
Abstract
The aim of this study is to evaluate the effectiveness of an intervention program, based on music, movement, and dance, aimed at improving motor skills in children at risk of developmental coordination disorder (DCD). Participants comprised 70 primary school children (47 boys/23 girls) aged between 6 and 8 years. Participants were given the Spanish adaptation of the Movement Assessment Battery for Children–Second Edition (MABC-2) to identify difficulties and initially classify into three groups: a group of 17 at risk of DCD who participated in the intervention program (Experimental Group), a group of 18 at risk of DCD who did not participate (Control Group with Risk) and a group of 35 children, with scores higher than the cutoff point (Control Group without Risk). The results show a significant improvement in the motor skills of children who participated in the intervention program, while those in the Control Group showed no significant changes in the second evaluation compared with the first. Likewise, it could be affirmed that this intervention based on group activities involving music, movement, and dance is a very successful blend for motor improvement in children with coordination problems, due to the combination of cognitive stimulation areas and techniques.
Developmental coordination disorder (DCD) is a relatively new pathology in scientific studies with increasing relevance due to its high prevalence in children (between 5% and 8%; Barnhart, Davenport, Epps, & Nordquist, 2003; Chan, 2007; Dewey, Kaplan, Crawford, & Wilson, 2002; Ferguson, Jelsma, Versfeld, & Smits-Engelsman, 2014). This pathology still presents many basic uncertainties such as its definition and diagnosis, although many authors (Deconinck et al., 2007; Dewey et al., 2002; Vasconcenlos, Rodrigues, Barreiros, & Jacobsohn, 2009; Visser, 2003) have adopted the Diagnostic Criteria for DCD by the American Psychiatric Association (2013), recently updated in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders.
As it is not a simple disorder, there are difficulties in its definition as it can be found in isolation, but is also commonly linked with other disorders such as attention deficit hyperactivity disorder (ADHD; Niemeijer, 2007), learning difficulties or dyslexia (Dewey, Wilson, Crawford, & Kaplan, 2000), language disorder (Dewey & Wall, 1997; Hill, 1998), or autism spectrum disorder (Gilberg & Kadesjö, 2003).
Different longitudinal studies (Cantell, Smyth, & Ahonen, 2003; Cousins & Smyth, 2003; Geuze & Börger, 1993; Losse et al., 1991) show that after a long follow-up of children with coordination difficulties, these are still present between 6 and 10 years later. In the same way, Camden, Wilson, Kirby, Sugden, and Missiuna (2014) highlight the difficulties in overcoming DCD by defining it as a chronic disease.
With regard to treatment, during the past 50 years, numerous proposals have been put forward classified according to Sugden and Wright (1998) into two basic categories: process-oriented approaches, whose purpose is to improve motor functioning to directly improve the performance and motor competence of children; and task-oriented approaches focused on learning the specific tasks or group of tasks in which the child has difficulties. Both approaches have developed treatments with satisfactory results, which is why some authors (Barnhart et al., 2003; Cantell, Smyth, & Ahonen, 1994; Gibbs, Appleton, & Appleton, 2007; Rasmussen & Gillberg, 2000) conclude that whatever the orientation of the approach, treatment is needed for improvement of DCD, as it has been shown that without intervention, motor coordination problems are difficult to overcome.
There are numerous studies for proposals to improve DCD, mainly from the field of physiotherapy and psychology (Chan, 2007; Dunford, 2011; Hung & Pang, 2010; Niemeijer, 2007; Zwicker et al., 2015). However, intervention programs based on music and movement/dance are very rare, which is unusual if one considers the benefits that these contribute to the child’s development, as verified by numerous studies (Bermell, 2000; Bradt, Magee, Dileo, Wheeler, & McGilloway, 2010; Hodges, 2000; Ruíz Palomo, 2008; Schaefer, Morcom, Roberts, & Overy, 2014). Ruíz Palomo (2008) states that music plays an essential role in acquisition of motor coordination, body language, concentration, and verbal language. Similarly, Cao, Lacruz, and Pais (2011) also showed improvements in attention in their study, along with memory, body awareness, and spatial structuring through cognitive stimulation by means of motor development. Dey et al. (2012) state that making music improves motor skills and Mado Proverbio, Manfredi, Zani, and Adorni (2013) argue that music modifies the functional structure of the brain and connectivity. Going deeper into this topic, Schaefer et al. (2014) show that a combination of music and movement produces cognitive improvements, with greater benefits when working synergistically than both separately, enhancing neuroplasticity and positively influencing cognitive abilities. They specifically claim that there are areas of the cerebellum responsible for motor movement activated by listening to music, highlighting the connection between cognition and motor coordination.
Jauset (2016, p. 23) has corroborated that “the execution of movements accompanied by music stimulates various brain areas of both hemispheres related to motor aspects and cognitive functions, such as planning and care.” Similarly, he verifies that musical practice involves the use of cognitive actions such as memory and attention, and motor skills like planning and performing movements, among others, which encourages the development of a more efficient network of neuronal connections. In addition, this author asserts that this means an increase of physical–corporal equilibrium allowing a succession of structural changes in the corpus callosum, cerebellum and prefrontal, auditory and premotor cortices. The same occurs with dance, which promotes structural brain transformations in the hippocampus, cortical motor areas, parietal lobe, and cerebellum (Jauset, 2016).
Based on ideas in the aforementioned publications on DCD and those that defend and prove the effectiveness of music and movement for cognitive and physical improvement, the general aim of this study is to evaluate the effectiveness of an intervention program, based on music, movement, and dance, aimed at improving motor skills in children at risk of DCD.
Method
Participants
Participants were 114 children (68 boys and 46 girls) aged between 6 and 8 years studying first, second, and third grade of primary school in four Public Primary Education Centers of the Region of Murcia (Spain). Parents provided informed consent according to the Bioethics Commission of the University of Murcia and the Research Ethics. Participants were given the Spanish adaptation of the Movement Assessment Battery for Children–Second Edition (MABC-2; Henderson, Sugden, & Barnett, 2012) to identify difficulties and initially classify them into two groups: children with a risk of DCD and children without. Children whose standard score was ⩽7 on the global test or as a percentile was ⩽16 (below this score is considered a serious risk zone for motor coordination problems) on the first administration of the battery were assigned to the treatment group (n = 35). However, as the group was too large for the intervention to be effective, a smaller group was selected. Considering that one of the four educational centers had a high number of children with scores below the cutoff point (n = 17), it was decided to only do the intervention with the students of this particular center, since another 18 children belonged to three different schools.
Participants who scored higher than the cutoff point (children without risk of DCD) were matched for age and gender with those who presented risk of DCD. We used a final sample in this study of n = 70 children divided into three groups: a group of 17 at risk of DCD who participated in the intervention program (Experimental Group [EG]), a group of 18 at risk of DCD who did not participate (Control Group with Risk [CGR]), and a group of 35 children, with scores higher than the cutoff point (Control Group with No Risk [CGNR]).
Instrument
The instrument used for motor assessment of this study was the MABC-2 (Henderson et al., 2012). Justified by its suitability for determining these types of difficulties and its validity is supported by its use in many research studies and by numerous authors (Batey et al., 2014; Ferguson, Duysens, & Smits-Engelsman, 2015; Hung & Pang, 2010; Jelsma, Geuze, Mombarg, & Smits-Engelsman, 2014; Liberman, Ratzon, & Bart, 2013; Niemeijer, 2007; Peters, 2006; Roebers et al., 2014; Schoemaker, Niemeijer, Reynders, & Smits-Engelsman, 2003). The MABC-2 allows researchers to determine with remarkable accuracy the presence of coordination difficulties in children and adolescents (4–16 years old) through four age-related batteries that measure different aspects of motor skills (manual dexterity, aiming, catching, and static and dynamic balance).
Procedure
A meeting was held with the teachers from the school groups involved, families of selected students were informed, and consent was provided to guarantee the children’s anonymity and privacy in compliance with Spanish Law 15/1999 of 13 December. Tests were initially carried out on the global sample during school hours, with a total duration of approximately 100 hr (35 days). Once the results were analyzed, there was an informational meeting with the families of the proposed children to participate in the intervention program.
The program was carried out in 10 weekly sessions of 50 min, with varied activities of short duration (between 5 and 15 min), to streamline session dynamics and avoid attention problems. The design of the exercises is mainly based on the playful aspect and distributed into three types: (a) games with song, (b) games without song, and (c) dance games.
Following implementation of the program, a posttest evaluation of the entire sample’s performance on the MABC-2 test was done.
Data analysis
To evaluate the effectiveness of the intervention program, empirical research was designed where the independent variable was manipulated through an “assignment variable,” used to include participants in the intervention program. The “assignment rule” was the cutoff point established in the MABC-2 Battery, to classify children according to their performance in the risk condition of DCD. A design with the nonequivalent Control Group was used and, within this design, for data analysis, the Change Model was selected in which the allocation variable is considered to directly affect pretest and posttest, but where pretest does not directly affect posttest. In this type of statistical analysis, an ANOVA with change scores is used as a response variable obtained through calculation of the difference between posttest and pretest, so treatment effect is the average change between the experimental and control groups (Ato & Vallejo, 2015).
To evaluate the effectiveness of the intervention program, the change scores were calculated from the pretest and posttest scalar scores of the total test score of the MABC-2 Battery, Manual Dexterity, Aiming and Catching, and Balance dimensions. In the ANOVA, the change score for each measure of the MABC-2 Battery was taken as the response variable and as a fixed factor the group variable with two levels: an EG (children at risk with intervention) who were given the intervention program and a control group that did not participate in the program.
For all comparisons, a difference with p < .05 was considered significant. The program used for statistical analysis was Version 24.0 for Windows of the statistical package SPSS.
Results
Table 1 shows that both the total test score and the scores of the three dimensions comprising the MABC-2 Battery underwent a significant change in the group of children participating in the intervention program (EG), while the other two groups showed a slight variation in the means of both pretest and posttest measures, especially in the CGR who did not participate in the intervention program.
Descriptive analysis of the total test score and dimensions of MABC-2 for CGNR, CGR, and EG.
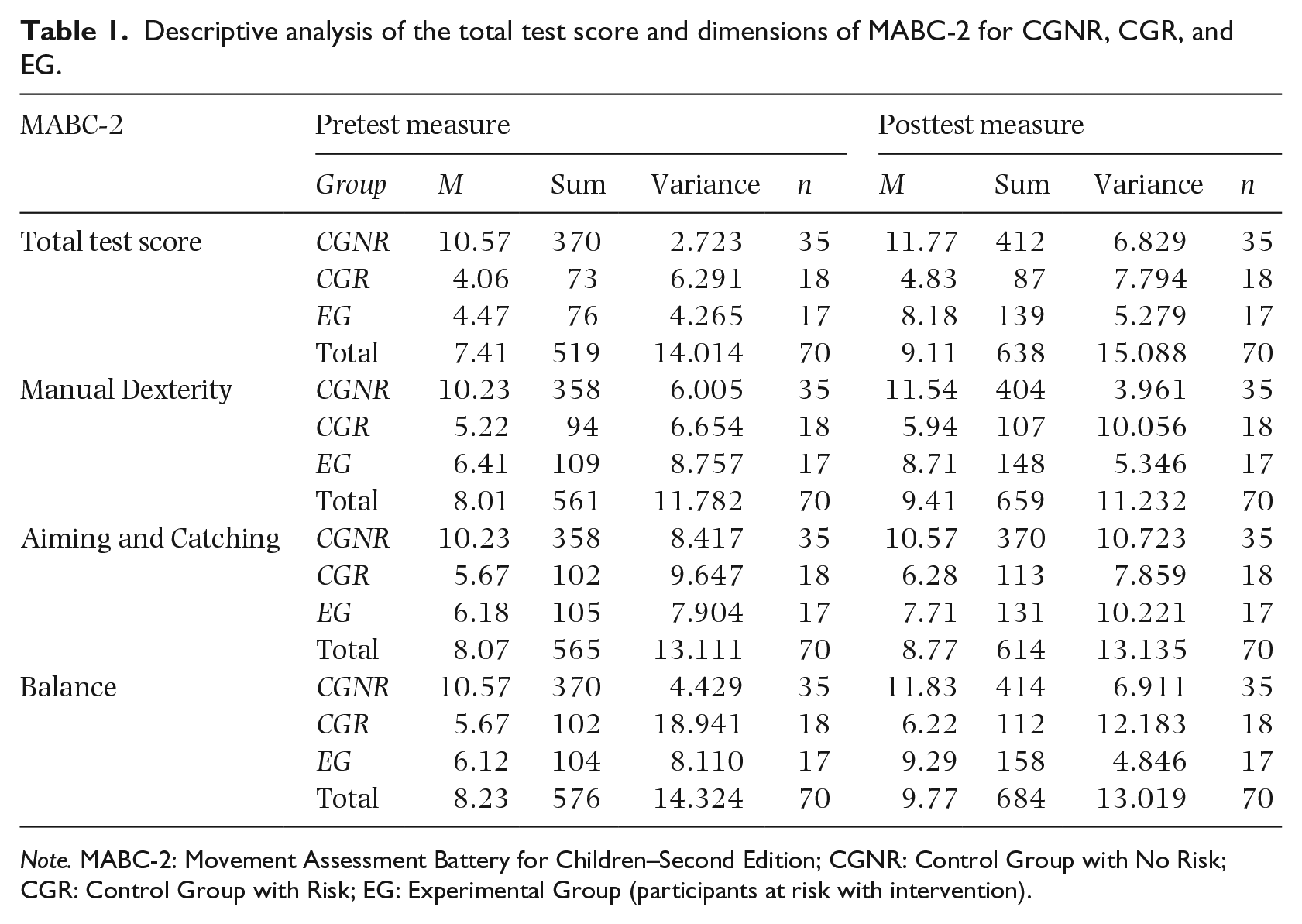
Note. MABC-2: Movement Assessment Battery for Children–Second Edition; CGNR: Control Group with No Risk; CGR: Control Group with Risk; EG: Experimental Group (participants at risk with intervention).
Regarding the Student’s t-test for paired samples for the three groups separately comparing the pretest and posttest measures of the response variable (Battery MABC-2), the results for CGR showed no significant differences in the total test score before the intervention program (M = 4.06, SE = .591) and after it (M = 4.83, SE = .658), t(17) = − 1.903, p > .05, r = .42. These results were similar for the other dimensions (Table 2).
Mean and standard deviation.
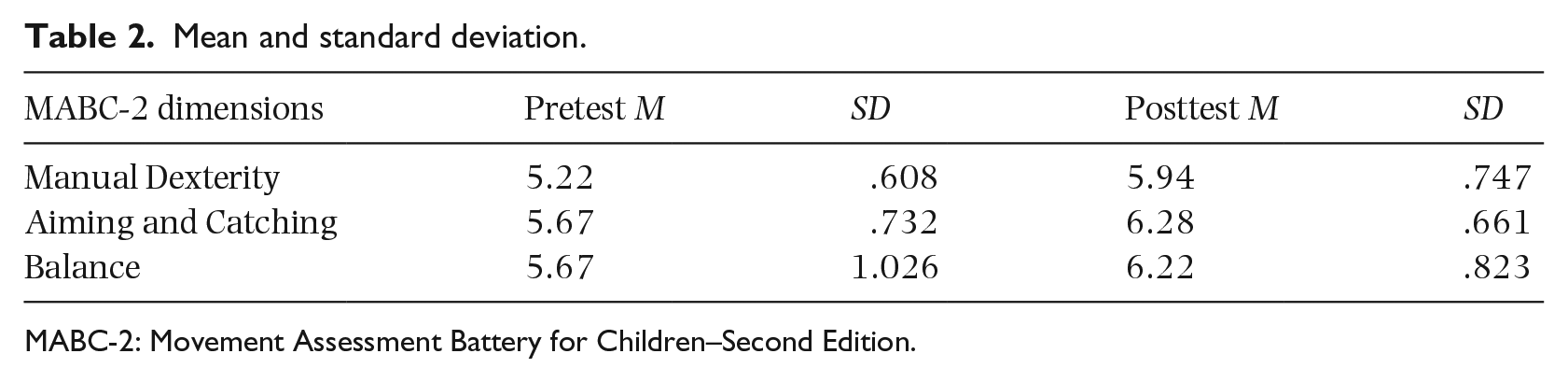
MABC-2: Movement Assessment Battery for Children–Second Edition.
The results of the Student’s t-test for the CGNR are quite different from previous ones. In this case, with the exception of the Aiming and Catching dimension, where scores in the pretest phase (M = 10.23, SE = .490) were not significantly different from those obtained in the second evaluation (M = 10.57, SE = .554), t(34) = −.430, p > .05, r = .07, the rest of the measures showed a significant increase in the posttest phase. The total test score of the MABC-2 Battery of the children from CGNR in particular was significantly lower in the pretest phase (M = 10.57, SE = .279) than the second evaluation (M = 11.77, SE = .442), t(34) = −2.991, p < .05, r = .46. Likewise, their performance in Manual Dexterity was significantly lower in the first administration of the battery (M = 10.23, SE = .414) than the second (M = 11.54, SE = .336), t(34) = −4.079, p < .001, r = .57. This same pattern of results was maintained in the Balance dimension, with significantly lower pretest scalar scores (M = 10.57, SE = .356) than those obtained in the second evaluation (M = 11.83, SE = .444), t(34) = −2.807, p < .05, r = .43.
As for the EG, its output results were similar to those of participants in the CGNR. However, Student’s t-test results for the EG showed significant differences for the total test score, Manual Dexterity, and Balance dimensions. Specifically, the total test score of the EG children was significantly lower before the intervention program (M = 4.47, SE = .501) than after (M = 8.18, SE = .557), t(16) = −8.354, p < .001, r = .90. Similarly, their performance in Manual Dexterity was significantly lower before the intervention program (M = 6.41, SE = .718) than after (M = 8.71, SE = .561), t(16) = −4.474, p < .001, r = .74. This same pattern of results was maintained in the Balance dimension, with significantly lower scalar scores before intervention (M = 6.12, SE = .691) than after the program (M = 9.29, SE = .534), t(16) = −4.215, p < .005, r = .72. However, in the Aiming and Catching dimension, improvement produced after the intervention phase was not statistically significant, t(16) = −1.879, p > .05, r = .42.
Finally, to analyze the effectiveness of the intervention program, we chose an ANOVA where change scores were taken as a response variable, obtained from the calculation of the difference between the posttest and pretest scores of each MABC-2 Battery test, while the group was used as a fixed factor. In this case, the results are presented in two separate blocks: the first presents the results for the EG and the CGNR, while the second shows those for the EG and the CGR. In both the cases, the assumption of homoscedasticity was previously checked through the Levene test, which yielded p > .05 for all scores of the MABC-2 battery, so there is the assumption of similarity or equality of variances.
In the first block of results where factor levels were EG and CGNR, the effectiveness of the intervention program was verified, as it was observed that the mean change was significantly higher in children of the EG than in the CGNR (Table 3), specifically the parameter estimate for the CGNR, a β(1,50) = −3.828, p < .001, in the Total Test Score of the MABC-2 Battery.
ANOVA with change scores as a response variable according to the group (CGNR and EG).
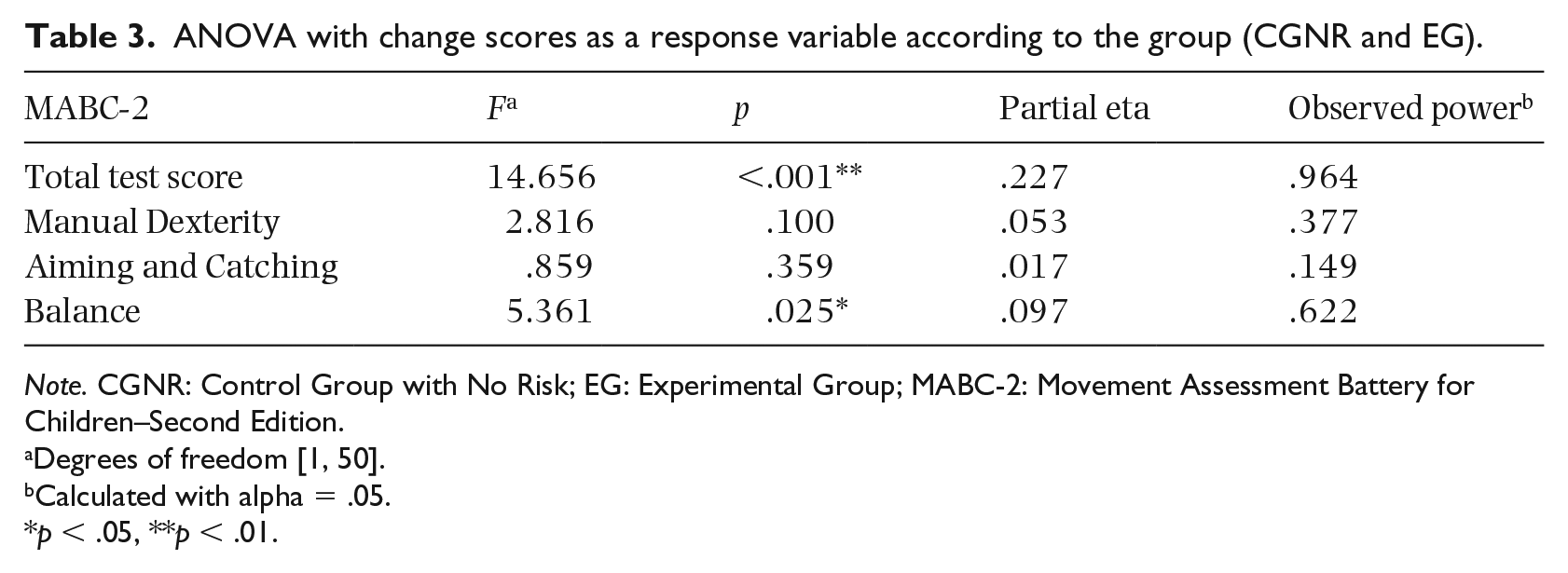
Note. CGNR: Control Group with No Risk; EG: Experimental Group; MABC-2: Movement Assessment Battery for Children–Second Edition.
Degrees of freedom [1, 50].
Calculated with alpha = .05.
p < .05, **p < .01.
In the second block of results where the factor levels were EG and CGR, the effectiveness of the intervention program could also be observed because, as seen in Table 4, the average change in the total test score was significantly higher in children of the EG than the CGR, and in the Manual Dexterity and Balance dimensions. However, these differences were not significant for the aim and catching dimension.
ANOVA with change scores as a response variable according to the group (CGR and EG).
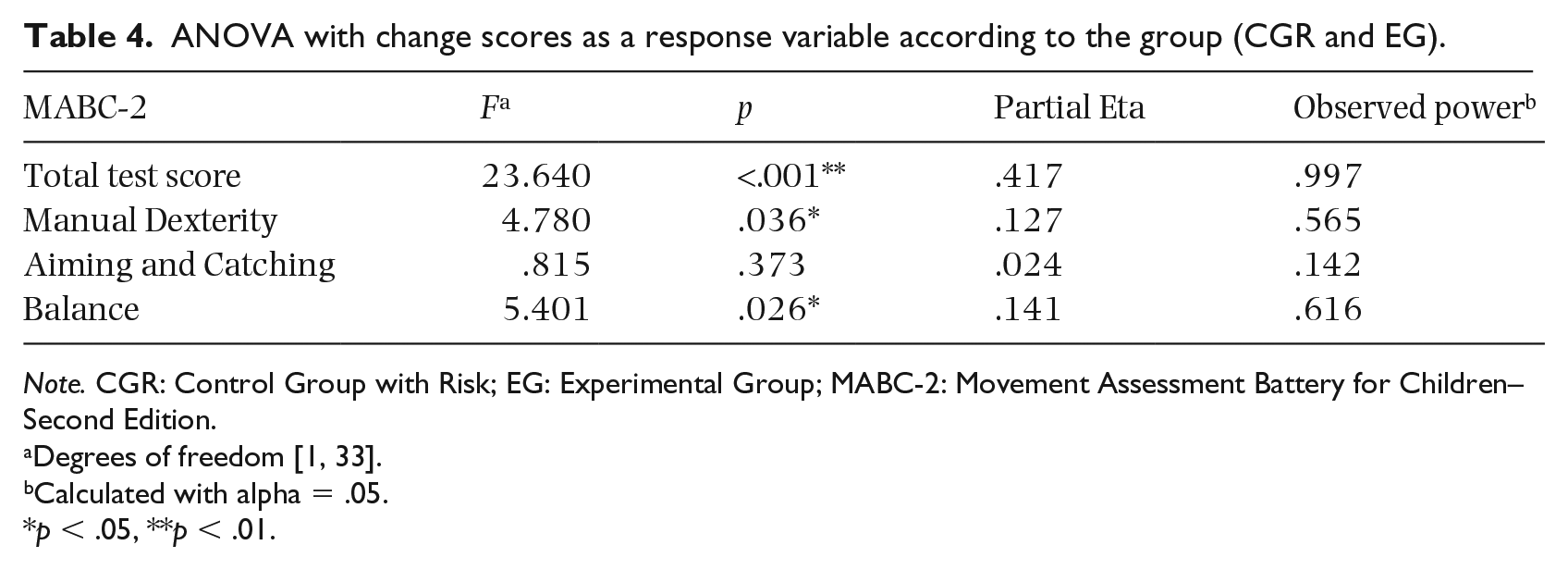
Note. CGR: Control Group with Risk; EG: Experimental Group; MABC-2: Movement Assessment Battery for Children–Second Edition.
Degrees of freedom [1, 33].
Calculated with alpha = .05.
p < .05, **p < .01.
Finally, as with the first block of results, although differences in the Aiming and Catching dimension were not statistically significant, change in the EG was superior.
Discussion
The results obtained following the study show a significant improvement in the motor skills of children who participated in the intervention program, while those in the CG showed no significant changes in the second evaluation compared with the first. This aspect is relevant, if we consider all children continued taking part in music and physical education activities at their educational centers. However, only those participating in the intervention showed significant changes in motor performance. In addition, it should be noted that these children had significant difficulties in coordination skills, which showed considerable improvement after treatment. This highlights the effectiveness of intervention through a program based on dance, movement, and music activities.
It should also be noted that the distribution of experimental sample and design of activities are essential for treatment success, so the performance of group intervention was based on the additional benefits that this provides to participants. Hung and Pang (2010) show the effectiveness of group interventions which are as effective as individual interventions, but with the added incentive of the socializing and motivating power that group activities entail. The objective-oriented group intervention proposed by Dunford (2011) for children with DCD, combining motor learning with cognitive strategies, could be highlighted. Likewise, it could be affirmed that this intervention based on playful group activities involving music, movement, and dance is a very successful blend for motor improvement in children with coordination problems, due to the combination of cognitive stimulation areas and techniques. This is verified by observing that the totality of the sample integrating the EG presents considerable improvements in posttest compared with pretest, even reaching almost equal to CGNR scores (children without motor difficulties). In the same way, it is remarkable how both CGNR and CGR do not present a positive evolution as accentuated as the EG. All children participating in the intervention program improve their motor skills and many even leave their difficulties behind and reach scores in the MABC-2 considered outside the risk level of motor coordination problems.
On the contrary, the CGR, comprising children with coordination difficulties, does not present important changes, maintaining very low scores, with a very narrow progress range and with participants with considerably worse results. Starting from equality of conditions in both the risk groups (EG and CGR), with 100% of samples below the scalar score 7 (with an average around score 5 of the MABC-2), following completion of the intervention sessions, posttest reveals that children with motor coordination difficulties do not evolve in the EG as in CGR. Posttest results test the suitability of the intervention program to keep the CGR below the score indicating motor problems, while the EG scores reach up to 4 points in some cases, showing a more than significant improvement. This shows the importance of intervention in children with low motor competence, while demonstrating the effectiveness of the intervention.
The performance of the CGNR was slightly lower in the posttest phase, showing scores similar to the children of the EG group after the intervention. This is, therefore, further evidence of the effectiveness of the intervention program. This intervention, despite being short, allows children with motor coordination difficulties to begin rehabilitating many of their shortcomings and provides them with the opportunity to strengthen brain areas which brings numerous associated benefits, such as improvements in attention, memory, spatial structuring, planning, or order, aspects where they usually present deficiencies.
The effectiveness of the intervention is also shown in significant advances that occur in each skill evaluated by the MABC-2 test. In Manual Dexterity, evolution is positive in the three groups, but although in the CG, the results hardly change from pretest to posttest, in the EG the advance is considerable. This inequality evidences the need for treatment in children with problems so they can be placed in a range similar to the rest of the child population without motor difficulties. Games played during the intervention program in which fine motor skills, motor integration, and manual dexterity are worked on, despite not being the most frequent and being of short duration were a great help in improving the skills of the experimental sample.
Pless and Carlsson (2000), after their meta-analysis of different intervention programs, conclude with the convenience of not randomly assigning the group samples, that is, they support the creation of a classification adjusted to the characteristics or measurements obtained by the participants, as done in this study for the division of the three groups (EG, CGNR, and CGR). Having two control groups (CGNR of children without difficulties and CGR of children with risk of DCD) to which the intervention was not applied, grants greater results reliability compared with other studies where they evaluate treatment programs, as with Martini and Polatajko (1998), Schoemaker, Hijlkema, and Kalverboer (1994), Wright and Sugden (1996) or Zwicker et al. (2015), where there was no control group. In particular, the usefulness of the CGR is clear when addressing the results. As in research such as Niemeijer (2007) or Schoemaker et al. (2003), it has been proven that after more than 3 months, the performance of these children with DCD who have not participated in the intervention remains practically the same as a deficit. Therefore, it is logical to deduce that the progress observed in EG is due to the treatment provided.
Likewise, application of early intervention in the first years of schooling is justified by numerous authors (Missiuna, Rivard, & Pollock, 2011; Pless & Carlsson, 2000; Schoemaker et al., 2003; Sugden, 2007; Taylor, Fayed, & Mandich, 2007), opinions that have guided the preparation of the sample and whose results prove the convenience of such selection. Taylor et al. (2007, p. 128) support the “theory that young children can be able to modify their own cognitive processes through training in skills such as planning, checking and monitoring,” so they are “able to draw on metacognitive strategies to improve on tasks that are meaningful to them.” Understanding that metacognition is the faculty of a person to analyze their thought processes and the way in which they learn, this ability allows knowing and adjusting the basic mental processes that intervene in knowledge. Therefore, bearing in mind that children presenting coordination difficulties and problems in skills learning do not have to present lesser metacognition to older children, we do not have to wait until they are older to perform an intervention. Early treatment prevents advance of difficulties of the disorder or that its consequences affect physical or mental wellbeing.