
Abstract
People with mirror-touch synaesthesia report tactile experiences on their body when seeing other people touched. Although this has been referred to as a type of synaesthesia, it is unknown whether it co-occurs with more commonly accepted variants of synaesthesia (e.g., grapheme-colour). If it did, then this would imply a common or partly shared causal mechanism. To this end, a sample of verified grapheme-colour synaesthetes (N = 80) were given a recently developed online diagnostic measure of mirror-touch. The prevalence in this group (∼20%) was around 10 times higher than the general population. Moreover, performance on this measure was significantly related to the self-report of mirror-touch given, on average, 3 years earlier.
Introduction
People with mirror-touch synaesthesia (MTS) report tactile sensations on their body when they observe other people being touched. However, whether it is related to more typical forms of synaesthesia such as grapheme-colour synaesthesia (experiencing colours for letters and numbers) is unknown. There are some reasons to believe that they might not be related. For instance, the mapping between inducing stimulus and synaesthetic experience is nonarbitrary in MTS (e.g., observed touch to face triggers felt touch to the face) but is far more idiosyncratic in grapheme-colour (Rothen & Meier, 2013). Also, whereas MTS has been explained in terms of a difficulty in attributing experiences to self versus other (Ward & Banissy, 2015), it is unclear how this explanation relates to other kinds of synaesthesia (Meier, Lunke, & Rothen, 2015).
There are, however, some reasons to expect that they may be related. Different types of developmental synaesthesia, in general, tend to co-occur both within individuals (synaesthetes often possess multiple types) and within families (such that any heritable component of synaesthesia does not specify how, exactly, it will be manifested; e.g., Barnett et al., 2008). One of the first case studies of MTS reported a familial history of other forms of synaesthesia (Blakemore, Bristow, Bird, Frith, & Ward, 2005), and in other well-publicised cases, both MTS and grapheme-colour are reported in the same individual (Salinas, 2017). One prevalence study has suggested that MTS does co-occur with other kinds of synaesthesia, although it used self-report of synaesthesia and hence is need of further investigation (Chun & Hupe, 2013).
The challenge for exploring whether these two types of synaesthesia co-occur more than expected by chance is that it involves studying the intersection of two rare symptoms. The prevalence of grapheme-colour synaesthesia is reported at 1.4% (Simner et al., 2006) and for MTS it is 1.6% (Banissy, Kadosh, Maus, Walsh, & Ward, 2009)—if they were fully independent then 1 in 4,464 people would have both types by chance. The approach taken here is to determine the presence of MTS amongst people with verified grapheme-colour synaesthesia (rather than the population as a whole). Whereas online screening tests have enabled remote testing for grapheme-colour synaesthesia (Eagleman, Kagan, Nelson, Sagaram, & Sarma, 2007), thereby enabling access to larger samples, comparable tests have not been available for MTS which, instead, has relied on in-person testing with visuo-tactile interference paradigms (Banissy & Ward, 2007). To address this, Ward, Schnakenberg, and Banissy (2018) reported a simple diagnostic measure for MTS. This was then compared, to provide external validity, to various objective tests (facial expression recognition, visuo-tactile interference) and subjective measures (empathy questionnaires) previously shown to be linked to MTS. The diagnostic test involves presenting video stimuli depicting touch in which the observer’s own phenomenology is reported. For instance, a report of touch would count as an instance of MTS whereas a report of itchiness would not. For the 14 stimuli presented, they recommended a cut-off of ≥7 instances of mirror-touch which corresponds, in a neurotypical sample, to a prevalence of 2.1% (Ward et al., 2018). The prevalence is similar to that noted before from lab-based assessments (Banissy et al., 2009), and this cut-off replicated previous findings on objective measures sensitive to MTS (e.g., Banissy et al., 2011).
In summary, the aim of this study is to explore the prevalence of MTS in a sample of verified synaesthetes (primarily grapheme-colour). A higher than expected prevalence is taken as indicative of a common causal mechanism.
Method
Participants
The sample consisted of 80 participants, with mean age of 34.313 years (SD = 10.110), and 9 men and 71 women. They had previously undertaken a test of grapheme-colour consistency (Eagleman et al., 2007) and had obtained scores below the suggested cut-off of 1.43 where lower scores are indicative of this form of synaesthesia (Rothen, Seth, Witzel, & Ward, 2013). These comprised of two different sub-samples recruited for somewhat different purposes. Sample 1 (N = 33) consisted of people who had previously declared MTS who were given the MTS test for confirmation purposes. Sample 2 consisted of a randomly selected sample of synaesthetes. Specifically, a representative sample of N = 201 synaesthetes were invited to take part (51/201 = 25.3% agreed to having MTS initially) and 47 of them completed the test. There was no evidence that people who initially claimed to have MTS were more likely to take the test (12/47 or 25.5% initially claimed to have MTS). Within our larger database, 23% of verified synaesthetes (N = 634) claim to experience MTS when shown a single movie exemplar (described in the next section).
Materials and Procedure
The main test involved the diagnostic measure of Ward et al. (2018). However, we also compared this against an initial question about MTS at the time the participants first contacted our research group. On volunteering to take part in synaesthesia research participants were given an online questionnaire (taking around 10 minutes) to self-report their synaesthesia. There was one item relating to MTS, in which participants saw a video clip depicting a male face being prodded on his left cheek with a finger. Specifically, they were asked: “Have a look at this clip: (http://www.youtube.com/watch?v=aoUdvuLrawE). Did you feel touch on your face in response to seeing this?.” From which they were given two options (Yes, No) and, for an affirmative response, were asked “On what side of your body did you feel it?” with three options (left face, right face, unsure). We also analysed responses to three control questions in an attempt to rule out a general acquiescence bias: that is, the people who said yes to having MTS may have a general inclination to say yes to any question put to them. Specifically, we examined the synaesthetes’ responses to three other screening questions. These were questions relating to the presence of sequence-space synaesthesia (“Some people always experience sequences in a particular spatial arrangement such as in these examples: Do you think this applies to you?” [yes/no]), tickertape synaesthesia (“When you hear someone speaking do you see the words spelled out?” [yes/no]), and hearing-motion synaesthesia (“Have a look at this clip: The moving dots are silent, but some people hear something when they see the dots move. Did you hear something?” [yes/no]). The first two questions were accompanied by a figure illustrating the experience, and the latter was the movie clip used to screen participants by Saenz and Koch (2008).
For this study, they were then given the more comprehensive measure of MTS (Ward et al., 2018). This test was conducted, on average, about 3 years after the participant had initially volunteered for research (average = 34.9 months, range = 5.4–87.6 months). The stimuli consisted of 14 movie clips depicting touch to humans, 6 depicting touch to objects/dummies, and 4 depicting scratching (the inanimate touch and scratching stimuli acted as fillers here). The 14 movie clips depicting touch to a human comprised of 7 pairs of stimuli depicting touch to either the left or right, namely, (a) touch to the cheek with a finger, (b) touch to the cheek with the tip of a knife, (c) touch to the hands in egocentric perspective with a finger, (d) touch to the hands in egocentric perspective with a knife, (e) touch to the hands in allocentric perspective with a finger, (f) touch to crossed hands in egocentric perspective with a finger and (g) touch to the cheek with a finger with face inverted. In all cases, the model was a Caucasian female and hands were palm down. After each video was played participants were asked: “Do you experience anything on YOUR body? (excluding feelings of unease, disgust or flinching) [Yes/No].” Upon an affirmative answer, they were asked three follow-up questions. First, they were asked “How would you describe the sensation?” and they were forced to choose one from the following checkbox options: Touch (without pain), Pain (without touch), Painful touch, Tingling, Itchiness, Feeling of being scratched and Other [Please specify__]. This question was designed to assess phenomenology but without guiding participants towards one particular desired answer. These questions are used to assess the presence of MTS. Subsequent questions, not analysed here, ask about the location of the experience and its intensity.
Results
Following Ward et al. (2018), MTS was indicated by 7 or more (/14) tactile responses to seeing a human touched: A tactile response includes the responses touch (without pain), painful touch and feeling of being scratched. Of the 80 synaesthetes who took the MTS test, 25% (20/80) were classified as having MTS using this method. In Sample 1, the prevalence rate was 11/33 or 33%. In Sample 2 (unbiased), the prevalence of people with MTS in the sample was 9/47 or 19.1%. These figures contrast with a general population prevalence rate, using the same stimuli and cut-off criteria, of 2.1%, N = 283 from Ward et al., 2018; χ2(1) = 49.101, p < .001. Thus, MTS is around 10 times more prevalent in people with more canonical types of synaesthesia.
The classification of MTS synaesthetes (using the more comprehensive test) relative to the initial screening question is shown in Table 1. There is a significant association between performance on the two measures, χ2(1)=10.476, p = .001, despite the tests being different (single item vs. multiple items) and despite the long elapsed time between them (∼3 years on average). However, it is rather asymmetrical. Few participants who initially failed to report MTS were subsequently shown to have it. But, by contrast, many participants who initially declared having MTS were subsequently classified as not having it. This is in line with previous research. For instance, Banissy et al. (2009) found that ∼10% of nonsynaesthetic participants agreed to having MTS on a single written question with 1.6% passing a laboratory test.
Frequency Distribution of Grapheme-Colour Synaesthetes According to Whether They Initially Reported MTS (Based on a Single Item) and Whether They Subsequently Passed a Diagnostic Measure (Based on Multiple Items).
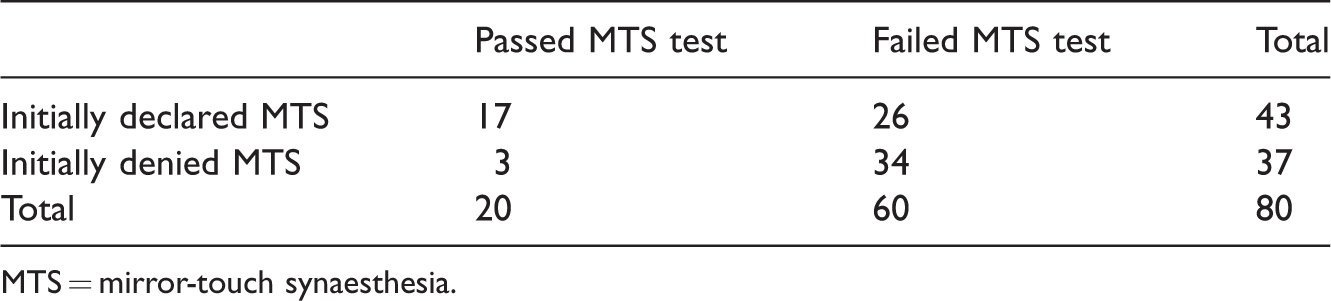
MTS = mirror-touch synaesthesia.
Figure 1 shows the exact scores on the MTS screener (from 14 stimuli) broken down according to their initial report of touch to a single stimulus (yes vs. no). Those who had initially said yes typically also gave an affirmative answer on at least one occasion when subsequently tested in more detail (70% of them), whereas the majority of people who had previously said no never reported a single tactile response (78%). Nonparametric analyses show that the two distributions differ (Mann–Whitney U = 363, Z = 4.51, p < .001).
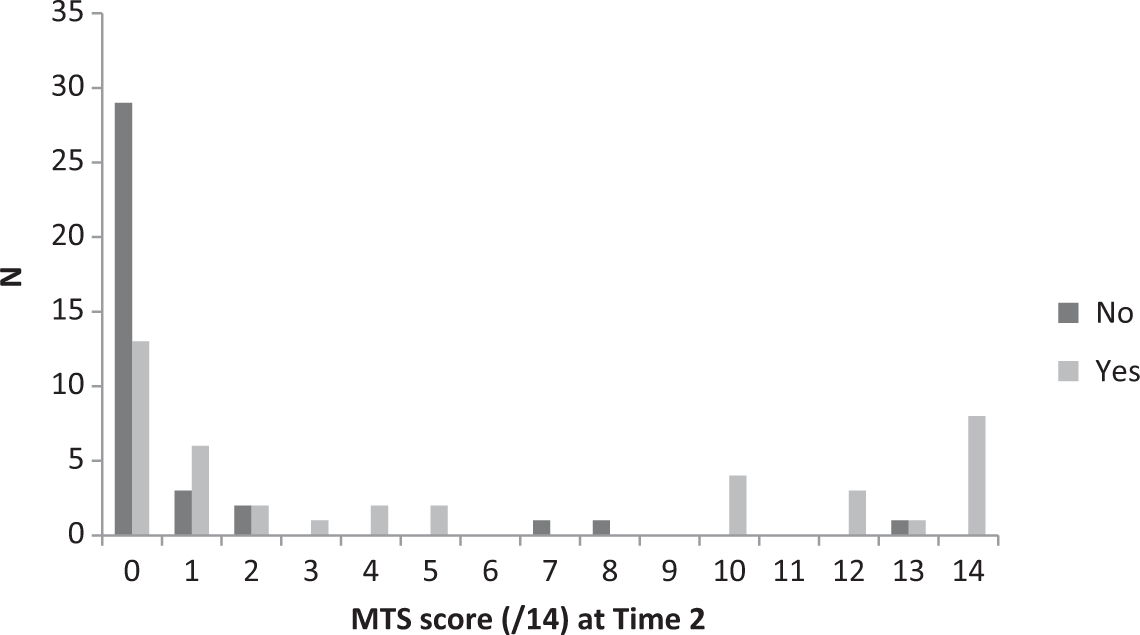
The distribution of MTS responses (declaring a tactile sensation when seeing a human touched) according to whether they had previously reported a tactile sensation (yes/no) when probed with a single item around 3 years earlier.
Ward et al. (2018) reported that people with MTS also have unusual responses on some of the other trials (i.e., independently of the trials used to diagnose MTS itself). For stimuli depicting itchiness, the modal response is for observers to report itchiness themselves, but people with MTS are more likely to report these stimuli as eliciting touch (i.e., they are not merely saying what they see). The same pattern was noted here. Collectively, people with MTS (N = 20) reported 20 touch sensations and 13 itch sensations, whereas the non-MTS group (N = 60) reported 16 touch sensations and 57 itch sensations. People with MTS also report tactile sensations when seeing dummies or objects touched but such reports are less frequent and less intense than when seeing touch to a human. The number of tactile responses reported to the dummy/object stimuli (mean = 52%, SD =39.0) was significantly lower than for humans, mean = 85%, SD = 16.7; t(19) = 3.913, p < .001.
Finally, synaesthetes classed as MTS did not show a tendency to give affirmative answers more than the other synaesthetes in the control questions. For sequence-space, tickertape, and hearing-motion, the levels of yes/no responding between groups did not differ, χ2(1) = 2.215, 0.883, and 0.640 and p = .137, .347, and .424. The levels of agreement for the N = 20 MTS group were 70%, 45%, and 45%, and for the N = 60 non-MTS group were 85%, 33%, and 35%. It is noteworthy that two of the MTS group who agreed to hearing-motion qualified their response by saying “I couldn’t hear it I could feel it” and “I actually feel it more than everything else. It’s soft and ‘massaging’.”
Discussion
This study shows for the first time that MTS is around 10 times more prevalent in people with grapheme-colour synaesthesia than estimates from the general population. This research is possible because of the development of an online diagnostic tool that has previously been shown to be sensitive to objective measures of MTS (Ward et al., 2018) which enables sufficiently large numbers of people with synaesthesia to be tested. This is unlikely to reflect a simple response bias (i.e., to give affirmative responses whether they are valid or not). Synaesthetes with MTS did not give more affirmative responses to control questions about other kinds of synaesthesia, and showed a different pattern to control stimuli (depicting itch or touch to inanimate objects). Moreover, they are relatively consistent in claiming to have MTS over a long period and the fact that this sample has another verified type of synaesthesia shows that their subjective reports are, in other respects, reliable.
The findings are consistent with Chun and Hupe (2013) who found that MTS tended to be reported more in people with other kinds of synaesthesia (including grapheme-colour, sequence-space, sound-colour). They did not use a verified measure of synaesthesia but, instead, a single question item (as indeed we did in our initial screening questionnaire). Although a single question measure is generally poor, it nevertheless captures something of relevance: It is likely to be imprecise rather than meaningless and so require larger samples to detect significant associations.
The question of why these kinds of synaesthesia are related in terms of causal mechanisms is far less clear. For instance, grapheme-colour synaesthesia is often accounted for in terms of exuberant connectivity between adjacent regions, but it is less clear that this account is appropriate for MTS (or indeed other kinds such as music-colour). MTS has been explained in terms of self-other confusion in which perceived bodily sensations are misattributed to one’s own body (Ward & Banissy, 2015). This does not have an obvious parallel in terms of grapheme-colour. The Threshold Theory of MTS claims that synaesthetic experiences are conscious versions of normally implicit multi-sensory processes (Ward & Banissy, 2015), and such an account could be extended to synaesthesia more generally (for discussion, see Deroy & Spence, 2016). Other theories that bridge the gap are predictive processing accounts. These have been suggested for both MTS (Ishida, Suzuki, & Grandi, 2015; Ognibene & Giglia, 2015) and grapheme-colour (Seth, 2014) and in which unusual experiences can arise because of differences in weighting between sensory evidence and internal models (termed priors). A prior might consist of an assumption or top-down knowledge, for instance, along the lines of “that’s my body” or “the letter A is red.” In predictive processing frameworks, internal models get updated in light of new sensory evidence but it has been argued that some people have stronger (or less flexible) priors and, for these people, the perceptual experience is updated to match the model. This gives rise to an illusory experience.
Finally, both mirror-touch and other forms of synaesthesia might share underlying latent variables that predispose towards these kinds of unusual phenomena. For instance, having vivid mental imagery may be a prerequisite for being able to experience vicarious tactile sensations (in MTS) or colourful images (in grapheme-colour). Synaesthetes report more vivid mental imagery across multiple senses (Spiller, Jonas, Simner, & Jansari, 2015).
In summary, MTS is linked to other kinds of synaesthesia and further research is needed to understand the nature of that link.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.