
Abstract
Autonomous sensory meridian response (ASMR) is a phenomenon characterised by a static-like tingling sensation spreading from the scalp and neck to the periphery in response to a variety of audio, visual, and tactile triggers resulting in a highly relaxed state and boosted positive affect. The limited literature on this phenomenon points to a potential of ASMR to alleviate pain. Emerging evidence also suggests that ASMR may be linked to increased sensory sensitivity more broadly. This study aimed to objectively address these claims by administering an algometer (measure of pain tolerance), and a visual analog scale (VAS) (measure of subjective pain sensitivity) to ASMR experiencers and controls at baseline, following an ASMR video, and a control video. Findings indicate that ASMR experiencers have a higher pain sensitivity than controls; however, there was no difference between the two groups in terms of pain tolerance. In addition, any potential analgesic properties associated with experiencing ASMR may reflect protective properties of ASMR buffering against the increased pain sensitivity among ASMR experiencers relative to controls.
Introduction
Autonomous sensory meridian response (ASMR) is a complex sensory and affective phenomenon in which individuals experience a pleasant and relaxing tingling sensation usually felt on the scalp and back of the neck, but also throughout the body in response to specific triggering audio, visual, and tactile stimuli such as whisper, personal attention, and hair brushing (Barratt & Davis, 2015; Janik McErlean & Banissy, 2017). The exact prevalence of ASMR is not known, although previous research has found that 47% of participants recruited among university students identified as ASMR experiencers (Janik McErlean & Banissy, 2018), suggesting that ASMR is likely to be relatively common, although broader population research using stricter verification methods is needed to establish the exact prevalence of this phenomenon. Although the sensation can be experienced in day-to-day life, in recent years many YouTube channels dedicated to producing ASMR content have become popular, further suggesting that the phenomenon is widespread (e.g., Gibi ASMR has over 3 million subscribers and over 1 billion views). Those individuals who are capable of experiencing ASMR watch such videos to promote relaxation and sleep, and in some cases to relieve depression, anxiety, stress, and even chronic pain (Barratt & Davis, 2015; Janik McErlean & Banissy, 2017).
With regards to empirical evidence, Barratt and Davis (2015) found ASMR to lead to a temporary reduction in depressive mood. Specifically, these authors found that when ASMR experiencers were asked about the effect of technologically induced ASMR on their mood, 80% of them reported it to be positive. They also found that this effect was most pronounced while engaging with ASMR content and that it dissipated with time. They also found that people scoring higher on the depressive symptoms reported the greatest boost to their mood but this effect did not last as long as for the individuals with lower levels of depression.
Other studies have also reported ASMR to have a positive impact on emotional states. Poerio et al. (2018) found across two studies that watching ASMR videos resulted in increased excitement and calmness in individuals who identified as ASMR experiencers compared to controls. Their first study also found that relative to the individuals who do not experience ASMR, ASMR group reported increased connectedness and concomitant reduction in stress and sadness in response to ASMR videos; however, this finding was not replicated in study 2. Importantly, the association between ASMR and boosted positive affect was also corroborated by physiological evidence in this study which showed that experiencing ASMR was accompanied by a reduction in heart rate and increased skin conductance, further demonstrating beneficial properties of ASMR which is both a stimulating and relaxing phenomenon with a distinct physiological signature.
Barratt and Davis (2015) also investigated the impact of ASMR on chronic pain and found that 42% of their sample of 91 ASMR experiencers with chronic pain reported a positive impact of experiencing ASMR on their symptoms. They also found that this positive effect lasted for several hours after experiencing the sensation. While these results are promising, as they are based on self-reports and are solely focused on chronic pain symptoms, a more systematic investigation of these potential therapeutic benefits of experiencing ASMR on pain perception is needed which is one of the aims of this study.
Although the exact mechanisms of ASMR are not known, converging evidence suggests that the propensity to experience ASMR and its potential mood lifting and analgesic benefits as suggested by the preliminary aforementioned findings may be underlined by increased sensory sensitivity and unusual integration of sensory and affective processes. For example, ASMR has been associated with increased self-reported sensory processing sensitivity (Poerio et al., 2022; Roberts et al., 2020) and with increased transliminality (Roberts et al., 2021), which pertains to ease with which external stimuli enter consciousness, which in turn, has been associated with heightened sensory experiences and with fantasy proneness and absorption (Lange et al., 2000; Sherwood & Milner, 2005; Thalbourne, 1996) both of which are elevated in ASMR experiencers (Janik McErlean & Banissy, 2017; Janik McErlean & Osborne-Ford, 2020). It is of note that while these findings point to a possibility that ASMR may be associated with increased sensory sensitivity no study to date has examined this claim objectively.
Moreover, ASMR has been linked to increased levels of misophonia (Del Campo, 2019; Janik McErlean & Banissy, 2018) which is a sensitivity to human-generated sounds such as whispering or tapping, which are also common ASMR triggers but result in aversive emotional, physiological and behavioural outcomes in misophonia (Jastreboff & Jastreboff, 2002). Even though the two phenomena appear to be polar opposites, the fact that ASMR is associated with elevated levels of misophonia suggests not only that they can coexist in the same individuals but also that ASMR appears to be characterised by enhanced sound sensitivity more broadly, and that this can have both positive and negative outcomes (Janik McErlean & Banissy, 2018). Interestingly, Rouw and Erfanian (2018) also found a high prevalence of ASMR in misophonia, which further supports the notion that the two phenomena are comorbid and supports the suggestion that ASMR is linked to sensory sensitivity in this instance within the auditory modality, although this needs to be further verified with objective measures.
Further evidence pointing to increased sensory sensitivity in ASMR comes from neuroimaging research. For example, ASMR has been associated with heightened activity within the somatosensory, visual, and auditory cortices and within the thalamus, which is involved in processing signals within all these sensory modalities (Smith et al., 2019). This is also in line with research showing atypical functional connectivity in ASMR experiencers within the thalamus and between the frontal regions and brain areas implicated in sensory processing and attentional control, which is likely to reflect altered integration of sensory input and reduced ability to suppress sensory-emotional associations (Smith et al., 2017). Additionally, ASMR experiencers have shown increased activity within the anterior cingulate cortex and insula (Lochte et al., 2018) which are also implicated in pain perception (Lieberman & Eisenberger, 2015; Segerdahl et al., 2015) interoception (Garfinkel & Critchley, 2013), and emotion processing (Lindquist et al., 2012) suggesting that these processes may also be altered in ASMR. Interestingly, recent self-report findings also suggest increased bodily awareness and interoceptive sensitivity among ASMR experiencers relative to controls (Poerio et al., 2022). ASMR has also been linked with enhanced activity within the alpha frequency range within the frontal regions which has also been suggested to underpin the altered attentional processes in ASMR (Fredborg et al., 2021). While current evidence may suggest heightened sensitivity to exteroceptive input within tactile, auditory, and visual modalities, but also potentially to signals coming from within one's body, no study to date has examined this directly. As such, any potential differences in sensory sensitivity among ASMR experiencers remain to be established.
In summary, based on the existing findings pointing to the positive impact of ASMR on pain perception, this study aimed to further evaluate this possibility directly by administering an algometer, as a measure of pain tolerance, and a visual analog scale (VAS) as a measure of subjective pain sensitivity, to a group of ASMR experiencers and controls at baseline, while watching an ASMR video, and a control video. In addition, in light of the literature suggesting enhanced sensory sensitivity in ASMR this research also wanted to establish whether this applies to the tactile domain by comparing pain tolerance and subjective pain ratings between ASMR experiencers and controls. It should be noted here that pain perception and tactile sensitivity are two distinct but related concepts. Consistent evidence has shown that factors that influence one tend to influence the other (as in Zamorano et al., 2015; and Bueno et al., 2018), and Gracely (1999) has suggested that tactile sensitivity modulates pain perception to some degree, although the two are not directly analogous. Pain tolerance/sensitivity therefore represent a potentially interesting area for further examination in regards to ASMR responding, which this paper will explore.
As such, the two primary research aims were to (i) examine whether there is an overall difference in pain tolerance and subjective pain perception between ASMR experiencers and controls and (ii) whether ASMR experiencers would show lower subjective pain ratings and/ or increased pain tolerance in the ASMR video condition compared to the control video and no video condition, which would suggest potential analgesic properties associated with experiencing ASMR.
Method
Participants
A total of 20 undergraduate students were recruited on a volunteer basis and university credits were offered to first-year psychology students. Participants were asked to indicate whether they classify themselves as controls or ASMR experiencers based on the following description of the phenomenon: “ASMR can be defined as a pleasurable tingling sensation which typically originates on the scalp and spreads down the spine and through the whole body which is typically induced by certain sounds (e.g. turning pages, crinkly wrapping paper, finger tapping, people whispering), watching someone perform repetitive mundane actions (e.g., folding towels, going through items in a handbag), watching someone closely inspecting day-to-day objects, watching someone's hair being brushed or watching videos with various role plays (visit a doctor, spa or a shop). ASMR is not frisson (e.g., ‘goosebumps’ when listening to music)” (as per Janik McErlean & Banissy, 2017).
To further verify that participants in the ASMR group were genuine ASMR experiencers, they were provided with a list of common ASMR triggers including crisp sounds (tapping/crinkling), personal attention, whispering, role-plays (e.g., visit to a hairdresser, spa, and doctor), hair brushing, paying attention to detail, slowly performing mundane actions or explaining something, or concentrating on something, people eating, other) and asked to select all the items that trigger their ASMR while viewing ASMR videos or in daily life. They also had an option to list other triggers not included on the list. They were also asked to indicate the intensity of their ASMR on a scale from 0 to 6 (0 = “no tingles”; 6 = “most intense ASMR experience”) in response to these triggers (as per Fredborg et al., 2018). This was done to ensure that those individuals who would not list any of the popular or any other triggers or chose 0—no tingles for all the common ASMR triggers listed, would not be classified as ASMR experiencers. No such cases were encountered. In addition, ASMR experiencers in this study rated the tingle intensity to be the highest for whispering and hair brushing (both: M = 2.91) followed by crisp sounds (M = 2.54), people eating (M = 2.00), role-plays (M = 1.91), paying attention to detail, concentrating on something, slowly performing mundane actions or explaining something (M = 1.18), and lastly personal attention (M = 0.55).
One participant was removed from the data set due to extreme scores (SD > 2.5) on a number of variables. This resulted in the final sample size N = 19 (ASMR = 11, Control = 8). The groups did not differ in terms of age (ASMR: M = 22.09, SD = 4.06; Controls: M = 21, SD = 2.44, t(17) = .67, p = .51) or gender (ASMR: F = 11, M = 0, Controls: F = 5, M = 3; Fisher's Exact Test p = .058). A priori power analysis suggested a sample size of 28 for a mixed ANOVA to obtain
Materials
Stimuli
The two video clips used in this experiment included (a) an ASMR video which consisted of a hairdressing scenario and (b) a control video which consisted of a close-up vegetable peeling tutorial. The videos were both clipped to three minutes in length as this amount of time allowed for at least three triggers in the ASMR video (personal attention, hair cutting, washing, slow deliberate expert hand movements, soft sounds, and crisp sounds) and at least three trigger-like stimuli in the control video (viewer centred perspective, giving instructions, repetitive hand movements, close-ups of the performed actions, and peeling and slicing of vegetables). Both videos were sourced from YouTube and were selected by the experimenter who is an ASMR experiencer. The ASMR video was chosen as it was filmed in an ASMR style and contained multiple different ASMR triggers which increased the chance of participants experiencing ASMR. The control video was chosen as it mimicked the ASMR videos (e.g., was filmed close-up, the people in the video were facing the viewer, also doing repetitive motions with their hands). However, the video did not contain typical ASMR triggers. For example, the people in the control video did not whisper or use soft speaking which are commonly used in ASMR videos, they were not smooth with their hand movements and as such it could be expected that this video would be less likely to trigger ASMR.
Measures
Pain Induction
Pain Tolerance
Pain induction was carried out using a manual algometer (Wagner Instruments FPX series), which induced pain through the application of pressure to the soft tissue of the dorsal forearm, close to the elbow joint, through a 1cm2 rubber surface, as per Edwards et al. (2017). An algometer is a highly reliable device used to measure the pressure or force (ft/lbs) which produces an objective pressure pain tolerance score that can be used multiple times in one session without carry-over effects in measurement between each condition (Kinser et al., 2009).
During the pain induction procedure, the algometer was applied to the soft tissue of the dorsal forearm, approximately 8cm from the elbow joint. During induction, participants were asked to verbally report the point at which the pressure was no longer tolerable— this is called pain tolerance. At each induction, three algometer measurements were taken, with the average of the three recorded as the participant's pain tolerance; this reduced measurement error. In order to control for any potential fatigue or increased sensitivity, the location of the induction site was moved slightly, although it always remained within 8cm of the elbow joint on the dorsal forearm of the same side. The non-dominant side was used at all times, as previous evidence has suggested variation in pain sensitivity on dominant versus non-dominant sides during pain induction (see Zhang et al., 2021).
Pain Sensitivity
A VAS was administered after each video/algometer session to obtain subjective pain ratings. The VAS is a reliable measure of pain perception that relies on a visual scale and has been used in numerous pain studies (Bijur et al., 2001; Hawker et al., 2011). The VAS was analysed using a ruler, and the score was determined by measuring the distance (mm) on the 10-cm line between the “no pain” anchor and the participant's mark, providing a range of scores from 0 to 100, which is more sensitive than a simple descriptive ordinal scale. A higher score indicates greater pain intensity.
Tingle Frequency
Participants were also asked to report how often they felt tingles on a scale from 1 to 7 (1 = “none of the time”; 7 = “all of the time”) in the baseline condition and after both the ASMR and control videos. The tingle frequency reported from this scale established whether participants experienced ASMR in response to the videos used in this study.
Procedure
All participants were provided with an Information Sheet and asked to provide an electronic consent prior to participation. Subsequently, each participant filled out the online ASMR survey which confirmed whether they were or were not an ASMR experiencer. Subsequently, we used an algometer to obtain a measure of pain tolerance. Algometer was pressed three times at specific times during each condition against participants’ forearms. This was timed with specific triggers occurring in the ASMR video, and was kept consistent in all conditions. Participants were asked to verbally indicate when they could not tolerate the pressure/pain anymore and the application of the algometer was immediately stopped and the tolerance value recorded. The three pain tolerance readings were used to calculate an average score for each condition. In the ASMR and control video conditions, this was done continuously with the presentation of the videos, that is the videos were not stopped as this could potentially disrupt the ASMR experience. At the end of each condition (baseline, ASMR, and control) participants rated how painful the pressure from the algometer was on the VAS scale and also rated their tingle frequency. As such, we obtained a subjective pain rating measured with the VAS and an objective pain measure using the algometer. Everyone completed the baseline condition first. Subsequently, the participants watched the control and ASMR video, the order of which was counterbalanced. This study was approved by the Ethics Reviewer Panel at Bath Spa University.
Design and Analytical Approach
The purpose of this study was to establish whether participants who identify as ASMR experiencers would show differences in terms of the three dependent variables (tingle frequency, pain tolerance indexed by algometer scores, and VAS as a self-report measure of pain) after watching an ASMR video when compared to a control video and no video and relative to control participants. To this effect a repeated measures experimental design was implemented and a series of 2 (group: ASMR experiencers, controls) × 3 (video type: ASMR, control, no video) ANOVAs were conducted.
Data Availability Statement
The data collected as part of this project can be accessed on the OSF page: https://osf.io/a2f35/.
Results
Tingle Frequency
First, in order to test whether ASMR experiencers experienced ASMR in response to the videos in this study and whether their responses differed to those of controls a 2 (group: ASMR experiencers, controls) × 3 (video type: ASMR, control, no video) ANOVA was conducted on the tingle frequency. This revealed a significant group × video-type interaction F(2, 34) = 4.29, p = .022, ηp2 = .20. Three post hoc independent samples t-tests with Bonferroni correction (p < .01) were conducted to compare the groups across the three conditions. This indicated that the only significant group difference was in response to the ASMR video in which ASMR experiencers reported higher tingle frequency relative to controls, t(17) = 3.23, p = .005, d = 1.59, Mdiff = 2.09, 95% CI = [.72, 3.45]. A significant main effect of group was also observed F(1, 17) = 9.44, p = .007, ηp2 = .36 with ASMR experiencers scoring higher than controls (Mdiff = 1.28, 95% CI = [.40, 2.17], p = .007). There was also a significant main effect of video type F(2, 34) = 18.35, p < .000, ηp2 = .52. Inspection of Bonferroni corrected pairwise comparisons indicated that tingle frequency was significantly lower at baseline compared to the control video (Mdiff = 1.11, 95% CI = [.29, 1.93], p = .007, d = −0.84) and compared to the ASMR video (Mdiff = 1.90, 95% CI = [1.04, 2.77], p < .001, d = −1.25], which overall had the highest tingle frequency rating, although, the difference between the ASMR and control videos only approached significance (Mdiff = .79, 95% CI = [ −.03, 1.62], p = .064, d = 0.63) (Table 1).
M(SD) for group and tingle frequency.
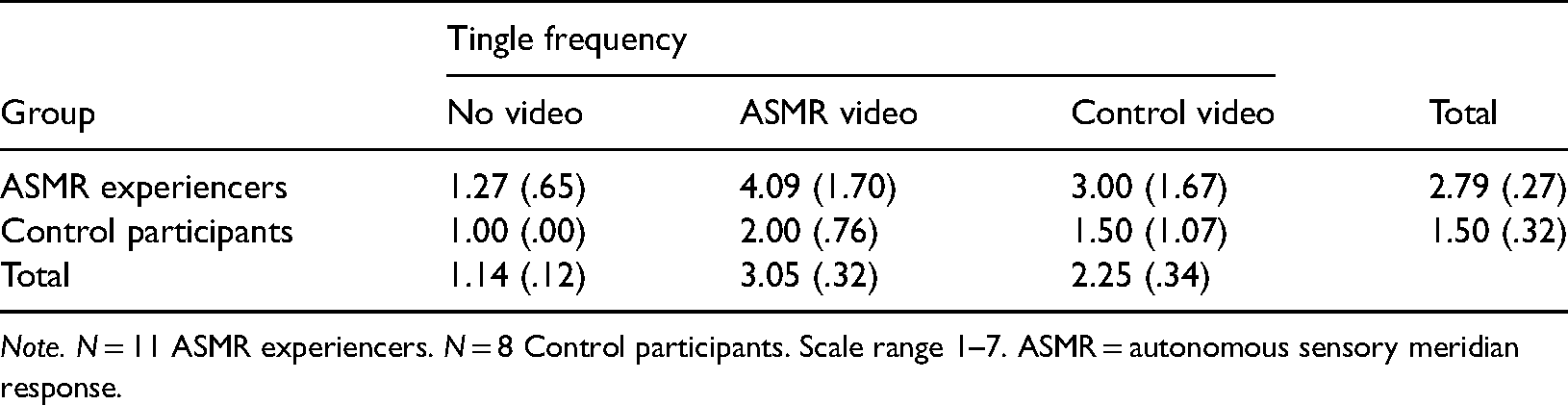
Note. N = 11 ASMR experiencers. N = 8 Control participants. Scale range 1–7. ASMR = autonomous sensory meridian response.
VAS Pain Scores
The second 2 (group: ASMR experiencers, controls) × 3 (video type: ASMR, control, no video) ANOVA was conducted on the VAS scores which measured the subjective pain level experienced in each condition. This revealed a significant main effect of group (F(1, 17) = 4.74, p = .04, ηp2 = .22) with ASMR -experiencers reporting more pain than controls (Mdiff = 1.39, CI[.043, 2.75], p = .04). The main effect of video type (F(2, 34) = 1.35, p = .27, ηp2 = .07), and the interaction between group and video type (F(2, 34) = .01, p = .99, ηp2 = .001) were both statistically non-significant (see Table 2 for descriptive results).
M(SD) for ASMR status and VAS scores.
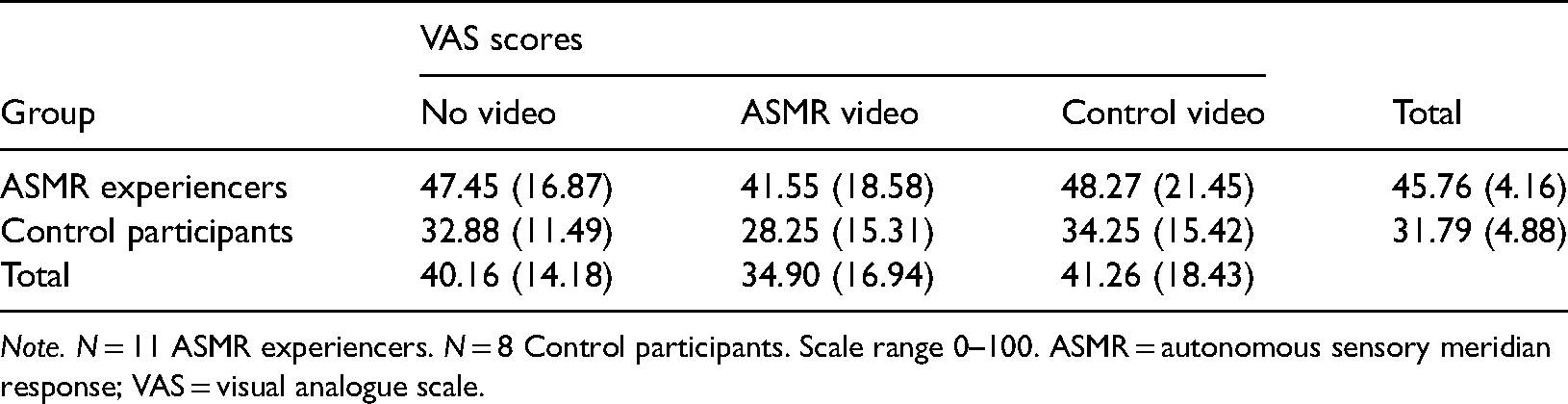
Note. N = 11 ASMR experiencers. N = 8 Control participants. Scale range 0–100. ASMR = autonomous sensory meridian response; VAS = visual analogue scale.
Algometer
The third 2 (group: ASMR experiencers, controls) × 3 (video type: ASMR, control, no video) ANOVA was conducted on algometer scores which measured pain tolerance. ASMR experiencers had a lower algometer tolerance overall (M = 12.68, SD = 2.04) compared to controls (M = 19.01, SD = 2.39), although, this effect was non-significant (F(1,17) = 4.05, p = .06, ηp2 = .19). The interaction between group and video type was also non-significant F(2, 34) = 2.56, p = .09, ηp2 = .13. There was a significant main effect of video type (F(2, 34) = 11.66, p < .001, ηp2 = .41). Inspection of Bonferroni corrected pairwise comparisons indicated that algometer scores were significantly lower at baseline compared to ASMR video (Mdiff = 2.61, CI [1.13, 4.09], p = .001, d = −1.07) and compared to the control video (Mdiff = 2.20, CI [ .35, 4.04], p = .017, d = −0.62). However, there was no significant difference in algometer scores between ASMR and control videos overall (Mdiff = .417, CI [−.83, 1.67], p = 1.00, d = 0.26). Interestingly ASMR experiencers had the highest algometer score (pain tolerance) when viewing the ASMR video, while the controls had the highest pain tolerance in response to the control video (Table 3).
M(SD) for ASMR status and algometer scores.

Note. N = 11 ASMR experiencers. N = 8 Control participants. Scale range 0–50. ASMR = autonomous sensory meridian response.
Discussion
In light of several lines of evidence suggesting there may be increased sensory sensitivity in ASMR (Poerio et al., 2022; Roberts et al., 2020; Smith et al., 2019) this study sought to establish whether ASMR experiencers compared to controls show enhanced sensitivity within the tactile domain, by administering an established lab-based pain induction procedure using an algometer and the VAS. Based on the existing self-reports of beneficial impact of ASMR on chronic pain symptoms (Barratt & Davis, 2015) this study also aimed to evaluate whether experiencing ASMR concurrently with the application of the algometer would lead to reduced pain perception/increased pain tolerance among ASMR experiencers relative to controls and compared to the baseline and control conditions.
The results of this study show that ASMR is indeed associated with increased sensitivity to exteroceptive nociceptive tactile stimulation as evidenced by greater self-reported intensity of the experienced pain resulting from the administration of the algometer, although our results also show that ASMR experiencers’ pain tolerance did not differ significantly from controls. This shows that while objectively defined pain tolerance was uniform in both ASMR responders and controls, ASMR responders rated the pain as being more intense. Overall, these findings are in line with fMRI results showing that experiencing ASMR is linked with increased activity within the brain regions implicated in somatosensation and pain perception (Lochte et al., 2018; Smith et al., 2019). They also fit more widely with evidence of general self-reported increased sensory sensitivity (Janik McErlean & Banissy, 2018; Poerio et al., 2022; Roberts et al., 2020; Smith et al., 2019) and transliminality (Roberts et al., 2021) in ASMR experiencers. As this is the first study to objectively measure sensory sensitivity in any modality among the ASMR experiencers it is essential to examine whether this extends beyond the tactile domain. It is possible that, similarly to synaesthesia, heightened sensory sensitivity may only be present within the concurrent (i.e., tactile) modality. Specifically, synaesthesia has been linked to enhanced sensory processing within the modality of the synaesthetic experiences (e.g., superior colour processing in grapheme-colour synaesthesia and enhanced tactile acuity in mirror-touch synaesthesia; Banissy et al., 2009). At the same time, initial findings suggest there may be an increased incidence of synaesthesia among ASMR experiencers. Specifically, Barratt and Davis (2015) reported the prevalence of synaesthesia in their ASMR group to be 5.9% which is higher than that of the general population (4.4%, Simner et al., 2006), but this finding was not statistically significant and as such wider research is needed to further investigate this claim.
Moreover, both conditions appear to rely on similar inducer-concurrent mechanisms and both have been linked to atypical neural connectivity (Dovern et al., 2012; Schweizer et al., 2013; Smith et al., 2017), and a similar personality profile (Banissy et al., 2013; Chun & Hupe, 2016; Rouw & Scholte, 2016). At the same time, neuroimaging research (Lochte et al., 2018; Smith et al., 2019) and findings based on self-reports (Janik McErlean & Banissy, 2018; Poerio et al., 2022; Roberts et al., 2020) suggest that ASMR may be characterised by heightened sensitivity within several sensory modalities. As such, further research using objective measures is needed to establish whether sensory sensitivity among ASMR experiencers is domain specific or domain general, as this would shed more light on the mechanisms underpinning the conscious ASMR experiences and its wider phenotype. It also remains to be established whether ASMR is associated with increased sensitivity to non-painful tactile stimulation. Considering that pleasurable tingling is the signature of ASMR it is expected that this would be the case. If confirmed, this would fit with the existing findings showing that heightened sensitivity to exteroceptive stimulation can lead to drastically different outcomes. Specifically, sensitivity to sound has been found to lead both to positive and negative responses in those individuals who experience ASMR and misophonia (Janik McErlean & Banissy, 2018).
Current findings also show that descriptively ASMR experiencers showed the highest pain tolerance and the lowest reported level of pain when watching ASMR videos, which is when they also reported the highest frequency of ASMR tingles relative to the baseline and control conditions. This may suggest that experiencing ASMR may lead to a temporary reduction in pain perception in ASMR experiencers, which is in line with prior findings of beneficial properties of ASMR in terms of pain reduction among ASMR experiences with chronic pain (Barratt & Davis, 2015). A likely mechanism for this is parasympathetic activation of the autonomic nervous system (ANS) by ASMR, as described by McGeoch and Rouw (2020), who propose that ASMR can increase vagal tone through parasympathetic activation. More established methods of reducing pain, such as deep breathing (see Busch et al., 2012), have a similar parasympathetic activation profile, and it is likely that ASMR influences pain in a similar way. However, it should be noted that this study did not directly measure ANS activity, and as such this is currently quite speculative. Future research should focus on further exploring this as a potential mechanism for the effect of ASMR on pain perception.
At the same time, it appears that control participants also experienced a reduction in pain perception when watching the ASMR video compared to the baseline and the control video, although this was not as pronounced as in the ASMR group and overall there was no statistically significant main effect of video type. Nevertheless, these results may point to a possibility that ASMR videos might also be beneficial to some extent for individuals who do not experience ASMR at least in terms of the subjective pain ratings as controls had the highest pain tolerance in response to the control video. Perhaps it is the caring nature of the ASMR video used in this study, which included personal attention, gentle hand movements, and low pitch sounds that contributed to this effect, potentially by eliciting a sense of calm. However, as we did not ask participants about the impact, the videos used in this study had on them beyond the tingling sensation this is only speculation and requires further exploration in future research. In addition, as Barratt and Davis (2015) did not examine the impact of ASMR videos on control participants and only included ASMR experiencers with chronic pain in their study it is essential to further explore the potential analgesic properties of ASMR content on individuals with chronic pain who do not experience ASMR.
It is of note, that our data collection was disrupted by the COVID-19 pandemic, resulting in a small sample size, thus, current results should be treated with some caution. While effect sizes observed suggest that this did not overly influence results, the findings reported here should be considered preliminary and it is essential to conduct more research with a larger sample to firmly establish whether experiencing ASMR can reduce pain perception. If this is confirmed this would be in line with the findings of elevated absorption among ASMR experiencers, which reflects a propensity to become immersed with the current experience and a concurrent loss of self-awareness (Janik McErlean & Osborne-Ford, 2020), and which has been shown to facilitate pain reduction, for example, by means of immersive virtual reality games (Dahlquist et al., 2007; Jameson et al., 2011). As such, reduced pain perception following ASMR induction in ASMR experiencers could be a result of one's attention being absorbed by the salient ASMR triggers and diverted away from the experienced physical discomfort. This suggestion is also supported by the neuroimaging findings which implicate potentially altered attentional control and emotional responses in ASMR experiences evidenced by increased activity within the dorsal anterior cingulate cortex (Lochte et al., 2018; Smith et al., 2019), atypical functional connectivity between the frontal lobe and brain regions involved in sensory processing and attention (Smith et al., 2017), and increased activity within the frontal alpha power (Fredborg et al., 2021). Moreover, increased activity has been reported in nucleus accumbens (Lochte et al., 2018) implicated in reward (Blood & Zatorre, 2001) and in areas involved in emotional arousal (dACC, insula: Lochte et al., 2018; Smith et al., 2019). As such, if the analgesic effect of experiencing ASMR is confirmed this may reflect the capturing of attention by ASMR triggers which may be particularly salient to ASMR experiencers due to their ability to elicit a pleasurable sensory experience and a positive emotional response. As such, the potential therapeutic benefits of boosted positive affect and reduced pain perception in ASMR may be driven by atypical attentional control combined with heightened sensitivity to sensory input and atypical integration of sensory and emotional responses. Although, as mentioned earlier, the fact that control participants also seemed to have benefited from watching ASMR videos in terms of reduced reported pain sensitivity, the potential analgesic effects of ASMR stimuli on ASMR experiencers and controls needs to be investigated further.
It is of note that while the frequency of ASMR tingles in this study was the highest in response to the ASMR video compared to baseline and the control video the overall ratings were relatively low. The scale ranged between 1 and 7 and the highest score in this study was only 6, while 4 was the most frequent rating. Two ASMR -experiencers indicated they did not experience any tingling in response to the ASMR video. This suggests that perhaps the chosen videos were not triggering extreme ASMR responses. The ability to become immersed in ASMR videos appears to be an important factor of ASMR experience and it is possible that the lab setting and the actual administration of the algometer may have disrupted participants’ ability to become absorbed in the videos resulting in subdued ASMR responses. It is also possible that due to the individual differences in trigger preferences (Barratt & Davis, 2015; Janik McErlean & Banissy, 2017; Poerio et al., 2018) the chosen videos may have not appealed to all participants equally, despite ensuring that several common triggers appeared in these videos. It, therefore, remains to be established whether more intense ASMR sensation could lead to a more pronounced positive effect on pain processing. It is possible that ASMR needs to be triggered to a sufficiently high level and perhaps for a sufficiently long duration to reverse the existing negative relationship between ASMR and pain tolerance and to shift it into a positive one. It may also be beneficial to tailor the videos to specific preferences of each participant to elicit the maximally intense ASMR experience and its beneficial effects.
Moreover, it also appears that while the control video elicited ASMR to some extent, this was not as pronounced as the tingles in response to the ASMR video, which highlights the effectiveness of the chosen media in this study but at the same time demonstrates that ASMR can be triggered to an extent unintentionally by a variety of stimuli. Interestingly, Poerio et al. (2018) also found that the control videos induced tingles in ASMR participants, although to a lesser extent than the current study. Similarly to our results, they also found that control participants indicated some level of tingling which suggests that the groups may perhaps be better distinguished based on the degree of the ASMR intensity. Recently it has been suggested that other factors such as calmness, intensity, pleasantness, and location of the sensation should all be taken into account when differentiating ASMR-responders from non-responders and in order to differentiate further subgroups within these categories (Swart et al., 2021)
Conclusion
This exploratory study has found that ASMR is associated with increased pain sensitivity. While the current results point to potential therapeutic benefits of experiencing ASMR in terms of pain reduction, this appears to reflect the protective properties of ASMR buffering against the already existing elevated pain sensitivity among ASMR experiencers relative to controls.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethics approval for this study was obtained from the Ethics Reviewer at Bath Spa University.