
Abstract
Objective
This study aimed to assess the infrazygomatic crest (IZC) bone thickness and insertion heights at varying insertion angles in patients with different vertical facial growth patterns using cone beam computed tomography (CBCT).
Materials and Methods
The study included 48 healthy Maharashtrian Indian subjects (24 males, 24 females; aged 20-30 years) with no history of previous orthodontic treatment. Subjects were classified into three groups—hypodivergent, normodivergent, and hyperdivergent based on cephalometric parameters (Sella–Nasion to mandibular plane angle, overbite depth indicator, Jarabak’s ratio). CBCT imaging (Carestream CS 9300) was used to assess IZC bone thickness and insertion heights at insertion angles from 40° to 80°. The measurements were taken bilaterally, and data were analyzed for group-wise, gender-wise, and side-wise differences using analysis of variance and Scheffé’s post hoc test.
Results
Bone thickness increased progressively with an increase in insertion angles across all the groups. Hypodivergent subjects exhibited the highest bone thickness, followed by normodivergent, with hyperdivergent showing the least. Males and the left side measurements showed higher bone thickness generally. Insertion heights decreased with increasing angles across all the groups, with hyperdivergent subjects having the highest heights. No consistent gender- or side-based variations in insertion heights were observed.
Conclusions
IZC bone morphology varies significantly with vertical facial growth patterns. Hypodivergent individuals exhibited greater cortical bone thickness, whereas hyperdivergent individuals demonstrated greater insertion heights. Bone thickness increased, and insertion height decreased with increasing insertion angulation.
Introduction
Temporary skeletal anchorage devices (TSADs), introduced by Kanomi in 1997, 1 have revolutionized anchorage management in orthodontics, allowing for precise tooth movements. Among these, the infrazygomatic crest (IZC) miniscrews have gained popularity because they offer a reliable, accessible site with relatively thick bone and minimal risk of root interference. 2 The success of miniscrew placement in the IZC region depends primarily on cortical bone thickness and insertion angle, both crucial for preventing complications such as maxillary sinus perforation and screw failure. 3 Notably, variations in vertical facial growth patterns significantly influence the craniofacial skeletal morphology, including cortical bone thickness and density in various regions.4-7
Despite the known variations, most existing studies evaluating IZC bone morphology according to vertical facial patterns have focused on Caucasian or East Asian populations, with limited data on Indian demographics, particularly the Maharashtrian subgroup, where distinct craniofacial patterns may necessitate modified placement protocols.
This study aims to bridge these gaps by using cone beam computed tomography (CBCT) to comprehensively assess bilateral IZC bone thickness and insertion heights at five insertion angles (40°-80°) in hypodivergent, normodivergent, and hyperdivergent adults from the Indian population, with a focus on the Maharashtrian demography. The investigation also evaluates gender and side-wise variations to provide orthodontists with optimized miniscrew placement guidelines, thereby improving treatment efficacy and minimizing complications.
Materials and Methods
Ethical approval for this study was provided by the Institutional Ethics Committee on March 20, 2023 (approval number: CSMSS/DCH/EC/2023/ORTHO/03). Written informed consent was obtained from all participants prior to their inclusion in the study.
A priori power analysis was conducted using G*Power software (version 3.1.9.7) assuming an effect size of 0.45, an alpha level of 0.05, and a power of 80%, which indicated that a minimum of 14 subjects per group would be required. To enhance statistical robustness and accommodate potential data exclusion, 16 subjects were recruited per group.
Sample Selection
The sample consisted of 48 subjects (24 males and 24 females), aged between 20 and 30 years, who required CBCT scanning as part of their diagnostic workup for orthodontic treatment.
The inclusion criteria were systemically healthy individuals with a full complement of maxillary teeth, good periodontal health, no prior orthodontic treatment, and no clinical signs of bruxism or heavy occlusal restorations. The exclusion criteria were the absence of maxillary permanent first or second molars, facial asymmetry, and a history of craniofacial trauma. After applying the exclusion criteria, the subjects were divided into three groups as follows.
Cephalometric Grouping
Standardized lateral cephalograms were obtained and analyzed using three skeletal vertical parameters:
Sella–Nasion to mandibular plane (SN–MP) angle. Jarabak’s ratio (posterior facial height/anterior facial height). Overbite depth indicator (ODI).
Based on these values, subjects were grouped into three vertical facial patterns, outlined in Table 1:
Grouping of Subjects Based on Cephalometric Parameters.

Group A: Hypodivergent (n = 16).
Group B: Normodivergent (n = 16).
Group C: Hyperdivergent (n = 16).
Subjects were classified based on the following cephalometric criteria:
Hypodivergent: SN–MP < 27°, ODI > 81°, Jarabak ratio 64%-80%.
Normodivergent: SN–MP 27°-37°, ODI 67°-81°, Jarabak ratio 59%-63%.
Hyperdivergent: SN–MP > 37°, ODI < 67°, Jarabak ratio 54%-58%.
Cone Beam Computed Tomography Imaging Protocol
All CBCT scans were taken as part of the patients’ orthodontic diagnostic records, and no additional scans were performed. CBCT scans were acquired using the Carestream CS 9300 (Carestream Health, Rochester, NY, USA) scanner under the following parameters: 85 kV, 6.3 mA, 11.3 s exposure time, voxel size of 300 µm, and a 17 × 13 cm field of view. Scans were exported in Digital Imaging and Communications in Medicine files and analyzed using Carestream 3D Imaging Software.
Infrazygomatic Crest Measurements
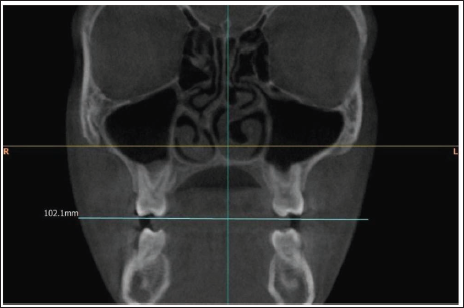
The coronal slice passing through the distobuccal root of the maxillary first molar was selected as the reference slice for all the measurements. The measurement procedure was as follows (Figure 1).
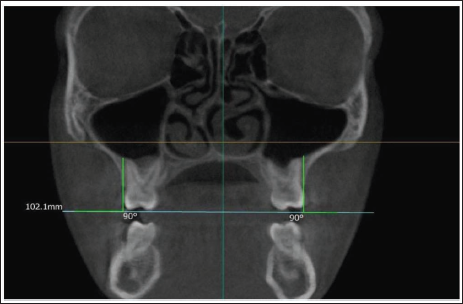
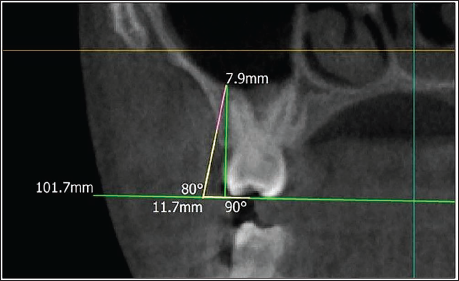
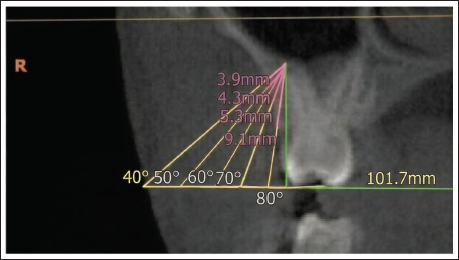
A horizontal reference line representing the maxillary occlusal plane and a vertical line tangent to the buccal surface of the distobuccal root of the first molar were drawn (Figures 2 and 3). The intersection of this vertical line with the floor of the maxillary sinus was marked as the sinus point (S). From this point, five lines were drawn at 40°, 50°, 60°, 70°, and 80° to simulate potential miniscrew insertion angles. For each angle, the bone thickness was measured along the trajectory from the S-point to the outer cortex of the IZC—L1-L5 (Figure 4). The vertical distance from the intersection point of each trajectory with the lateral surface of IZC to the occlusal plane was measured as the insertion height—H1-H5 (Figure 5).
Diagrammatic Representation of the Infrazygomatic Crest Measurement Protocol Used in the Study.

Coronal Cone Beam Computed Tomography (CBCT) Section Showing the First Reference Plane Represented by the Maxillary Occlusal Plane.
Coronal Cone Beam Computed Tomography (CBCT) Section Showing the Second Reference Plane Drawn as a Vertical Tangent to the Buccal Surface of the Distobuccal Root of the Maxillary First Molar.
Measurement of Infrazygomatic Crest Bone Thickness (Pink) and Insertion Height (Yellow) at an Insertion Angulation of 80°.
Measurement of Infrazygomatic Crest Bone Thickness (Pink) and Insertion Heights (Yellow) at All Simulated Insertion Angulations (40°-80°).
All measurements were performed bilaterally. To ensure accuracy and reduce inter-observer variability, each measurement was repeated three times, and the mean value was used for analysis. To assess intra-observer reliability, 20% of the sample was randomly re-evaluated after a 2-week interval. Intraclass correlation coefficient (ICC) was calculated using a two-way mixed-effects model (Shrout and Fleiss type 2) for absolute agreement. The intra-observer reliability was excellent, with an ICC value of 0.99 (95% CI: 0.96-1.00).
This observational study was conducted in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology guidelines. 8 Efforts to minimize bias included standardized CBCT acquisition protocols, consistent landmark identification, repeated measurements with calculation of intra-observer reliability, and the use of predefined cephalometric criteria for group classification.
Statistical Analysis
Statistical analysis was performed using Statistical Package for the Social Sciences software (version 20.0). Descriptive statistics were calculated for all variables, including the mean and standard deviation. Comparisons of bone thickness and insertion heights across the three groups (hypodivergent, normodivergent, and hyperdivergent) were conducted using one-way analysis of variance to determine significant differences among the groups. For pairwise comparisons, Scheffé’s post hoc test was applied to identify specific group differences. A significance level was set at P < .05 for all tests.
Results
This study assessed IZC bone thickness (L1-L5) and insertion heights (H1-H5) bilaterally in male and female subjects across three vertical facial patterns:
Group A: Hypodivergent, Group B: Normodivergent, and Group C: Hyperdivergent.
Intra-group Comparisons
Group A: Hypodivergent
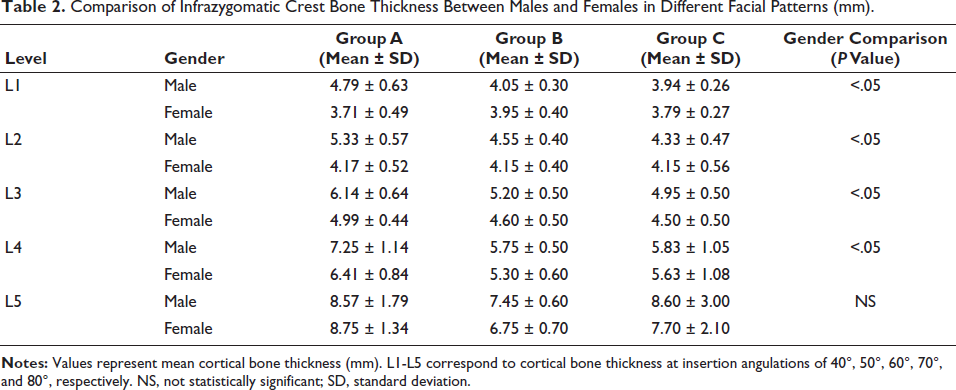
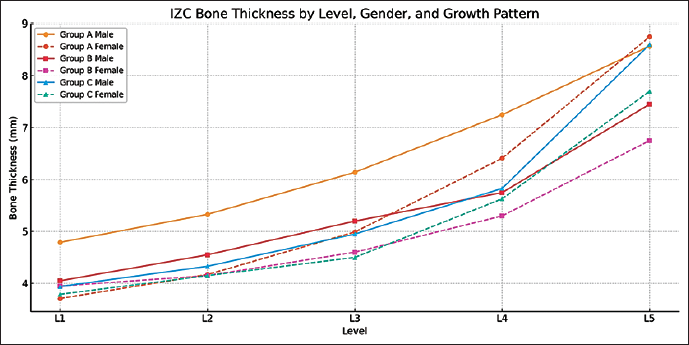
Mean cortical bone thickness increased progressively from L1 to L5 on both sides. The left side exhibited significantly higher thickness than the right at all levels (P = .02-.04). Males demonstrated significantly greater cortical bone thickness than females at all levels on the right side (P < .05), while, on the left side, males had significantly higher values at L1-L3, and females had greater thickness at L5 (P = .04) (Table 2, Figure 6).
Comparison of Infrazygomatic Crest Bone Thickness Between Males and Females in Different Facial Patterns (mm).
Gender-wise Comparison of Cortical Bone Thickness (L1-L5) at the Infrazygomatic Crest Region Among Hypodivergent (Group A), Normodivergent (Group B), and Hyperdivergent (Group C) Facial Growth Patterns.
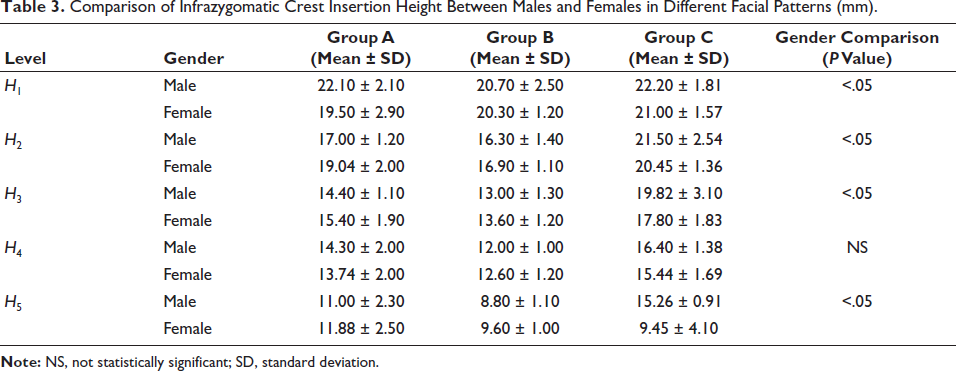
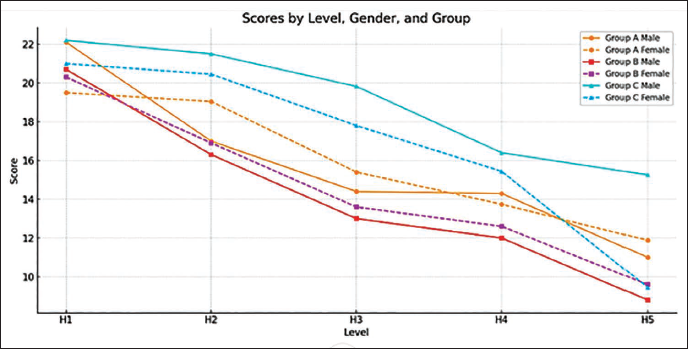
Insertion heights exhibited a decreasing trend from H1 to H5. The right side showed consistently higher mean values, with a significant difference at H1 (P = .003). Gender comparisons revealed significant differences at H1, H2, and H5 on the right side (P < .05), whereas on the left side, females had significantly greater insertion heights at H1 and H2 (P = .03 and P = .049, respectively) (Table 3, Figure 7).
Comparison of Infrazygomatic Crest Insertion Height Between Males and Females in Different Facial Patterns (mm).
Gender-wise Comparison of Insertion Height (H1-H5) at the Infrazygomatic Crest Region Among Hypodivergent (Group A), Normodivergent (Group B), and Hyperdivergent (Group C) Facial Growth Patterns.
Group B: Normodivergent
Mean cortical bone thickness increased progressively from L1 to L5, with higher values observed on the left side. Significant differences were noted at L3 and L5 (P = .04 and P = .03, respectively). Males showed greater bone thickness than females, significantly at L3 and L5 on the right side, and at L2, L3, and L5 on the left side (P < .05) (Table 2, Figure 6).
Insertion heights decreased from H1 to H5. The right side demonstrated significantly greater values at H1 and H5 (P = .0002 and P = .0342, respectively). Males exhibited greater insertion height at H1, while females had higher values at H5 on both sides (P = .03 and P = .04, respectively) (Table 3, Figure 7).
Group C: Hyperdivergent
As with the other groups, the mean cortical bone thickness values progressively increased from L1 to L5. The left side exhibited significantly higher thickness at L3 and L5 (P = .016 and P = .010, respectively). Males showed greater bone thickness on the right side, significantly at L3 (P = .002). On the left side, significant differences were observed at L3 and L5 (P = .016 and P = .010) (Table 2, Figure 6).
Insertion heights decreased from H1 to H5. The right side demonstrated higher values, with significant differences at H3 and H5 (P = .005 and P = .03, respectively). On the right side, males had significantly higher insertion heights at H3 and H5 (P = .005 and P = .03). On the left side, females exhibited higher values at most levels, with a significant difference at H5 (P = .001) (Table 3, Figure 7).
Inter-group Comparison
Cortical bone thickness:
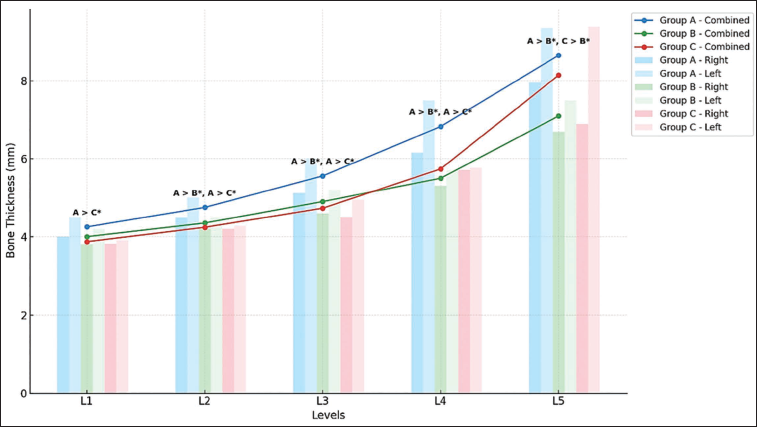
Group A demonstrated the highest bone thickness values across most angulations, followed by Group B and Group C. Statistically significant differences among groups were detected at several levels (Scheffé’s test, P < .05) (Table 4, Figure 8).
Insertion heights:
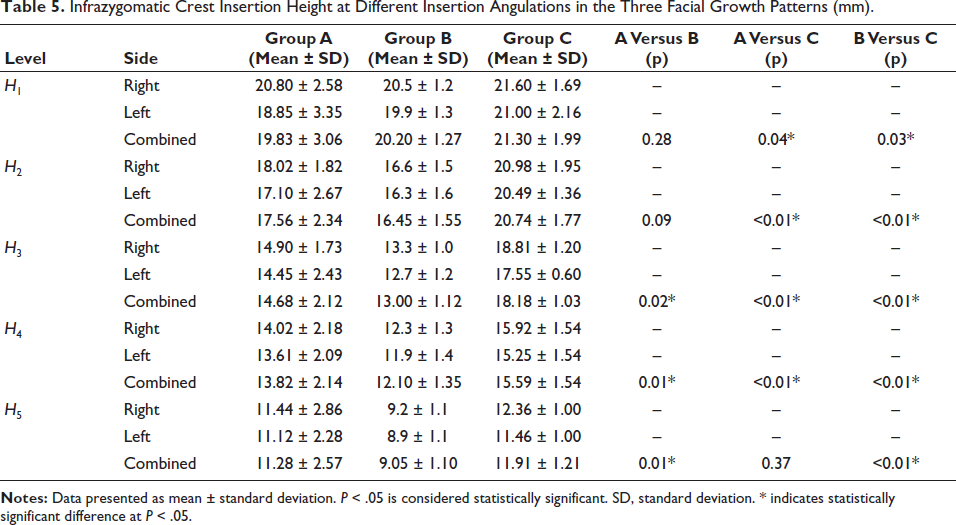
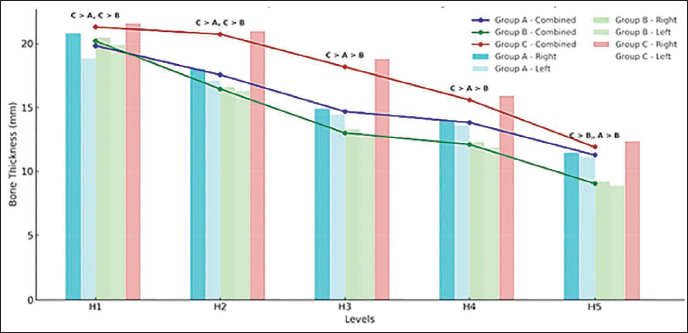
Insertion heights were greatest in Group C, followed by Group A and Group B. Significant differences between groups were noted, particularly at H1 and H3 (P < .05) (Table 5, Figure 9).
Infrazygomatic Crest Cortical Bone Thickness at Different Insertion Angulations in the Three Facial Growth Patterns (mm).

Inter-group Comparison of Infrazygomatic Crest Cortical Bone Thickness (L1-L5) Among Hypodivergent (Group A), Normodivergent (Group B), and Hyperdivergent (Group C) Facial Patterns Based on Combined Right- and Left-side Measurements.
Infrazygomatic Crest Insertion Height at Different Insertion Angulations in the Three Facial Growth Patterns (mm).
Inter-group Comparison of Infrazygomatic Crest Insertion Heights (H1-H5) Among Hypodivergent (Group A), Normodivergent (Group B), and Hyperdivergent (Group C) Facial Patterns Based on Combined Right- and Left-side Measurements.
Discussion
Accurate assessment of IZC bone morphology is essential for TSAD placement. This CBCT-based study evaluated IZC bone thickness and insertion heights in hypodivergent, normodivergent, and hyperdivergent individuals using the protocol of Liou et al. for clinically relevant and reproducible measurements. 9 The distobuccal root of the permanent maxillary first molar was preferred over the mesiobuccal root as a reference, based on evidence suggesting reduced tangential error and better reproducibility.10-12
In Group A, the IZC bone thickness ranged from 4 to 9.36 mm, increasing with angulation. These findings are consistent with the findings from Liou et al. 9 and Sharan et al. 18 Our study revealed significantly higher bone thickness values on the left side at all the angulations, which could be explained by differential functional loading, vascularization, and craniofacial asymmetry.14, 15 This finding aligns with Santos et al. 16 but contrasts with Dangal et al. 5 Sexual dimorphism was evident in Group A. Bone thickness values were generally higher in males, likely due to the greater occlusal forces causing cortical bone adaptation. 15 These results are consistent with the findings by Lee et al., and Sharan et al.17, 13 but contrast with Santos et al. 16
Insertion heights progressively decreased from H1 to H5. The right side exhibited higher values at H1 only. These findings align with Dangal et al., Murugesan et al., and Sharan et al.5, 13, 18 Gender-based differences were observed at specific levels, notably higher insertion heights in females at some sites, consistent with Sharan et al. 13
In Group B, bone thickness values varied from 4.20 to 8.20 mm, showing a progressive increase with higher insertion angles, which is consistent with previous literature.9, 20
No significant side-based differences were observed in Group B for most of the angulations except L3 and L5, where the left side exhibited higher values, consistent with earlier studies. 3
Males demonstrated significantly higher bone thickness at L2, L3, and L5. These findings align with Sharan et al. 13 but differ from Santos et al. 16
Group B also exhibited a progressive decrease in insertion heights from H1 to H5. The right side exhibited significantly greater heights at H1 and H5. Gender comparison revealed a mild trend of higher values in females at certain angulations, consistent with Sharan et al. 13
In Group C, bone thickness ranged from 3.82 to 9.40 mm, increasing with greater insertion angles, consistent with previous studies.9, 13
No significant side-wise differences were noted at L1, L2, and L4. Significant left-side differences were seen at L3 and L5, reflecting craniofacial asymmetry.6, 19, 21
Bone thickness was slightly higher in males at L3 and L5, aligning with Sharan et al. 13 Insertion heights progressively decreased from H1 to H5. The right side demonstrated significantly greater heights at H3 and H5. Gender-based trends showed generally higher insertion heights in females at certain sites, again, in agreement with Sharan et al. 13
Inter-group Comparison
Bone Thickness Among Groups
Bone thickness increased progressively from L1 to L5 across all the groups. Hypodivergent (Group A) subjects exhibited the highest IZC thickness, followed by Normodivergent (Group B) and Hyperdivergent (Group C) subjects. These differences are attributed to the variations in muscle function, skeletal architecture, and occlusal load patterns.6, 18, 19, 21
The findings of our study are consistent with previous studies demonstrating greater cortical bone thickness in hypodivergent individuals and reduced cortical bone thickness in hyperdivergent individuals.19, 21 However, they are inconsistent with Tavares et al. 22 and Ansari et al., 23 who reported no significant differences based on vertical skeletal patterns.
Insertion Heights Among Groups
Insertion heights decreased progressively from H1 to H5 across all groups. Hyperdivergent subjects exhibited the highest insertion heights, reflecting the dentoalveolar compensation pattern characteristic of long-face morphology.19, 24-26
These findings align with those of Kumar et al. 19 but differ from Tavares et al., 22 who found no association between insertion height and facial pattern.
Overall, the present study indicates that while vertical facial pattern, sex, and side-based differences do influence the IZC bone morphology, these factors alone may not be reliable predictors of bone availability for miniscrew placement. As such, individualized assessment using CBCT remains essential to accurately evaluate bone dimensions, determine the optimal insertion site and angle, and avoid potential complications. 27 This study also provides data for an underrepresented Maharashtrian Indian population. While trends are generally similar to East Asian and Caucasian populations, the findings underscore the need for population-specific CBCT assessment when planning IZC miniscrew placement. Despite anatomical variability, certain IZC locations consistently demonstrated adequate bone thickness and height across all groups, supporting their clinical reliability for extra-alveolar miniscrew insertion.
Although previous CBCT-based studies have evaluated IZC morphology in Indian populations, most have not specifically focused on Maharashtrian subjects or performed a comprehensive evaluation across multiple insertion angulations (40°-80°) in relation to vertical facial patterns. The present study uniquely integrates angulation-based assessment with facial pattern stratification, thereby providing clinically relevant guidance for individualized miniscrew placement.
Limitations
Although this study provides a comprehensive anatomical framework with respect to bone thickness, the clinical outcomes following placement of TSADs were not evaluated. The findings are anatomical and radiographic in nature, and extrapolation to clinical performance should be done cautiously. Additionally, the assumed effect size (f = 0.45) represents a large effect, and therefore, the study may be underpowered to detect smaller but clinically relevant differences. Future research incorporating clinical outcomes and larger and more diverse populations is recommended to validate these results and enhance their applicability in clinical orthodontics.
Conclusion
IZC bone morphology varies significantly with the vertical facial growth pattern. Hypodivergent individuals exhibited greater cortical bone thickness, whereas hyperdivergent individuals demonstrated greater insertion heights. Bone thickness increased, and insertion height decreased with increasing insertion angulation.
Footnotes
Authors Contribution
S.R.M.: Conceptualization, data acquisition, analysis, manuscript drafting.
S.T.D.: Study supervision, methodology, critical revision of the manuscript.
R.K.M.: Statistical guidance, interpretation of data, manuscript review.
All authors read and approved the final manuscript.
Data Availability Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflict of Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
Ethical approval for this study was provided by the Institutional Ethics Committee of C.S.M.S.S. Dental College and Hospital, Chhatrapati Sambhajinagar, India, on March 20, 2023 (approval number: CSMSS/DCH/EC/2023/ORTHO/03). Written informed consent was obtained from all participants prior to their inclusion in the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.