
Abstract
Background
Orthodontic force application induces an inflammatory response in periodontal tissues, resulting in bone remodeling. Gingival crevicular fluid (GCF) provides a non-invasive medium to evaluate these biological changes. With the increasing use of clear aligner therapy, it is clinically relevant to compare its biological effects with those of fixed orthodontic appliances.
Aim
To systematically review and compare biomarker levels in GCF among patients treated with clear aligners and fixed orthodontic appliances.
Materials and Methods
Electronic searches were conducted in PubMed, Cochrane Central, Web of Science, Scopus, LILACS, and Google Scholar from January 1, 2000, to June 30, 2025. Clinical studies evaluating GCF biomarkers during active orthodontic treatment with clear aligners or fixed appliances were included. Risk of bias was assessed using the Cochrane RoB tool and ROBINS-I. Meta-analysis was performed using a random-effects model.
Results
Ten studies (six randomized controlled trials, two non-randomized trials, and two observational studies) involving 380 participants were included. Clear aligner therapy was associated with higher levels of interleukin-2, interleukin-6 (IL-6), and interleukin-8, while fixed appliances demonstrated elevated tumor necrosis factor-alpha and IL-6 levels. Meta-analysis of IL-1β levels revealed no statistically significant difference between the two groups (SMD = 1.11; 95% CI = −2.54 to 4.77; P = .55). Substantial heterogeneity was observed (I2 = 98%).
Conclusion
Both clear aligners and fixed orthodontic appliances elicit inflammatory responses during active treatment, reflected by increased GCF biomarker levels. While cytokine expression patterns differ between modalities, current evidence does not establish a clear association with the rate of tooth movement. Due to the high heterogeneity, the findings should be interpreted cautiously, and further standardized longitudinal studies are required.
Introduction
Orthodontic tooth movement is an intricate process, beginning with the application of force that enables a tooth to shift beyond its normal range of movement during activities like chewing. Throughout orthodontic tooth movement, various elements of the periodontium, such as alveolar bone, gingiva, periodontal ligament, and, to a certain extent, cementum, are subjected to remodeling. 1 Currently, due to the increasing emphasis on esthetics among patients, there is a wide range of options available in the market for achieving orthodontic tooth movement. Among these options, clear aligners stand out as the most esthetically pleasing choice for correcting mild to moderate malocclusions, particularly in adult patients who prioritize their appearance. 2
Kuncio et al. 3 suggested that the movement of teeth with aligners differs from the conventional stages of movement described by Krishnan and Davidovitch, 4 primarily because of the intermittent forces applied by the aligners. However, even though these forces are perceived as intermittent by the periodontium due to its viscoelastic nature,5, 6 they still effectively produce orthodontic tooth movement with minimal cell damage.7, 8
Clear aligner therapy delivers orthodontic forces through removable polymer-based appliances, producing distinct force application patterns compared to fixed appliances, which may influence periodontal inflammatory responses.9-12
The application of orthodontic forces by aligners and fixed appliances triggers vasodilation in periodontal capillaries, leading to the migration of inflammatory cells and subsequent cytokine production. These cytokines play a pivotal role in bone remodeling and are reflected in gingival crevicular fluid (GCF), which serves as a non-invasive indicator of periodontal biological activity during orthodontic treatment.13-20
To date, no systematic review has comprehensively compared GCF biomarker levels between patients treated with clear aligners and those treated with fixed orthodontic appliances. Therefore, this systematic review aims to compare biomarker levels in GCF between these two treatment modalities.
Materials and Methods
Protocol and Registration
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines. The review protocol was registered in the PROSPERO database (registration number is provided on the title page).
Eligibility Criteria and Clinical Standardization
Studies were selected based on the following criteria:
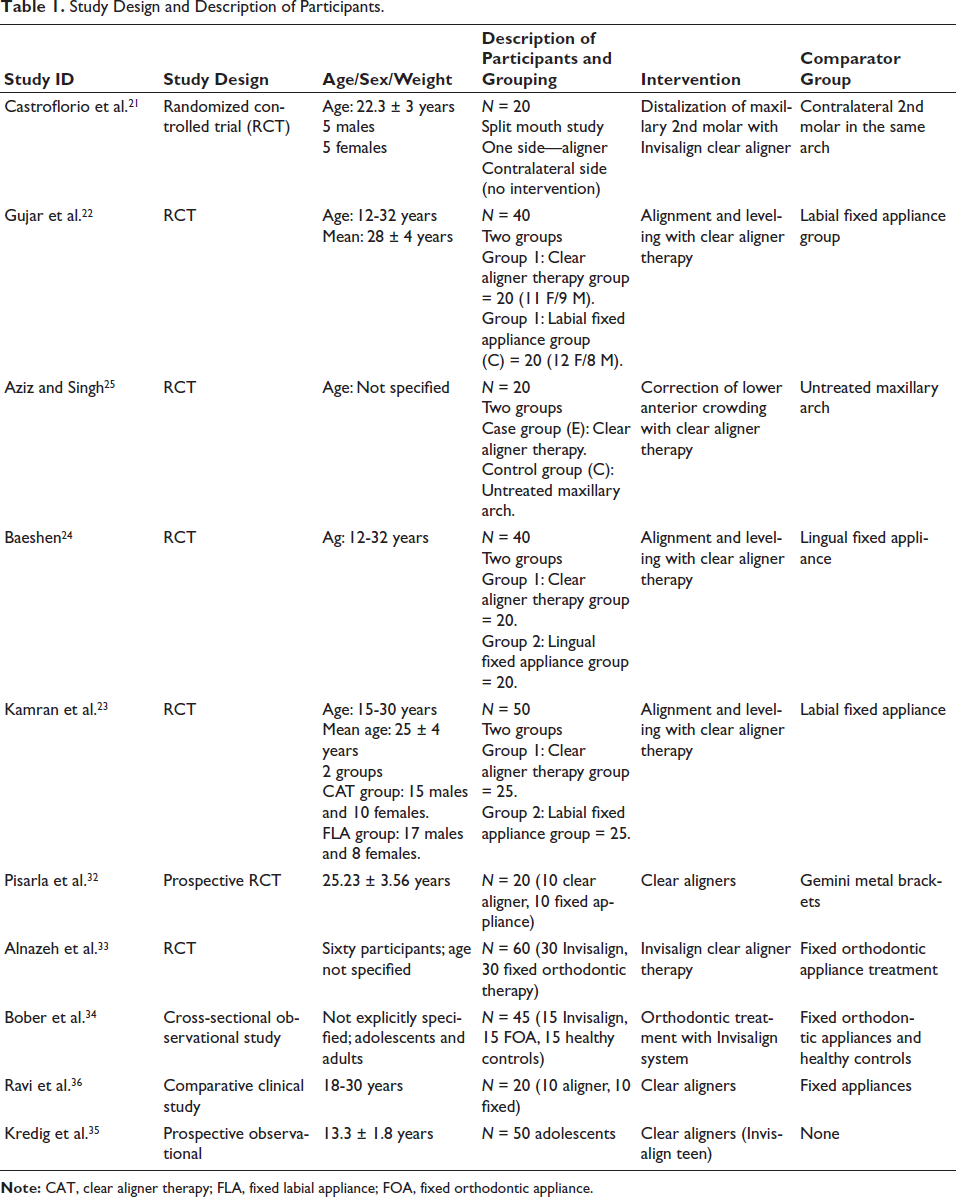
Population: Human subjects undergoing orthodontic treatment. Intervention: Clear aligner therapy using removable aligner systems. Comparator: Fixed orthodontic appliances (labial or lingual). Outcomes: Quantitative assessment of inflammatory or bone metabolism biomarkers in GCF. Study design: Randomized controlled trials, non-randomized clinical trials, and observational studies (Table 1).
Study Design and Description of Participants.
GCF samples were required to be collected during the active phase of orthodontic treatment following initiation of orthodontic force. Studies assessing samples exclusively during retention or post-treatment phases were excluded.
Only studies involving periodontally healthy participants at baseline were included. Most studies reported gingival and plaque indices and provided standardized oral hygiene instructions before GCF collection; however, variations existed in oral hygiene protocols and clinical indices used. Although most studies attempted to standardize periodontal conditions before sampling, the lack of uniformity in gingival indices and oral hygiene protocols may have influenced baseline inflammatory biomarker levels.
Methodological variability was noted in GCF analysis techniques. Enzyme-linked immunosorbent assay (ELISA) was the most common method, while some studies used proteomic approaches such as MALDI-TOF/MS. Differences in sampling duration, storage, assay sensitivity, and analytical protocols may have influenced biomarker levels. These methodological variations may partly explain the wide dispersion of reported biomarker values and contribute to the substantial heterogeneity observed in the meta-analysis.
Information Sources and Search Strategy
A comprehensive search was conducted in PubMed, Cochrane Central, Web of Science, Scopus, LILACS, and Google Scholar from January 1, 2000, to June 30, 2025. Manual searches of orthodontic journals and ClinicalTrials.gov were also performed. Brand names were included solely to ensure comprehensive literature retrieval. The search strategy was developed using relevant Medical Subject Headings terms, keywords, and the Boolean operators “AND” and “OR” in combination. The following search terms and their combinations were used in the search strategy: “Clear aligner therapy,” “Aligner,” “Aligner treatment,” “Invisalign,” “Orthodontic tooth movement,” “Conventional appliance,” “Fixed appliances,” “Labial fixed appliances,” “Lingual fixed appliances,” “Biomarkers,” “Bone remodeling,” “Cytokines,” “Interleukin,” “Inflammatory biomarkers,” “GCF” with Boolean characters “AND” and “OR” combination. The search strategy was adapted to the specific syntax and subject headings of each electronic database. Using the Boolean operators AND/OR, the following Boolean formulas were worded:
Boolean formula #1: ((Orthodont* OR clear OR removable) AND aligner*) OR (Invisalign®). Boolean formula #2: Conventional orthodontic treatment OR traditional orthodontic treatment OR brace* OR bracket* OR fixed appliance*.
Boolean formula #3: #1 AND #2.
Study Selection
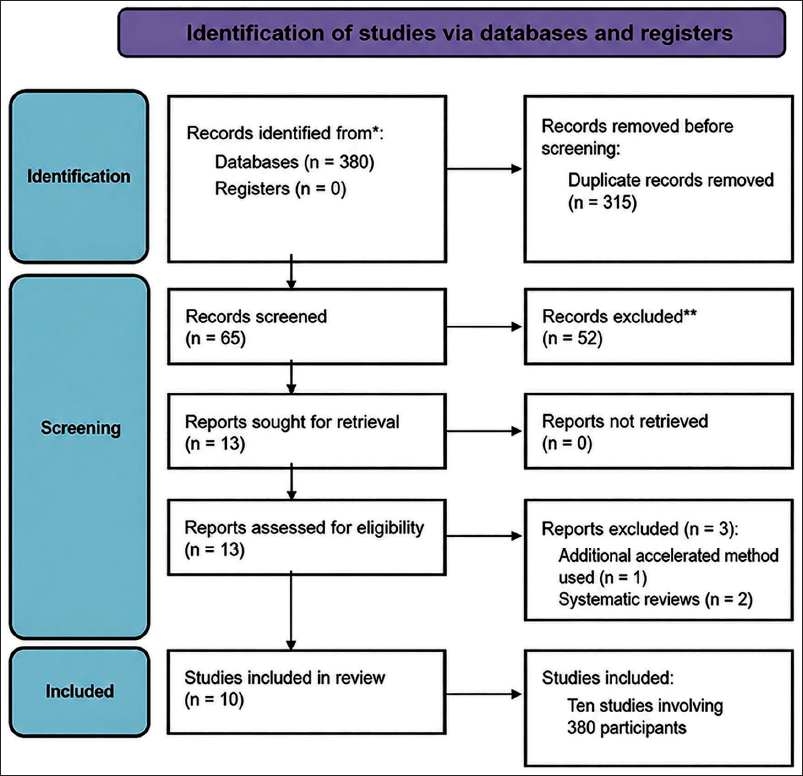
The study selection process adhered to the PRISMA 2020 flow diagram, which outlines the number of records identified, screened, excluded, and included (Figure 1). Two reviewers independently screened titles, abstracts, and full texts. Inter-reviewer agreement was high (Cohen’s kappa > 0.89). Discrepancies were resolved through discussion or consultation with a third reviewer.
Data Extraction
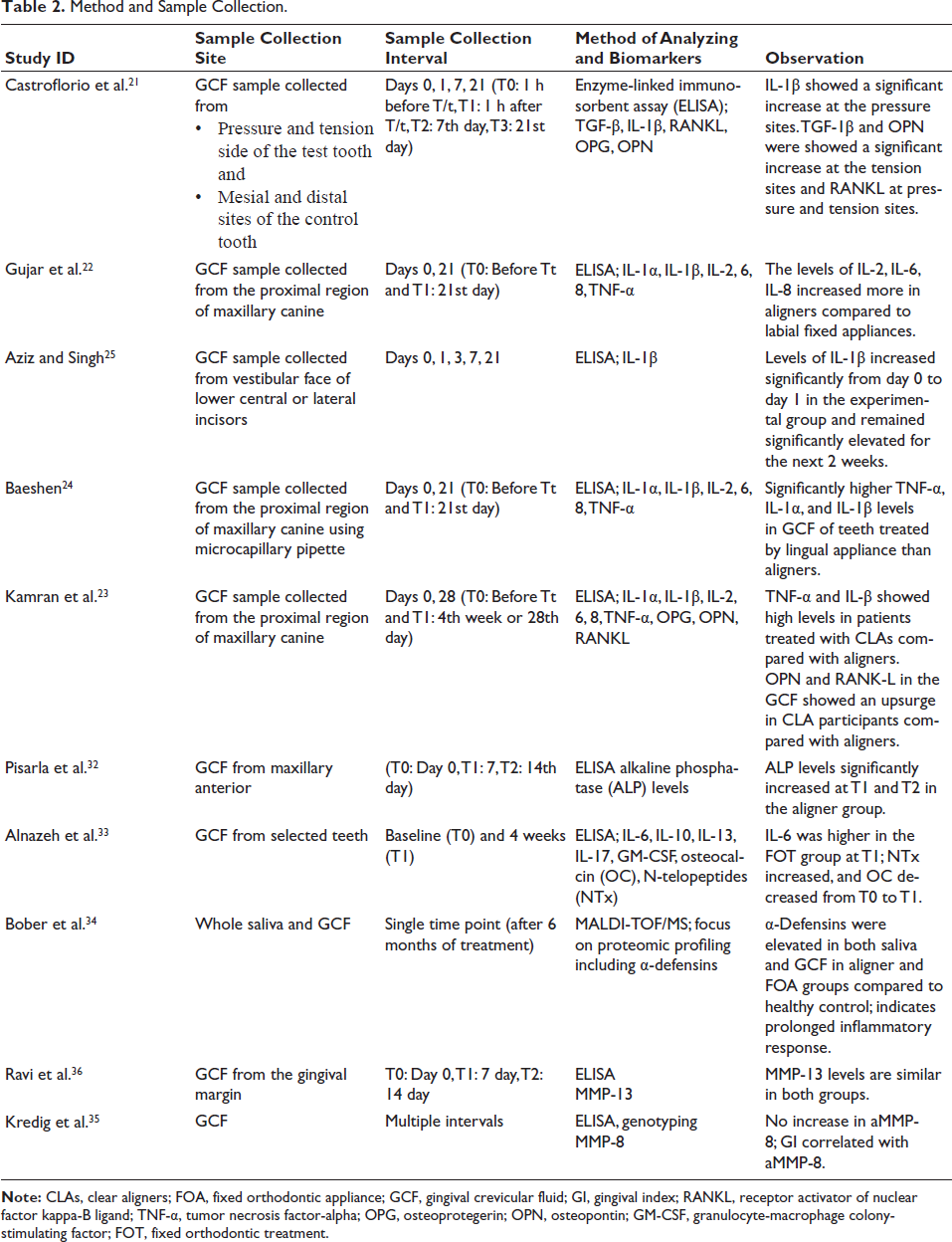
Data were extracted independently by two reviewers using standardized forms, including study characteristics, participant details, GCF sampling protocols, biomarkers analyzed, and outcomes (Table 2).
Risk of Bias Assessment
Risk of bias was assessed using the Cochrane Risk of Bias tool for randomized studies and ROBINS-I for non-randomized studies. The methodological quality of each study was classified as low, high, or unclear risk. Publication bias was explored using funnel plots; formal testing was not performed due to the limited number of studies.
Statistical Analysis
Meta-analysis was performed using a random-effects model in RevMan 5.4. Heterogeneity was assessed using the I2 statistic. Standardized mean differences with 95% confidence intervals were calculated for continuous outcomes.
Results
Study Selection and Characteristics
Ten studies involving 380 participants were included. After adjusting the duplicates, 65 articles were scrutinized for inclusion in the study. The majority of them were excluded as they did not have relevant titles and abstracts, leaving only 13 articles after retrieval. Out of 13 articles, three articles were excluded because one of them used an additional accelerated method, in addition to the aligner treatment, in the study group, and the other two were systematic reviews. Finally, 10 articles were selected for full-text review and abstracted, with the following information: sample size and characteristics, GCF collection protocol, type of control, and biomarkers identified. The PRISMA flowchart of the electronic database search is represented in Figure 1.
Participants ranged in age from 12 to 32 years. Biomarkers analyzed included interleukins, tumor necrosis factor-alpha (TNF-α), alkaline phosphatase, matrix metalloproteinases, and defensins.
Risk of Bias
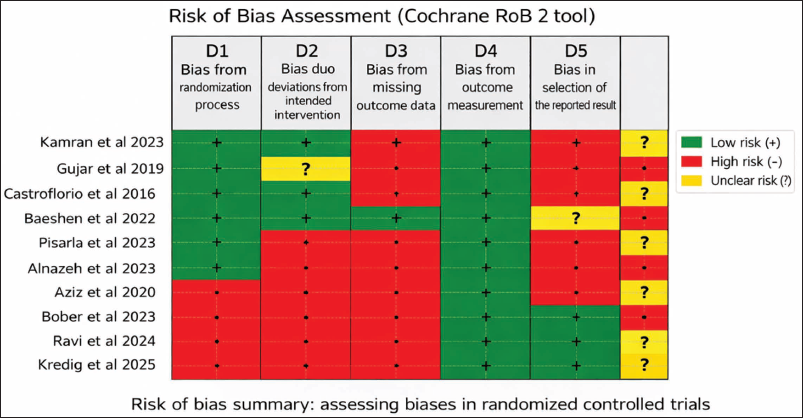
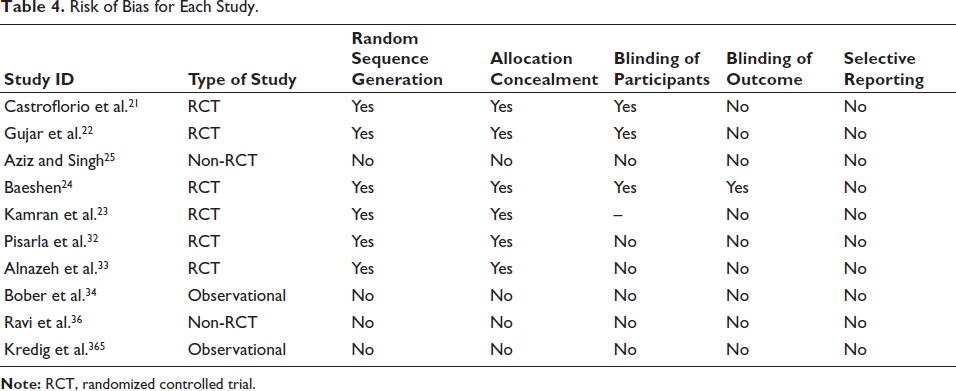
The detailed risk of bias assessment of included studies is summarized in Table 4. The risk of bias assessment for all studies was summarized in Figure 2 and Table 3. Most studies exhibited a high or unclear risk in random sequence generation and allocation concealment. Blinding was limited due to the nature of the interventions. Outcome assessment was blinded in eight studies.
It Shows the Risk of Bias Assessment Using the Cochrane RoB 2 Tool, Which was Applied Due to Its Relevance in Assessing Bias in Randomized Controlled Trials.
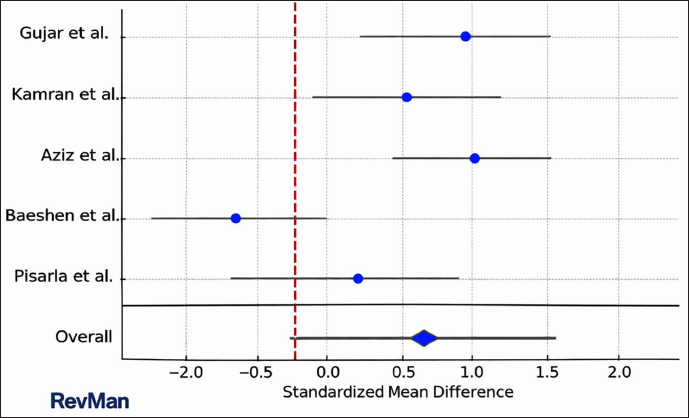
Forest Plot of IL-1β Levels Comparing Aligners Versus Fixed Appliances Includes All Relevant Meta-analyses, Generated by RevMan.
Method and Sample Collection.
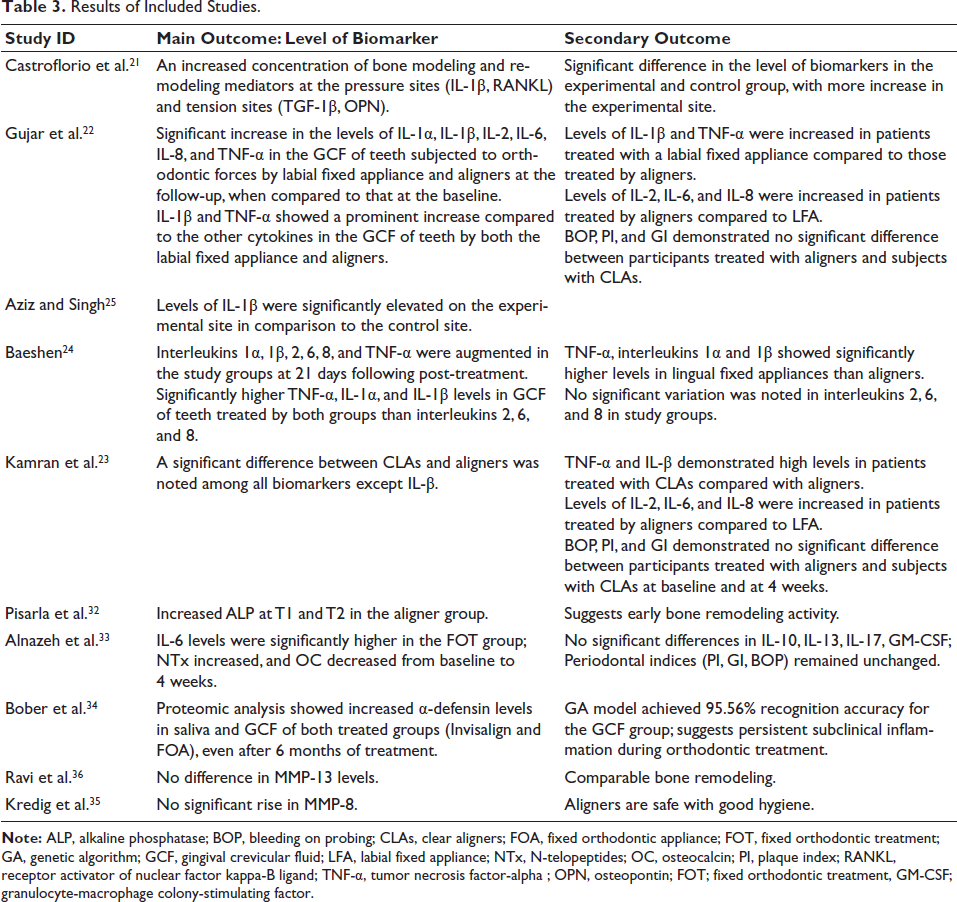
Results of Included Studies.
Risk of Bias for Each Study.
The results of the overall comparison have been depicted as a forest plot (Figure 3).
Meta-analysis and Heterogeneity
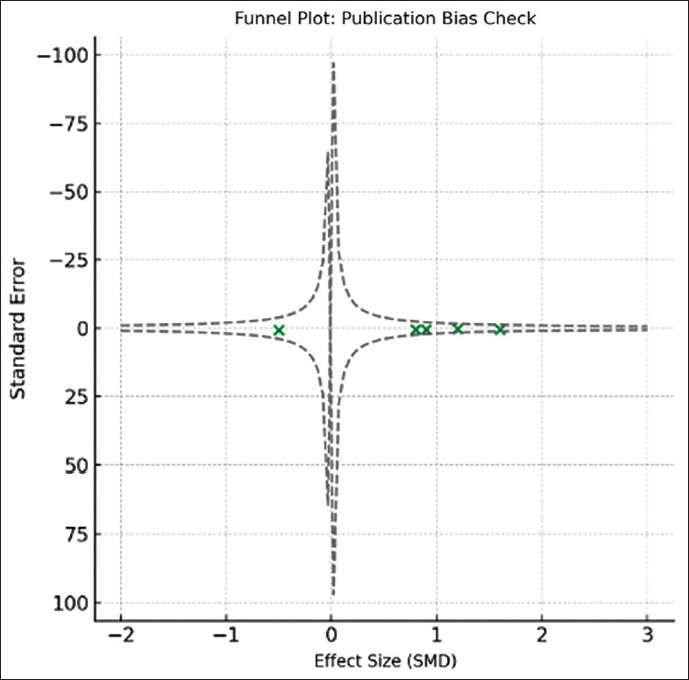
Meta-analysis of IL-1β levels demonstrated no statistically significant difference between aligner and fixed appliance groups (SMD = 1.11; 95% CI = −2.54 to 4.77; P = .55). Substantial heterogeneity was observed (I2 = 98%), reflecting clinical and methodological variability. Therefore, the pooled quantitative estimates should not be interpreted as definitive evidence of the biological superiority of either clear aligners or fixed orthodontic appliances. The funnel plot showed a possibility of publication bias since it shows an asymmetrical distribution of the studies considered (Figure 4).
Funnel Plot Showing Absence of Publication Bias.
Biomarker Outcomes
Clear aligner therapy was associated with higher interleukin-2 (IL-2), interleukin-6 (IL-6), and interleukin-8 (IL-8) levels, whereas fixed appliances demonstrated elevated TNF-α and IL-6. Proteomic analyzes revealed persistent elevation of α-defensins in both groups, suggesting sustained low-grade inflammation (Table 3).
Discussion
The primary purpose of this systematic review was to summarize and compare the evidence from clinical studies evaluating the effect of clear aligner therapy and fixed orthodontic appliances on biomarker levels in GCF. Thorough screening of the literature yielded 10 human studies, all of which demonstrated an increase in inflammatory and bone metabolism biomarkers following orthodontic force application, irrespective of the type of appliance used. This finding supports the established biological concept that orthodontic tooth movement is mediated by a controlled inflammatory response within the periodontal tissues.
The application of orthodontic forces through aligners and fixed appliances initiates a cascade of biological events involving the activation of inflammatory cells and the release of cytokines, chemokines, prostaglandins, and enzymes associated with alveolar bone remodeling. 26 Cytokines such as interleukin-1 (IL-1), IL-2, IL-6, IL-8, and TNF-α play a central role in regulating osteoclastic activity and periodontal ligament remodeling during orthodontic tooth movement.27–30
Basaran et al. 31 reported increased levels of IL-2, IL-6, IL-8, TNF-α, and IL-1β during orthodontic treatment, highlighting the role of pro-inflammatory mediators in bone resorption. Similarly, Castroflorio et al. 21 observed elevated levels of IL-1β and receptor activator of nuclear factor kappa-B ligand (RANKL) at pressure sites during early orthodontic tooth movement with clear aligners, indicating active bone remodeling. These findings are consistent with the results of the present review, which showed elevated inflammatory mediator levels during both aligner-based and fixed orthodontic therapy.
Gujar et al. 22 compared cytokine levels between patients treated with clear aligners and labial fixed appliances and reported significantly higher levels of IL-2, IL-6, and IL-8 in the aligner group. Kamran et al. 23 similarly observed higher TNF-α and IL-1β levels in patients treated with conventional labial appliances, while aligner-treated patients showed greater increases in IL-2, IL-6, and IL-8. Baeshen 24 reported significantly higher TNF-α, IL-1α, and IL-1β levels in patients treated with lingual fixed appliances, attributing this finding to increased mechanical stress and plaque accumulation associated with the lingual appliance design.
Although these studies demonstrate distinct cytokine expression profiles between aligners and fixed appliances, it is important to emphasize that such differences should be interpreted as variations in the biological inflammatory response rather than definitive indicators of treatment efficiency. Cytokine levels in GCF primarily reflect the periodontal tissue response to applied orthodontic forces and do not directly represent the rate of orthodontic tooth movement. Future longitudinal studies integrating simultaneous biomarker assessment with objective measurements of tooth displacement are required to clarify the clinical relevance of inflammatory mediator expression.
Aziz and Singh 25 reported peak IL-1β levels at 24 h following aligner insertion, indicating an acute inflammatory response, but did not assess tooth movement outcomes. Therefore, although elevated biomarker levels were observed with both treatment modalities, the present evidence does not support a direct association between inflammatory mediator levels and accelerated orthodontic tooth movement.
In addition to inflammatory cytokines, several studies evaluated bone metabolism markers. Pisarla et al. 32 reported significantly higher alkaline phosphatase levels in the aligner group during early treatment stages, suggesting active bone remodeling. Alnazeh et al. 33 observed elevated IL-6 levels in patients treated with fixed appliances, while bone turnover markers such as N-telopeptides (NTx) and osteocalcin showed similar trends in both groups. Kredig et al. 35 found no significant increase in aMMP-8 levels in adolescents treated with clear aligners, indicating periodontal safety when adequate oral hygiene is maintained. Ravi et al. 36 reported comparable MMP-13 levels between the aligner and fixed appliance groups, suggesting similar remodeling responses.
The meta-analysis conducted for IL-1β levels revealed no statistically significant difference between clear aligner and fixed appliance therapy. However, substantial heterogeneity was observed (I2 = 98%). This high heterogeneity may be attributed to differences in study design, sample size, biomarker selection, timing of GCF collection, appliance configuration, force magnitude, and analytical techniques such as ELISA and proteomic methods. Consequently, the pooled estimates should be interpreted with caution, and the results are better viewed as indicative of biological trends rather than definitive quantitative differences.
Overall, both clear aligners and fixed orthodontic appliances elicit inflammatory responses essential for orthodontic tooth movement. While aligners and fixed appliances appear to induce distinct cytokine expression patterns, current evidence does not establish a clear relationship between these differences and the rate of tooth movement. Given the methodological variability and high heterogeneity among the included studies, further well-designed, standardized longitudinal trials correlating inflammatory biomarkers with clinical measures of orthodontic tooth movement are warranted.
Importantly, increased biomarker levels cannot be directly equated with accelerated orthodontic tooth movement. None of the included studies directly correlated cytokine levels with quantitative measures of tooth displacement. Therefore, observed biomarker differences likely represent biological response patterns rather than differences in treatment outcomes.
The substantial heterogeneity observed may be attributed to differences in biomarker selection, GCF sampling intervals, appliance design, force magnitude, and analytical methods. Consequently, pooled estimates should be interpreted with caution.
Limitations
High heterogeneity and methodological variability among the included studies limit the strength of the conclusions. Differences in GCF analysis methods, timing of sample collection, and small sample sizes further reduce comparability. The GRADE approach was not applied due to these limitations.
Conclusion
Both clear aligner therapy and fixed orthodontic appliances induce an inflammatory response in periodontal tissues during active orthodontic treatment, reflected by increased levels of inflammatory and bone metabolism biomarkers in GCF. Although differences in cytokine expression profiles were observed between the two treatment modalities, these variations indicate differences in the biological inflammatory response rather than definitive differences in the rate of orthodontic tooth movement. The meta-analysis demonstrated no statistically significant difference in IL-1β levels between the groups, and substantial heterogeneity among the included studies limits the strength of the quantitative conclusions. Therefore, the findings should be interpreted with caution. Further well-designed, standardized longitudinal studies correlating biomarker levels with clinical measures of tooth movement are required to establish meaningful clinical implications.
Authors Contribution
Priyanka Tarde conceived and designed the study, performed the literature search and study selection, and carried out data extraction and statistical analysis.
Priyanka Tarde, Anjali Kalekar, and Priyanka Badu drafted the manuscript.
Santosh J. Chavan and Jyoti Manchanda supervised the study.
All authors critically reviewed and revised the manuscript for important intellectual content.
All authors have read and approved the final manuscript.
Footnotes
Declaration of Conflict of Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
Ethical approval and informed consent were not required for this systematic review and meta-analysis as the study utilized data from previously published studies.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.