
Abstract
The negative side effects of mask-wearing on reading facial emotional cues have been investigated in several studies with adults post-2020. However, little is known about children. This study aimed to determine the negative influence of mask-wearing on reading emotions of adult faces by Japanese school-aged children, compared to Japanese adults. We also examined whether this negative influence could be alleviated by using a transparent face mask instead of an opaque one (surgical mask). The performance on reading emotions was measured using emotion categorization and emotion intensity rating tasks for adult faces. As per the findings, the accuracy of emotion recognition in children was impaired for various facial expressions (disgust, fear, happy, neutral, sad, and surprise faces), except for angry faces. Conversely, in adults, it was impaired for a few facial expressions. The perceived intensity for happy faces with a surgical mask was weaker in both children and adults than in those without the mask. A negative influence of wearing surgical masks was generally not observed for faces wearing a transparent mask in both children and adults. Thus, negative side effects of mask-wearing on reading emotions are observed for more facial expressions in children than in adults; transparent masks can help remedy these.
Face masks effectively prevent the spread of the coronavirus disease 2019 (COVID-19) pandemic (Abaluck et al., 2022). Since the onset of the COVID-19 pandemic, however, people have experienced difficulties communicating with others while wearing masks. Face masks cover not only verbal information (Atcherson et al., 2017) but also nonverbal information such as facial expressions, which are important for interpersonal communication. For example, emotion recognition from a face is more difficult when wearing a face mask than when not wearing it (Carbon, 2020; Marini et al., 2021; Pazhoohi et al., 2021). Furthermore, the perceived intensity of emotions (i.e., perceived strength of emotional expression) is reduced by wearing masks (Pazhoohi et al., 2021; Sheldon et al., 2021; Tsantani et al., 2022). These results have been derived from the unavailability of cues around the mouth, which are essential for reading facial expressions (Schyns et al., 2002).
The negative side effects of wearing masks on reading emotions have been investigated in several studies since the onset of the COVID-19 pandemic (Pavlova & Sokolov, 2022). However, these findings rely heavily on empirical studies with adult participants, with the exception of nine studies (Bourke et al., 2023; Carbon & Serrano, 2021; Chester et al., 2022; Cuzzocrea et al., 2023; Gil & Le Bigot, 2023; Giordano et al., 2022; Gori et al., 2021; Ruba & Pollak, 2020; Schneider et al., 2022). It is questionable whether the results for adult participants can be generalized to school-aged children. Indeed, in terms of specific emotions, the impairments caused by mask-wearing on the recognition of facial expressions are different between adult and child participants. For example, impairments are observed for angry, disgusted, happy, and sad faces among adult participants (Carbon, 2020), whereas those are found for disgusted, fearful, happy, and sad faces among child participants (Carbon & Serrano, 2021). For anger and neutral faces, the accuracy of emotion recognition is improved by mask-wearing (Carbon & Serrano, 2021). In addition, the effect size of mask-wearing impairments on emotion recognition depends on the developmental stage: impairments are larger in children aged 3–5 years than in those aged 6–8 years (Gori et al., 2021). To prepare for the next large-scale pandemic, it is essential to examine how to cope with the negative side effects on children and increase the levels of evidence readiness (i.e., how ‘ready’ the application or intervention is, IJzerman et al., 2020).
It should also be noted that no studies have been conducted on East Asian children. Post-2020, as mentioned above, nine studies have shown that face masks reduce children's emotion recognition performance. These studies have been conducted in the USA (Carbon & Serrano, 2021; Chester et al., 2022; Giordano et al., 2022; Ruba & Pollak, 2020) and Europe (Bourke et al., 2023; Cuzzocrea et al., 2023; Gil & Le Bigot, 2023; Gori et al., 2021; Schneider et al., 2022). The bias of the sample was also common in previous studies conducted before the COVID-19 pandemic (Gagnon et al., 2014; Guarnera et al., 2017, 2015; Roberson et al., 2012), in which emotion was recognized from parts of the face (e.g., trimmed eyes or mouth). The fact that a limited number of studies with Western children has been conducted is important partly because Western Caucasians rely on both mouth and eye regions compared to East Asians, who mainly use the eye region, resulting in greater negative impacts of face masks on the recognition of emotional expressions. Cultural differences in scanning during emotion recognition have emerged seven months after birth (Geangu et al., 2016). Nonetheless, there is no doubt that the mouth region and configural face information are critical for the early development of perception and communication for infants regardless of ethnicity (Carnevali et al., 2022). They are also essential for the development of emotion recognition in children (Roberson et al., 2012). Given that a greater proportion of the population generally accepts mandatory mask-use requirements and adheres to using face masks in East Asian countries (Chang et al., 2021; Chen et al., 2020), the impact of face masks on the recognition of emotional expressions should be examined for children in East Asia, where examinations of mask-wearing on emotion recognition are apparently missing.
The aim of the present study was not only to determine the negative influence of mask-wearing on emotion recognition from faces in East Asian children compared to East Asian adults but also to find a way to alleviate it. During the COVID-19 pandemic, researchers have suggested plausible approaches to reduce this negative influence (Mheidly et al., 2020). One approach is to complement this with body language or gestures. The perception of facial expressions is modulated by body language (Aviezer et al., 2008). Indeed, some facial expressions can be read by body language even when wearing masks (e.g., a mask-worn angry face with an angry arm and a fist raised in the air). However, the improving effects of body language on reading emotions from mask-worn faces are limited to specific emotions, that is, angry, fearful, and sad faces (Ross & George, 2022; note that these findings were observed in studies with adult participants). In addition, such an indirect approach using body language cannot solve the fundamental problem that children cannot perceive the entire face of the mask-wearer. Developing the ability to recognize emotions from a child's face continues into late adolescence (Gao & Maurer, 2010; Herba et al., 2006). The use of visual cues during the recognition of facial expressions also changes from 9 to 10 years old: children depend less on the eye region to recognize emotions (Roberson et al., 2012). This development may be inhibited in daily life with face masks.
Our direct approach to solving the negative influence of wearing masks on reading emotions is to introduce a transparent face mask (hereinafter referred to as a transparent mask). The transparent mask is adapted with clear antifog plastic sheets in the front part of the mask. Unlike a conventional opaque face mask (hereinafter referred to as a surgical mask), the transparent mask allows people facing the wearer to see around the wearer's mouth. Several transparent masks have been developed, and their effectiveness and usability in various contexts have been explored post-2020 (Department of Health and Social Care, 2021). It is evident that the wearer's facial expressions can be accurately identified by wearing a transparent mask. The results for adult participants were consistent with this assumption (Marini et al., 2021; Miyazaki et al., 2022). However, contrary to this assumption, reading emotions from faces with a transparent mask might be difficult for child participants. Since children prefer novel objects (Hutt, 1975; Smock & Holt, 1962), they may be distracted by the attentional capture of the transparent mask based on novelty (i.e., attending to the mouth region covered with the transparent mask compared to the eye region). Consequently, reading specific facial expressions, such as angry, fearful, and sad faces, may be more difficult because visual cues in the eye area are important in the expressions (Bombari et al., 2013; Wegrzyn et al., 2017). Considering this possibility, it is important to confirm the effects of wearing a transparent mask (vs. not wearing a mask) on reading emotions.
The purpose of the present study was to determine the negative influence of wearing a surgical mask on reading emotions from adult faces among Japanese school-aged children compared with Japanese adult participants. The performance on reading emotions was measured using emotion categorization and emotion intensity rating tasks for adult faces. Through analogy with a previous study conducted in the Western culture (Carbon, 2020; Carbon & Serrano, 2021; Chester et al., 2022), we predicted that the negative influence would differ between Japanese children and adult participants when examined for each facial expression. In addition, we examined whether the negative influence, if any, could be alleviated by using a transparent mask, as in a previous study with adult participants (Marini et al., 2021; Miyazaki et al., 2022).
Methods
Participants
The data for the adult participants were drawn from our previous study (Miyazaki et al., 2022). The sample size in the previous study was determined to be more than 159 to detect the medium-sized effect in the type of face mask for each facial expression (f = 0.25, α = .05, 1 − β = .80, number of groups = 3; Faul et al., 2007). However, considering invalid responses, we recruited 300 adult participants from a crowdsourcing service. Data for child participants were obtained from a Japanese elementary school. We planned to collect a similar amount of data (>250) for children, as for adult participants. The child participants and their guardians provided informed consent. Finally, data from 282 children (141 girls, 138 boys, and three did not specify their sex; Mage = 10.2 years; 9–12 years) and from 258 Japanese adults (149 women, 107 men, and two did not specify their sex; Mage = 39.0 years; 20–59 years) who passed the data inclusion/exclusion criteria (see below) were used in the statistical analysis. This research project was approved by the research ethics committee of the institution of the last author.
Design
There were three independent variables of interest: age (between-participants factor: child and adult groups), the type of face mask (between-participants factor: no-mask, surgical mask, and transparent mask groups), and the facial expression of the stimulus (within-participants factor: anger, disgust, fear, happy, neutral, sad, and surprise faces). The child and adult participants were randomly assigned to one of three face mask groups (no-mask group, n = 90 and n = 91; surgical mask group, n = 97 and n = 80; transparent mask group, n = 95 and n = 87). To exclude the influence of demand characteristics and carryover effects, the type of face mask was manipulated as a between-participants factor. The order of the seven facial expressions was randomized across participants.
Face Stimuli
Two face models of East Asian young women (Y48F and Y52F) with seven facial expressions were selected from the Tsinghua Facial Expression Database (Yang et al., 2020) with permission. These 14 images were used as stimuli in the no-mask group. The stimuli of the surgical and transparent mask groups were digitally edited using a graphic editor (Adobe Photoshop 22.4, Adobe Inc.). An image of the surgical mask product or that of the transparent mask product was superimposed on the original face (i.e., no mask) images in the surgical and transparent mask groups, respectively (Figure 1). An additional face image (Y6F) was drawn from the same database for practice trials. The size of all facial stimuli was reduced to 300 × 400 pixels.

Examples of face stimuli used in the present study. Images were obtained from the Tsinghua Facial Expression Database with permission (Yang et al., 2020).
Considering that the stimuli in the surgical mask group were digitally edited, the digital editing may not fully capture the nuances of real-life mask usage, as face masks tend to deform with mouth and cheek movements. However, Grenville and Dwyer (2022) showed similar results between the condition created by digital editing and the condition of actually wearing a surgical mask. The subtle deformation with mouth and cheek movements when a person wears a surgical mask in real life would not be a critical cue to improve the performance of emotion recognition. Therefore, digitally edited stimuli were used in the present study.
To create the stimuli in the transparent mask group, we adjusted the opacity level to simulate the appearance of the actual product (Kao-ga-mie [face-visible] mask, Unicharm Corporation). The opacity level of the plastic part (the front part of the mask) in the image was manipulated in Adobe Photoshop (Adobe Inc.) from 100 to 20 (see https://osf.io/mkt2r/). The opacity level was determined by the discussion with the developers of the transparent face mask.
Procedure
The experimental platform was created by Qualtrics. The task was identical between the children's and adults’ experiments, except that the wording was simplified for the child participants to understand the task. The task consisted of emotion categorization and intensity ratings. Participants were required to categorize the perceived facial emotion of a stimulus into one of seven categories (anger, disgust, fear, happy, neutral, sad, and surprise) and to evaluate the perceived intensity of the facial emotion using a linear slider that ranged from 0 (extremely weak) to 100 (extremely strong) at their leisure. One face stimulus was shown on the screen at a time during each trial. Subsequent facial stimuli appeared after the responses.
The tasks in the practice and test trials were identical. In the practice trials, participants were required to practice using the extra face stimuli that were not used in the experimental trials without a mask, regardless of the assigned face mask group. Before initiating the experimental trials, the following instructions were presented depending on the assigned group: in the surgical mask (or transparent mask) group, participants were instructed to respond regardless of whether the faces were covered by a surgical mask (or a transparent mask). For participants who were unfamiliar with the transparent mask, example images of a woman wearing a transparent mask were displayed along with the descriptions in the transparent mask group. In the no-mask group, no additional instructions were displayed, and the participants proceeded to categorize the perceived facial emotion and its intensity. After completing the test trials, participants answered their age (plus their grade for child participants) and sex and were debriefed.
The data for the child participants were obtained via in-person group experiments at an elementary school on May 26, 2022. The experiments were conducted in each classroom under the instruction of elementary school teachers and the sixth and last author. The child participants individually accessed the experimental platform on their tablet computer (Chromebook). The viewing distance was not fixed. The instruction, practice, and test trials were designed to be sufficiently comprehensible to children, based on the advice of their elementary school teachers. First, after accessing the experimental platform, the child participants performed practice trials to learn the emotion intensity rating (see below) using a linear slider. Second, they performed two practice trials in which happy or angry faces were presented in a random order without a face mask, regardless of the assigned group of face masks. For the practice trials only, the child participants received feedback on whether their responses were correct or incorrect (there was no feedback for the test trials). Following the practice trials, the child participants performed 14 (two models × seven facial expressions) test trials.
Data for adult participants were obtained via online experiments in our previous study (Miyazaki et al., 2022, Experiment 1). The data were collected on June 9, 2021. In the experiment, adult participants conducted 28 test trials (four models × seven facial expressions) following seven practice trials. Fourteen of the 28 test trials were selected for analysis in the present study. In the 14 test trials, the same two models were presented to the participants as in the experiment with the child participants. Data from the remaining 14 trials were excluded because the models of these trials were not used in the experiment with child participants. The reason for shortening the number of trials from 28 to 14 for the child participants was to maintain their concentration regarding the task. Note that the experiment with the adult group included attention checks.
Data Exclusion
The data inclusion/exclusion criteria were determined in accordance with the previous study (Miyazaki et al., 2022) before administering the present study. A total of 315 children accessed the experimental platform. Thirty-three participants were excluded from the statistical analysis as follows: (a) participants who answered incorrectly in emotion categorization in all practice trials (n = 10); (b) participants with low intensity (<2 SD from the group mean) in the emotion intensity rating in practice trials (n = 10); and (c) participants with low accuracy or low intensity (<2 SD from the group mean) in emotion categorization or emotion intensity rating in the test trials (no-mask group, n = 7; surgical mask group, n = 2; transparent mask group, n = 4).
Data of certain adult participants were excluded based on the data inclusion/exclusion criteria of our previous study (Miyazaki et al., 2022). A total of 579 adult participants accessed the experimental platform. Three hundred and twenty-one participants were excluded based on the following criteria: (a) participants who did not return valid answers for attention checks (n = 280); (b) participants with low accuracy or low intensity (<2 SD from the group mean) in emotion categorization or emotion intensity rating in the practice trials (n = 28); and (c) participants with low accuracy or low intensity (<2 SD from the group mean) in emotion categorization or emotion intensity rating in the test trials (no-mask group, n = 7; surgical mask group, n = 4; transparent mask group, n = 2).
Results
The following analyses were performed using JASP 0.16.4 (JASP Team, 2022).
Emotion Recognition
A three-way (age × face mask × facial expression) mixed analysis of variance was conducted on the mean scores of correct answers in the emotion categorization (Figure 2). The main effects of the age (F(1, 534) = 37.06, p < .001, ηp2 = .06), face mask (F(2, 534) = 101.41, p < .001, ηp2 = .28), and facial expressions (F(6, 3204) = 409.66, p < .001, ηp2 = .43) were identified. In addition, two-way interactions were observed between age × face mask (F(2, 534) = 4.63, p = .010, ηp2 = .02) and face mask × facial expressions (F(12, 3204) = 21.58, p < .001, ηp2 = .07). No other significant interactions were observed. The interaction of age × face mask indicated that emotion categorization in the adult group was better than that in the child group (F(1, 179) = 12.30, p < .001, ηp2 = .06) and surgical mask group (F(1, 175) = 28.97, p < .001, ηp2 = .14). However, the effect of age was not significant in the transparent mask group, F(1, 180) = 2.39, p = .124, ηp2 = .01. The lack of advantage of the adult participants in the transparent mask group might be explained by the novelty of the transparent mask, which captures the attention of child participants (Hutt, 1975; Smock & Holt, 1962). As a result of the attentional capture of the transparent mask and, eventually, of the mouth region, which is important for recognizing facial expressions (Schyns et al., 2002), the advantage of adult participants, compared to child participants, could be obscured in the transparent mask group.
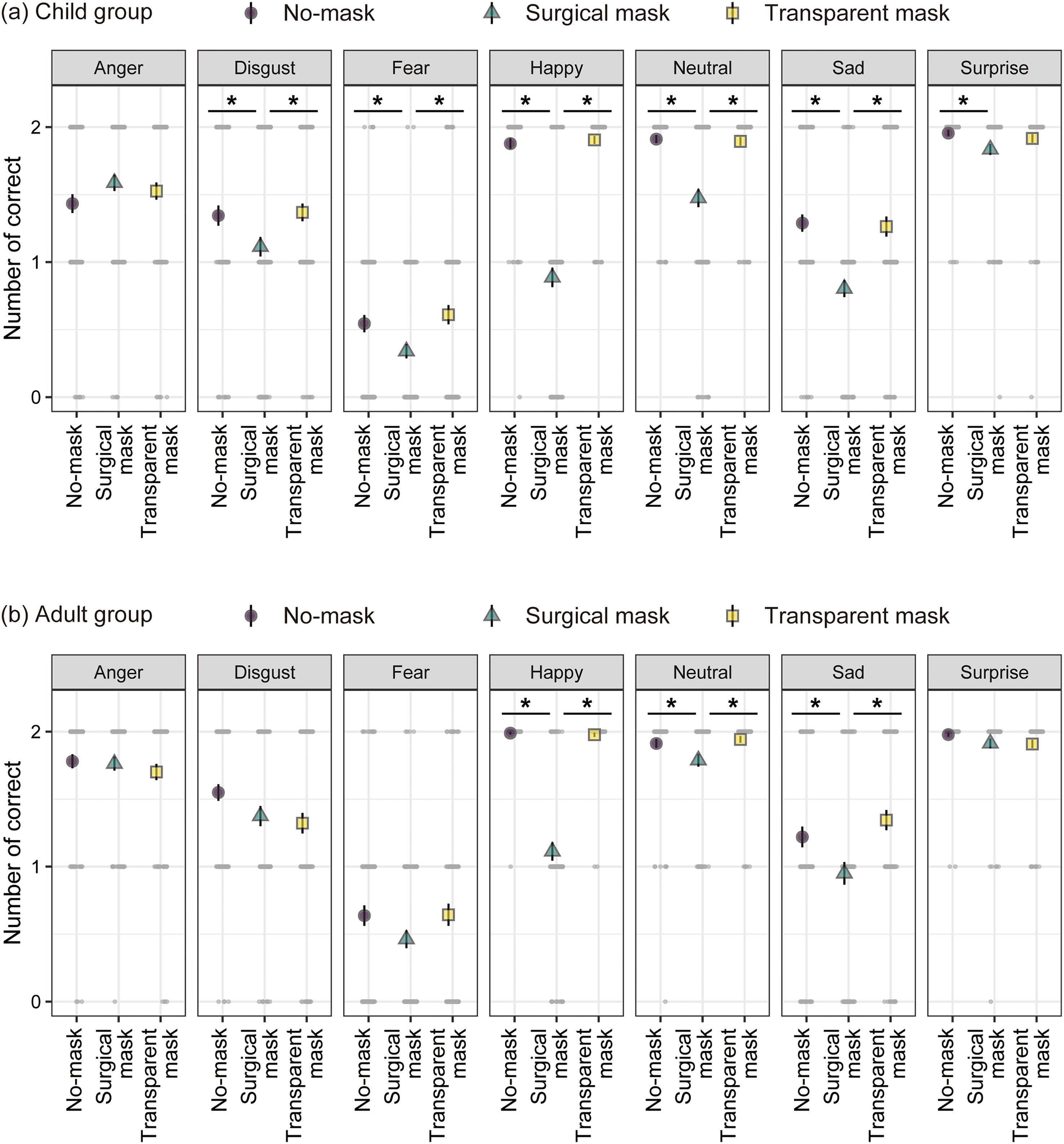
Means of the number of corrects for the emotion categorization as a function of the face mask and facial expression in the child group (a) and adult group (b). The black points with bars represent means ± 1 standard errors. The gray dots depict single data points. *p < .05.
Although the three-way interaction was not significant (F(12, 3204) = 1.35, p = .181, ηp2 = .01), simple interaction tests were conducted on the child and adult groups based on the current study's purpose. The details of the post hoc analyses are presented in the following sections. To summarize the analysis results, accurate emotion recognition from faces with a surgical mask compared to those without the mask was impaired for children, except for angry faces. In contrast, impairments in emotion recognition were relatively limited for adults (impairments were found for happy, neutral, and sad faces). In addition, no such impairments were observed in faces with a transparent mask instead of a surgical mask in both children and adults. We also created confusion matrices and found no remarkable differences in the confusion patterns of facial expressions between the adult and child participants (see https://osf.io/mkt2r/).
Child Participants
Since a two-way interaction (face mask × facial expression) was found (F(12, 1674) = 13.06, p < .001, ηp2 = .09), a simple effect of the face mask for each facial expression was tested. A simple effect was identified for all facial expressions (Fs(2, 279) > 3.47, ps < .033, ηp2s > .02), except for angry faces (F(2, 279) = 1.46, p = .234, ηp2 = .01).
Multiple comparisons using Holm's method revealed that the number of correct answers in the surgical mask group was lower than that in the no-mask group for disgust (t(279) = 2.31, p = .043, d = 0.34), fear, (t(279) = 2.30, p = .044, d = 0.34), happy (t(279) = 13.76, p < .001, d = 2.01), neutral (t(279) = 6.52, p < .001, d = 0.95), sad (t(279) = 5.09, p < .001, d = 0.74), and surprise faces (t(279) = 2.58, p = .032, d = 0.38). However, no such difference was observed when wearing a transparent mask instead of a surgical mask (ts(279) < 0.85, ps > .398, ds < 0.13). In addition, the number of correct answers was larger in the transparent mask group than in the surgical mask group for disgust (t(279) = 2.59, p = .031, d = 0.37), fear (t(279) = 3.09, p = .007, d = 0.45), happy (t(279) = 14.34, p < .001, d = 2.07), neutral (t(279) = 6.37, p < .001, d = 0.92), and sad faces (t(279) = 4.89, p < .001, d = 0.71). No difference was found for surprise faces (t(279) = 1.75, p = .163, d = 0.25).
Adult Participants
Since a significant two-way interaction was identified (F(12, 1530) = 10.08, p < .001, ηp2 = .07), the same post hoc analysis for the child group was conducted for the adult group. Simple effects of face mask were identified for happy, neutral, and sad faces (Fs(2, 255) > 5.18, ps < .007, ηp2s > .03). No significant effects were observed for anger, disgust, fear, and surprise faces (Fs(2, 255) < 2.98, ps > .052, ηp2s < .03).
Multiple comparisons showed that the number of correct answers in the surgical mask group was fewer than that in the no-mask group (and transparent mask group) for happy, t(255) = 15.91, p < .001, d = 2.44 (and t(255) = 15.53, p < .001, d = 2.41); neutral, t(255) = 2.48, p = .028, d = 0.38 (and t(255) = 3.05, p = .008, d = 0.47); and sad faces, t(255) = 2.44, p = .031, d = 0.37 (and t(255) = 3.53, p = .002, d = 0.55). There were no differences between the no-mask and transparent mask groups (ts(255) < 1.16, ps > .249, ds < 0.18).
Emotion Intensity
A three-way mixed analysis of variance was conducted on the mean scores of the perceived intensities of emotion (Figure 3). The rating scores for each facial expression were averaged for the correct trials of the emotion categorization task. Since there were missing values for some facial expressions (i.e., the number of correct answers in some participants was 0 for a specific facial expression), data from 162 of 540 participants were used in the analysis of variance after treatment with list-wise deletion. The 162 participants included in the analysis correspond to those who have at least one correct response to all seven facial expressions. Out of the 162 participants, 79 (no-mask group = 30; surgical mask group = 18; transparent mask group = 31) were adult participants, and 83 (no-mask group = 34; surgical mask group = 11; transparent mask group = 38) were child participants. A significant main effect of facial expression (F(6, 936) = 19.00, p < .001, ηp2 = .11) and a significant two-way interaction between age × facial expression (F(6, 936) = 5.99, p < .001, ηp2 = .04), and between face mask and facial expression (F(12, 936) = 4.64, p < .001, ηp2 = .06), were identified. No other main effects or interactions were found.

Means of rating scores for perceived intensity of emotions as a function of the face mask and the facial expression in the child group (a) and adult group (b). The black points with bars represent means ± 1 standard errors. The gray dots depict single data points. Half-violin plots depict the kernel densities of the data. *p < .05.
Although no significant three-way interaction was found (F(12, 936) = 1.54, p = .105, ηp2 = .02), simple interaction tests of face mask × facial expression in the child and adult groups were conducted separately in accordance with the present study's purpose. The details of the post hoc analyses are presented in the subsequent sections. In sum, a lower perceived intensity of emotion for happy faces when wearing a surgical mask than when not wearing a mask was shown in both child and adult participants. However, such results were not observed when a transparent mask was used instead of a surgical mask.
Child Participants
Simple effect tests were performed for each facial expression based on the study purpose, although a two-way interaction (face mask × facial expression) did not reach significance (F(12, 480) = 1.76, p = .052, ηp2 = .04). A face mask had a significant effect only on happy faces (F(2, 248) = 8.99, p < .001, ηp2 = .07). No significant effects of face mask were observed for the other facial expressions (Fs < 2.92, ps > .057, ηp2s < .05). Multiple comparisons for happy faces revealed that the perceived intensity in the surgical mask group was lower than that in the no-mask (t(248) = 4.10, p < .001, d = 0.66) and transparent mask groups (t(248) = 3.26, p = .003, d = 0.52). However, there was no significant difference between the no-mask and transparent mask groups (t(248) = 0.97, p = .332, d = 0.14).
The n of data on the simple effect test of face mask for angry faces was 263, that for disgust faces was 243, that for fear faces was 122, that for happy faces was 251, that for neutral faces was 273, that for sad faces was 230, and that for surprise faces was 280. The ns of the data per facial expression differed because participants with zero correct answers were excluded from each expression.
Adult Participants
A two-way interaction (face mask × facial expression) was identified (F(12, 456) = 6.13, p < .001, ηp2 = .14). Significant simple effects of face mask were observed for angry (F(2, 247) = 4.72, p = .010, ηp2 = .04), fear (F(2, 116) = 4.11, p = .019, ηp2 = .07), happy (F(2, 244) = 53.86, p < .001, ηp2 = .31), and surprise faces (F(2, 254) = 3.75, p = .025, ηp2 = .03). No significant effects were found for disgust, neutral, and sad faces (Fs(2, 204–254) < 1.78, ps > .172, ηp2s < .02). Multiple comparisons for happy faces showed similar patterns in the results for child participants: perceived intensity in the surgical mask group was lower than that in the no-mask (t(244) = 9.90, p < .001, d = 1.58) and transparent mask groups (t(244) = 8.14, p < .001, d = 1.31). No significant difference was observed between the no-mask and transparent mask groups (t(244) = 1.79, p = .075, d = 0.27).
The results of multiple comparisons for angry, fear, and surprise faces were somewhat complicated. Regarding angry faces, the perceived intensity was higher in the surgical mask group than in the transparent mask group (t(247) = 2.95, p = .010, d = 0.46). Significant differences between the no-mask and surgical mask groups (t(247) = 2.26, p = .050, d = 0.35), and between the no-mask and transparent mask groups (t(247) = 0.75, p = .454, d = 0.11), were not identified. Regarding fear faces, the perceived intensity was lower in the surgical mask group than in the no-mask group (t(116) = 2.35, p = .041, d = 0.54). However, there was no significant difference between perceived intensity in the surgical mask and transparent mask groups (t(116) = 0.03, p = .980, d = 0.01). Furthermore, the perceived intensity in the transparent mask group was lower than that in the no-mask group (t(116) = 2.52, p = .039, d = 0.54). Regarding perceived intensity for surprise faces, it was lower in the transparent mask group than in the no-mask group (t(254) = 2.52, p = .037, d = 0.39). No significant differences were found between the surgical mask and no-mask groups (t(254) = 0.42, p = .672, d = 0.07) and between the no-mask and transparent mask groups (t(254) = 2.18, p = .061, d = 0.33).
The n of data on the simple effect test of face mask for angry faces was 250, that for disgust faces was 234, that for fear faces was 119, that for happy faces was 247, that for neutral faces was 257, that for sad faces was 207, and that for surprise faces was 257.
Discussion
We examined the negative influence of wearing a surgical mask compared to not wearing a mask on reading emotions from a face in Japanese school-aged children (9–12 years old) and adults (20–59 years old). This negative influence was observed in a greater number of facial expressions among child participants than adult participants. Compared to adult participants, child participants demonstrated poor performance in emotion recognition from mask-worn faces in a variety of facial expressions. To the best of our knowledge, this is the first study with a sample of East Asian children to test the effects of mask-wearing on reading emotion from a face (Bourke et al., 2023; Carbon & Serrano, 2021; Chester et al., 2022; Cuzzocrea et al., 2023; Gil & Le Bigot, 2023; Giordano et al., 2022; Gori et al., 2021; Ruba & Pollak, 2020; Schneider et al., 2022, for Western children), including studies investigating emotion recognition from parts of the face (Gagnon et al., 2014; Guarnera et al., 2017, 2015; Roberson et al., 2012, for Western children). In addition to identifying the negative influence of wearing masks, we further demonstrated that this impairment in emotion recognition can be alleviated by using a transparent mask.
The present findings suggest that differences in developmental stages should be considered to comprehensively understand the negative influence of mask-wearing on emotion recognition. The pattern of performance decline in emotion recognition in child participants was inconsistent with that in adult participants. However, these results are unlikely to be derived from the use of adult facial stimuli. To our knowledge, no studies have demonstrated own-age advantages for recognition of basic emotions: children (5–8 years old and 9–13 years old) and adults do not recognize emotions better on faces of their age group (Griffiths et al., 2015; also see Tremblay et al., 1987). Such advantages do not occur even for mask-worn faces (Chester et al., 2022). Rather, this inconsistency indicates that the empirical findings observed in adults cannot be generalized to children. In addition, a previous study demonstrated that the negative influence of mask-wearing on emotion recognition was more significant in younger children (3–5 years) than in older children (6–8 years) (Gori et al., 2021). It is possible that the results for older children may not be generalizable to younger children. In the present study, we recruited older children (9–12 years old) because their teachers were afraid that younger children would be incapable of complying with verbal instructions in the experiment. Further studies with younger children are required to clarify the differences in developmental stages regarding the negative influence of mask-wearing on emotion recognition.
The present results for Japanese children differ from those of US children of similar age groups (Carbon & Serrano, 2021; Chester et al., 2022). In the present Japanese children sample, the accuracy of emotion recognition was impaired in a variety of facial expressions, except for angry faces, by wearing masks (Figure 2(a)). In a US sample of children, the accuracy was impaired for disgust, fear, happy, and sad faces, while it was improved for angry and neutral faces (Carbon & Serrano, 2021). In another sample of US children, impairments were identified for fear, happy, and sad faces, but not for angry and neutral faces (Chester et al., 2022). The differences between Japanese and US children cannot be attributed to cultural differences in attention orienting during emotion recognition from the face (i.e., East Asians, including children, pay more attention to the eyes relative to the mouth than Western Caucasians (Geangu et al., 2016; Jack et al., 2009). It is worthwhile to examine whether the results observed in Western children can be generalized to East Asian children using equivalent stimulus sets with comparable intensity of emotional expressions and identical low-level image characteristics (e.g., the appearance of crow's feet, which is a striking cue for perceiving happy faces) that were different among the databases used in the present and previous US studies.
There were two major findings regarding the ratings of perceived intensity. First, we found that the perceived intensity for happy faces was weakened by wearing a surgical mask for both children and adults (Figure 3). These results are reasonable because the mouth and zygomaticus major provide critical cues for signaling happiness in both children (Guarnera et al., 2017, 2015; Kestenbaum, 1992) and adults (Bombari et al., 2013; Eisenbarth & Alpers, 2011). It is likely that occluding these cues reduces the perceived intensity of happy faces with a surgical mask. Given that exchanges of smiles (i.e., happy faces) are critical for forming the caregiver–child attachment bond (Bowlby, 1958), erroneous interpretations of smiles and reduction in the strength of smiling expression would be disadvantageous for young children (Emde & Harmon, 1972; Over, 2016). This disadvantage, with a reduction in smiling expressions, is similar for school-aged children. In classrooms, teachers use smiles with diverse meanings as a pedagogical resource; their smiles express affiliative and pedagogical responsiveness to children (Jakonen & Evnitskaya, 2020). Considering that smiles contribute to pedagogical interactions between teachers and children in classrooms, mask-wearing may inhibit children's learning opportunities in their school life (Spitzer, 2020). Second, some complex results were observed in adult participants. Mask-wearing increased the perceived intensity of anger compared to wearing a transparent mask in adult participants (left-most panel in Figure 3b). The increase in perceived intensity by wearing masks might be due to a relative increase in attention to the eyes. Attending to the eyes is important for detecting anger (Bombari et al., 2013; Eisenbarth & Alpers, 2011). However, a similar increase was not found for fear faces, although attending to the eyes is also important when detecting fear (Bombari et al., 2013; Eisenbarth & Alpers, 2011). Rather, mask-wearing reduced the intensity of fear faces (third panel from the left in Figure 3b). Thus, attention to the eyes cannot fully explain the differences in the results. Similarly, the perceived intensity of fear or surprise faces was decreased by wearing a transparent mask only in adult participants. The reason for these results is unclear and further studies are required.
In contrast to the accuracy of emotion recognition, the ratings of the perceived intensity of emotion for each facial expression did not differ between adult and child groups except for the uninterpretable results in the adult participants mentioned above. Might these results imply that the negative influence of mask-wearing on the perceived intensity of emotion in the child participants did not occur across many facial expressions? However, there was one caveat to these results. The null aspects of the negative influence of mask-wearing on the perceived intensity of emotion could have been caused by the small power to detect the effect of the type of face mask. In the analysis, we averaged the rating scores for the correct trials in the emotion recognition task. As the number of correct answers in some participants was zero for a specific facial expression and for a specific face mask group, there were some missing values in the analysis. Although the analysis of some facial expressions involved data, such as the simple effect test of the type of face mask on surprise faces, other simple tests did not involve enough data. For instance, the n of data on the simple effect test for the type of face mask in fear faces was 122 (out of 282) for the child group (no-mask group, n = 44; surgical mask group, n = 31; transparent mask group, n = 47) and 119 (out of 258) for the adult group (no-mask group, n = 45; surgical mask group, n = 33; transparent mask group, n = 41). The sample size had been planned to detect the medium-sized effect in the type of face mask for each facial expression (f = 0.25, α = .05, 1 − β = .80) in child and adult groups, respectively (see Methods). However, these ns of 122 and 119 were insufficient to detect the medium-sized effect. The lack of significant effects of mask-wearing on the perceived intensity of emotion might be derived from the insufficient power. An additional study with a sufficient sample size with the replacement for the missing values is necessary for understanding the impact on the perceived intensity of emotion.
We acknowledge the limitation arising from using only two female facial stimuli. The small number of face stimuli and, eventually, the small number of trials were for two reasons. The first reason was the constraints on resources and time in the field. When the present data were collected in the elementary school, COVID-19 was still spreading in Japan (April–May 2022). We had to prioritize reducing the burdens on the students and shortening the time of the experiments as much as possible when we conducted experiments in the elementary school under these situations. The second reason was the difficulty in maintaining the concentration of elementary school students on the present task for many minutes. After conducting a preliminary experiment and receiving advice from elementary school teachers, the number of face stimuli was determined as two images, yielding the number of trials as 14 trials, accordingly. We also considered the previous studies investigating emotion recognition from masked faces or parts of faces using only two face stimuli (for adult participants, Blazhenkova et al., 2022; for child participants, Guarnera et al., 2015, 2017) in determining the number of face stimuli. This small number of face stimuli and trials could be inadequate to assess the strength of the negative influence of mask-wearing. Specifically, the number of correct answers was approximately one or above one out of the two trials for each facial expression (Figure 2), except for fear faces. This reduction in the number of correct answers due to mask-wearing, whether substantial or minor in impact, might produce different opinions among readers.
In 2015, Bill Gates, a cofounder of Microsoft, warned of the next epidemic following the Ebola epidemic in West Africa in his TED talk (Gates, 2015). In the talk, he concluded with the following statement: “In fact, if there is one positive thing that can come out of the Ebola epidemic, it is that it can serve as an early warning, a wake-up call, to get ready. If we start now, we can be ready for the next epidemic.” We must learn lessons from the current experience from 2020 to prepare for the next pandemic. The authors believe that one of the essential tasks for researchers in experimental psychology in preparing for the next pandemic is to identify the negative psychological side effects of mask-wearing and to investigate ways to remedy them. The development and improvement of transparent mask products are one facet of this investigation. We believe that these are especially important for children in terms of the development of the ability to read emotions from faces (Gao & Maurer, 2010; Herba et al., 2006), when a situation arises where face masks must be worn on a daily basis, as in 2020.
Footnotes
Acknowledgements
We would like to thank the elementary school students, their teachers, and their guardians for their cooperation with our research. We also thank Rie Iizuka, a staff member of the Research Promotion Office at Hokkaido University, for coordinating our research.
Author Contribution(s)
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The transparent and surgical face masks used in this study were commercial products produced by the Unicharm Corporation. Authors T. S., K. W., and K. M. are employees of the Unicharm Corporation.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present study was funded by the Unicharm Corporation.