
Abstract
The paper investigates the challenges that musicians face when playing in a paediatric hospital, drawing on case study evidence from a long-standing programme in Italy. The research focussed on identifying: (i) the inherent challenges of being a performer in a hospital; and (ii) the professional characteristics of the musicians who perform in hospitals. As part of a wider, cross-cultural study, musicians (N = 8) were asked to report their (i) physical and (ii) psychological perceptions, before and after their musical performance in the hospital across four weeks. Interview data were analyzed according to content analysis and were informed by grounded theory. Results suggest that performing in a hospital setting is particularly demanding psychologically and emotionally where the nature of the musicians’ role requires them to improvise (i) as part of their normal performance practice, seeking active collaboration by the patient, and (ii) environmentally, in relation to changes in the medical condition of their client/patient/audience. The results are also explained in terms of inherent tensions in a professional musical identity that requires expert performance in a clinical setting.
Previous research in the fields of music therapy and music medicine indicates that music can be an effective means of decreasing the perception of pain among hospitalized children (Caprilli, Anastasi, Grotto, Abeti, & Messeri, 2007), providing distraction from hospital procedures (Robb, 2003) and relieving the child/patient from the anxiety and stress connected to hospitalization (Longhi & Pickett, 2008). The literature reviews on the impact of music on hospitalized children (Mrázová & Celec, 2010; Naylor, Kingsnorth, Lamont, McKeever, & Macarthur, 2010; Robb & Carpenter, 2009) show that the focus of these studies is primarily on the impact of the music on the child and that few studies have examined the role of musicians’ and/or music therapists’ interaction with the client in medical settings.
This gap in research is mainly due to the fact that, in these studies, music is perceived as something that stands in its own right without being connected with the role of the players. Nevertheless the use of live music in hospitals, and healthcare settings more generally, is a multifaceted process involving not only the music played and the patients who are listening – together with their carers and medical staff – but also the performers (Preti & Welch, 2004, 2011; Robb & Carpenter, 2009). For example, through their performance, musicians play a leading role in the communication of emotion, fostering an emotional response in the listeners (Juslin, Liljestrom, Vastfjall, & Lundqvist, 2010). Consequently it may be that much of the success of live music sessions depends on the player’s ability to interact positively with the patients while also responding meaningfully to the hospital environment.
At present there is no empirical evidence about the professional background of musicians playing in healthcare settings, as argued in the recent arts and health debate (Dileo & Bradt, 2009; Moss & O’Neill, 2009). What we know about this type of musician derives from the selection criteria specified by some of the associations and charities involved in the organization of live music programmes in healthcare settings in the United Kingdom (UK), Europe and United States (US). The emerging profile, so far, is that of a professional musician with high levels of musicianship, well-developed communication skills, and with an extensive and diverse repertoire (Preti, 2009). If selected – through an audition process – the musicians undergo a short induction from one of their more experienced colleagues and they are usually supervised for the first few performances. The quality and length of the training is one of the main differences between musicians playing in hospitals and music therapists. While the training for musicians playing in hospitals is in its early stages, the one for music therapists has a long and established tradition (Bruscia, 1998). Their training is approved by an independent certification board and each practitioner is required to adhere to a code of ethics (see Dileo & Bradt, 2009, p. 170).
Besides the role of charities and organizations in providing live music in hospitals, in some of these settings there is also the active involvement of resident music therapists who often act as a point of contact between the hospital and the musicians (Curtis, 2011; Shoemark, 2007). The Sweet Melodies programme at the Royal Children’s Hospital in Melbourne is an example of the collaboration between the hospital’s resident music therapist and four professional musicians that has led to the publication of guidelines for visiting musicians in hospitals (Shoemark, 2009). Musicians performing in hospitals for the first time can find insightful information on: (i) the likely challenges that they will face in different spaces of the hospital; (ii) the selection of appropriate repertoire; and (iii) how to connect with the audience, amongst other suggestions. The guidelines are also an example of how music therapists can share aspects of their practice and expertise with professional musicians, facilitating their access in the hospital while fostering awareness of different musical issues when performing in healthcare settings.
While the specific aims of music therapists within a hospital context are clinical, those of musicians are mainly cultural (Bouteloup, 2010). Their aim is to distract the child-patient from the hospital routine by creating a space where the child can choose to engage in musical activities. Their action is thus not part of a therapeutic protocol, nor is it aimed as a substitute, unlike the role of music therapists, who seek to prioritize individualized goals (such as pain and anxiety reduction or physical rehabilitation) within a therapeutic relationship. Moreover, musicians playing in hospitals create a safe space where children, their carers and the hospital staff are free to interact musically. Although there are significant differences between the work of music therapists and those of musicians performing in hospitals, the Community Music Therapy movement (Pavlicevic & Ansdell, 2004; Stige, 2010) seems to offer a bridge between the two interventions. By addressing and advocating the social and cultural use of music in relation to ‘health, human development, and social change in some way or another’ (Stige, 2010, p. 9), the Community Music Therapy perspective broadens the contexts of music therapy by offering an engaging platform for discussion opened to different music programmes. The concept of ‘music environmental therapy’ introduced by Aasgaard (1999, 2004) emerges from the Community Music Therapy debate. His work is also in line with some aspects of hospital design research that aims to re-create a familiar environment in hospitals where patients, their families and hospital staff can interact in a less stressful way (Ulrich, 2006). Aasgaard (1999) defines music environmental therapy as: a systematic process of using music to promote health in a specific environment, inside or outside institutions. [. . .] The techniques are often combinations of receptive activity or recreative categories. [. . . ] Music environmental therapy can take place in corridors, halls or common rooms, treatment rooms or out-of-doors. To regard musical environmental therapy as a school of practice in its own right is questionable, but it certainly has a focus which is unique. (1999, pp. 34–35)
Aasgaard points out that amongst the challenges that a music therapist is likely to face while performing in hospitals is the ability to improvise musically and environmentally in a variety of situations as well as the issue of satisfying the high level of expectations from the hospital staff and the carers. This aspect in particular has been described as one of the most recurrent sources of burn out 1 in music therapists, together with the lack of support from within the institutions where they work (Knoll, Reuer, & Henry, 1988). A more recent survey conducted by Decuir and Vega (2010) found that, amongst the primary factors contributing to burn out in music therapists, there were few employment and advancement opportunities in their careers along with low salaries. The survey also investigated the reasons that motivated the music therapists to remain in their job. The authors found six emerging themes (2010, p. 138) that were reported by music therapists as keeping them engaged with their particular type of employment. These were: (1) the interdisciplinary nature of music therapy; (2) being part of the growth and development of a new and expanding profession; (3) the personal and professional growth experienced through clinical practice; (4) observing the dynamic relationship between music and the patient; (5) working in a musical environment; and (6) music’s unique ability to reach across generations. Additionally, among the sources of job satisfaction the literature reports the experience of working in collaboration with other music therapists (Knoll et al., 1988), the continuous personal and professional development (Stewart, 2000), having supervisions (Sutton, 2002) and witnessing changes in one’s client (Hills, Norman, & Forster, 2000).
Despite the number of studies that have been focussed on different groups of professional musicians (Creech et al., 2008; MacDonald & Wilson, 2005; Williamon, 2004), the particular category of musicians performing in healthcare settings is reported to be under-researched and under-theorized (Dileo & Bradt, 2009). Of the limited previous research, what it is known about these musicians is that they frequently do not have a music therapy background and that their stated purpose within the hospital is reported as primarily to entertain children, carers and staff (Lindsay, 1995). Similar to other types of professional musicians (Cunningham & Higgs, 2010; McAndrew & McKimm, 2010; Throsby & Zednik, 2010) and music therapists (Stewart, 2000), these musicians do not have a single full-time position, but rather a portfolio of different jobs (Wakin, 2010). This is chiefly due to the short-term nature of the music programmes and the related issue of irregular and limited funding (Knell & Taylor, 2011).
The aim of the present study was to investigate musicians’ experiences of performing for a non-voluntary audience. Furthermore, the research focussed on identifying: (i) the inherent challenges of being a performer in a hospital; and (ii) the professional characteristics of the musicians who perform in such a setting.
Participants
The group of musicians consisted of eight players, two males and six females, who made up the total number of musicians employed in an Italian paediatric hospital. The hospital was selected for the research because of its long-term music programme that extended across the whole hospital. Six of the eight musicians were professional who played in local orchestras and had music teaching experience, while the other two had unrelated jobs. As part of the requirements for the role, all the musicians had to attend a one-year part-time training course to be allowed to play in the hospital. A local school of music selected by the hospital foundation was in charge of both the training and the music programme in the hospital (for more details on the training and for an in-depth description of the music programme, see Preti & Welch, 2011).
All the musicians sang and played an instrument: Guitar, violin and viola, woodwind (oboe, flute) and saxophone. Their age ranged between 30 and 50 years old. At the time of this research four musicians had been playing regularly in the hospital for five years, while the other four had been employed for just over a year. The more experienced musicians were playing an average of eight hours a week, while their less experienced colleagues played an average of four hours a week.
The music programme covered 23 wards with 45 hours of music a week. The timetable was the result of a careful matching between the requirements of single wards (previously discussed by the member of the association and head nurses) and the availability of the musicians. The musicians were allocated to play in different spaces of the hospital and were not scheduled to play more than one hour in each space. They were scheduled to play an average of three hours per session in a typical day; therefore breaks were not included in the timetable and the musicians had to change location within the hospital and start a new session straight away.
Music sessions were taking place in corridors, waiting rooms and wards, each with a slightly different focus related to the patient and client group. This meant that the musicians had to prepare different repertoire for both large groups and one-to-one sessions. Their sessions always included parents and staff, and each group was considered as having an ‘instrumental’ focus for the success of the session. The repertoire included mainly children’s songs and a small proportion of popular and classical music. Musicians also used little percussion instruments to improvise simple rhythmic patterns while singing.
Research design and data collection
A multi-methods research design was adopted in this study, using semi-structured interviews supplemented by self-report measures. As part of a wider, cross-cultural study in the UK and Italy, the eight musicians involved in this paediatric hospital music programme were asked to self-report using a seven-point faces scale (Figure 1, coded from 1 to 7 moving from left to right) on their (i) physical and (ii) psychological perceptions, both before and after their musical performance in the hospital, across a period of four weeks.

Seven-point faces scale.
The self-report measure data were also used as prompts for linked semi-structured interviews. Each musician reported on both their physical and psychological states, once before and once after their musical sessions in the hospital. These rating pairs were made an average of three times per musician. Each musician was asked by the first author to complete the rating scale at the beginning and at the end of each music session. Semi-structured interviews took place while the musicians were completing the faces scale, once prior to the beginning of their music session and once after. Previously Curtis (2011) reported on the use of a faces scale in pre- and post-test measures at the hospital’s request. She found out that the faces scale was identified by 90% of palliative care nursing professionals as easy to use and appropriate for administration by non-nursing professionals. Furthermore, Preston and Colman (2000) in their review of rating scales suggest that a seven-point scale is amongst one of the most reliable instruments. The musicians verbalized their face-choices (from ‘sad’ to ‘happy’) and expanded on their perceived psycho-physical conditions while ticking a particular face, before and after their session and while still in hospital. At the same time, they were interviewed according to an interview guide (Rice & Ezzy, 1999; Appendix 1).
The musicians were invited to use their own definition of ‘physical state’, as we were looking for emerging themes in the musicians’ work in the hospital and possible connections to their professional life outside the hospital. The musicians were told that, in the case of their ‘physical state’, (i) they were expected to make a judgement on how they felt in relation to their perception of either being tired and/or discomforted (such as lack of sleep, or having low blood pressure, being too hot, having some kind of physical pain, etc.), neutral, or more energetic. In the case of ‘psychological state’, (ii) they were expected to rate how they felt before (pre-session) and after (post-session) their music session in the hospital in relation to perceived stress, anxiety, happiness and self-satisfaction. After the first week the musicians’ verbalization of their self-reported measures on the seven-point faces scale became progressively more articulated and their reflections – on both their musical actions and their individual perception of reward, fatigue and stress – more detailed. All the musicians had the nature of the research explained in advance and in writing and provided informed consent for their participation in the study, knowing that they could withdraw at any time, with or without reason. With regard to ethical procedures it was made clear that the researchers adhered to the code of ethics approved by The British Educational Research Association (BERA) 2 . A standard form supplied by the hospital – guaranteeing confidentiality and anonymity in the data processing – was used to provide written consent and to ensure that the research also met the ethical requirements of the hospital.
A grounded theory approach (Bryant & Charmaz, 2007; Glaser & Strauss, 1967) was selected for the analysis of the semi-structured interviews. Grounded theory provides clear procedures for the analysis of the data that can be verified by people external to the research process. Moreover it is a flexible and yet systematic approach to data analysis. The aim of this approach was to generate an explanation that is central to the data and to find categories that have both a high level of abstraction and that are derived from the data collected (Robson, 2002, p. 493). The coding process was carried out in three stages (adapted from Robson 2002, p. 493): (1) open coding, to find conceptual categories in the data; (2) axial coding, to find relationships between these categories; and (3) selective coding to conceptualize the established relationships through core categories. In our case (Appendix 2) interviews were translated from Italian into English by the first author, and then they were subsequently transcribed into Microsoft Word documents and the files were then imported into Atlas.ti (Atlas.ti, 2005) a software tool for qualitative analysis. The open coding stage was carried out by the first author according to emergent features related both to the inherent focus of the transcriptions and concepts from the literature. Atlas.ti automatically grouped codes and presented them as a list with links to the original text. The list of codes was then clustered in categories according to the emergent relationships between the grouped categories (axial coding). Finally, four categories emerged (selective coding): (i) risk of burn out and related causes; (ii) the average length of the session and repercussions on the musicians; (iii) rotation issues; and (iv) coping strategies. The coding process was validated by a research colleague undertaking a review of selected sections of open coding and also inspecting the emergent axial codes.
Results
Rating scale data
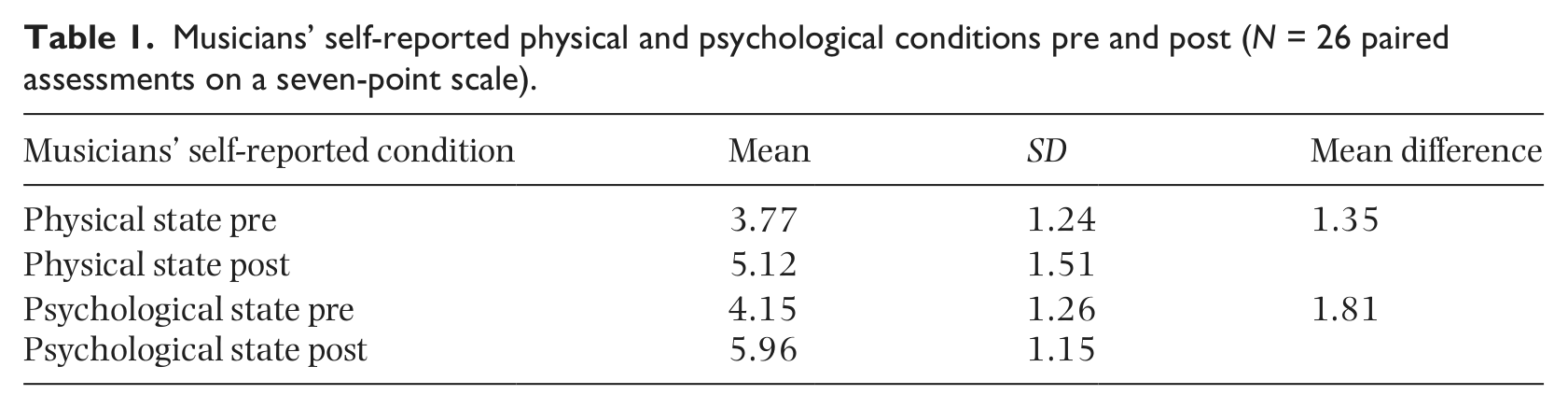
A Wilcoxon Signed Ranks test was used to investigate whether musicians’ ratings of how they felt physically and psychologically had changed after a session of playing in the hospital. Results suggest that musicians’ perception of their physical condition had improved after the music session (Z = −3.00, N = 26, p = .003). Similarly, their psychological condition was also rated as improved after they had played in the hospital (Z = −3.67, N = 26, p < .001). Musicians reported feeling psychologically better than they did physically (Table 1, Cohen’s d = .407 for before and after, scores collapsed). On both measures the musicians reported that the perception of how they felt physically and psychologically had improved after their playing in the hospital (Table 1), with the small difference that their psychological conditions were reported to be improved slightly more than their physical ones. However, these results should be interpreted with caution given the relatively small sample size.
Musicians’ self-reported physical and psychological conditions pre and post (N = 26 paired assessments on a seven-point scale).
Interview data
Risk of burnout and related causes
From the interviews an image emerged of the musicians seeing themselves as having constantly to work while juggling complex lives. The aspect of ‘being tired’ emerged progressively as a recurring theme from the interviews with seven of the eight musicians. Musicians reported being physically ‘tired’ both when arriving and leaving the hospital. They were generally arriving at the hospital rushing from a previous job and, soon after the music session, they would feel the need to hurry to the next job, conveying the impression of a rather ‘out of breath’ routine. Maria,
3
for example, was teaching in two music schools and was playing professionally in three orchestras. She was also playing in two different paediatric hospitals; she was married and had a young child. This was her comment when she was asked about how she felt before starting her session in the hospital: If I stop, I collapse. Tuesday and Wednesday I cannot see my daughter. I find it difficult, but one needs to work. (Maria)
Marta and Pietro reported the same feeling of being exhausted just before starting their scheduled music sessions. This feeling originated both from their personal lives (e.g., having young children and juggling several jobs at the same time) and from the work in the hospital itself, which was perceived as being demanding in terms of both physical and emotional engagement: This morning I had two eggs and milk with biscuits. If I don’t eat properly when I play here I faint, because it’s a stressful experience, both from a physical and psychological point of view. (Pietro)
The aspect of ‘being tired’, which initially was associated with the musicians’ life styles, subsequently became unpacked as being more connected to an emotional aspect of the musicians’ work in the hospital. Physical tiredness was a concept that the musicians used to describe their work, which was defined in a polarized way. On one hand the work was perceived as emotionally rewarding (discussed in ‘coping strategies’) while, on the other hand, it was seen as emotionally draining, up to the point that some of the musicians needed to take a break from it: In April I had a breakdown. I was stressed out. I couldn’t cope with coming here anymore. This job is emotionally draining. You have to pay attention to a thousand different things when you play; it is really stressful. There are a lot of children, lots of different situations. This morning was positive; there was no tension, but on other occasions there’s a lot of tension around you. Even if the session goes well, it sucks a lot of energy out of you. If I have to play in the hospital for an hour or teach in school, there’s no comparison! Here, I have to give out everything and sometimes it’s not enough. (Cinzia)
When the musicians reported being tired they also reported a different reaction to the ‘crying’ that they heard in the hospital. In fact, if in general they were attracted towards a child who was crying, representing a situation that music could alleviate, when they were tired their perception changed up to the point that ‘crying’ became one of the main stressors that prevented some of them from continuing their musical activity in the hospital, even if only for a short time: After a year of playing, I had to stop for a month, as I couldn’t cope with it anymore. Every time I got in the hospital, I was distressed. Whenever I heard a child crying, I felt I had a block and that I simply could not go in. (Maria) There has been a period when I felt the only thing I was hearing was crying and that there was no other sound in the hospital. I found it very hard to cope with that. (Paola)
The reported tiredness was perceived to have had an impact on the musicians’ work in the hospital as they reported struggling, both physically and emotionally, with implications for the quality of their musical performance: Being tired is also connected to how you feel inside. When my father died I was very low and I kept playing here. This is a very rewarding job, but sometimes you just cannot cope. . . (Pietro)
In addition to the emotional fatigue, the musicians often had to play bent on their knees (to be able to make eye-contact with the child), and they had to wear a special waistcoat, with lots of pockets for the little percussion instruments, which was reported to be very hot attire in the summer.
The average length of a music session and its effects on the musicians
The length of the music session was perceived by several musicians to be one of the causes of their tiredness. Some musicians had to play an average of three to four hours in a row and, even if on the day they seemed to cope well, on the next day they reported a sense of being exhausted. The musicians did not feel that they had time to recover after their sessions in the hospital, as some of them (three at least, according to the official timetable, without considering the extra-timetable arrangements) had to play consecutively for three or more hours on consecutive days. One of the likely outcomes was that they tended to cancel some of their scheduled sessions as they reported themselves to be ‘drained’ as a consequence of the previous day’s work: Maybe I play for 15 minutes, and then for other bits of fragmented time, but when I get to the end of my three hours, I collapse. Before I had four hours, but I couldn’t do it and I asked if I could just do three. (Paola)
When asked about how they felt physically and psychologically soon after their music session, generally the musicians expressed a positive feeling, almost like being on a ‘high’: Now I feel great. As soon as I finish playing, it’s fine. It’s when I stop for a break that I got down. (Paola)
But when the same musician was interviewed on the following day, they provided a more nuanced account of how the high peak almost evolved into a negative dip when the effect of the ‘high’ had faded out: Today, I’ll do a bit less because I am tired. I have already played for two hours in a nursing home and we are playing Wagner in the theatre, so I am really tired. Last week I couldn’t make it. (Paola) This morning I only came because I knew you were waiting for me, otherwise I would have probably stayed at home as I am very tired. (Bruna)
The musicians’ busy lives, interwoven with the emotional demand of the work in the hospital, had led, at different stages (and with only two exceptions) to minor burnout, with the consequence that the musicians had to take unpaid leave from their work. As their musical activity in the hospital was part of a relatively tight monthly personal budget, musicians might have been motivated to keep working in the hospital until they reached, and probably, exceeded, a healthy psychological and physiological threshold. Moreover, musicians were provided with very few occasions to meet and to verbalize their experiences with their fellow performers, which might have enabled a release of tension, and the finding of some kind of mutual support. The relative professional isolation in their performance context meant that the management of their experiences was left to their personal resources.
Musicians explicitly talked about the musical challenge of their work in the hospital in relation to the variety of children involved and the need to master a broad repertoire, which they did not have the time to update. Playing in the same spaces was more likely to result in the same encounters, as in some waiting rooms children were visiting for treatment on a weekly basis: To prepare a session I have to study at least for three hours every week. I find it difficult to play always the same music. (Pietro)
To compensate for a lack of new repertoire, the musicians often used musical improvisation with percussion instruments which, nonetheless, they had to prepare, as most of the musicians, except two, came from a strictly Western classical music background where, customarily, there are likely to be few opportunities to engage in improvisation for most instrumentalists (cf. Creech et al., 2008). The musicians were aware of the limitations of their musical repertoire. Furthermore, the musicians reported that the weekly preparation needed at home was at least the same amount of time that they spent (weekly) in the hospital, but with the difference that this time was not factored in by the local association that employed them. The result was that – although musicians had to spend time preparing their session – this time was not considered by them to be enough, hence causing a sense of frustration for not being able to perform at their best.
Rotation issues
One factor in the perceived stress that seven of the eight musicians reported in the interviews concerned the fixed timetable with which the musicians had to comply. The musicians were supposed to play in their assigned wards for at least six months, even if the timetable had been the same for over a year. This caused a series of repercussions for both the musicians and the hospital staff. In two cases, the musicians explicitly asked to be moved from their designated wards after they had witnessed the death of a child while they were playing: When I came into the ward, as always, I asked the nurse how the situation was on that day and she told me to start from the left side of the ward, and so I did. After a few minutes, I noticed a nurse crying and then a couple of parents that were holding each other, crying as well. I immediately withdrew. I didn’t expect that. At that point I was playing a cheerful tune and I felt broken. Luckily, I met Luca [a musician] who is very experienced and we talked about what had just happened and I felt better. (Paola)
This episode triggered a strong emotional reaction defined by the musicians as a ‘shock’. Furthermore, the musician reported that she had not received any support from the association and only some by her fellow musicians whom she met subsequently. In another case, the experience of the event forced one of the musicians to have a break from the hospital for a few months as she could not bring herself to play anymore. She also had doubts about continuing to play in the hospital, as the experience had been emotionally very difficult for her.
The organization of the timetable emerged as a central issue in the overall balance between musicians’ sense of wellbeing and their perceived effectiveness as performers. Playing in their own preferred wards or waiting rooms was, in fact, reported as being an enjoyable activity and was perceived as ‘less demanding’ compared to playing in some of the assigned wards. Moreover it seemed quite evident that each musician had their own preferences – and felt more at ease – when it came to playing in certain spaces: I like to play where there are children. I don’t like neonatology because babies are too small to interact with, or they are sleeping. Also, there is a lot of noise in that ward [heart monitors machines continuously beep]. (Maria)
And a contrasting account: I prefer neonatology because it’s a quiet ward and there are no children running everywhere [she laughs]. I usually find wards less demanding, they are quieter. Waiting rooms are more tiring. It’s noisier and you cannot use certain percussion instruments, you have to use different sonorities. (Cinzia)
Even though musicians operated on the basis of a fixed timetable there was a degree of flexibility allowed, mainly related to a musician’s personal health condition (such as having a sore throat) that often restricted the range of wards in which they were able to play. This sometimes forced them to reschedule their time in the hospital. Although it was reported to be paramount to keep to the timetable, it was also observed that, when a musician was not able to attend on the designated day, they tended to make up their time, either by swapping with a colleague or turning up in the ward without necessarily a previous agreement with the hospital staff. Moreover, the issue of updating the repertoire was exacerbated by the length of time spent in each space of the hospital. If for six months the same musician had to play in the same ward, this would inevitably cause some staff to notice the ‘sameness’ of their repertoire and, in some cases, to be irritated by it (Preti & Welch, 2012).
Coping strategies
Each musician had developed their own strategies to cope with the lack of rotation in hospital spaces and, in some cases, a perceived excessive amount of hours spent in a stressful environment. Five of the eight musicians used the very limited time in between sessions to disinfect the little percussion instruments and take a break from playing while doing it; the other three had developed some specific musical strategies that enabled them to relax while playing: To feel at ease, I play songs that I have practised a lot and that I especially like, so that I both enjoy and relax while playing. (Maria)
In particular, playing without singing and looking for an interaction with a particular child were reported as being moments within the session where the musicians felt more confident and in control. Musicians also made use of the ‘instrumental’ time as a space in between interactions, when they were observing the situation around them, determining the next phase of the session: I feel tired. Singing continuously is rather demanding for me. If I play, I relax as that is my main job and I am in control. I often introduce the songs with the violin without singing, as I can quickly go through the lyrics while I am playing the introduction. (Cinzia) If you play for four hours, towards the end you are really looking forward to finishing. At that point, I prefer to play in wards where there’s not so much interaction with children and you don’t have to use percussion instruments, such as neonatology where you just sing lullabies. (Marta)
As a result of their experience and relative unfamiliarity with the working environment, the less experienced musicians were more hesitant musically and less experienced emotionally in handling situations in the hospital. They tended to spend less time focussing on a single interaction, favouring a more collective approach, as this required less intense emotional involvement. They also appeared to be more cautious with the selection of music, preferring rather ‘neutral’ songs to more emotionally charged ones that their more experienced colleagues were playing. Overall, and cutting across the amount of experience that they had, two main approaches with patients were evidenced: One privileging instrumental improvisation and the other privileging singing.
However, despite the physical and psychological challenges, playing in the hospital was reported to be a rewarding experience for all the musicians. They felt empowered by a sense of music acting as a powerful tool through which they were able to impact positively on the lives of the hospitalized children. This feeling was examplified by Bruna:
Whenever I hear someone crying, I always go there as it is very rewarding if you manage to calm a child down. I feel really good if I manage to do so.
Thus the main source of reward and motivation to keep playing in the hospital was reported to come from the musical interaction with the children: I play to improve people’s lives and then, indirectly, the positiveness of this objective has a beneficial return for me. Therefore if I am depressed, this action becomes therapeutic; if I am nervous, I unwind, and if I am anxious, I relax. (Marta)
Discussion
This study has investigated the experience of a group of musicians that have been performing regularly and for a long time in a paediatric hospital. It has also explored the challenges inherent in performing in such a setting and the professional characteristics developed by the musicians. From the semi-structured interviews and the self-report measures, a picture emerges of the musicians experiencing what they described as emotional and psychological fatigue, which translated into physical symptoms. These symptoms seemed to reflect the nature of their musical performance in the hospital, which consisted of two components: (i) musical-emotional; and (ii) physical.
In addition to the performance elements, the musicians were directly involved with children, their carers and the hospital staff and, as a consequence, they reported experiencing related stress and distress in being exposed to the suffering witnessed in the hospital. However, somewhat paradoxically, it was also the intensity of these relationships that was seen as worthwhile and that kept the musicians motivated. If, on the one hand, the work in the hospital was perceived as exhausting, on the other hand it was perceived also as extremely rewarding and sufficiently so that they seemed to be able to forget the negative aspects of it and were able to find new energies that enabled them (usually) to keep returning to the hospital.
An explanation for the musicians’ attitude can be traced in flow theory (Csikszentmihalyi, 1990), which suggests that ‘optimal experience requires a balance between roughly equal levels of perceived challenge and skill in a situation that involves intense concentration’ (O’Neill & McPherson, 2002, p. 35). In this case the challenges for the musicians are represented by: (i) performing at a high standard; (ii) detecting the emotional situation of the space they are walking in; (iii) selecting the right piece of music to establish a contact with the child whom they are about to start a musical interaction with; and (iv) perform variations on the piece, often improvising.
According to the musicians’ ratings, they reported feeling worse at the beginning of their ‘performance’ compared to the end. This was an indication that they were ‘tired’ due to the continuous amount of playing that they were doing, but also that behind what they described as ‘being tired’ there might have been different feelings such as anxiety and fear, symptoms that are usually associated with performance anxiety (Papageorgi, Creech, & Welch, 2011). What they reported as ‘tiredness’ appeared to be a mixture of emotional and physical elements, not easily distinguishable, which resemble ‘burnout’ as defined by Maslach and Jackson (1981). The seven-point faces scales that the eight musicians completed supported the energizing effects of playing in the hospital. Thus despite the small sample size (which is a reflection of the small population of musicians in hospitals at the time the study was conducted), the possible demand effects (where ratings scales spontaneously show ‘improvement’; see Steele-Johnson, Beauregard, Hoover, & Schmidt, 2000) and the use of a conservative, non-parametric statistical testing, the quantitative results were significant and revealed a moderate effect size. The consistency of quantitative and qualitative data provides a stronger and more confident basis upon which the conclusions of this study can be made.
What emerges from the data is that the musicians behaved like performers. They exhibited high levels of arousal at the end of their sessions in the hospital (see Table 1), but the results from the semi-structured interviews suggest that these levels dropped as soon as they arrived at home and also tended to stay low until the next day. Musicians had little time to recover in between ‘performances’. Furthermore, there was no evidence of systematic support amongst themselves as a group, nor a support system which had been organized by the association managing the longstanding music in hospital project. The musicians were left to cope with emotionally difficult situations, like witnessing the death of a child, and some of them felt that they were not equipped with either the emotional skills or musical techniques to cope with these situations. Part of the problem appeared to be a lack of defined spatial and situational boundaries, an absence that likely stemmed from the training according to their comments. The musicians were expected to play in emotionally challenging wards like the oncology ward or the neonatology ward without possessing specific tools to help them to perform in such spaces, and so they were relying mainly on their craft knowledge and experience.
The results emerging from the interview data do not show any significant difference between the more and less experienced musicians. The new musicians were scheduled to play in corridors and waiting rooms of non-life threatening wards. However, despite playing less than their more experienced colleagues, they provided a similar account of the challenges faced when playing in the hospital. This group of performers was not aware of the potential importance of supportive supervision in preserving a healthy balance in their personal and professional lives. It appeared that musicians were not provided with any space to verbalize their experiences, neither by their professional association nor by the hospital and, ultimately, nor by themselves, as there was no reported attempt to organize a support network among themselves, although they recognized the need for one.
In the Italian paediatric setting the work of the musicians was characterized by playing in a context that required particular musical skills, such as being able to improvise musically and rhythmically, and interpersonal skills that the musicians had partly developed in the training course and partly by the actual daily challenge of playing in the hospital. Musicians were interacting continuously with different audience(s) (children, parents, and hospital staff) and each interaction required an adequate musical repertoire and a range of different communications skills that musicians had to adapt constantly in real time.
Even if the musicians never mentioned dissatisfaction openly, a number of issues were considered to be problematic and a source of discontent and personal frustration. The most important was the musicians’ awareness of the amount of time needed to prepare for a music session in terms of renewing the repertoire and for building new percussion instruments. The time that the musicians needed to integrate and renew their repertoire was not paid for by the association managing the programme. Moreover, the inclusion of new songs in their repertoire was not demanded explicitly by the association. The musicians had to find their own motivations, time and resources within a busy working schedule made up of different jobs, as is often common for freelance musicians (Creech et al., 2008). Unlike music therapists they did not have a network of colleagues with whom to share different materials, nor an accessible library with available resources. Therefore some of them had to go through a time-consuming task each time they decided to update their repertoire. Also the implementation of a more frequent rotation across the wards would have been a simple improvement for the musicians as well as for the hospital staff that, on some occasions, complained about the ‘sameness’ of the repertoire, as each musician had a different musical style and repertoire (Preti & Welch, 2012).
The literature about job satisfaction among music therapists suggests that their average length of employment is five years or less (Lathom, 1982; Oppenheim, 1987). The relatively short average length of this experience suggests that many of them do not find the satisfaction (professional, financial) that they had hoped for in music therapy practice (Oppenheim, 1987). Oppenheim (1987, p. 105) believed that the majority of therapists do not work in the field long enough to experience burnout. In the case of the Italian musicians, they appeared to be highly rewarded emotionally by the contact with the children, but they were perhaps not sufficiently aware of their professional identity as ‘musicians in hospital’ and of the potential impact of their work on their personal and professional lives. As Stewart discovered (2000, p. 19; see also Sutton, 2002) in a related context, the music therapist’s sense of fulfilment is reported to largely depend on a variety of support networks, such as individual supervisions, good communication with parents and staff, individual opportunities to share work with colleagues and further training opportunities. In contrast, the reality of the musicians working in the Italian paediatric hospital was noted to be a solitary and often isolated existence.
Nevertheless, the musicians were passionate about and committed to their work in the hospital. Even if they perceived their role as being rather demanding, both emotionally and physically, at the same time they described it in highly positive terms. The rewards of their work were encapsulated in a powerful awareness that they were able to ‘make a difference’, even if for a short time, in the lives of the children and their carers in the hospital. The fulfilment that the musicians derived from witnessing a positive change in their clients is in line with similar findings in the literature on music therapists’ job satisfaction (Hills et al., 2000).
Overall the self-rating and interview data suggests that, in the observed hospital context, powerful positive and negative emotional and physical correlates are associated with the music session. For the musicians, playing in the hospital appears to be an advanced form of performance. In order to succeed in their work they had to be equipped with extensive musical and interpersonal skills. Their ‘audience’ was generally made up of distressed children, often in pain, and their consequently worried and stressed carers. As might be expected when catering for a broad cross-section of a local and regional population, children in hospitals represent different socio-cultural backgrounds, different prior (as well as current) experiences of hospitalization and, often, different ethnicities with associated belief and value systems, and perhaps also limited expertise in a non-native language. The musicians have to be able to ‘convince’ and motivate the children to participate in the session, allowing themselves to be distracted, even if only for few minutes.
The tools that the musicians had at their disposal to involve the young patients appears to be: (i) the selection of a suitable repertoire; (ii) the little percussion instruments that they distribute to the children to encourage their participation and foster a sense of control over the session (cf. Preti and Welch, 2011); (iii) interpersonal skills to motivate and involve different participants (including carers and medical staff), improvising on a number of both musical and emotional levels; and (iv) a constant awareness of the changes, both emotional and spatial, that progressively unfold around and within the session and, consequently, an on-going musical and emotional ‘tuning’ (adjustment) to the new situation (Preti & Schubert, 2011). The musicians are live agents of change in the hospital and this is simultaneously perceived by them as both enriching and exhausting. Their work is a solitary professional activity (at least in this particular instance) in an emotionally pressured environment and with little sense of acting as part of a collective.
Conclusions
For the first time data were gathered empirically from a group of musicians without a music therapy background playing in a hospital. These musicians were able to create a music routine informed by their craft knowledge and experiences as performers in the hospital. The study presents the contradiction of a group of musicians that play professionally for the wellbeing of the hospital patients, but at a potential longer-term cost to their own health. The nature of hospital performance – simultaneously engaging people in and through music – needs to be recognized as requiring a supportive professional organization if the risk of burn-out is to be minimized.
Footnotes
Appendix 1
Funding
This research was supported by a Research Studentship, PTA030200300938, from the Economic and Social Research Council, and by a Wingate Scholarship both held by the first author.