
Abstract
The objective of this cross-sectional study was to determine the extent and nature of self-reported musical abilities in persons with mild cognitive impairment (MCI). We recruited 60 older adults with a diagnosis of MCI from the Alzheimer’s disease Core Center. We evaluated self-reported musical abilities using the Goldsmiths General Musical Sophistication Index. We examined correlations between musical abilities and neuropsychological measures of verbal learning and memory, processing speed, executive function, verbal fluency, naming, and visuoconstructive abilities, while controlling for key demographic and participant characteristics. Older adults with MCI reported varying degrees of musical abilities. Nearly half of participants reported that they did not engage in regular, daily practice of a musical instrument. When adjusting for key demographic and participant characteristics, we found modest associations between four musical ability subfactors (active engagement, perceptual abilities, musical training, and emotional engagement with music) with three cognitive abilities: verbal fluency, executive function, and verbal naming. Except for the emotional engagement with music subfactor, none of the remaining musical ability subfactors correlated with any demographic or participant characteristics. While our study findings provided support for the relationship between musical and cognitive abilities in older adults with MCI, this relationship warrants further investigation.
Persons with mild cognitive impairment (MCI) are three to eight times more likely to convert to Alzheimer’s disease (AD) compared to persons without cognitive impairment (Bennett et al., 2002; Fisk, Merry, & Rockwood, 2003). Individuals with MCI often present with subjective and objective deficits in memory, executive function, attention, language, and/or visuospatial skills but retain functional independence in daily activities (Petersen et al., 2014). Despite the fact that persons with MCI and AD experience deficits in cognition, emerging neuroscientific evidence suggests that musical abilities remain intact in AD. Brain regions associated with music processing are relatively preserved in persons with AD compared to the rest of the brain (Jacobsen et al., 2015).
Persons with AD exhibit preserved musical abilities in the areas of playing a musical instrument, identifying basic musical features, and identifying familiar melodies (Johnson & Chow, 2015). In a series of studies, individuals with AD demonstrated preserved musical memory (Fornazzari et al., 2006; Johnson et al., 2011) and the ability to play a musical instrument (Beatty, Brumback, & Vonsattel, 1997), learn new songs (Cowles et al., 2003), and recognize emotions derived from music (Gagnon, Peretz, & Fulop, 2009). Persons with AD also demonstrated preserved musical semantic knowledge (Basaglia-Pappas et al., 2013) possibly driven by preserved procedural and episodic memory in AD (Fornazzari et al., 2006). In addition, even in the moderate and severe stages of AD, individuals showed a preserved ability to learn new songs (Samson, Dellacherie, & Platel, 2009). Conserved musical abilities may allow individuals with AD to continue to participate in musical activities and to remain emotionally engaged with music throughout the disease process (Cuddy, Sikka, & Vanstone, 2015).
Only a handful of studies have examined musical abilities in MCI. Kerer et al. (2014) found no differences in assigning emotional expressions (happy, sad, or unsure) to musical excerpts between older adults with MCI, early AD, and normal cognition. In contrast, compared to healthy controls, participants with MCI and early AD did better on the tests of musical discrimination (Kerer et al., 2013). In the same study, individuals with MCI demonstrated unimpaired performance in recognizing chords (Kerer et al., 2013). Since MCI is a multi-faceted construct and the individuals diagnosed with MCI present with varying degrees and domains of cognitive impairment, persons with MCI may differ widely in the aspects of preserved musical abilities.
There is growing evidence that engagement in music-related activities throughout the lifespan is associated with cognitive and health benefits. In a large cross-sectional study in older adults, playing a musical instrument or singing was associated with improved attention, episodic memory, and executive function (Mansens, Deeg, & Comijs, 2017). When Seinfeld, Figueroa, Ortiz-Gil, and Sanchez-Vives (2013) explored the effects of a 4-month piano training regimen on older adults, they found that older adults who received piano lessons had higher scores on the measures of executive function, inhibitory control, and divided attention compared to a control group. In a separate study of 89 persons with dementia and their caregivers, singing and music listening enhanced mood, orientation, remote episodic memory, attention, and executive function in older adults with dementia (Särkämö et al., 2014). The majority of these studies have been conducted in cognitively normal older adults or individuals with varying stages of dementia; thus, much less is known about the extent and the potential cognitive benefits of preserved musical abilities in individuals with MCI. Given the shift of employing preventative strategies to earlier stages of dementia and the current state of knowledge regarding the preservation of musical abilities in AD, there is a growing need to understand the extent of musical abilities in persons with MCI. Therefore, the purpose of this study was to determine the extent and nature of self-reported musical abilities in persons with MCI.
Method
Sample
For this cross-sectional study our team recruited sixty participants with a recent diagnosis of MCI (< 12 months) and those participants who maintained a diagnosis of MCI in a recent (< 12 months) follow-up appointment. Participants were included if they spoke and understood English. We excluded participants from our study if they were younger than 55 years old, had a primary psychiatric disorder, a systemic illness that could interfere with cognitive functioning, history of stroke and/or hydrocephalus, or were unable to provide informed consent.
Setting
We enrolled study participants from the Alzheimer’s Disease Core Center (ADCC) research and clinical cohort at the University of Pennsylvania. As part of the ongoing clinical assessment, these patients completed an annual battery of cognitive measures and physical assessments (Beekly et al., 2007; Morris et al., 2006). The ADCC clinical team assigned an MCI diagnosis through consensus using previously published guidelines and a standardized clinical protocol (Petersen, 2004). All participants completed a neuropsychological battery aimed to assess many of the cognitive abilities most impacted by MCI. Our study received Institutional Review Board approval from the University of Pennsylvania. All participants provided written informed consent. In the informed consent document, we requested the permission to extract participants’ data from the ADCC records. For the prospective data collection, we met with the study participants at the ADCC or a location of mutual convenience.
Measurements
To reduce respondent burden, multiple measures were extracted from the ADCC database on our study participants at the time of enrollment in our study. The participants at the ADCC had neuropsychological data stored in the Integrative Neurodegenerative Database (Morris et al., 2006; Xie et al., 2011). For all participants, we extracted their demographic and already-completed neuropsychological test data collected closest to their date of enrollment in our study. For our study, the primary author first asked the participants to complete the self-reported Goldsmiths Musical Sophistication (Gold-MSI) questionnaire items. Next, the primary author screened the participants for depression using the Geriatric Depression Scale. We chose to administer the Gold-MSI first in order not to confound the answers on the Gold-MSI with responses on the depression screening tool.
Neuropsychological tests
We extracted scores for the following areas of neuropsychological functioning: verbal episodic memory, processing speed, executive function, verbal fluency, naming. and visuoconstructive abilities. The verbal episodic memory test was a 10-item Word List that included immediate recall (total of three learning trials), delayed recall, and recognition testing (Morris et al., 1989). We used the results from the Trail Making Tests A and B (TMT A and B; Reitan & Wolfson, 1993) to gauge processing speed and executive function, respectively. The verbal fluency measure was a semantic fluency task (total number of animals produced in 60 seconds; Morris et al., 1989). We examined scores for verbal naming using the 30-item Boston Naming Test (BNT; Goodglass & Kaplan, 1983; Kaplan, 2001). Lastly, we used the results from the Clock Drawing Test (CDT; Shulman, Pushkar Gold, Cohen, & Zucchero, 1993) to measure visuoconstructive abilities. For all cognitive tests, higher scores indicate better performance with the exception of the Trail Making Tests A and B and Clock Drawing Test. Next, we converted the raw scores of each neuropsychological test to a z-score using Weintraub et al. (2009) norms or norms based on the ADCC computed normative data using the same methods published by Weintraub et al. (2009). Doing so allowed for standardization of the sample scores against the published norms and aided in the interpretation of the results.
Demographic characteristics
We collected the following demographic and health information about the study participants from the ADCC records: age, gender, Mini-Mental State Examination (MMSE) scores, years of education, and the number of chronic illnesses. To further characterize the sample, we extracted the following information from the database: marital status, race, ethnicity, living status, and caregiving relationship. In addition, we used the Wechsler Test of Adult Reading (WTAR; Holdnack, 2001) as an estimate of educational attainment and premorbid intelligence. Each patient completed the WTAR at his/her initial ADCC visit.
Musical abilities
To gauge musical abilities, we used the Goldsmiths Musical Sophistication Index (Gold-MSI). The Gold-MSI is a self-report questionnaire that measures musical abilities in a comprehensive way in the general (i.e., non-professional musician) population (Müllensiefen, Gingras, Musil, & Stewart, 2014). The Gold-MSI is sensitive to differences among “non-musicians” in five distinct categories: (a) active musical engagement (e.g., how much personal time and financial resources are spent on music), (b) self-reported perceptual abilities (e.g., accuracy of musical listening skills), (c) musical training (e.g., amount of formal musical training received), (d) self-reported singing abilities (e.g., accuracy of one’s own singing), and (e) sophisticated emotional engagement with music (e.g., ability to talk about emotions that music expresses; Müllensiefen, Gingras, Musil, et al., 2014).
All Gold-MSI items, except for one open-ended question, are scored on the same 7-point Likert scale and receive equal weights for scoring, which is known to make the scale more robust. Embedded within the Gold-MSI is the General Musical Sophistication Subscale (GMSS), which includes 18 items with excellent internal consistency (Cronbach’s alpha = 0.926). For our analysis we used the GMSS since these items load highest on the general factor of what it means to be musical and have roughly the same weights (Müllensiefen, Gingras, Musil, et al., 2014). Higher scores on the GMSS correspond to higher self-reported musical abilities. We also examined individual subfactors (active engagement, perceptual abilities, musical training, singing abilities, and emotional engagement with music) as they relate to participant characteristics and cognitive abilities.
Depression
The Geriatric Depression Scale (GDS-15) is a brief measure of depressive symptoms found to be an effective screening tool for depression in older adults (Burke, Roccaforte, & Wengel, 1991; Yesavage et al., 1982). The GDS-15 includes 15-forced-choice questions with yes or no answers. A score of ⩾ 5 is considered a positive screen for the presence of depressive symptoms. Depression can influence cognitive functioning and mimic the clinical presentation of MCI. Therefore, it was essential to control for depression in the analysis. Depression may also decrease engagement in all types of activities, including music-related ones. In previous studies, depression was included as a covariate in the analysis of leisure activity in cognitively intact and impaired older adults (Sörman, Sundström, Rönnlund, Adolfsson, & Nilsson, 2014).
Analysis
To conservatively estimate the power required to detect a moderate Pearson correlation of 0.35 between musical and cognitive abilities measures at the 0.05 significance level (power = 0.80), we used a correlation observed in related literature (Müllensiefen, Avron, & Skiada, 2014; Müllensiefen, Gingras, Musil, et al., 2014). A power analysis revealed that 60 participants were required to detect a relationship between musical and cognitive abilities measures. We described the demographics of the overall and continuous measures of neuropsychological testing and musical abilities using means and standard deviations. We calculated Pearson correlation coefficients between measures of verbal episodic memory (word list learning, memory and recognition), processing speed (TMT A), executive function (TMT B), verbal fluency (animal list generation), verbal naming (BNT), visuoconstructive abilities (CDT), and the measure of musical abilities (GMSS and five subfactors). We generated the data analysis for this paper using IBM SPSS Statistics for Windows, Version 24.0. Armonk, NY: IBM Corp.
Results
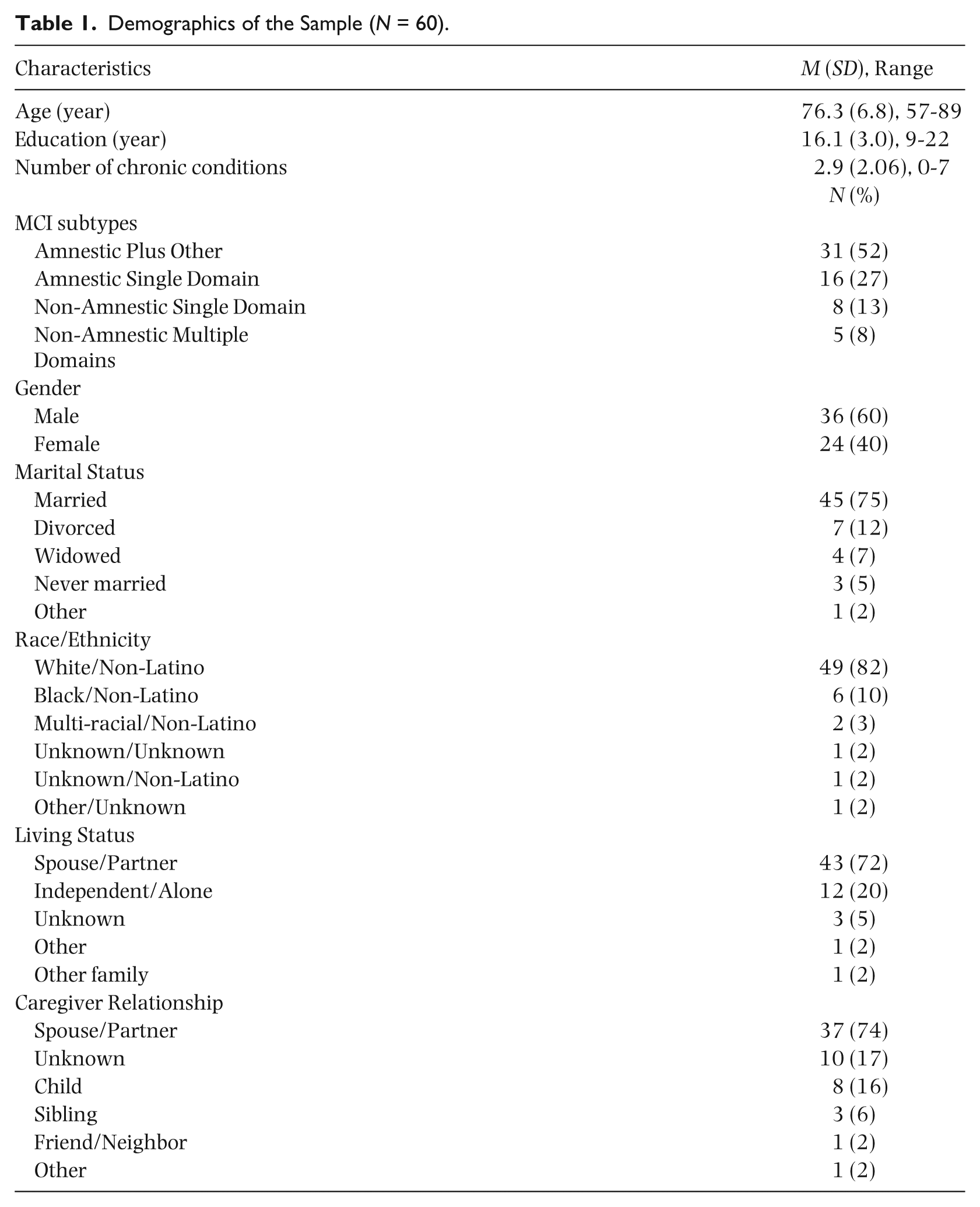
The sample consisted of 60 participants with a diagnosis of MCI. The demographic characteristics of the sample are summarized in Table 1. The mean age was 76.3 (SD = 6.8). Sixty percent of the sample was male. The participants were highly educated (mean years = 16.1), the majority were married (75%), predominantly White and non-Latino (82%), living with a spouse/partner (72%), and cared for by a spouse or a partner (74%). On average, participants had 2.9 (SD = 2.1) chronic conditions. Fifty-two percent of the sample was diagnosed with amnestic multiple domain MCI (Table 1) consistent with previous prevalence-based studies (Petersen et al., 2010; Ravaglia et al., 2008). The mean MMSE score among the participants was 25.8, consistent with the Petersen criteria for MCI (Table 2; Petersen, 2004). Participants’ scores for the neuropsychological assessment ranged between half a standard deviation below the average (Trail Making Test A) and nearly 2.5 standard units below the average (Word List Memory Recall; Table 2).
Demographics of the Sample (N = 60).
Neuropsychological and Depression Test Results (N = 60).
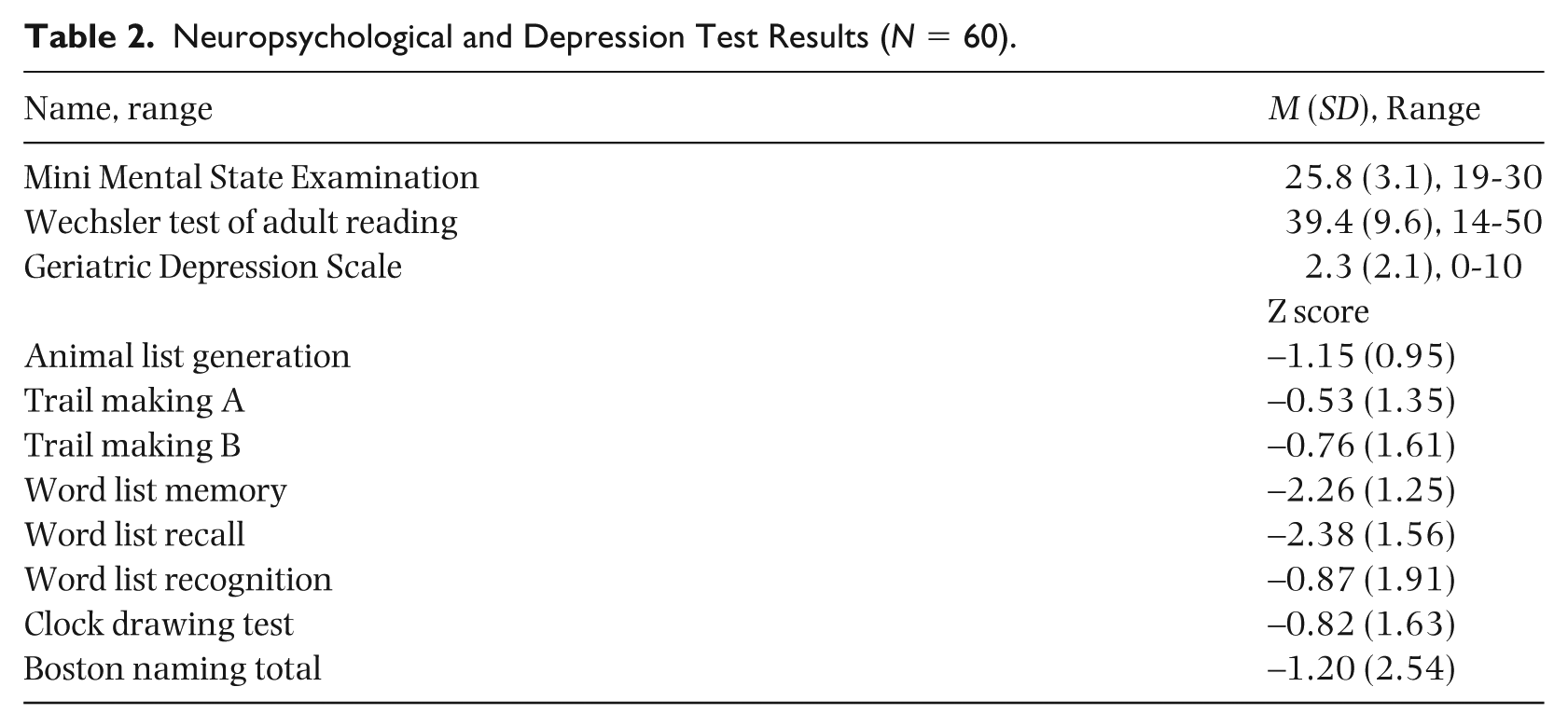
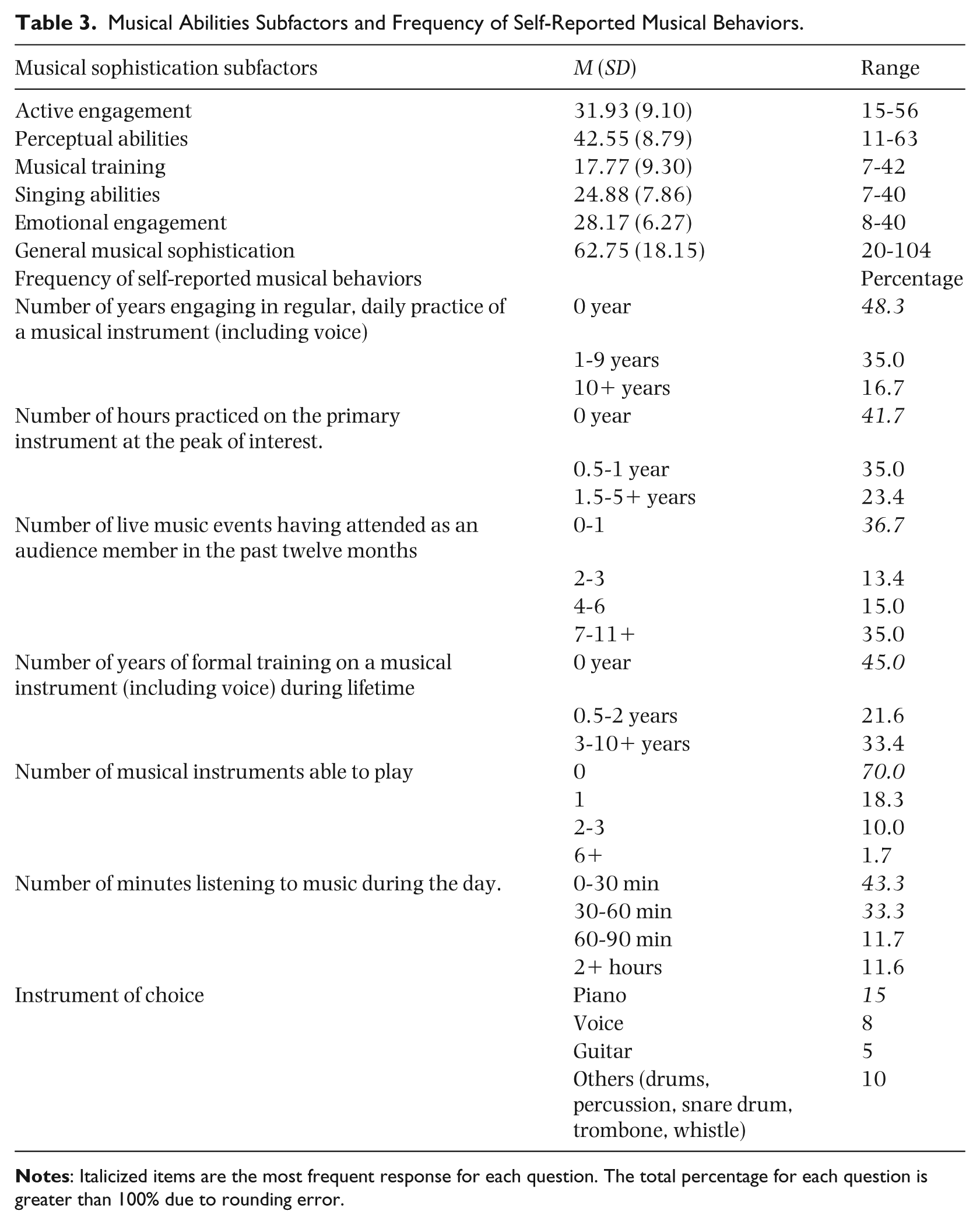
Figure 1 demonstrates the GMSS’ distribution. The participants scored in the nineteenth percentile on the GMSS compared to the non-age based published norms (Müllensiefen, Gingras, Stewart, & Musil, 2014). As shown, the scores for the GMSS are normally distributed and clustered around the mean with a possible bimodal distribution at the upper percentiles. The frequency of self-reported musical behaviors on the Gold-MSI is presented in Table 3. The mean GMSS score was 62.8 (SD = 18.2; Table 3). Nearly half of participants (48.3%) reported that they did not engage in regular, daily practice of a musical instrument. About a third of participants (35%) reported engaging in regular, daily practice of a musical instrument for between 1 and 9 years. Sixty-three percent of the sample did not report currently playing a musical instrument (Table 3). The GMSS Cronbach’s alpha in our study was 0.934.
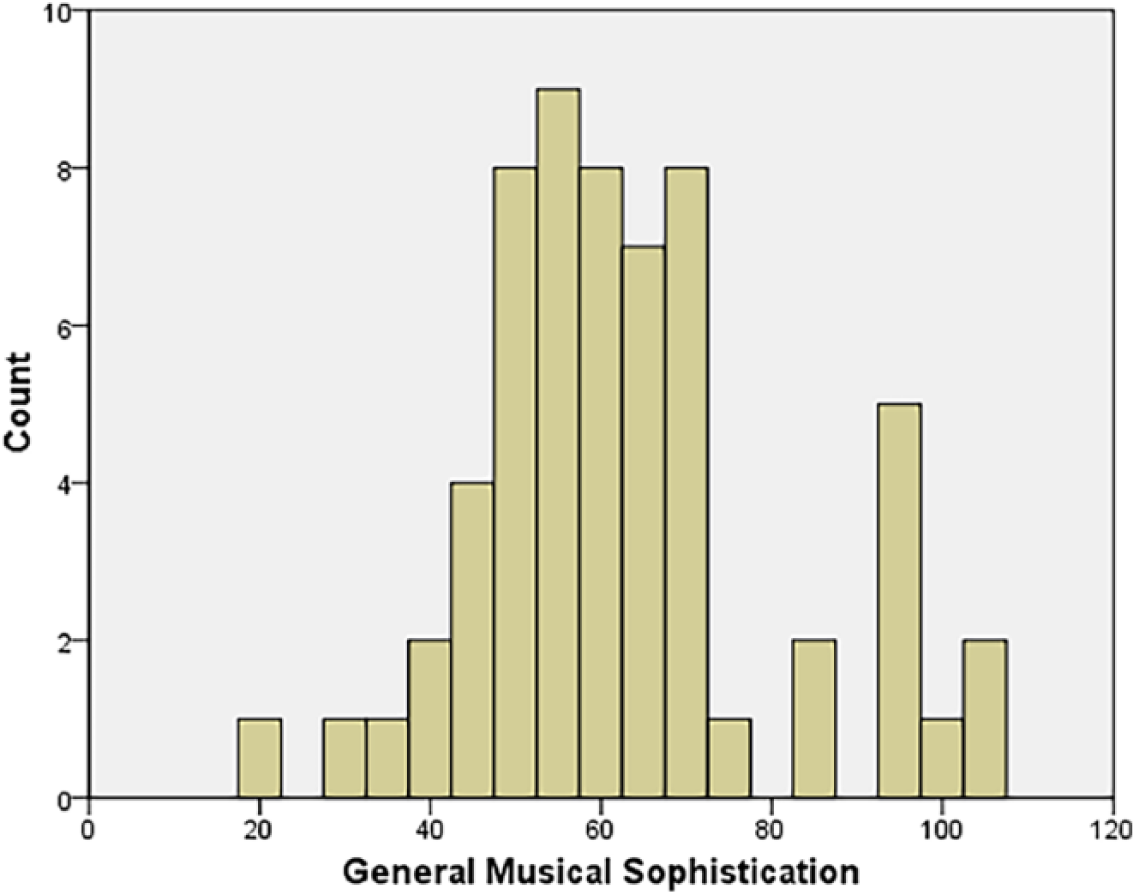
Distribution of scores on the General Musical Sophistication Subfactor: Count frequency.
Musical Abilities Subfactors and Frequency of Self-Reported Musical Behaviors.
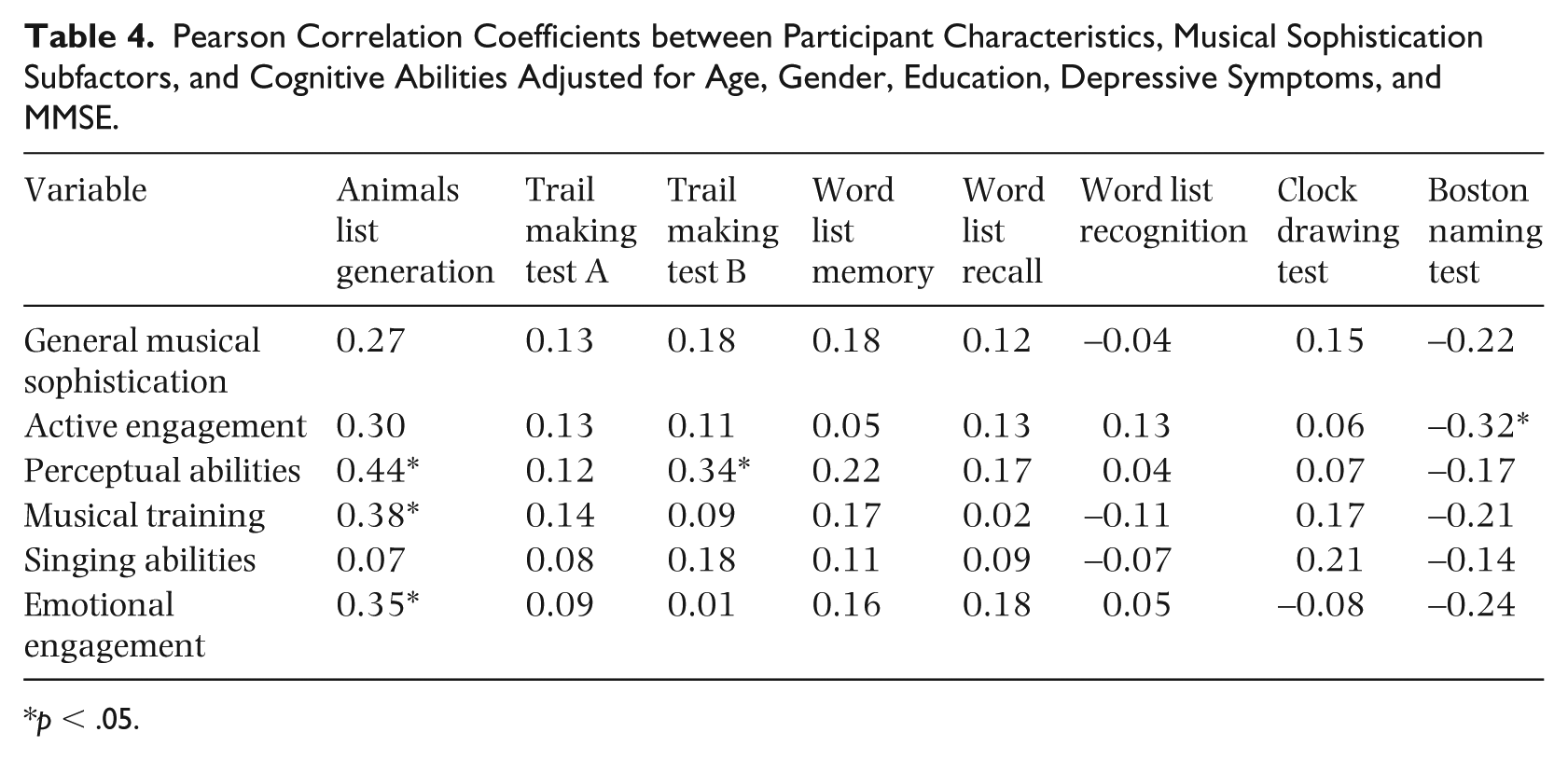
We found no significant correlations between GMSS and cognitive abilities (Table 4). With respect to musical sophistication subfactors, we found significant positive correlations between categorical fluency (animal list generation) and perceptual abilities, r = .44, p = .01, musical training, r = .38, p = .02, and emotional engagement, r = .35, p = .03. We also found significant positive correlations between executive function (TMT B) and perceptual abilities, r = .34, p = .04. A negative correlation was found between naming (BNT) and active engagement, r = -.32, p = .04.
Pearson Correlation Coefficients between Participant Characteristics, Musical Sophistication Subfactors, and Cognitive Abilities Adjusted for Age, Gender, Education, Depressive Symptoms, and MMSE.
p < .05.
Discussion
In summary, in this prospective, cross-sectional study we examined self-reported musical abilities in older adults with MCI. Older adults with MCI reported varying degree of musical abilities. Nearly half of participants reported that they did not engage in regular, daily practice of a musical instrument. About a third of participants reported engaging in regular, daily practice of a musical instrument for between 1 and 9 years earlier in their lives. Sixty-three percent of the sample did not report currently playing a musical instrument. When adjusting for key demographic and participant characteristics, we found modest associations between four musical ability subfactors (active engagement, perceptual abilities, musical training, and emotional engagement with music) and three cognitive abilities: verbal fluency, executive function, and verbal naming. Except for the emotional engagement with music subfactor, none of the remaining subfactors of musical abilities correlated with any demographic or participant characteristics. The participants, on average, scored lower on the general musical sophistication subscale compared to the published norms (Müllensiefen, Gingras, Stewart, et al., 2014).
Activities associated with musical abilities tend to peak at a young age (Müllensiefen, Gingras, Musil, et al., 2014). Bailey and Penhune (2012) argue for an existence of a sensitive period of musical training (prior to age 7), such that any formal musical training obtained prior to age seven may contribute to enhanced cognitive abilities later in life. Based on findings from the Müllensiefen, Gingras, Musil, et al. (2014) study, we expected older adults with MCI to report a lower frequency of musical activities compared to published norms. For instance, compared to younger adults, healthy older adults scored lower on the subscale of general musical sophistication, except for those older adults whose occupation required continuous involvement with music (Müllensiefen, Gingras, Musil, et al., 2014). Alternatively, older adults with MCI may choose not to partake in music-based activities due to their cognitive deficits. Previous research has demonstrated that participation in leisure activities declines with age (Agahi, Ahacic, & Parker, 2006). Furthermore, in a US nationally representative survey of older adults, individuals who screened positive for MCI had 8% less social engagement in the community compared to cognitively normal individuals (Kotwal, Kim, Waite, & Dale, 2016). Individuals with MCI may withdraw from social activities due to feeling anxious about their performance, both in the areas of language and memory. In addition, individuals with MCI may have more difficulty managing the tasks associated with engaging in these activities, such as coordinating social activities around music, managing transportation, and reading music. Taken together, the decline in musical abilities in healthy adults, along with the decline in persons with MCI participating in musical activities due to their perceived deficits, may help explain our finding of lessened musical abilities in older adults with MCI.
Given the breadth of musical abilities, older adults with MCI reported varying degrees of self-reported musical abilities. Using self-reported responses on the musical sophistication questionnaire, we gauged musical abilities in six major areas: active musical engagement, perceptual abilities, musical training, singing abilities, emotional engagement with music, and a general factor of musical abilities (GMSS). In addition, we asked participants to answer questions about the frequency of their musical behaviors, such as daily practice of a musical instrument, attending live music events, and listening to music in everyday life. Previous studies examining the benefits of instrument playing or singing used arbitrary cut off points for being a musician (Franklin et al., 2008; Hanna-Pladdy & Gajewski, 2012; Helmbold, Rammsayer, & Altenmüller, 2005). Similar to Slevc, Davey, Buschkuehl, and Jaeggi (2016), we chose a continuous measure of musical abilities to account for a range of musical abilities in our highly educated, urban sample and the fact that most of our participants did not have extensive musical experiences.
Previous research explored cognitive benefits associated with music-making in young adults (Helmbold et al., 2005) and cognitively intact older adults (Gooding, Abner, Jicha, Kryscio, & Schmitt, 2014; Mansens et al., 2017). Based on previous work, we hypothesized that musical abilities would be associated with several cognitive abilities in older adults with MCI, namely executive function and verbal episodic memory. Interestingly, we did not find any associations between the general subfactor of musical abilities and neuropsychological tests.
We did find, however, several significant associations between verbal fluency (gauged by the animal list generation test) and three of the musical abilities subfactors (perceptual abilities, musical training, and emotional engagement). Older adults who reported having better musical listening accuracy, greater musical training, and being emotionally engaged with music scored higher on the animal list generation test. These findings contradict results from the Mansens et al. (2017) study, where singing or playing a musical instrument was associated with better performance in letter fluency, but not category fluency, in 1101 cognitively intact adults age 64 and over. Furthermore, we found a weak correlation between perceptual abilities and executive function (measured by the TMTB). Similar to our findings, Slevc et al. (2016) found that musical ability is associated with a related, although different sub-domain of executive function – updating – in a sample of 96 college students. In our study, we found a negative correlation between naming and active engagement. Our findings are contrary to the study in which Hanna-Pladdy and Gajewski (2012) compared healthy older adults with less than ten years of music training to older adults with greater than ten years of musical training controlling for levels of general lifestyle activities and education. The researchers found that older adults with more than ten years of musical training scored higher on the test of verbal naming compared to older adults with less than ten years of musical training (Hanna-Pladdy & Gajewski, 2012). Similarly to Hanna-Pladdy and Gajewski (2012), in a recent study healthy older high-activity musicians showed cognitive benefits in executive function, language, and visuo-spatial ability when compared to low-activity older musicians (Strong & Mast, 2018).
These disparate findings may stem from several factors. First, since we did not measure musical ability objectively in our study, we cannot rule out the possibility that cognitive impairment may impact the accuracy of their responses on the musical abilities questionnaire. Previous research, however, suggests that self-reported musical abilities correlate with tests of musical abilities in a general population. For example, Müllensiefen, Gingras, Musil, et al. (2014) reported moderate correlations (r range 0.38–0.51) between self-reported general musical abilities (using the Gold-MSI) and actual listening tests in a large online sample (N = 136,924; mean age 35.2 years, SD = 15). Nevertheless, we cannot presume that this correlation is well-preserved in older adults and adults with impairments. Second, individuals with MCI may have difficulty recalling recent events possibly influencing their ability to accurately respond to the questionnaire items. Third, while using a questionnaire of musical abilities that covers a broader spectrum of subjective musical abilities beyond objective measures of musical training and creates a continuous variable of musical abilities can be a strength, the breadth of musical abilities questions may have contributed to some of our null findings. In addition, our sample did not contain many participants with 10+ years of training, contributing to a sample bias issue.
There are limitations to our study. First, cross-sectional data do not support a causal relationship between musical and cognitive abilities making it impossible to conclude that greater musical abilities result in worse performance on the verbal naming domain. Second, we did not ask participants in this study about their involvement in other leisure activities. Participation in leisure activities may be a confounding factor that may influence participation in music related activities. For instance, individuals with MCI may isolate themselves from social activities, including music. Alternatively, in doing so persons with MCI may engage with music at home. The index of musical abilities might not have been reliable in persons with MCI. Several statements in the questionnaire rely on participants’ memory. Older adults with MCI typically can recall remote memories, but are impaired on recall of recent memories. They may have had an intact sense of their musical abilities at an earlier time in their lives, but possibly, due to their mild memory deficits, lacked the insight into their present musical abilities. Additionally, we did not include a group of cognitively intact older adults to compare how musical abilities in participants with MCI differ from a control group. We hypothesize that cognitively intact older adults may have been more accurate in recalling recent events and had more insight into their current abilities compared to older adults with MCI. Lastly, the sample was not a random sample from a community population and consisted mainly of White, highly-educated older adults participating in a longitudinal study.
This study has many research implications. Future studies need to consider larger, more diverse samples, followed longitudinally to better establish the validity and generalizability of these findings. Adding an objective measure of musical ability can provide a more accurate representation of musical abilities in older adults with MCI as participants may have overestimated or underestimated their musical abilities. Additionally, obtaining a collateral source report (from someone who knows the individual well) may provide a more complete understanding of the nature of musical abilities in persons with MCI. Future studies should also control for the level of leisure activity participation and use an established index of comorbid illnesses. Finally, given the interest in protective and compensatory strategies that delay the MCI-AD conversion, future investigations should compare conversion rates in older adults with high vs. low degrees of musical ability.
Conclusions
In this cross-sectional study, we examined the extent and nature of self-reported musical abilities in sixty persons with MCI. Our study findings provided further support for the relationship between musical and cognitive abilities in older adults with MCI. The findings, however, were not consistently in the expected direction. The index of musical abilities relies heavily on self-assessment of current musical abilities, which may be hindered by the mild memory deficits in persons with MCI. Larger longitudinal studies with more diverse samples including subjective, objective, and collateral source measures are needed to better establish the link between musical and cognitive abilities.
Footnotes
Acknowledgements
We are most grateful to Liming Huang who provided statistical support during data analysis.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Darina V. Petrovsky was a 2014–2016 National Hartford Centers of Gerontological Nursing Excellence Patricia G. Archbold Scholar and a 2014–2016 Jonas Nurse Leader Scholar. This work was supported by the National Institute on Aging of the National Institutes of Health under grant number F31AG055148, the Mayday Fund, and the University of Pennsylvania School of Nursing Office of Nursing Research. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.