
Abstract
Popular (i.e., nonclassical) musicians have higher rates of depression, anxiety, and alcohol misuse than the general population. In this study, occupational and financial stresses were hypothesized to be associated with depression, anxiety, and alcohol misuse in popular musicians. An online cross-sectional survey was sent to a sample of popular musicians who had received mental health services in the preceding 2 years (n = 655). Validated measures were used to represent the key constructs. A total of 317 musicians (48.4%) completed the survey; 45.4% endorsed significant occupational stress and 81% rated their financial stress as high or overwhelming. Over 36% reported moderate to severe depression, 33.5% expressed similar levels of anxiety, and 65.4% screened positive for alcohol misuse. Univariate tests showed a strong association between occupational stress and depression (odds ratio [OR] = 3.62; 95% confidence interval [CI] = [2.6, 5.0]) and anxiety (OR = 3.05; 95% CI = [2.2, 4.2]). Financial stress also was associated with depression (OR = 1.90; 95% CI = [1.6, 2.2]) and anxiety (OR = 1.72; 95% CI = [1.5, 2.0]). Multivariate analyses showed statistical associations between both occupational stress and financial stress with depression and anxiety persisting when adjusted for by the other variables. Alcohol misuse was not associated with occupational or financial stress. Occupational and financial stresses are strongly associated with depression and anxiety in popular musicians seeking mental health treatment. Future studies should include musicians not engaged in mental health treatment to determine the generalizability of these findings. More research is needed to identify confounding variables associated with musician occupational and financial stress and alcohol misuse.
Music—what a noble art, what a terrible profession
Professional performers of contemporary musical genres—sometimes referred to as “popular” musicians to distinguish them from their classical counterparts—are highly susceptible to mental illness. Studies show significant numbers of popular musicians endorsing a mental health issue affecting their performance in the past year, including depression (20%–51%) and anxiety (12%–26%) (Brodsky, 1995; Chesky et al., 2002; Krueger & Zhen, 2018; Raeburn et al., 2003). A national survey of British musicians revealed lifetime depression and anxiety rates of 69% and 71%, respectively, almost three times higher than the general population (Gross & Musgrave, 2016). Musicians also have higher rates of risky alcohol consumption and substance misuse compared with the general population (Krueger & Zhen, 2018; Parker, 2015). Anxiety, depression, and alcohol and substance use disorders are significant suicide risk factors and may provide a partial explanation for alarming musician suicide rates. A retrospective study of over 12,000 musicians found suicide rates to be between 2 and 7 times the national average (Kenny, 2016). Census death records from 1990 showed a musician suicide rate of 42.6 per 100,000, or 3.4 times greater than the general population (Stack, 2009; Suicide.org, n.d.). Musicians are included in the Centers for Disease Control and Prevention’s occupational group that from 2012 to 2015 showed the largest increase in suicide among males (47%) and the highest overall female suicide rate (Peterson et al., 2018).
Musicians and other artists have been theorized to be constitutionally predisposed to mental illness due to their creative temperament (Andreasen & Canter, 1974). Early research found high rates of mental illness in eminent writers and other artists, including bipolar disorder in particular (Andreasen & Canter, 1974; Jamison, 1989). Although these studies have been criticized because of small sample size and selection bias, large national registry studies also point to a genetic creativity–mental illness link (Kyaga et al., 2011; MacCabe et al., 2018; Power et al., 2015; Rothenberg, 2001). Genetic markers associated with schizophrenia and mood disorders in these studies, however, only accounted for approximately 0.25% of the variation in subjects’ presumed artistic ability (Sample, 2015).
Social determinants of mental health, including occupational and financial stress, may be more salient contributors to musician mental health burden. Many popular musicians are freelance workers and vulnerable to the precarious nature of a hypercompetitive music industry. A lack of predictability in performance schedules makes social and financial planning difficult. Music-related earnings are often insufficient, causing musicians to seek additional part-time service industry work or give music lessons to allow for touring flexibility. Touring is often associated with difficult physical work conditions, interpersonal conflicts, erratic sleep schedules, and prolonged separations from family and social supports. Many musicians consider their work a calling, yet are frustrated as talent and persistence do not necessarily translate to greater opportunity or success. Those that do find their music careers advancing often struggle over artistic control with producers and other decision-makers in the industry. Compared with the general workforce, musicians report higher levels of job demands, less perceived support, feel less rewarded both in terms of salary and acknowledgment, and endorse higher levels of work–family conflict and less work motivation (Détári et al., 2020).
Researchers Geoffrey Wills and Cary Cooper conducted seminal studies of popular musician occupational stress in the 1980s, including in-depth interviews and surveys with professional popular musicians about perceived work stressors (Cooper & Wills, 1989; Wills & Cooper, 1988). They identified a number of stressors, including performance anxiety, perceived public ignorance and low esteem of their musicianship, work overload and underload, career development concerns, and work relationships. Popular musicians were found to have higher levels of anxiety than a normative sample, with gigging musicians, “the kind who work in clubs . . . and touring musical shows,” identified as the most stressed, demonstrating the poorest overall health and expressing the least satisfaction in their work (Wills, 2001, p. 27).
Over the past decade, diminished earnings from recorded music have forced many musicians to rely more on live performance and touring to offset these losses. Musicians today generate 75% of their income from live events and tours, compared with less than a third in the 1990s (Lunny, 2019). Streaming royalties now account for less than 2% of music-related income (Krueger & Zhen, 2018). Unfortunately, a greater emphasis on touring exposes musicians to the environmental factors (Wills and Cooper, 1988) found to be associated with the highest levels of occupational stress. The impact is apparent in a national survey of Australian entertainment industry professionals: 57% of musicians surveyed reported working evenings and nights, 67% worked weekends, 61% endorsed unpredictable work hours, and 65% reported disrupted sleep patterns (van den Eynde et al., 2016). Over half strongly endorsed problems finding time for their families and experiencing difficulties maintaining their social life.
Several complementary theories of occupational stress have been utilized to explain the association between musician work stress and mental ill-health. According to the job–demand–control (JDC) model, symptoms of fatigue, anxiety, depression, and physical illness are associated with high physical and psychological job demands and the worker lacks the autonomy or resources to deal with those demands (Karasek, 1979). This model has been expanded to include workplace social support as a potential moderator between occupational demands and stress-related outcomes (Johnson & Hall, 1988; Karasek & Theorell, 1990). Alternately, the effort–reward imbalance (ERI) model proposes that psychological distress occurs when an individual invests high effort in their work, but expectations of financial reward, career advancement, and/or recognition are not realized (Siegrist, 1996). A meta-analysis in the occupational health literature has shown robust evidence of the combination of high job strain and ERI to be prospective risk factors for common mental disorders (Stansfeld & Candy, 2006). More recently, Willis and her colleagues (2019) conducted a mixed-methods systematic review of the literature studying the relationship between occupational demands and wellbeing in performing artists. A total of 20 studies met the criteria for review, 17 of which were conducted with musicians. The researchers found the JDC model to be appropriate for exploring the effects of organizational demands, autonomy, and support systems on musician wellbeing, while the ERI model highlighted effects of low remuneration, job insecurity, and lack of career progression on musician health. However, 13 of the 17 studies investigating musician occupational stress included only classical musicians, which limits the generalizability of findings to popular musicians. For example, classical musicians and large orchestral performers report less control over their work than performers of other musical genres, while musicians who perform contemporary forms of music endorse higher levels of job demands and work–family conflicts (Détári et al., 2020). Of the studies including nonclassical musicians, three did not reference an occupational stress model (Bodner, 2008; Dobson, 2010; Kubacki, 2008) and the fourth (Cooper & Wills, 1989) drew upon an unrelated stress framework (Selye, 1946).
A third occupational stress framework that has been applied to the study musician mental health is the job demands–resources (JDR) model (Bakker & Demerouti, 2007). According to this model, the occupational environment encompasses both job demands and job resources. Job demands are defined as the physical, social, or organizational work responsibilities that require sustained effort and are associated with strain. Job resources refer to organizational or personal variables that promote work engagement and buffer the effect of job demands. Examples of job resources include social support, resilience, self-efficacy, autonomy, and perceived control. This framework was used in a recent large study of 1,600 Norwegian musicians to examine the associations of work-related demands, work-related resources, and personal resources with psychological distress (Aalberg et al., 2019). Consistent with the JDR model, the personal resource constructs of neuroticism and low sense of mastery were associated with distress. However, all predicted work context concepts, including job demands, effort–reward, job control, social support, and work–family conflict, had either weak or no relationship with psychological distress. The authors hypothesized that the JDC-S and ERI explanatory models may be too narrowly applicable to traditional forms of work and imprecisely reflect the unique work demands of the freelance musician.
Another explanation for these surprising findings could be the presence of a confounding variable associated with both musician occupational stress and psychological distress. Stress associated with financial hardship, for example, is frequently endorsed by popular musicians working as freelance artists (Record Union, 2019; Vaag et al., 2014). Financial hardship refers to the nature and extent of deprivation a person is experiencing due to a lack of financial resources relative to basic needs, including affordable housing, paying bills, transportation, health care, and purchasing food and clothes (Frankham et al., 2020). Financial hardship has been associated with depression (Mirowsky & Ross, 1999), with the risk of depression statistically stronger for financial hardship than other measures of income, occupation, or education (Butterworth et al., 2012; Lahelma et al., 2006). Significant economic downturns also have been associated with increased suicide rates (Reeves et al., 2014). According to a national survey of over 1,200 US musicians, the median musician salary between 2012 and 2016 was only US$20,000–US$25,000. In all, 61% of musicians in this survey reported that their music-related income was not sufficient to meet their living expenses (Krueger & Zhen, 2018). In Austin, Texas, the self-proclaimed Live Music Capital of the World, three-quarters of musicians make less than the mean annual wage for the Austin metropolitan area and 20% live below the federal poverty line (Titan Music Group, 2015). In a survey of 1,400 independent musicians, almost three-quarters (73%) reported that they had experienced significant stress, anxiety, and depression in the context of their musical endeavors. The two most common attributions for these negative emotional experiences were fear of failure and financial instability (Record Union, 2019).
Occupational and financial stress may also help explain the high prevalence of alcohol misuse among popular musicians. In one Australian study, for example, 62% of surveyed musicians endorsed harmful drinking behaviors (Parker, 2015). In the aforementioned Record Union (2019) study, over half (54%) of the surveyed musicians admitted that they self-medicated with alcohol to cope with music industry-related stressors.
A review of the existing musician occupational stress research reveals a gap in the understanding of the relative associations of occupational and financial stresses with mental health burden in popular musicians. In this study, we hypothesized that musician occupational and financial stress would each be associated with clinically significant levels of depression, anxiety, and alcohol misuse.
Materials and methods
Sample
This was a cross-sectional survey study of mainly low-income popular musicians who had received treatment for mental health concerns. An online survey was emailed between March and April 2015 to 655 musicians who had accessed mental health services within the previous 2 years through the SIMS Foundation, a nonprofit organization that annually provides counseling, psychiatric medication management, and addiction recovery services to over 600 musicians, music industry professionals, and their families in Austin, Texas (Berg & Garcia-Pittman, 2014). The community in question resides in a non-Medicaid expansion state with a large number of uninsured individuals in the lowest income quartile. There is a safety net medical insurance service run by the county to cover low-income individuals on a sliding-scale basis. However, there is almost no low-cost, affordable mental healthcare treatment outside of crisis response systems.
Before the survey was distributed, eligible subjects were notified by the SIMS Foundation via text message to expect a telephone call regarding a SIMS-sponsored research study on musician mental health. Investigators then contacted subjects, following a script in explaining the purpose of the study and the voluntary nature of participation. An email with an embedded link to the online survey was sent to all who agreed to participate. Two reminder emails were sent within a 2-week span to those who had not yet responded. SIMS clinical providers also distributed written information about the study to musicians receiving services from SIMS mental health providers. All participants who fully completed the survey were entered into a lottery to win 1 of 10 US$25 gift certificates from a local music retailer. Consent was obtained by participants checking a box acknowledging that they had read the informed consent statement and agreed to participate in the study before proceeding to the survey. Screening questions confirmed that all subjects were still active working musicians. The study and recruitment materials used were reviewed and approved by the Seton Healthcare Family Institutional Review Board in Austin, TX (CR-14-197).
Measures
A 101-item survey was designed, beginning with two items confirming subject eligibility and followed by validated measures of the key constructs of musician-specific occupational stress, financial stress, depression, anxiety, and alcohol misuse. The self-administered, online survey was designed to take approximately 15 min to complete and also included quantitatively assessed items regarding social and economic circumstances, the type of musical work in which the subjects participate (e.g., instruments played, touring frequency), mental health treatment history, and basic demographics.
Musician occupational stress was measured with the Musician Occupational Stress Scale (MOSS), a 54-item, quantitative instrument adapted from the Musician Sources of Pressure Instrument, originally developed with popular musicians in England by Wills and Cooper (1988) and revised for American terminology (King et al., 2019). Responses were scored on a 5-point Likert-type scale, ranging from 1—no pressure at all to 5—a great deal of pressure, plus a not applicable response option. A factor analysis of the original instrument revealed 11 factors: Performance Anxiety, Work Over/Underload Related to Traveling, Performance-Related Anxiety, Instruments and Equipment, Career Development, Poor Physical Work Conditions. Effects on Social and Family Life, Playing Disliked Gigs, Things Going Wrong on the Gig, Conflicts within a Band, and General Relationships in the Working Situation. Pilot testing of the MOSS showed good internal consistency (α = .91), test–test reliability (r = .86), and construct validity (King et al., 2019).
Financial stress was measured with the Personal Financial Wellness Scale (PFW), an 8-item instrument designed to measure level of stress and wellbeing derived from one’s personal financial condition (Prawitz et al., 2006). Items are constructed of eight 10-point Likert-type scales (1 = overwhelming financial distress/lowest level of financial well-being, 10 = no financial distress/highest level of financial well-being), with a final score obtained by dividing the total score by the number of items. Internal consistency of the PFW is 0.956 and a factor analysis using principle components extraction confirms that the PFW measures a single factor that accounts for 78.9% of the variance. A cutoff score of four or less is associated with high financial stress; a score of two or less reflects extremely high financial stress.
Depression levels were assessed with the PHQ-9, a 9-item instrument commonly used in depression research (Kroenke & Spitzer, 2002). The PHQ-9 assesses severity of depression symptoms over a previous 2-week period with 4-point Likert-type scales ranging from not at all to nearly every day. Scores range from 0 to 27, with higher scores indicating greater depression level; a cutoff score of 10 is considered clinically significant. The PHQ-9 has excellent psychometric properties, with a cutoff score of 10 or greater associated with 88% sensitivity and specificity for detection of major depression.
Anxiety levels were measured with the GAD-7, consisting of seven 4-point Likert-type scales, with respondents indicating symptom frequency ranging from not at all to nearly every day during the prior 2 weeks (Spitzer et al., 2006). Scores range from 0 to 21, with higher scores denoting greater anxiety. The GAD-7 has been shown to have good reliability, as well as criterion, construct, factorial, and procedural validity. A cutoff score of 10 or greater identifies generalized anxiety disorder with a sensitivity of 89% and specificity of 82%.
Alcohol misuse was assessed with the AUDIT-C, a brief 3-item screen adapted from its 10-item parent scale (Bradley et al., 2007). The AUDIT-C has been found to perform as well as the full AUDIT and significantly better than self-reported risky drinking or augmented CAGE questions. Scores range from 0 to 12, with higher scores associated with misuse. Screening thresholds maximizing sensitivity and specificity were 4 or greater in men (86% sensitivity, 89% specificity) and 3 or greater in women (73% sensitivity, 91% specificity).
The PHQ-9, GAD-7, and AUDIT-C were all formatted as continuous (total score), by rank-order (i.e., ordinal) categories determined by standardized risk thresholds, and dichotomous measures (diagnostic thresholds or moderate–severe vs. low risk). The PFW scale was inverted so that higher scores corresponded with higher levels of financial stress.
Analysis
Key characteristics (demographics, income, background as a musician), the standardized measures incorporated, and the global questionnaire items related to stress and career satisfaction were summarized to characterize the sample. In order to examine the role of collinearity between the primary independent and dependent variables of interest, matrices of nonparametric Spearman correlations (ρ) and pairwise Spearman correlations were generated across all five measures. Finally, the relationships between occupational stress (MOSS) and financial stress (PFW) and each of the clinical symptom measures were tested using univariate and multivariate ordinal (PHQ-9, GAD-7) or logistic (AUDIT-C) regression models. Multivariate ordinal or logistic regression models included incorporation of both the MOSS and PFW measures (Model 1) in models of each clinical symptom measure, followed by adjustment for the other respective symptom scales (Model 2; e.g., ordinal GAD-7 levels in the model of PHQ-9). While the combinations of stress and symptom scales were not theorized to act as instrumental variables in Models 1 or 2, generalized Durbin–Wu–Hausman tests were used to assess endogeneity due to the potential collinearity among independent variables. Summary tables and all analyses were performed using STATA statistical software (v13.1; College Station, TX).
Results
The survey resulted in 317 musicians completing the questionnaire, with a response rate of 48.4%. The median age of respondents was 40–49 years. Approximately 64% were male, primarily Caucasian race (81%), and half were married (see Table 1 for details).
Musician Respondent Characteristics (n = 317).
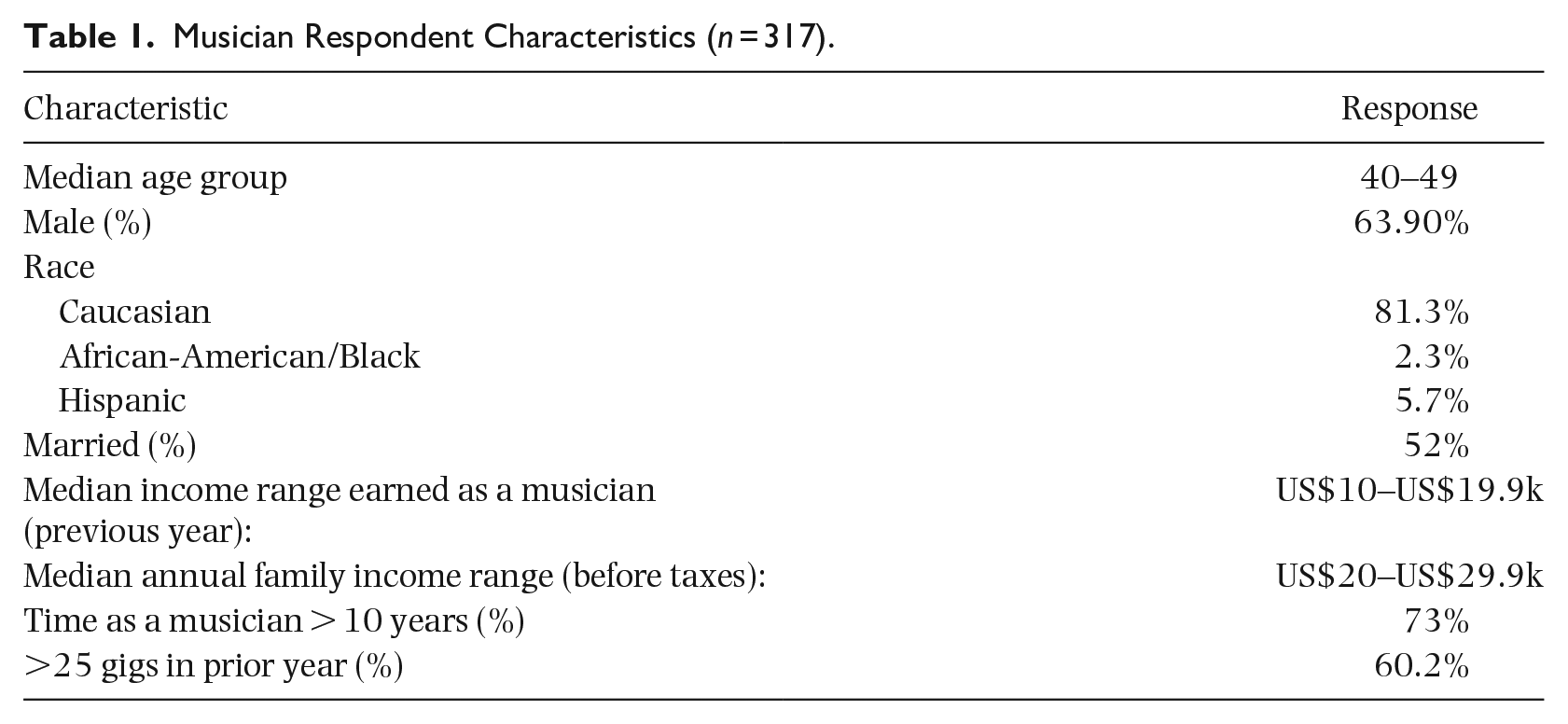
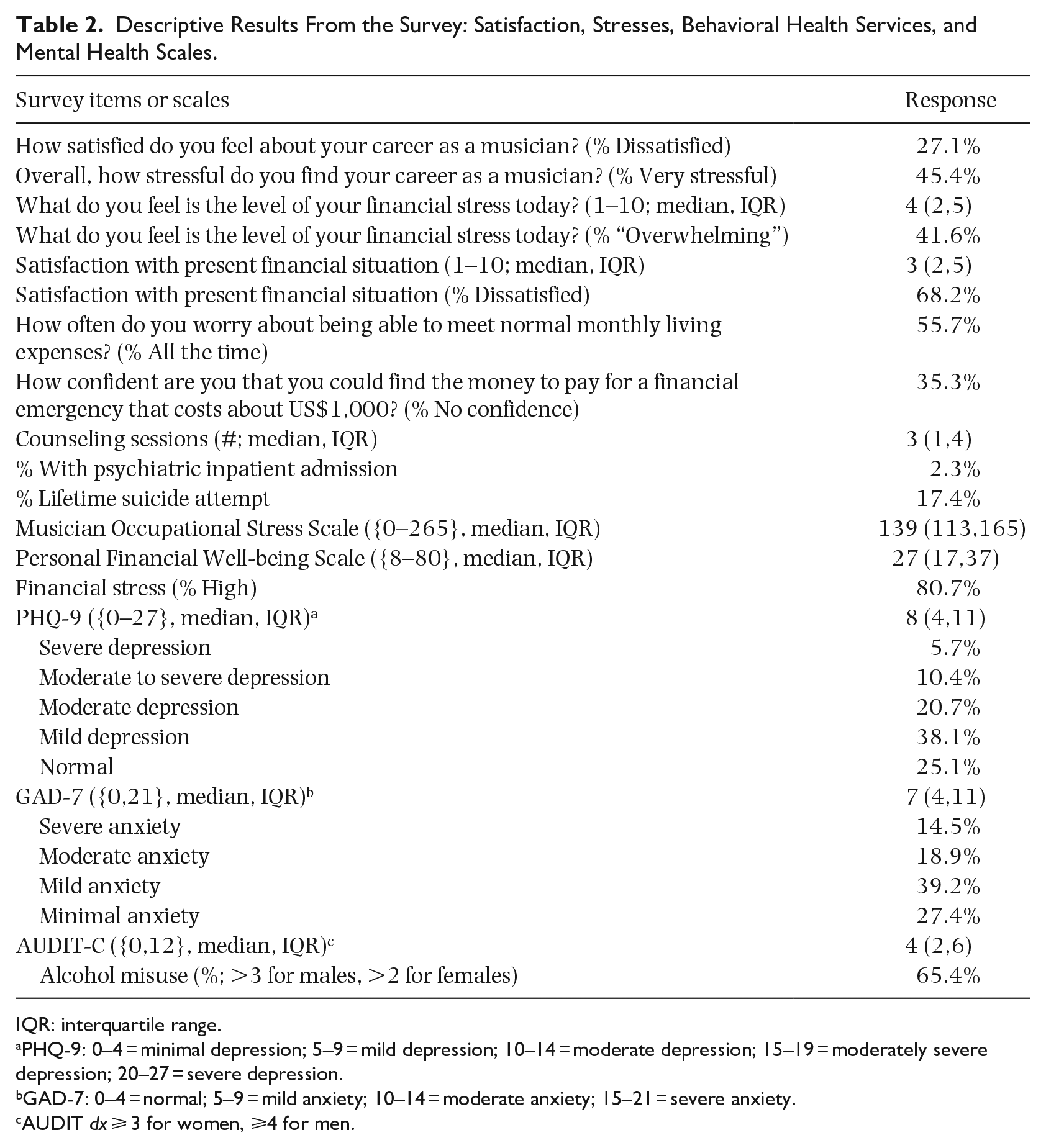
The subjects were notably low-income. While 73% of the sample had been working as a musician for greater than 10 years, the median category of prior-year income from work as a musician was just US$10,000 to <US$20,000 and the median category of total family income was US$20,000 to <US$30,000. Respondents worked a median number of two jobs in order to support their musical career. Almost half (45.4%) endorsed significant levels of occupational stress; 68% were dissatisfied with their financial status and 81% rated their financial stress as “high” or “overwhelming.” Over 36% reported at least moderate depression levels and over 33% expressed similar levels of anxiety; 17.4% reported a history of at least one lifetime suicide attempt. Almost two-thirds (65.4%) of respondents screened positive for alcohol misuse (see Table 2).
Descriptive Results From the Survey: Satisfaction, Stresses, Behavioral Health Services, and Mental Health Scales.
IQR: interquartile range.
PHQ-9: 0–4 = minimal depression; 5–9 = mild depression; 10–14 = moderate depression; 15–19 = moderately severe depression; 20–27 = severe depression.
GAD-7: 0–4 = normal; 5–9 = mild anxiety; 10–14 = moderate anxiety; 15–21 = severe anxiety.
AUDIT dx ⩾ 3 for women, ⩾4 for men.
Multicollinearity
As expected, there was a reasonably high correlation between total scores on the PHQ-9 and GAD-7 scores. The MOSS and PFW showed moderate levels of correlation with each other and with the PHQ-9 and GAD-7. However, those four measures showed weak correlation with the AUDIT-C (see Table 3 for Spearman correlation matrix and pairwise correlations).
Multicollinearity Between Total Scores on Mental Health and Stress Scales (n = 207).
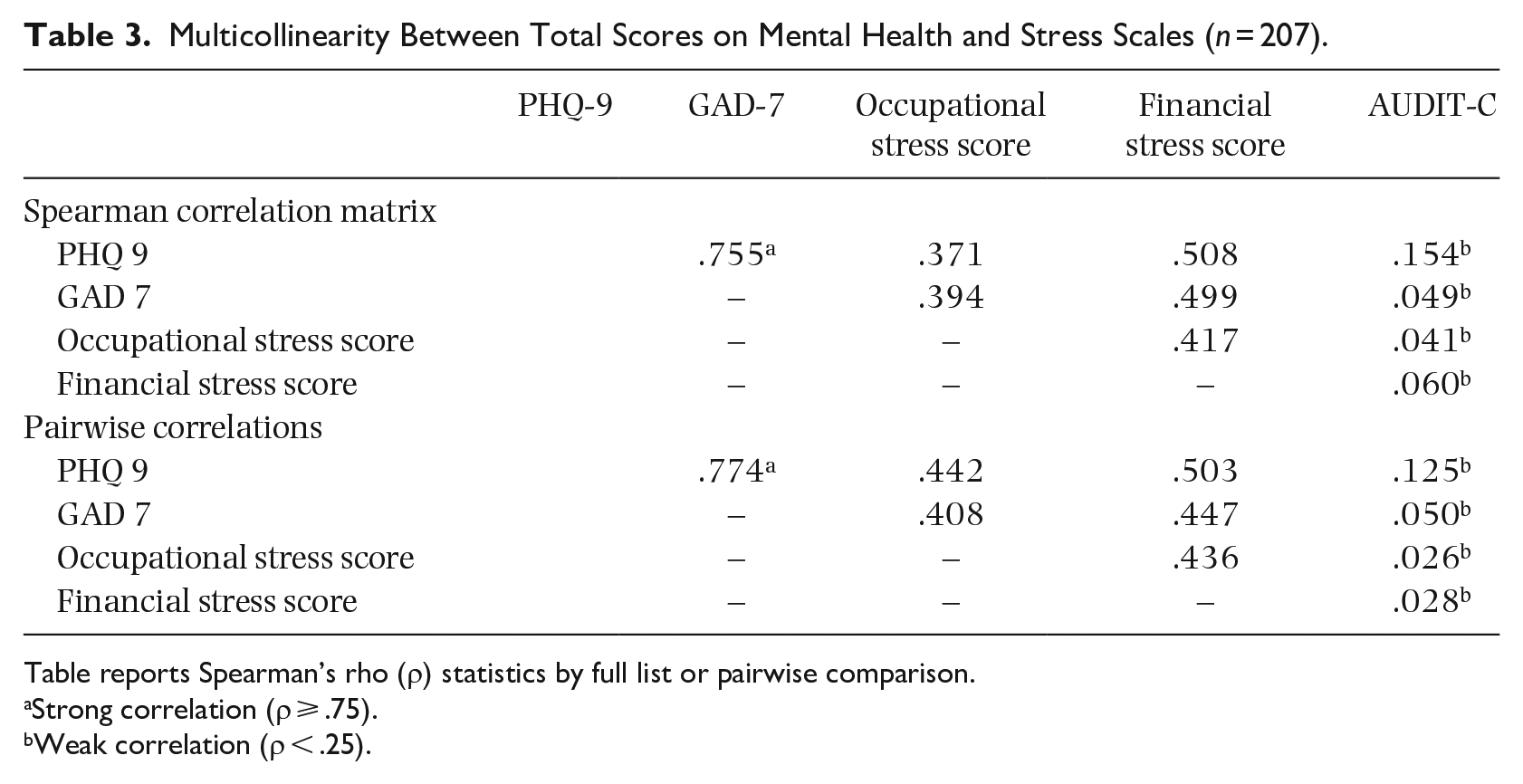
Table reports Spearman’s rho (ρ) statistics by full list or pairwise comparison.
Strong correlation (ρ ⩾ .75).
Weak correlation (ρ < .25).
Ordinal regression models
Univariate tests showed a strong association between the MOSS and the PHQ-9 (OR = 3.62; 95% confidence interval [CI] = [2.6, 5.0]) and GAD-7 (OR = 3.05; 95% CI = [2.2, 4.2]) as well as between the PFW and the PHQ-9 (OR = 1.90; 95% CI = [1.6, 2.2]) and GAD-7 (OR = 1.72; 95% CI = [1.5, 2.0]). Neither measure of stress was significantly associated with the AUDIT-C.
Multivariate analyses showed that the statistical association between the MOSS and ordinal level on the PHQ-9 and between the MOSS and ordinal level on the GAD-7 persisted when adjusted for by PFW (PHQ-9 aOR = 2.32; 95% CI = [1.6, 3.3]; GAD-7 aOR = 2.12; 95% CI = [1.5, 3.0]). The significant relationship of PFW with PHQ-9 and GAD-7 was similarly maintained when adjusted for by MOSS. Even when models of PHQ-9 or GAD-7 adjusted for GAD-7 and PHQ-9, respectively, associations with MOSS (PHQ-9 aOR = 2.00; 95% CI = [1.4, 2.8]; GAD-7 aOR = 1.80; 95% CI = [1.2, 2.6]) and PFW (PHQ-9 aOR = 1.49; 95% CI = [1.3, 1.8]; GAD-7 aOR = 1.32; 95% CI = [1.1, 1.6]) were maintained (see Table 4).
Multivariate Models of PHQ-9, GAD-7, and AUDIT-C Scores.
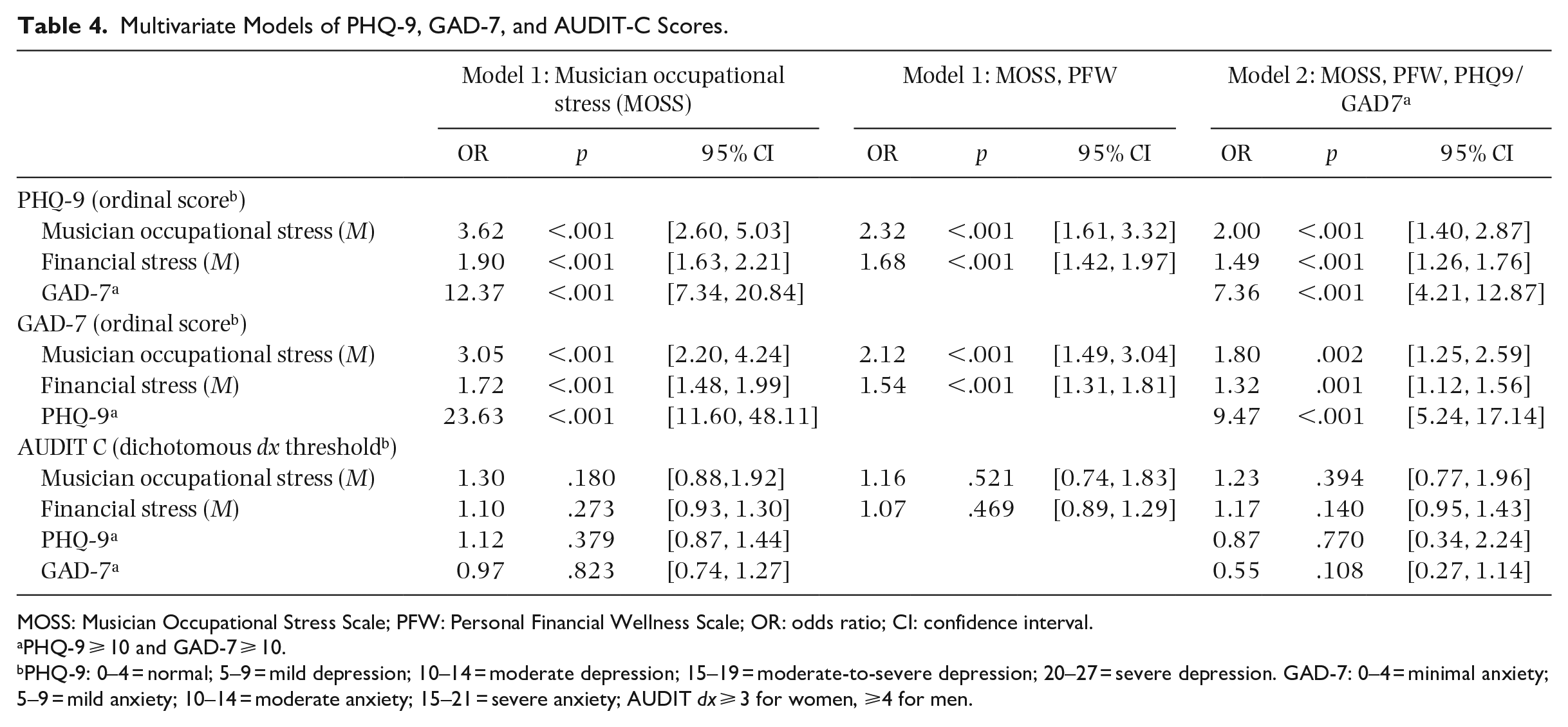
MOSS: Musician Occupational Stress Scale; PFW: Personal Financial Wellness Scale; OR: odds ratio; CI: confidence interval.
PHQ-9 ⩾ 10 and GAD-7 ⩾ 10.
PHQ-9: 0–4 = normal; 5–9 = mild depression; 10–14 = moderate depression; 15–19 = moderate-to-severe depression; 20–27 = severe depression. GAD-7: 0–4 = minimal anxiety; 5–9 = mild anxiety; 10–14 = moderate anxiety; 15–21 = severe anxiety; AUDIT dx ⩾ 3 for women, ⩾4 for men.
Endogeneity tests were consistently significant between the univariate and combined Model 1 (MOSS and PFW) of both PHQ-9 and GAD-7. In addition, endogeneity was confirmed by testing the differences between Models 1 and 2 (MOSS, PFW, and the corresponding mental health scale) of both PHQ-9 and GAD-7 (all ps < .001). This indicates that addition of each new independent variable created systematic differences in coefficients relative to the more parsimonious model.
In either univariate or adjusted models, meeting the diagnostic threshold level on the AUDIT-C (indicating alcohol misuse) was not associated with either occupational stress (aOR = 1.23; 95% CI = [0.8, 2.0]) or financial stress (aOR = 1.17; 95% CI = [0.9, 1.4]). Endogeneity tests between the univariate models and Model 1 and/or between Models 1 and 2 were also all nonsignificant.
Discussion
The findings of this study support the hypothesis that occupational stress and financial stress are each associated with clinically significant levels of depression and anxiety in popular musicians. Both stressors were associated with depression and anxiety, even when controlling for each other and the severity of these closely related mental health conditions. While a strong majority of participants (72%) reported satisfaction with their musical career, almost half (45%) reported significant levels of work-related stress. The relationship between musician occupational stress and mental health burden was robust. Musicians reporting higher levels of occupational stress were over three times more likely to report depression and/or anxiety than their less-stressed counterparts. They were still more than twice as likely to be emotionally distressed when the variance attributed to financial stress was controlled.
These predicted findings contradict the results of a recent Norwegian study of musician occupational stress that found weak or insignificant relationships between measures of job demand, effort–reward, job control, social support and work–family conflict, and predicted psychological distress (Aalberg et al., 2019). One explanation is that the current study utilized a validated psychometric measure with items specific to the occupational stresses of popular musicians, an approach recommended by Jacukowicz and Wezyk (2018), as opposed to assessing occupational stress typical of most occupations, which was utilized by the above-mentioned Norwegian study.
Over three-quarters of the musicians in this study rated their financial stress as high or overwhelming, which was also associated with higher levels of self-reported depression and anxiety. Financial hardship has been identified in a number of musician surveys as a significant stressor adversely affecting mental health (see Krueger & Zhen, 2018; Record Union, 2019). This variable, however, has received less systematic attention in the musician mental health research literature compared with other occupational stressors. Suicide researcher Steven Stack (2009) has noted that creative artists, including musicians, represent one of the few occupational groups associated with increased suicide risk independent of demographic confounders. He cites financial stress due to labor market strains, including unemployment, underemployment, client dependency (i.e., self-employment), multiple job holding, and low incomes, as a significant suicide risk factor in this group.
The importance of considering the effects of financial hardship on popular musician mental health has been amplified by the deleterious economic impact of the COVID-19 pandemic on the live music industry. Music venues were among the first to close during the pandemic and many have yet to fully reopen, resulting in severe economic hardship for touring musicians. A recent study of performing arts professionals, including a majority in the music industry, revealed a substantial decrease in work and income during the pandemic, with 53% reporting financial hardship and 85% endorsing increased anxiety. Perceived financial hardship was associated with lower wellbeing and higher depression scores (Spiro et al., 2020).
Contrary to expectations, musician alcohol misuse was not associated with either occupational stress or financial stress in this study. It is conceivable that these variables are unrelated. Other factors implicated in elevated rates of musician alcohol and substance misuse include sensation-seeking traits and the role of alcohol in musicians socializing professionally (Dobson, 2011; Miller & Quigley, 2012). Another explanation is that the relationship between musician occupational stress and alcohol misuse is nuanced. One study, for example, found high career insecurity in musicians, paired with “poor quality” (i.e., externalized or contingency-based) forms of work motivation correlated with elevated AUDIT scores (Parker et al., 2021).
Limitations of this study include its cross-sectional design, which limits the causal inference of the relationship between work and financial stress and musician mental health burden. The survey response rate of almost 50% was good, but the results remain susceptible to nonresponse bias. Another limitation is that all the study participants had received mental health services within the previous 2 years. It is possible that help-seeking musicians may be more willing to report work and financial stress. These participants may also have been predisposed to mental health problems and therefore more susceptible to work or financial stress. The mental health burden reported by musicians in this survey was high; over a third endorsed moderate to severe levels of anxiety and depression and nearly one in five reported a lifetime suicide attempt history. Similar findings, however, were reported in a national survey of Australian entertainment workers, in which 54.1%, 24.4%, and 7.5% of musicians reported moderate to severe levels of depression, anxiety, and lifetime suicide attempt history, respectively (van den Eynde et al., 2016). Over half (59.6%) the entertainers surveyed had sought out mental treatment. Nonetheless, future studies should include musicians who have not sought out mental health services to increase the generalizability of findings and investigate possible differences in psychological distress in musicians who do or do not seek out mental health services. A strength of this study was the use of validated measures of all the key constructs.
It is important to note that the endogeneity identified in multivariate models and the correlation between occupational and financial stresses suggest the potential for influence from one or more additional, unmeasured constructs involved in the relationships between these identified stressors and heightened psychological distress in popular musicians. Further research is indicated to identify possible instrumental variables. Future studies should continue to investigate which theory-driven musician occupational stress factors are most strongly associated with mental health burden and ideally engage larger samples longitudinally.
Conclusion
To our knowledge, this is the first study to identify occupational and financial stress as separately associated with depression and anxiety in popular musicians. Better understanding the relative impact of these social determinants of mental health should be helpful in designing targeted, evidence-based treatment interventions for musicians and decreasing morbidity and mortality in this high-risk population. Clarifying these associations could also lead to the development of psychometrically valid screening instruments to identify at-risk musicians and promote effective prevention strategies. Despite higher rates of mental health problems compared with the general population, musicians also have been shown to be open to seeking mental health treatment and responsive to mental health interventions (Berg et al., 2018; Visser et al., 2021). Dissemination of these findings may also help dispel societal stereotypes of musicians as “tortured artists” who intentionally embrace emotional suffering in the service of their art and provide a better understanding of the conditions that make them psychologically vulnerable.
Footnotes
Acknowledgements
The authors thank Heather Alden, Brad Pierson, LCSW, J. Jade Adair, LCSW, and Carlos Tirado, MD, MPH for their contributions and Rock n Roll Rentals for their financial support.
Author’s Note
Ben King is now affilitation to Department of Neurology, Dell Medical School, The University of Texas at Austin, Austin, TX, USA.
Jessica Koenig, MD has a new affiliation with Santa Rosa Community Health Center, Santa Rosa, CA, USA.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.