guide prehospital management and immediately activated the relevant emergency response system, including the team leader, specialty consultants, laboratory department, and transfusion service. Third, the emergency physician immediately activated the transfusion protocol, ordered transfusion-related laboratory tests, and submitted the transfusion request electronically. A balanced transfusion strategy was initiated with a predefined packed red blood cell (PRBC)-to-fresh frozen plasma (FFP) ratio of approximately 1:1, whereas platelets and cryoprecipitate were prepared in parallel when indicated. No paper requisition forms were required, thereby enabling a paperless transfusion process and reducing administrative delays. Fourth, on arrival at the emergency department, the team leader reassessed the patient's vital signs and bleeding status. If the patient met the criteria for emergency transfusion, a nurse immediately collected blood samples for laboratory testing and blood typing. The transfusion service then performed crossmatching without delay, and the blood bank released the required blood products. These products were delivered to the emergency department by designated personnel already on standby, thereby minimizing the interval from transfusion decision to blood product administration.
Outcomes
The primary outcome was time to first transfusion, defined as the interval from the documented physician decision to activate emergency transfusion to the initiation of the first blood product. In the conventional workflow group, the physician decision time was defined as the time at which the attending emergency physician or trauma team leader documented emergency transfusion activation after patient arrival in the emergency resuscitation area. In the integrated workflow group, the physician decision time was defined as the time at which the in-hospital emergency physician confirmed activation of emergency transfusion based on prehospital transmitted information or, when prehospital information was insufficient, immediately after reassessment on emergency department arrival. The transfusion start time was defined as the first nursing-recorded administration time of any blood product. Time stamps were obtained from emergency resuscitation records, electronic transfusion orders, nursing transfusion records, and transfusion service logs. The same extraction rules were applied to both study groups. Because the integrated workflow was designed to move recognition and activation upstream, this primary outcome was interpreted as a process-efficiency measure rather than as an independent measure of clinical effectiveness.
Secondary outcomes were hemoglobin, platelet count, prothrombin time (PT), international normalized ratio (INR), and activated partial thromboplastin time (APTT) before transfusion and at 24 h after initiation of transfusion, PRBC and FFP utilization within 24 h after initiation of transfusion, ICU length of stay, and in-hospital mortality. In-hospital mortality was defined as death from any cause during the index hospitalization before hospital discharge and was not restricted to 30-day mortality.
Data collection and missing data
Clinical, laboratory, and transfusion data were extracted from electronic medical records, emergency resuscitation records, transfusion service logs, and laboratory information systems. Baseline variables included age, sex, systolic blood pressure on arrival, heart rate, ISS, 11 Glasgow Coma Scale (GCS) score on arrival, 12 injury mechanism, and the presence of active bleeding identified by FAST or CT. When available, additional clinical variables including traumatic brain injury, emergency surgery, and other major interventions related to hemorrhage control were reviewed to aid interpretation of between-group differences. Missing data were assessed for all variables included in the main analyses. Patients with insufficient data for assessment of the primary outcome were excluded. For included patients, missingness for reported baseline variables, laboratory variables, transfusion variables, and clinical outcomes was summarized descriptively. No imputation was performed because no missing data were observed for the variables included in the main analyses.
Statistical analysis
Continuous variables were expressed as mean ± standard deviation or median (interquartile range), according to distributional characteristics, and categorical variables as number (percentage). Between-group comparisons were performed using the independent-samples t test for normally distributed continuous variables and the Mann–Whitney U test for non-normally distributed variables when appropriate. Categorical variables were compared using the chi-squared test or Fisher's exact test, as appropriate. To reduce, but not eliminate, the influence of measured confounding in this before-and-after observational study, multivariable regression analyses were additionally performed for key outcomes. Time to first transfusion, 24-h INR, 24-h APTT, and ICU length of stay were analyzed using multivariable linear regression models, and in-hospital mortality was analyzed using multivariable logistic regression. Prespecified covariates included age, sex, systolic blood pressure on arrival, heart rate, ISS, injury mechanism, and active bleeding identified by FAST or CT. Adjusted effect estimates are reported with 95% confidence intervals (CIs). Model assumptions were assessed using residual diagnostics for linear regression analyses. Multicollinearity was assessed using variance inflation factors. For the logistic regression model for in-hospital mortality, model discrimination and calibration were assessed using the area under the receiver operating characteristic curve (AUC) and the Hosmer–Lemeshow goodness-of-fit test, respectively, when sample size permitted stable estimation. Adjusted R2 values for linear models and discrimination/calibration statistics for the logistic model are reported in Table 1 where available. All tests were two-sided, and p < 0.05 was considered statistically significant. Statistical analyses were performed using Statistical Package for the Social Sciences version 21.2 (IBM Corp., Armonk, NY, USA).
Adjusted associations between integrated workflow and key outcomes.

Adjusted for age, sex, arrival SBP, HR, ISS, injury mechanism, and active bleeding on FAST/CT.
APTT: activated partial thromboplastin time; AUC: area under the receiver operating characteristic curve; CI: confidence interval; FAST: focused assessment with sonography for trauma; H-L: Hosmer–Lemeshow; HR: heart rate; ICU: intensive care unit; INR: international normalized ratio; ISS: Injury Severity Score; OR: odds ratio; SBP: systolic blood pressure.
Results
Baseline characteristics and missing data
A total of 120 patients were included, with 60 patients in the conventional workflow group and 60 patients in the integrated workflow group. Baseline demographic and clinical characteristics were generally comparable between the groups. No significant between-group differences were observed in age, sex, systolic blood pressure on arrival, heart rate, ISS, GCS score on arrival, injury mechanism, or the proportion of patients with active bleeding identified by FAST or CT (all p > 0.05) (Table 2). Median GCS score on arrival was 11.0 (interquartile range, 9.0–13.0) in the conventional workflow group and 11.0 (interquartile range, 7.75–14.0) in the integrated workflow group (p = 0.841). In the integrated workflow group, active bleeding identified by FAST or CT was present in 49 of 60 patients (81.7%); therefore, 11 patients (18.3%) were treated using the integrated workflow but did not have active bleeding confirmed by FAST or CT according to the study definition. These patients met emergency transfusion activation criteria based on hemodynamic instability, suspected major hemorrhage, and clinical signs of hypoperfusion. Among the 120 included patients, no missing data were observed for the primary outcome, reported baseline variables, transfusion variables, pretransfusion laboratory variables, 24-h laboratory variables, ICU length of stay, or in-hospital mortality; therefore, no imputation was performed.
Baseline characteristics.
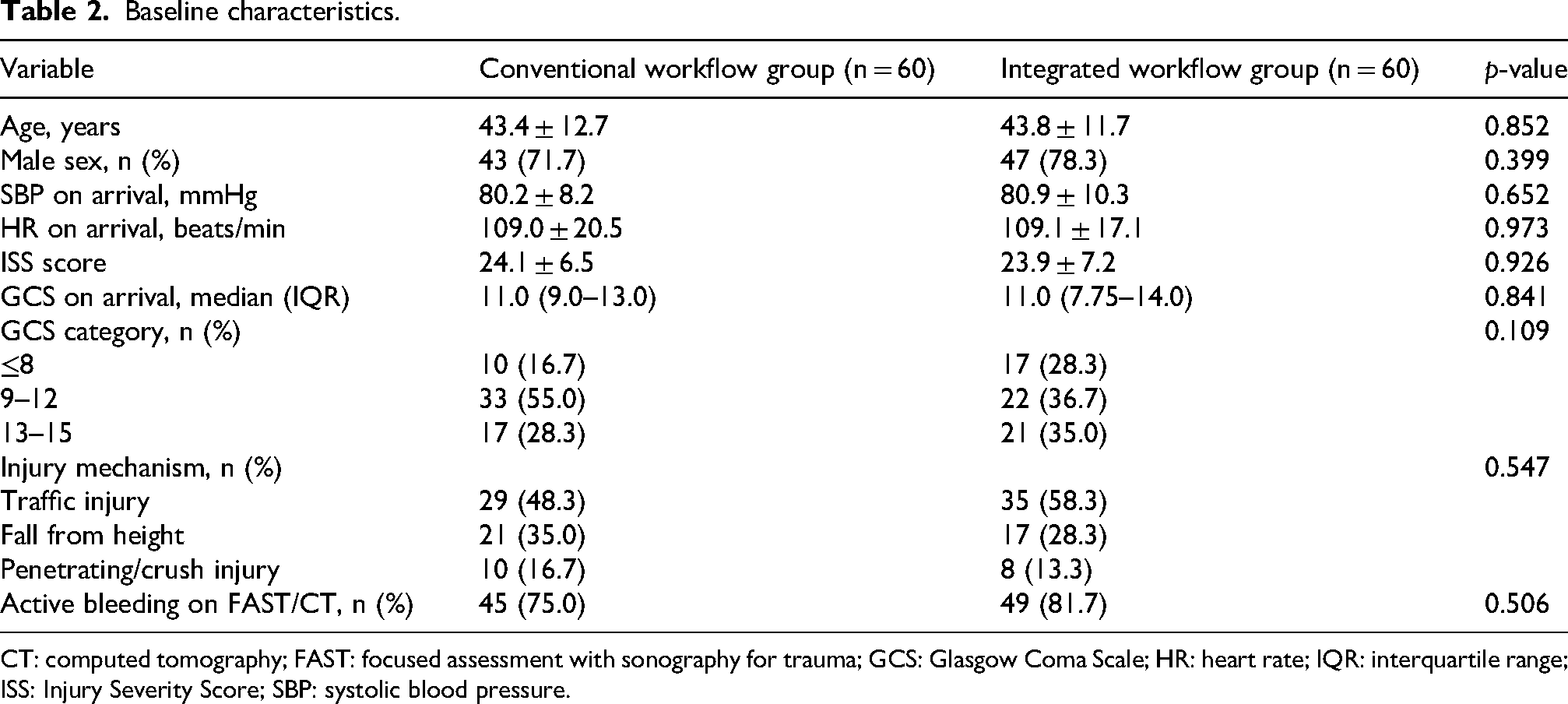
CT: computed tomography; FAST: focused assessment with sonography for trauma; GCS: Glasgow Coma Scale; HR: heart rate; IQR: interquartile range; ISS: Injury Severity Score; SBP: systolic blood pressure.
Time to first transfusion and blood product utilization
The integrated workflow group had a significantly shorter time to first transfusion than the conventional workflow group (25.1 ± 6.4 min vs. 56.3 ± 8.2 min, p < 0.001). FFP transfused within 24 h was significantly greater in the integrated workflow group than in the conventional workflow group (1776.3 ± 348.2 mL vs. 1395.2 ± 316.9 mL, p < 0.001). By contrast, 24-h PRBC utilization did not differ significantly between the groups (14.2 ± 5.4 U vs. 14.7 ± 5.7 U, p = 0.645). The absolute between-group difference in time to first transfusion was −31.13 min (95% CI −33.79 to −28.47) (Table 3).
Process measures and clinical outcomes.

In-hospital mortality was defined as death from any cause during the index hospitalization before hospital discharge.
FFP: fresh frozen plasma; ICU: intensive care unit; PRBC: packed red blood cell.
Laboratory findings before transfusion
Before transfusion, hemoglobin, platelet count, PT, INR, and APTT were similar between the groups (all p > 0.05) (Table 4). Mean hemoglobin was 87.1 ± 23.8 g/L in the conventional workflow group and 91.3 ± 23.3 g/L in the integrated workflow group. Mean INR was 1.50 ± 0.57 and 1.49 ± 0.51, respectively, and mean APTT was 47.1 ± 8.4 s and 44.9 ± 8.3 s, respectively.
Laboratory variables before transfusion.

APTT: activated partial thromboplastin time; INR: international normalized ratio; PT: prothrombin time.
Laboratory findings at 24 h after transfusion
At 24 h after transfusion, INR and APTT were significantly lower in the integrated workflow group than in the conventional workflow group. Mean INR was 1.24 ± 0.29 in the integrated workflow group versus 1.37 ± 0.33 in the conventional workflow group (p = 0.022), and mean APTT was 35.1 ± 6.6 s versus 42.1 ± 8.1 s, respectively (p < 0.001). Hemoglobin, platelet count, and PT did not differ significantly between the groups (Table 5).
Laboratory variables at 24 h after transfusion.

APTT: activated partial thromboplastin time; INR: international normalized ratio; PT: prothrombin time.
Clinical outcomes
ICU length of stay was significantly shorter in the integrated workflow group than in the conventional workflow group (7.3 ± 2.3 days vs. 8.7 ± 3.8 days, p = 0.013). In-hospital mortality, defined as death during the index hospitalization before hospital discharge, was numerically lower in the integrated workflow group (8/60 (13.3%) vs. 13/60 (21.7%)), but the difference was not statistically significant (p = 0.337) (Table 3). The absolute between-group difference in ICU length of stay was −1.45 days (95% CI −2.59 to −0.32).
Adjusted analyses
After adjustment for age, sex, systolic blood pressure on arrival, heart rate, ISS, injury mechanism, and active bleeding identified by FAST or CT, the integrated workflow remained independently associated with shorter time to first transfusion (adjusted β = −30.96 min, 95% CI −33.70 to −28.22, p < 0.001). The integrated workflow was also independently associated with lower 24-h INR (adjusted β = −0.15, 95% CI −0.26 to −0.04, p = 0.009) and lower 24-h APTT (adjusted β = −7.26 s, 95% CI −9.91 to −4.62, p < 0.001). For ICU length of stay, the adjusted β was −1.34 days (95% CI −2.50 to −0.18, p = 0.024). For in-hospital mortality, the adjusted odds ratio was 0.60 (95% CI 0.22 to 1.64, p = 0.324) (Table 1). Model strength indicators are shown in Table 1. Adjusted R2 values were 0.813 for time to first transfusion, 0.078 for 24-h INR, 0.219 for 24-h APTT, and 0.031 for ICU length of stay. For the in-hospital mortality model, the AUC was 0.668, and the Hosmer–Lemeshow goodness-of-fit test p-value was 0.739.
Discussion
The principal finding of this study was that implementation of a prehospital-to-in-hospital integrated transfusion workflow was associated with a substantial reduction in time to first transfusion in patients with severe trauma requiring emergency transfusion. This reduction was accompanied by greater early FFP administration, more favorable INR and APTT values at 24 h, and a shorter ICU length of stay. However, the reduction in time to first transfusion should be interpreted primarily as evidence of improved workflow efficiency because the intervention was specifically designed to move recognition, activation, blood preparation, and delivery coordination upstream. Therefore, this process outcome does not by itself establish independent clinical effectiveness. The strongest evidence from this study relates to workflow performance and intermediate physiologic outcomes, whereas the findings regarding patient-centered outcomes remain hypothesis-generating.
Among these findings, the reduction in time to first transfusion is operationally plausible. Under the integrated workflow, recognition of likely transfusion need, team activation, transfusion request submission, and blood preparation began before hospital arrival rather than only after the patient entered the resuscitation area. In patients with life-threatening hemorrhage, multiple in-hospital steps performed sequentially after arrival can introduce clinically meaningful delays. By shifting these steps upstream, the integrated workflow may reduce cumulative process delays and improve the timeliness of initial hemostatic support. This interpretation is consistent with major bleeding guidelines and trauma quality improvement literature emphasizing that avoidable delays in blood product delivery are associated with worse clinical trajectories.1,2,13
An important methodological consideration is the comparability of the starting point used to calculate time to first transfusion. Although the same operational definition was applied to both groups, the integrated workflow changed the clinical context in which transfusion activation occurred. In the conventional workflow, transfusion activation usually occurred after emergency department arrival and bedside reassessment. In contrast, the integrated workflow allowed activation based on prehospital information sharing and in-hospital preparation before arrival. This difference reflects the intended mechanism of the intervention but may also introduce non-equivalent timestamp bias. For this reason, the observed reduction in time to first transfusion should be interpreted as a measure of system-level process acceleration rather than as a fully independent clinical endpoint.
The present workflow should also be distinguished from established early blood availability strategies, such as massive transfusion protocol activation or early release of uncrossmatched type O blood. In mature trauma systems, these strategies may already provide rapid access to blood products for patients with suspected life-threatening hemorrhage. The integrated workflow evaluated in this study was not intended to replace such strategies. Rather, it represented a local systems-integration model designed to synchronize prehospital recognition, real-time information transmission, in-hospital team activation, electronic transfusion ordering, blood bank preparation, and dedicated blood product delivery. Its novelty therefore lies less in the concept of early transfusion itself and more in the coordinated movement of multiple preparatory steps from the post-arrival phase to the pre-arrival phase. This distinction may be particularly relevant for hospitals or regional trauma systems in which prehospital-to-in-hospital coordination and blood bank activation are not yet fully integrated.
The differences in INR and APTT at 24 h are biologically plausible. Trauma-induced coagulopathy may develop early after injury and is closely linked to shock, hypoperfusion, endothelial dysfunction, and dysregulation of coagulation and fibrinolytic pathways. 14 Timely hemostatic resuscitation is therefore a key component of damage-control management. In the present study, the integrated workflow group received more FFP within the first 24 h without a significant increase in PRBC use, suggesting that workflow redesign may affect not only when transfusion begins but also how early balanced component therapy is delivered. This pattern supports the view that improved process coordination can translate into more appropriate early transfusion composition and, in turn, more favorable short-term coagulation profiles. Updated patient blood management guidance similarly emphasizes early and repeated coagulation assessment as part of major hemorrhage protocols. 13
The shorter ICU length of stay observed in the integrated workflow group may also be clinically meaningful. Although ICU stay is influenced by many factors after admission, more efficient early resuscitation, earlier correction of coagulopathy, and better initial physiologic stabilization may reduce downstream deterioration and facilitate earlier recovery. This interpretation should be considered cautiously, but it is consistent with the broader possibility that gains in early workflow performance may extend beyond process metrics alone.
The overall pattern of findings is broadly consistent with previous trauma transfusion literature. PROMMTT highlighted the importance of timely plasma and platelet administration in massively transfused trauma patients, whereas PROPPR supported balanced component therapy as a core principle in severe trauma resuscitation.4,7 A previous Chinese before-and-after study of emergency transfusion workflow optimization reported shorter time to first transfusion, greater early plasma use, improved coagulation indices, and shorter ICU stay after process redesign. 9 The present study extends this line of evidence by suggesting that workflow gains may be further enhanced when activation begins in the prehospital phase rather than only after hospital arrival. This systems-oriented perspective is also consistent with recent civilian emergency medical services guidance, which frames prehospital transfusion as a coordinated regional resuscitation program requiring protocolized activation, training, quality oversight, and close integration with receiving hospitals and blood suppliers. 15
The absence of a statistically significant difference in in-hospital mortality should be interpreted with caution. Mortality after severe trauma is influenced by multiple factors beyond transfusion timeliness, including injury burden, traumatic brain injury, severity of shock, need for emergency surgery, definitive hemorrhage control, and overall trauma system capability. In before-and-after studies with moderate sample sizes, process measures and intermediate physiologic outcomes are often more sensitive to workflow change than mortality itself. Therefore, the lack of a statistically significant mortality signal in the present study does not negate the potential clinical importance of the observed improvements in transfusion timeliness, plasma delivery, coagulation-related indices, and ICU length of stay. This pattern is not inconsistent with recent prehospital transfusion evidence. In the RePHILL (Resuscitation with Prehospital Blood Products) randomized trial, prehospital PRBC plus lyophilized plasma was not superior to saline for the primary outcome in trauma-related hemorrhagic shock, whereas a more recent meta-analysis of randomized trials likewise did not demonstrate a clear overall mortality benefit for prehospital plasma-based strategies despite signals of physiologic or transfusion-related improvement in some secondary outcomes.16,17
The externally generalizable element of this study is likely the systems principle rather than the exact local workflow. Specifically, early identification of suspected life-threatening hemorrhage, structured pre-arrival notification, early blood bank activation, electronic transfusion ordering, and dedicated blood product delivery are workflow concepts that may be adaptable to other emergency and trauma systems. However, the magnitude of time reduction observed in this single-center study may not be directly generalizable because it depends on local ambulance communication infrastructure, blood bank organization, emergency department layout, staffing, and baseline transfusion delays. Therefore, the findings should be interpreted as supporting a transferable workflow concept rather than a universally reproducible effect size.
Several limitations should be acknowledged. First, the before-and-after design is inherently susceptible to temporal confounding. Changes over time in staff experience, trauma team coordination, transfusion service readiness, prehospital communication, ICU management, or institutional resources may have contributed to the observed differences independently of the integrated workflow. Second, the primary outcome was embedded in the intervention mechanism. Because the workflow was designed to move transfusion recognition and activation upstream, the reduction in time to first transfusion mainly reflects improved process efficiency and should not be interpreted as independent proof of clinical effectiveness. Third, although the same timestamp extraction rules were applied to both groups, the clinical context of the physician decision time differed between groups, which may have introduced non-equivalent starting-point bias. Fourth, exclusion of patients who died within 2 h of emergency department arrival may have introduced survivor bias by excluding the sickest hemorrhagic trauma patients, thereby limiting interpretation of mortality and other clinical outcomes. Fifth, formal prehospital transmission failure rates were not prospectively recorded during the study period and therefore could not be incorporated into the temporal adherence analysis. Sixth, the single-center design and moderate sample size limited generalizability and statistical power, especially for in-hospital mortality. Seventh, detailed temporal adherence data for individual workflow steps, including prehospital video transmission, electronic transfusion order submission, blood bank preparation, and dedicated blood delivery, were not systematically captured; therefore, this study evaluates the integrated workflow as a bundled process intervention and cannot identify which component contributed most strongly to the observed reduction in time to first transfusion. Finally, residual confounding related to definitive hemorrhage control and other concurrent management decisions could not be excluded. Future multicenter studies should use standardized time stamps, collect protocol-adherence data, include early deaths in sensitivity analyses when feasible, and adjust for both patient-level and system-level confounders.
Despite these limitations, the present findings have both practical and academic relevance. From a clinical perspective, they support the rationale for moving transfusion-related recognition, decision-making, and resource activation upstream in patients with suspected life-threatening traumatic hemorrhage. From a systems perspective, integrating prehospital recognition with early in-hospital transfusion preparation may represent a feasible strategy for improving early resuscitation efficiency in hospitals where prehospital-to-in-hospital coordination is not yet fully synchronized. Further multicenter studies are warranted to determine whether this approach can produce consistent improvements in patient-centered outcomes across different trauma care settings.
Conclusion
In this single-center observational before-and-after study, a prehospital-to-in-hospital integrated transfusion workflow was associated with shorter time to first transfusion, greater early plasma administration, more favorable coagulation-related indices at 24 h, and shorter ICU length of stay in patients with severe trauma requiring emergency transfusion. These findings mainly support improved workflow efficiency and suggest possible benefits for early hemostatic resuscitation processes. Because of the nonrandomized design, potential timestamp bias, survivor bias, and moderate sample size, these results should be considered hypothesis-generating. Multicenter studies with standardized workflow time points, protocol-adherence assessment, and stronger control of confounding are needed to determine whether this model improves patient-centered outcomes.
Supplemental Material
sj-docx-1-imr-10.1177_03000605261463827 - Supplemental material for Association of an integrated prehospital-to-in-hospital transfusion workflow with early outcomes in severe trauma requiring emergency transfusion: A single-center observational before-and-after study
Supplemental material, sj-docx-1-imr-10.1177_03000605261463827 for Association of an integrated prehospital-to-in-hospital transfusion workflow with early outcomes in severe trauma requiring emergency transfusion: A single-center observational before-and-after study by Huiping Zhou, Pengfei Xu, Yabin Chen, Weiting Chen and Chongjun Du in Journal of International Medical Research
Footnotes
Acknowledgments
The authors used Grammarly Premium and ChatGPT (OpenAI) only to assist with English language editing and grammar refinement. No artificial intelligence tool was used to generate, analyze, or interpret research data. The authors take full responsibility for the scientific content, data interpretation, and final wording of the manuscript.
Ethics approval and consent to participate
This single-center observational before-and-after study was conducted in accordance with the Declaration of Helsinki of 1975, as revised in 2024. The study protocol was reviewed and approved by the Institutional Review Board of the Linhai Second People’s Hospital, Taizhou, Zhejiang, China (approval no. 2024052101; approval date: January 2024). The requirement for informed consent was waived by the Institutional Review Board because of the observational nature of the study and the use of routinely collected clinical data. All patient data were de-identified before analysis.
Consent for publication
Not applicable.
Author contributions
Huiping Zhou and Chongjun Du conceived and designed the study, collected and analyzed the data, drafted the manuscript, and critically revised the manuscript. Pengfei Xu and Yabin Chen contributed to data collection, patient management, and manuscript revision. Weiting Chen analyzed the data. Chongjun Du supervised the study, contributed to interpretation of the data, and critically revised the manuscript. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Taizhou Science and Technology Program Project (grant number 24ywb137).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The de-identified datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request, subject to institutional and ethical approval requirements.
Preprint statement
This manuscript has not been posted as a preprint.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.