
Abstract
Introduction
Torque control of maxillary incisors is essential for esthetics and stability. In clear aligner therapy, torque expression is often unpredictable due to material and design limitations. Finite element method (FEM) analysis offers insights into optimizing aligner biomechanics.
Objectives
To evaluate the torque mechanics of maxillary incisors during anterior retraction with aligners alone and in combination with auxiliaries, including skeletal anchorage.
Methods
A cone beam computed tomography-derived finite element model of the maxilla and dentition was constructed. Five configurations were simulated: D1—aligner only, D2—aligner with ellipsoid attachment, D3—aligner with power ridge, D4—aligner with labial elastic from a mini-implant, and D5—aligner with linguoincisal elastic from a mini-implant. A 100 g bilateral retraction force was applied. Crown and root displacement of maxillary incisors and von Mises stress distribution in cortical and cancellous bone were analyzed.
Results
D1 exhibited uncontrolled tipping with a crown-to-root ratio of 411.11. D2 improved displacement (ratio 3.57), while D3 showed limited root control (ratio 214.81). D4 demonstrated a favorable root-dominant translation pattern (ratio 0.20) with maximum root displacement and highest but physiologically acceptable stress values. D5 also achieved favorable torque control (ratio 0.31) with slightly lower stress compared to D4.
Conclusions
Within the limitations of a single-anatomy proof-of-concept FEM model, the study shows that clear aligners alone are insufficient for effective torque expression. The addition of skeletal anchorage with elastics significantly enhances root control, with labial mini-implant-supported mechanics providing the most favorable outcomes. This hybrid approach expands the biomechanical efficacy of aligners in complex cases.
Introduction
Torque control, particularly of the maxillary incisors, is a critical component of orthodontic treatment that significantly influences esthetic outcomes and long-term stability. In fixed appliance systems, torque is managed predictably through bracket design, wire mechanics, and the use of auxiliaries. However, in clear aligner therapy (CAT), achieving effective and controlled torque remains a biomechanical challenge due to the limited force-couple systems inherent to thermoformed plastic aligners.1, 2
With the increasing adoption of aligners for comprehensive orthodontic treatment, including complex movements such as root torque, there is a growing need to understand and improve their biomechanical capabilities. Although recent advancements—such as optimized attachments, power ridges, and precision features—have aimed to enhance aligner force systems, clinical discrepancies persist between the planned and actual root movement, particularly in the labio-lingual inclination of the upper incisors.3, 4
Finite element method (FEM) analysis has emerged as a valuable tool in orthodontics, enabling detailed simulation of tooth movement, stress distribution, and force application under controlled conditions. It offers the ability to model complex biomechanical interactions between the aligner, tooth, periodontal ligament (PDL), and alveolar bone, thereby providing insights into optimizing appliance design.
The aim of this FEM-based study is to develop and analyze a biomechanically efficient system for improving the torque expression of maxillary incisors in CAT. By simulating various aligner modifications and attachment designs, the study seeks to identify configurations that enhance torque predictability and aligner performance.
Materials and Methods
This study was conducted in the Department of Orthodontics and Dentofacial Orthopaedics. EFORT biomechanical modeling guidelines were followed.
Data Acquisition and Sample Selection
Cone beam computed tomography (CBCT) data were obtained from a single adult patient who had undergone diagnostic imaging (CBCT) for therapeutic purposes. The patient met the following inclusion criteria: cervical vertebral maturation index stage 4-6, no history of orthodontic treatment, and absence of craniofacial syndromes. Exclusion criteria included multiple missing teeth, prior orthodontic treatment, or craniofacial anomalies. This study was designed as a proof-of-concept biomechanical investigation to isolate and compare force-system behavior under a single, idealized anatomical condition, thereby eliminating inter-patient variability and allowing a controlled comparison of auxiliary designs.
Image Processing and Model Development
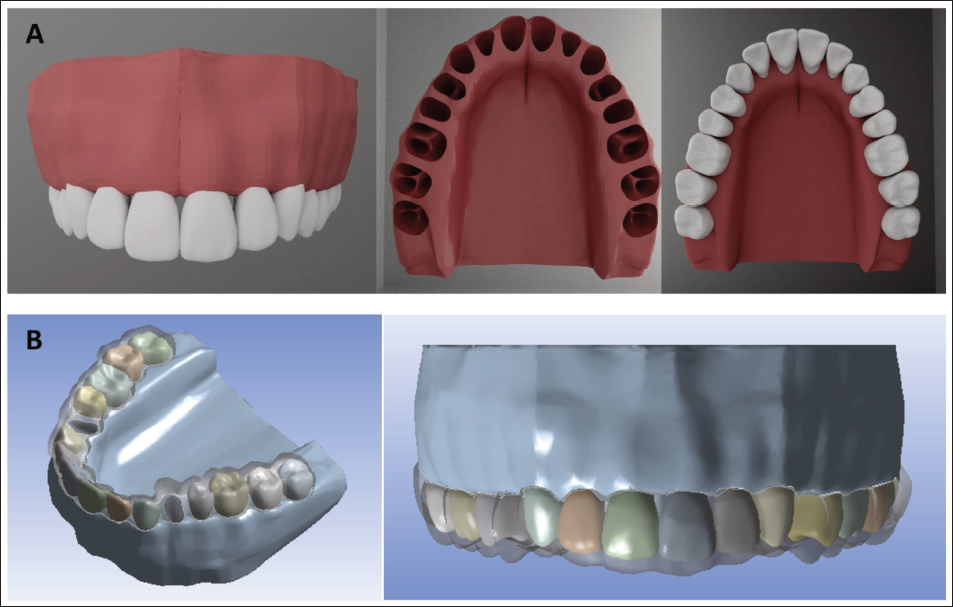
CBCT images (130 kV, 81 mAs, 0.5 mm slice increment, 512 × 512 resolution, 0.5 mm pixel size) encompassing the maxillofacial region (vertex to manubrium) were segmented using 3D Slicer (v4.7) and Seg3D (v2.1). The data were refined using CONTROL software, and DICOM files were converted to STEP format via CREO Parametric (v2.0) for geometric modeling. The final 3D models of the maxilla and dentition were processed using MIMICS and Fusion 360 (Figure 1).
(A) 3D Geometric Model Prepared from DICOM File; (B) Aligner Fabricated over Meshed Model.
Finite Element Model Construction
Five finite element models were developed, each representing a distinct clinical scenario of anterior tooth retraction following bilateral first premolar extraction (Figure 2):
D1: Clear aligner only (control). D2: Clear aligner with a horizontal ellipsoid attachment (3 mm height × 2 mm width × 1 mm thickness) on the maxillary central incisor. D3: Clear aligner with a power ridge on the maxillary central incisor. D4: Clear aligner with a labial elastic from a mini-implant placed labially to button on the maxillary central incisor. D5: Clear aligner with linguoincisal elastic from a mini-implant placed labially to the lingual precision cuts on the aligner.
(A) Frontal & Palatal View of Meshed D1 Model with Aligner; (B) Frontal & Palatal View of Meshed D2 Model with Aligner & Composite Attachment; (C) Frontal &; Palatal View of Meshed D3 Model with Aligner & Power Ridge; (D) Frontal &; Palatal View of Meshed D4 Model with Aligner and Mini Implant with Labial Elastics; (E) Frontal &; Palatal View of Meshed D5 Model with Aligner and Mini Implant with Linguoincisal Elastics.

Model meshing was performed using HyperMesh (v11.0, Altair Engineering, Troy, MI, USA). Material assignments were made based on established values in the literature, assuming isotropic, linear-elastic behavior. The element and node distribution across model components is provided in Table 1.
Number of Nodes and Elements in Model.

Material Properties
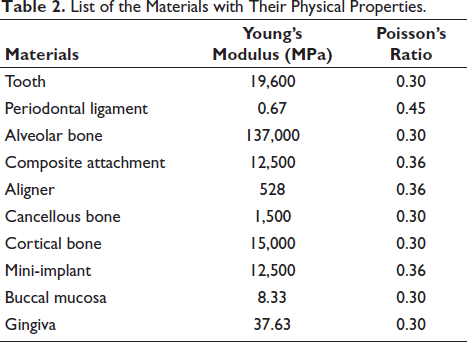
The elastic modulus and Poisson’s ratio for various anatomical and material components were derived from previously published data (Table 2). Bone mineral density values corresponding to D1 and D2 bone quality were incorporated into the simulations. The PDL was modeled as a homogeneous, isotropic, linear-elastic material with a Young’s modulus of 0.67 MPa and a Poisson’s ratio of 0.45, consistent with widely adopted orthodontic finite element studies. Although the PDL exhibits viscoelastic behavior in vivo, a linear-elastic approximation was selected to permit controlled, instantaneous comparison of force-system behavior across different aligner–auxiliary configurations under identical loading conditions, which was the primary objective of the present study. A linear-elastic approximation allows standardized comparison across different biomechanical configurations by eliminating the confounding effects of stress relaxation and remodeling.
List of the Materials with Their Physical Properties.
Boundary Conditions and Loading Protocol
All models were solved using ANSYS (v20.1, Swanson Analysis Inc., Houston, PA, USA). A retraction force of 100 g was applied bilaterally to the maxillary anterior teeth to simulate en-masse retraction following premolar extractions. The contact interfaces were defined using bonded or frictional interactions based on anatomical relevance. All degrees of freedom were restricted at the superior and posterior borders of the maxilla to simulate craniofacial stability.
Outcome Measures
The primary outcomes evaluated included stress distribution (von Mises stress) and root displacement of the maxillary central incisors across all groups. Comparative analysis of different auxiliary configurations was performed to assess the influence on anterior tooth torquing mechanics. In the present study, torque was assessed indirectly using crown-to-root displacement ratios, which provide a surrogate indicator of tipping versus bodily movement. A lower ratio suggests greater root control and a tendency toward translation, whereas a higher ratio indicates uncontrolled tipping.
Results and Observations
Finite element analysis was performed to evaluate the torque expression of maxillary incisors in CAT using five different configurations of clear aligners and auxiliaries (Models D1-D5). A retraction force of 100 g was applied bilaterally in each model, and the crown and root displacements of the maxillary central and lateral incisors were measured. A retraction force of 100 g was selected as it lies within the clinically accepted optimal force range for anterior tooth retraction and torque control, as reported in orthodontic biomechanics literature. Forces in the range of 75-150 g are considered sufficient to produce effective tooth movement while minimizing the risk of hyalinization and excessive stress concentration. Additionally, the von Mises stresses generated in the cortical and cancellous bone were analyzed (Figures 3-7).
(A) Frontal & Palatal View of Deformation Pattern on Composite D1 Model; (B) Deformation Levels in Aligner in D1; (C) Stress Levels in Cancellous Bone in D1 Models; (D) Stress Levels in Cortical Bone in D1 Mode; (E) Deformation in Crown and Root in D1 Models.

(A) Frontal & Palatal View of Deformation Pattern on Composite Model (D2); (B) Deformation Levels in Aligner in D2 Model; (C) Stress Levels in Cortical & Cancellous Bone in D2 Models; (D) Deformation in Crown and Root in D2 Model.

(A) Frontal & Palatal View of deformation Pattern on Composite Model(D3); (B) Deformation Levels in Aligner in D3 Models; (C) Stress Levels in Cortical & Cancellous Bone in D3 Models; (D) Deformation in Crown and Root in D3 Model.

(A) Frontal & Palatal View of Deformation Pattern on Composite Model (D4); (B) Deformation Levels in Aligner in D4 Model; (C) Stress Levels in Cortical & Cancellous Bone in D4 Models; (D) Deformation in Crown and Root in D4 Model.

(A) Frontal & Palatal View of Deformation Pattern on Composite Model (D5); (B) Deformation Levels in Aligner in D5 Models; (C) Stress Levels in Cortical & Cancellous Bone in D5 Models; (D) Deformation in Crown and Root in D5 Model.

Tooth Displacement and Crown-to-Root Ratios
The crown and root displacements for each model are summarized in Table 3. The highest crown displacement was observed in Model D3 (1.16 × 10⁻6 m), and the lowest in Model D5 (0.14 × 10⁻6 m). Root displacement was minimal in Model D1 (0.003 × 10⁻6 m), corresponding to a crown-to-root ratio of 411.11, indicating excessive uncontrolled tipping.
Deformation Values for Crown and Root with 100 g Force.

In contrast, Model D4 showed the highest root movement (0.59 × 10⁻6 m) with a crown-to-root ratio of 0.20. Similarly, Model D5 displayed a favorable ratio of 0.31, indicating efficient torque control.
Model D2, with ellipsoid attachments, improved the displacement pattern (ratio: 3.57) compared to the control. Model D3, though showing a slightly greater crown movement, still had a high crown-to-root ratio (214.81), indicating limited root movement.
Stress Distribution
The von Mises stress values generated in the cortical and cancellous bone are presented in Table 4. Model D1 demonstrated the lowest stress values in both cortical (0.064 MPa) and cancellous bone (0.025 MPa), corresponding with its minimal root movement and predominantly tipping movement. In contrast, Model D4 exhibited the highest stress in both cortical (0.094 MPa) and cancellous bone (0.093 MPa), which correlated with maximum root displacement, indicating increased force transmission to the supporting bone structures.
Cortical and Cancellous Stress Values for Crown and Root with 100 g Force.
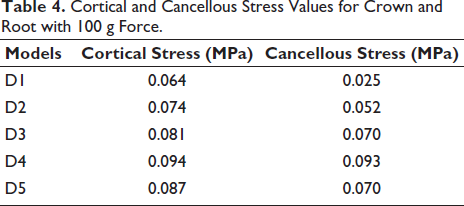
Model D5, utilizing linguoincisal elastics, also showed elevated stress levels (cortical: 0.087 MPa, cancellous: 0.070 MPa) along with controlled root movement, suggesting effective force distribution without excessive concentration.
Comparative Analysis
Among all five configurations, Model D4 (mini-implants with labial elastics) demonstrated the most favorable root movement and the highest stress transmission to the supporting structures, indicating effective torquing of the incisors. Model D5 also exhibited a favorable biomechanical response, with slightly reduced stress compared to D4. Conversely, Model D1 showed the least desirable outcome, with minimal root movement and low stress values, indicative of uncontrolled tipping.
Discussion
This FEM study sought to analyze the biomechanical effects of different auxiliary configurations on the torque expression of maxillary incisors using clear aligners. Through comparison of crown and root displacement patterns and stress distribution in the alveolar bone, the study provides critical insights into the limitations of aligners alone and the benefits of adjunctive mechanics—particularly skeletal anchorage via mini-implants.
Clear Aligners Alone: Limitations in Root Control
Model D1, which used clear aligners without any auxiliary features, exhibited a crown-to-root displacement ratio of 411.11, indicating significant uncontrolled tipping. This finding aligns with a large body of literature suggesting that clear aligners, while effective for mild to moderate tooth movements, struggle to generate adequate moment-to-force ratios necessary for root control in complex movements such as en-masse retraction or torque application.5-7 The limited contact area between the aligner and tooth surface, along with the material properties of thermoplastic polymers (low stiffness and elastic recovery), contributes to diminished transmission of targeted forces to the root apex.8, 9
In line with these mechanical constraints, FEM studies by Kravitz et al. 5 and Hahn et al. 9 demonstrated that aligners alone are inadequate for torqueing maxillary incisors and often result in uncontrolled tipping and insufficient root translation—posing risks for root resorption, compromised esthetics, and periodontal stress.
Effect of Attachments and Power Ridges
Model D2, which employed ellipsoid composite attachments, showed improved root engagement with a crown-to-root ratio of 3.57. These attachments serve as “handles” that increase the mechanical interlock between the aligner and the tooth surface, thereby enhancing force application efficiency and rotational control. 8 Although some degree of tipping persisted, the improvement over the control model supports their clinical use in improving force systems.
Model D3, designed with power ridges—strategically placed engineered corrugations on the aligner—yielded a high crown-to-root ratio of 214.81, similar to the control. While power ridges are purported to enhance torque by distributing forces across the incisal third and gingival margin, their clinical efficacy remains controversial. Studies by Simon et al. 6 and Elkholy et al. 10 have shown that power ridges may be insufficient to produce significant lingual root torque without reinforcement, especially in extraction cases requiring bodily retraction.
The difference in torque efficiency observed between the ellipsoid attachment (D2) and the power ridge configuration (D3) can be explained by differences in force-vector geometry and moment-arm effectiveness (Figure 8) rather than attachment presence alone.

Ellipsoid attachments increase the effective contact surface area between the aligner and the tooth, improving mechanical interlock and reducing aligner slippage. This allows the aligner to generate a more stable force couple, producing a moment arm closer to the center of resistance of the maxillary incisor. As a result, D2 demonstrated improved root engagement and a substantially reduced crown-to-root ratio compared to the control model.
In contrast, power ridges rely primarily on controlled deformation of the thermoplastic aligner material along the incisal and gingival margins. During anterior retraction in extraction cases, the retraction force is applied coronally, and the deformation induced by power ridges alone is insufficient to counteract the tipping moment generated by this force vector. Consequently, D3 exhibited excessive crown displacement with minimal root movement, resulting in an unfavorable crown-to-root ratio despite the presence of a torque-enhancing feature.
These findings suggest that, in extraction mechanics, attachment designs that establish a true force couple through enhanced aligner–tooth interlock may be biomechanically superior to features that depend predominantly on aligner material deformation.
These findings align with the findings of Sandhya et al. 11 FEM demonstrating ellipsoid attachment root displacement of 75.00 × 10⁻6 mm versus power ridge of 72.7 × 10⁻6 mm, while resolving the apparent discrepancy with the systematic review by Pandian et al., 12 noting equivalence only for mild torque corrections (<5°).
Skeletal Anchorage with Elastics: A Paradigm Shift
The most favorable results emerged from Models D4 and D5, which incorporated mini-implants with labial and linguoincisal elastic attachments, respectively. Model D4 demonstrated a crown-to-root ratio of 0.20, while Model D5 followed closely at 0.31, indicating a favorable root-dominant translation pattern. Root displacement was highest in these models, which was corroborated by higher von Mises stress values in both cortical and cancellous bone, suggesting effective transmission of forces to the alveolar structures. Although such movement enhances root engagement, excessive root dominance may increase the risk of intrusion and apical stress concentration if applied clinically without appropriate force modulation.
Mini-implants provide absolute anchorage, allowing orthodontic forces to be delivered with precision while minimizing reactive forces on adjacent teeth.13, 14 Elastics connected to skeletal anchorage act closer to the tooth’s center of resistance, creating a force vector that favors translation rather than tipping. This was clearly reflected in the displacement patterns observed in D4 and D5. Although both models demonstrated superior anchorage control compared to D1-D3, the D4 model emerges as biomechanically superior for torque control. This is in contrast to a previous study by Liu et al., 15 which concluded that linguoincisal elastics are superior to labial elastics. In D4, the elastic was attached directly to the tooth, elevating the force application point in line with the center of resistance. This created a favorable moment-to-force ratio, enhancing lingual root torque and promoting bodily retraction. The skeletal anchorage minimized reciprocal forces, allowing efficient force transfer to the root apex without compromising posterior anchorage.
In D5, the elastic was attached to the aligner surface, introducing variability in force transmission. Thermoplastic aligners may deform or flex under elastic traction, especially when attached closer to the gingival margin. This reduces the effective moment arm and increases the risk of uncontrolled tipping, compromising root control.
The aligner material was modeled as linear-elastic and time-independent; however, in clinical conditions, thermoplastic materials exhibit viscoelastic deformation, stress relaxation, and force decay. This may reduce effective force transmission in aligner-mediated mechanics such as D5, thereby diminishing torque expression.
Additionally, FEM assumptions such as a perfect fit, the absence of aligner slippage, and simplified material properties may further influence force delivery patterns. These factors could collectively explain the observed deviation from previously reported findings.
Therefore, the superior performance of D4 in this model should be interpreted in the context of direct force application versus aligner-mediated force transmission, rather than as a definitive contradiction of existing literature.
Stress Analysis and Biological Implications
Bone stress analysis further reinforces these findings. Model D1, with minimal root displacement, showed the lowest stress levels in both cortical (0.064 MPa) and cancellous bone (0.025 MPa), consistent with its ineffective force application. On the other hand, Model D4 recorded the highest bone stress values (cortical: 0.094 MPa; cancellous: 0.093 MPa), corresponding to its superior root movement.
It is essential to note that all stress values remained well within the physiological limits defined for orthodontic forces, typically below 0.1 MPa for safe bone remodeling without necrosis or resorption.16, 17 The uniform stress distribution in Models D4 and D5 suggests a more harmonious load application, potentially reducing the risk of undesirable biological responses.
Additionally, it has been hypothesized that controlled stress in cortical bone stimulates bone turnover and enhances PDL remodeling, facilitating more predictable and efficient tooth movement. 18 Hence, moderate stress elevation—such as seen in D4 and D5—may be desirable rather than detrimental.
Clinical Relevance
From a clinical standpoint, the findings of this study provide valuable direction for the treatment planning of cases requiring torque control. While clear aligners alone offer esthetic and hygiene benefits, their biomechanical limitations are apparent in scenarios requiring bodily movement or torque. Attachments and power ridges may provide some assistance, but their efficacy is limited.
The integration of skeletal anchorage via mini-implants, especially when combined with directional elastics, emerges as a powerful adjunct to aligner therapy. This hybrid approach combines the esthetic advantages of aligners with the biomechanical control of fixed appliances—broadening the scope of treatable malocclusions within clear aligner systems.
The findings emphasize that even with the use of skeletal anchorage, auxiliary design and force delivery mechanics (the point of elastic attachment) play a vital role in treatment outcomes. D4 offers a more predictable and controlled movement pattern, making it the preferable option for clinicians aiming to achieve root torque and bodily retraction using aligners in extraction space closure. In extraction cases, clear aligners alone tend to apply a retraction-extrusion force, which increases the risk of crown tipping and lingual inclination due to the coronal position of force application. This may compromise torque expression and vertical control, particularly in patients with a deep bite or proclined incisors. The incorporation of mini-implants with elastics significantly alters the force vector by adding an intrusive component. This promotes more favorable bodily tooth movement with lingual root torque and reduces undesirable extrusion.
Although Model D4 demonstrated superior torque control, Model D5 exhibited lower peak stress with comparable root engagement. Clinically, D4 may be preferred in cases demanding maximum biomechanical control, while D5 may offer advantages in patient comfort, esthetics, and stress moderation. The labial configuration may be easier to manage clinically, although it is more visible. The choice between the two could, therefore, be tailored based on esthetic preferences and clinical goals (Table 5).
Clinical Summary.

Clinical Translation and Validation Pathway
Finite element analysis is inherently limited in its ability to directly replicate the complex biological processes governing orthodontic tooth movement, including PDL remodeling, bone turnover, and time-dependent force decay. Consequently, FEM results should be interpreted as indicators of biomechanical feasibility and relative efficiency rather than exact predictors of in vivo displacement magnitude. A prospective clinical validation study is planned as a subsequent phase of this investigation. This will involve CBCT and digital model superimposition before and after anterior retraction using aligners with mini-implant-supported elastics. Predicted displacement vectors and torque changes will be compared with observed clinical outcomes to assess translational accuracy. Based on prior orthodontic FEM validation studies, the expected prediction error is anticipated to fall within the reported range of 0.36%-8.96%.
Limitations and Future Directions
While FEM provides precise control over variables and eliminates patient-related confounders, this study is inherently limited by its static nature and the assumption of isotropic, homogeneous material properties. The complex biological environment of the oral cavity—featuring dynamic bone remodeling, PDL viscoelasticity, and patient variability—cannot be fully replicated in silico. The aligner material was modeled as linear-elastic and time-independent; therefore, the findings represent the initial biomechanical response rather than long-term intraoral force decay associated with thermoplastic stress relaxation. The assumption of linear-elastic PDL behavior implies that the present results represent the initial displacement phase of tooth movement rather than the long-term biological response. Consequently, the magnitude and pattern of torque expression observed in this study reflect the immediate mechanical response to applied forces. Therefore, torque efficiency—particularly differences between configurations—should be interpreted as relative biomechanical performance rather than absolute clinical movement.
Moreover, the study utilized a single patient’s CBCT scan, limiting generalizability. Future research should incorporate patient-specific modeling, dynamic time-based simulations, and validation with clinical outcomes to improve translational relevance. While crown-to-root displacement ratios provide a useful indication of tipping versus root-dominant movement, they do not fully characterize true torque, which is an angular phenomenon. The absence of direct angular measurements and M/F ratio calculations limits precise biomechanical quantification of torque. Experimental studies and randomized trials comparing aligners with and without mini-implant-supported elastics would further substantiate these findings.
Conclusion
Within the limitations of a single-anatomy proof-of-concept FEM model, mini-implant-supported elastic mechanics demonstrated superior biomechanical efficiency for torque control compared to aligner-only and attachment-based systems.
This FEM study demonstrated that while clear aligners alone result in uncontrolled tipping and insufficient root movement, the addition of skeletal anchorage with elastics—either labial or linguoincisal—significantly improves root control and facilitates bodily movement during anterior retraction. Among the five models, mini-implant-supported elastics attached to the tooth provided the most favorable biomechanical environment, with optimal crown-to-root ratios and physiologically safe stress distributions. These findings support the integration of skeletal anchorage systems in aligner therapy, particularly in complex orthodontic cases requiring high degrees of control.
Footnotes
Authors Contribution
Dr. Priyank Rai: Conceptualization, project administration, supervision.
Dr. Sandeep Kumar: Data Curation, formal analysis, software.
Dr. Tulika Tripathi: Project administration, writing—review and editing.
Dr. Anup Kanase: Writing—review and editing.
Dr. Anshika Gandhi: Writing—original draft, writing—review and editing.
Data Availability
3D models available upon request from the corresponding author.
Declaration of Conflict of Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was obtained from the Institutional Research Ethics Committee (File no. EC/NEW/INST/2020/1207).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent was obtained from all participants.