
Abstract
Music preferences are molded with numerous personality variables, yet, this relation, as assumed in the study, may be mediated by functions of music expressing the psychological needs of the listener. Not many studies are devoted to the music preferences of listeners with personality disorders, whereas, none investigate this topic among people with Borderline Personality Disorder (BPD). A correlational study that was conducted among 549 individuals (274 displayed BPD symptoms). The main goal was to examine the extent to which the severity of BPD symptoms directly interacts with the following: (a) music preferences and (b) music function formation, and whether the functions of music can explain the mechanism through which BPD symptoms interact with music preference formation. Using structural equation modeling (SEM), we demonstrated that the severity of BPD-spectrum symptoms is closely related to types of music preferred. In addition, BPD symptoms severity is substantially linked to the perception of the social relatedness and self-awareness functions of music, whereas emotional function seems to be independent of the BPD symptoms aggravation. Finally, the functions of music can partly act as a mediator in shaping the mechanism of forming music preferences based on personality predispositions. Further music preference analyses among individuals with BPD is highly warranted.
Keywords
The omnipresence of music in human life inspires one to ask questions about its psychological functions (for an overview see Schäfer, Sedlmeier, et al., 2013). People use music to accomplish certain goals and satisfy individual needs (Getz et al., 2012; Kuntsche et al., 2016; Laukka, 2007; North, 2010; Randall et al., 2014; Randall & Rickard, 2016; Vella & Mills, 2017). Music is the source or tool of various psychological experiences: social (Dingle et al., 2013), emotional (Saarikallio, 2011), but also those related to self-awareness (Lawendowski & Besta, 2020), or health (Gustavson et al., 2021).
The literature highlights the issue of music choices among individuals with a range of mental health problems (cf. Doak, 2003; Miranda & Claes, 2008; Miranda et al., 2012). Studies have shown that teenagers experiencing mental health problems are more likely to listen to particular types of music, like hard rock, heavy metal, or rap. However, it bears mentioning here that this relationship has a complex character, such that latent mental health problems are more likely revealed by music preferences rather than shaped by music (cf. Baker & Bor, 2008). Listening to music could be thus considered a form of self-therapy, in that doing so aids in coping with mental health problems (Kanagala et al., 2021).
It has been demonstrated that current well-being and long-term mental condition determine the ways in which people enjoy music (Skånland, 2013). Individuals characterized by negative affect or depressed individuals tend to listen to music for the purpose of mood regulation (Thomson et al., 2014). Nevertheless, until now, few studies have been devoted to the issue of mental health and uses of music (cf. Kanagala et al., 2021) and none have discussed this topic in relation to the specific functioning of individuals with Borderline Personality Disorder (BPD).
Borderline Personality Disorders (BPD)
Personality disorders are defined as fixed deep-seated patterns of behavior, perception, reasoning, and emotion experience which diverge from the typical functioning of an individual in a given culture and society (American Psychiatric Association [APA], 2013). An example of such a disorder is BPD, determined as a heterogeneous mental state defined by a pervasive pattern of unstable interpersonal relations, identity, affects, and also pronounced impulsivity (APA, 2013).
Abnormal interpersonal relationship patterns are indicative of BPD psychopathology and the relational style of individuals with BPD can be determined as unstable, ambivalent, and intense. BPD is characterized by a strong fear of abandonment, accompanied by simultaneous efforts to avoid it (APA, 2013). A perpetual state of alertness and readiness to look for situations marked by potential threat of rejection is often imaginary, and thus leads to cognitive and emotional changes that also influence the patient’s interpretation of themselves and others (Cierpiałkowska & Soroko, 2017).
Emotional dysregulation and impulsivity are further traits considered as basic symptoms of this disorder (Fossati et al., 2014). Difficulties in appropriately regulating emotions are simultaneously reflected in several areas, namely, at the emotional, but also cognitive, behavioral, biological, and interpersonal levels (Farrell & Shaw, 1994; Pastuszak, 2012). Emotional dysregulation of individuals with BPD manifests itself primarily through emotional instability and poor level of awareness of experiencing emotions (Cole et al., 2009), accompanied by exaggerated, frequently incomprehensible reactions to circumstances and a feeling of being overtaken by their own emotions (Cole & Hall, 2008; Tragesser et al., 2007). In contrast, the inability to recognize their own inner states, and consequently, inability to assess their own reactions whereas acting, inhibits their self-regulation (Farrell & Shaw, 1994).
Another characteristic criterion of BPD is identity disorders that are characterized by lack of coherence/distinctiveness and sense of continuity over time. Accordingly, identity disorders manifest themselves through instability as to one’s own choices, difficulty in recognizing one’s own attributes and feelings and a tendency to confuse them with the desires of another person with whom they have a close relationship (cf. Erikson, 1968). Typically people with BPD experience anxiety about the disintegration of “the self,” which is associated with, for instance, a difficulty in recognizing who they are, a sense that the “self” presented to the world differs from their inner experiences, an impression of being unreal, and a fear of losing their own identity when a close relationship is established or breaks down (Westen & Cohen, 1993; Wilkinson-Ryan & Westen, 2000).
Due to inconsistencies in the concept of the “self,” the displayed behavior is perceived as unpredictable, ambiguous, and unclear. It is reflected in lack of stable goals in life, assumed social roles, views, and, owing to inability to plan for the future, living in the present (Andrałojć & Suchańska, 2013). This causes negative consequences, including social dysfunction, problems with self-awareness and psychological identity, and emptiness (Price et al., 2022). The severity and broad spectrum of BPD symptoms make the issue a significant one, and further studies are still required.
Personality-based determinants of music preferences
The literature identifies several personality-based determinants of music preferences (e.g. Bansal et al., 2021; Bonneville-Roussy et al., 2013; Clark & Lonsdale, 2023; Dunn et al., 2012; Greenberg et al., 2022; Herrera et al., 2018; Rentfrow et al., 2011; Rentfrow & McDonald, 2010; Santos et al., 2023; Schäfer & Mehlhorn, 2017; Schäfer & Sedlmeier, 2009; Soares-Quadros et al., 2019). Studies have so far focused on variables such as introversion and extraversion (Crawford & Strapp, 1994; Daoussis & McKelvie, 1986; Dollinger, 1993; Furnham & Bradley, 1997; Furnham et al., 1999; Furnham & Strbac, 2002; Payne, 1980; Pearson & Dollinger, 2004; Rawlings & Ciancarelli, 1997) and sensation seeking (Daoussis & McKelvie, 1986; Dollinger, 1993; Gowensmith & Bloom, 1997; Litle & Zuckerman, 1986; McNamara & Ballard, 1999). The available research shows a clear association between music preferences and Big Five factors: (a) openness to experiences (Cleridou & Furnham, 2014; Dollinger, 1993; Rawlings & Ciancarelli, 1997; Rawlings et al., 2000; Vella & Mills, 2017; Zweigenhaft, 2008); (b) agreeableness (Delsing et al., 2008; Greenberg et al., 2022); (c) conscientiousness (Delsing et al., 2008; Langmeyer et al., 2012; Rentfrow & Gosling, 2003); (d) neuroticism (Chamorro-Premuzic & Furnham, 2007; Payne, 1967; Weaver, 1991); and (e) psychoticism (Bleich et al., 1991; Dillman Carpentier et al., 2003; McCown et al., 1997; Rawlings et al., 1995; Robinson et al., 1996; Weaver, 1991).
Some researchers, inspired by Cattell and Anderson (1953), have attempted to infer personality traits based on an individual’s music preferences by taking into account the differences in music preferences in relation to apparent population trends. Hahn (1954) indicated that music preferences may accurately reflect information collected in the course of a clinical personality diagnosis. Janicki and Natanson (1974), in turn, undertook studies on the perception of music by individuals suffering from schizophrenia, whereas Galińska (1975) focused on neurotic patients. Bokcharev et al. (1995) concluded that anxious people are more sensitive to negative emotions conveyed through music, whereas Garrido and Schubert (2013, 2015) stated that patients who have greater tendencies to rumination do not gain the same benefits from listening to music as those who display a more reflective personality type.
In addition to the ways in which music is perceived and used, a few studies have explored differences in music preferences in relation to health and the type of disorder exhibited (e.g. Baker & Bor, 2008; Gebhardt & von Georgi, 2015; Kanagala et al., 2021; North & Hargreaves, 2007). At this point, no direct relation between the type of music preferred and one’s health has been proposed (Miranda et al., 2012), but there may be some mediating variables that shape this relationship.
This topic arouses particular interest among music therapists, who, against the background of music-related activity, focus on the psychological functioning of listeners with mental disorders (cf. Foubert et al., 2017; Kenner et al., 2020; McDonald et al., 2012). Specific patterns of psychological reactions that are rooted in personality, may, therefore, determine the perception and use of music (cf. Lamont & Hargreaves, 2021; Pałosz, 2009).
Functions of music in human life
People listen to music in various situations and for different purposes. This makes the answers to questions of why we like music extremely complex (Chmiel & Schubert, 2019). Sloboda (2005), when explaining the concept of the functions of music, emphasized that it refers to the role that people attribute to music in their lives. In fact, for many people, music is a means to achieve their goals and pursue individual intentions (Sloboda et al., 2001). Music functions include the use of music in everyday life to support various psychological needs and processes (e.g. Boer & Fischer, 2012).
Psychological processes that are linked to the functions attributed to music include the following: (a) regulation of physiological arousal (Krause & North, 2017; North & Hargreaves, 1997); (b) emotional self-regulation (Saarikallio & Erkkilä, 2007; van Goethem & Sloboda, 2011; van den Tol & Edwards, 2015); (c) regulation of the self-system (DeNora, 1999; Elvers, 2016; Elvers et al., 2018; Morgan et al., 2015); (d) building the identity of an individual—both in the sense of individual identity, as well as in relationships with others (Creech et al., 2013; DeNora, 1999; Hargreaves & North, 1999; Lawendowski & Besta, 2020; North & Hargreaves, 1999); (e) support for memory, especially autobiographical memory (DeNora, 1999; Schäfer, Fachner & Smukalla, 2013); (f) building and maintaining relationships with others (Croom, 2015; Dingle et al., 2013; Lonsdale & North, 2011); (g) building social and cultural values (Boer et al., 2012; Boer & Fischer, 2012; DeNora, 1999); and (h) promoting co-operation and group cohesion (Boer & Abubakar, 2014; Koelsch, 2013; Lawendowski & Besta, 2020).
Schäfer, Sedlmeier, et al. (2013) identified over 500 potential functions of music, which they reduced to the following three factors: social relatedness, self-awareness, and arousal and mood regulation. Overall, it can be said that music is a kind of activity that helps individuals to explore their identity, eliminate anxiety and regulate mood, or build relationships with others (cf. Hargreaves & North, 1999; Koelsch, 2013; North & Hargreaves, 1999; Saarikallio & Erkkilä, 2007).
The relationships between music preferences and functions of music have been studied in recent literature. For instance, Schäfer and colleagues demonstrated that particular types of music (rock, pop, and classical music) were preferred by listeners because of the specific functions held by that music (Schäfer & Sedlmeier, 2009). Moreover, studies imply a link between the intensity of preference for a particular type of music and the various functions it serves (Schäfer, 2016; Schäfer & Sedlmeier, 2009, 2010).
Models have been developed of the relationship between the uses of music, personality traits, and music preferences (Vella & Mills, 2017). However, it is not the functions of music that are considered a mediating factor in forming music preferences, but the particular characteristics of the listener (e.g. Vella & Mills, 2017). To the best of the authors’ knowledge, nothing is known about the music preferences of individuals with BPD and whether and how psychological functions of music are related to their formation.
The present study
Individual differences in music preferences are still one of the most mysterious phenomena in psychology (Schäfer, 2016). As already mentioned, despite the fact that numerous variables regarding music style/genre which might form music preferences have already been recognized, knowledge on this topic is far from comprehensive (Kanagala et al., 2021) and this study is an attempt to further develop this.
The literature has suggested that favorite pieces of music are chosen because of their specific purpose and effect. Lately, it has been noted that the functions of music and the ways that music is used constitute crucial variables for understanding the characteristics of music preferences (Schäfer & Sedlmeier, 2009, 2010). Functionality, herein, refers to the conscious use of music to achieve certain goals in specific situations (Sloboda et al., 2001), such as evoking positive emotions, strengthening social relations, or coping with physiological arousal (Schäfer, Sedlmeier, et al., 2013). Due to the variety of the results obtained so far regarding the purpose of turning to music, further in-depth research on the nature of the functions of music in the context of music preferences formation is suggested.
The topic of this study is the characterization of music preferences and the functions of music within the group of individuals without/with risk of BPD. This type of personality disorder (a) has degrees of severity and (b) is characterized by a distinct specificity of functioning within the spheres of self-awareness, social relatedness, and arousal and mood regulation (Fossati et al., 2014; Goldstein, 2002; Gunderson et al., 1995; Kernberg, 1967; Siever & Davis, 1991; Wilkinson-Ryan & Westen, 2000). Based on the knowledge that (a) music preferences may be formed by the specific nature of personality-related functioning (Schäfer & Sedlmeier, 2009) and (b) that music through its psychological functions is related to self-awareness, emotional processes, and functioning of an individual in society (Schäfer, Sedlmeier, et al., 2013), an effort has been made to verify the characteristics of music preferences of individuals without/with risk of BPD. The research also addresses questions of exploring the link between personality and music preferences and treating functions of music as a mediator of the relations described.
The search for mediators is a significant element of the present research as it allows for a description of the boundaries within which the analyzed regularities occur. A typical situation in which mediators are pursued is when weak and/or unreliable correlations arise (Hayes, 2017), or, as in the case of the presented problem, poorly understood dependence.
Owing to the exploratory nature of studies, the following hypotheses have been put forward: H1: the severity of BPD symptoms directly affects music preferences; H2: the severity of BPD symptoms directly affects the formation of music functions; H3: music functions may clarify (in fully or in part) the mechanism of the influence of BPD symptoms on the formation of music preferences (the mediatory role of music functions).
Method
Sample
We included N = 549 responses for the analysis, with n = 275 (50.1%) individuals with a low score (below 10 points) in the abbreviated version of BPD and n = 274 (49.9%) individuals with a high score (more than 10 points). The bipolar categorization of participants (individuals with low or high severity of BPD symptoms) was based on the empirical median BPD measure score in the study sample (cf. Howell, 2010). We used the Polish version of all measures as all participants were Polish-speaking. The study sample was mostly composed of females (n = 415; 75.6%), with males constituting around a quarter of the study sample size (n = 134; 24.4%). The majority of the participants had undergone or were currently undergoing secondary or higher education (n = 512; 92.3%). Most disclosed they had a romantic relationship (partner, fiancé, or spouse; n = 333; 60.7%; Table 1).
Characteristics of the Study Participants.
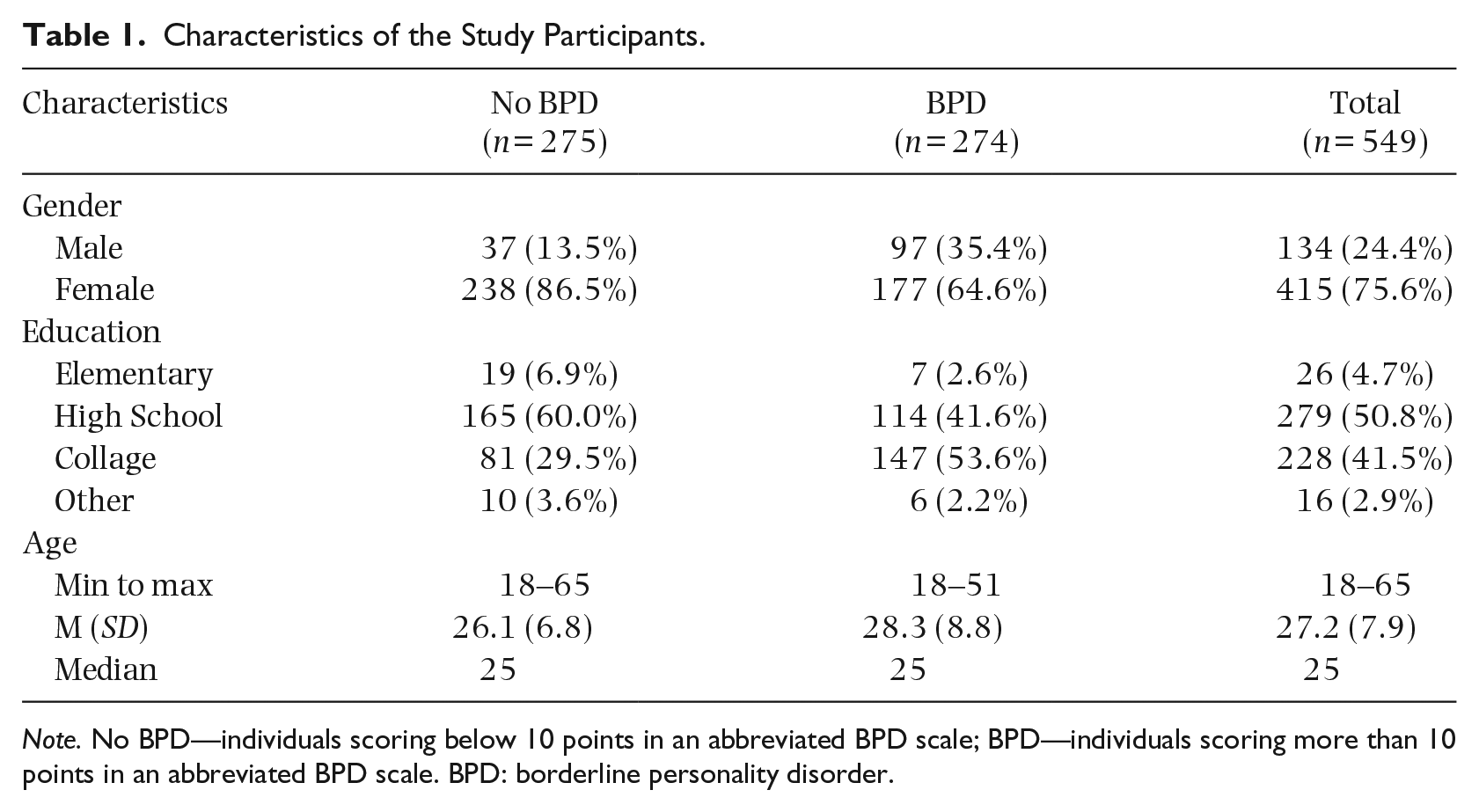
Note. No BPD—individuals scoring below 10 points in an abbreviated BPD scale; BPD—individuals scoring more than 10 points in an abbreviated BPD scale. BPD: borderline personality disorder.
A comparative analysis of groups with and without BPD symptoms revealed that individuals with BPD were slightly older (t(547) = –3.275, p < .001, g = –.28, CI95 = [–.45, –.11]), with the age difference between groups ranging from 0.9 to 3.5 years with 95% population probability. At the same time, the risk of being diagnosed with BPD symptoms was approximately 3.5 times higher among men (OR = 3.52, CI95 = [2.30, 5.40]), which is a statistically significant relationship between gender and BPD syndrome (χ2(1) = 36.841, p < .001, Cramer V = .26). Similarly, the education level is significantly associated with the presence of BPD symptoms (χ2(3) = 35.520, p < .001, Cramer V = .25). Thus, it can be said that gender and age, as well as the level of education might be factors that differentiate between people with BPD and those without such symptoms.
Instruments
Borderline personality
The Borderline Personality Inventory is a tool invented by Leichsenring (1999) and adapted to Polish by Cierpiałkowska (2001). It is a short screening tool (53 questions), of the true–false type, intended for the self-assessment of an examined person. According to the author’s recommendations, the test is applicable for diagnosing BPD, for deriving BPD type and for dimensional testing of BPD traits. The Borderline Personality Inventory is based on the organization of borderline personality according to the concept of Kernberg (1967), although the diagnostic criteria are consistent both with the concept of Gunderson’s BPD (Gunderson & Kolb, 1978), and with the DSM V (APA, 2013).
The questionnaire contains four subscales to assess: diffused sense of identity, primary defense mechanisms, impaired reality testing, and fusion anxiety. Sample items are the following: “When my relationship with someone gets closer I feel trapped,” “Sometimes someone who is not me appears inside me,” where the respondent specifies whether a particular statement refers to them or not (yes or no answer). The survey used a shortened scale of the tool (cut-off 10), in which the criterion for diagnosing BPD was established following the authors of the tool at a minimum of 10 points. The results indicate satisfactory reliability (Cronbach’s α = .68–.91).
Music preferences
The Short Test of Music Preferences was developed by Rentfrow and Gosling (2003) and adapted to Polish by Lawendowski (2011). STOMP contains 14 categories corresponding to theoretically described music genres. Each participant responds to each of the listed categories/genres on a 7-point Likert scale, from 1 = strongly dislike to 7 = definitely like. The average of all responses on a given scale denotes the strength of preference for a particular music factor. The first factor, that is, Reflective and Complex (RC), comprises the genres of blues, classical music, jazz, and folk music. Within the Intense and Rebellious (IR) three genres are distinguished: heavy metal, rock, and indie. The Upbeat and Conventional factor (UC) includes country, pop, religious, and film music. The last factor, namely Energetic and Rhythmic (ER), is composed of rap, soul, and electronic music. The results of the test with the current sample indicate satisfactory internal consistency in all four dimensions: Reflective and Complex (Cronbach’s α = .76), Intense and Rebellious (Cronbach’s α = .86), Upbeat and Conventional (Cronbach’s α = .79), and Energetic and Rhythmic (Cronbach’s α = .69).
Functions of music
To measure the functions ascribed to music, we used Schäfer and Sedlmeier’s (2009) scale as adapted for application in Poland (see Lawendowski & Besta, 2020). This questionnaire includes 11 test items (Schäfer, Sedlmeier, et al., 2013) which are ordered into the following three basic music functions: self-awareness and the regulation of the “self” system (e.g. “I listen to music because it lets me forget my problems”), social functions of music that concern the feelings of belonging and communication with a social group (e.g. “I listen to music because it helps me feel close to others”), and emotional and arousal regulation and stimulation (e.g. “I listen to music because it energizes me”). The participants answered on a 7-point scale (1 = strongly disagree, 7 = strongly agree). Cronbach’s alpha reliability coefficients in the current sample were as follows: .84 for self-awareness, .78 for social, .61 for emotional and arousal regulation and stimulation.
Procedure
The sample was obtained by approaching members of an Internet-panel, wherein individuals displaying BPD-spectrum symptoms and those manifesting no BPD symptoms were recruited through Facebook social media. A link containing an invitation and information on the survey was posted in closed support groups for people suspected of having symptoms on the BPD spectrum, those already diagnosed, and also their relatives. The exclusion criterion was below the age 18. Data collection used convenience sampling. The survey was fully anonymous and it was not intended to provide clinical diagnosis. The data generated two groups of the respondents: those with low and with high probability of the presence of BPD.
Ethics statement
The study was carried out in accordance with the Declaration of Helsinki and the guidelines of the Ethics Committee at the Institute of Psychology of the University of Gdańsk. It did not include ethically doubtful procedures, sensitive data, or vulnerable populations. Participants were given detailed information about the study and their role in it, assured that they would be providing data anonymously, and told that they could withdraw at any point. Obtaining formal and written informed consent was not regarded as necessary, as voluntary completion of the questionnaires was regarded as providing consent. No medical information was collected.
Results
To explore the hypotheses, mediation analyses were conducted by applying the Hayes and Preacher procedure (Hayes & Preacher, 2010) involving a structural equation models framework, using the “lavaan” package (Rosseel, 2012; Yoon & Choi, 2015) in the environment of R 4.05 for Windows (R Core Team, 2020). All analyses were undertaken using bootstrap resampling through the k = 1000 random resampling procedure to obtain percentile confidence intervals for direct, indirect, and total effects as suggested by MacKinnon (2012).
A Pearson’s linear correlation analysis was conducted between the BPD symptoms severity measure and the measure of music preferences and functions of music. The adopted model illustrates the assumption that BPD symptom severity interacts with preference for each of the music factors directly and indirectly through each of the three fundamental functions of music. The overall research model is presented as a path diagram below (Figure 1).

Final Model of the Relationship Between BPD Symptoms, Functions of Music, Music Preferences.
The analysis indicates that the mediating role of the functions of music in molding the relationship between BPD symptom severity and music preferences is only found for IR music preference (λ = .013, β = .050, R2MED = .356) and ER music preference (λ = .006, β = .027, R2MED = .091) factors (Table 2). Together, all the functions of music account for about 35.6% of the relationships between BPD symptom severity and IR music preference and about 9.1% of all relationships between BPD symptom severity and ER music preference. Detailed analysis of the mediation effects indicates that among the functions of music, self-awareness (λ = –.01, β = –.039, R2MED = .17), and social relatedness (λ = –.008, β = –.031, R2MED = .14) functions are found to explain approximately 17% and 14%, respectively, of all the relationships between BPD symptoms and IR music preference. In contrast, the relationship between BPD symptoms and ER music preference is substantially (at the limit of the adopted level of significance) mediated by the arousal and mood regulation (λ = .003, β = .003, R2MED = .059) and social relatedness (λ = –.005, β = .025, R2MED = .048) functions, which enable us to explain approximately 5.9% and 4.8%, respectively (Tables 2 and 3).
Summary of the Results of the Analysis of Mediating Effects of the Music Functions on the Shaping of Relationships Between BPD Severity Symptoms and Music Preferences.
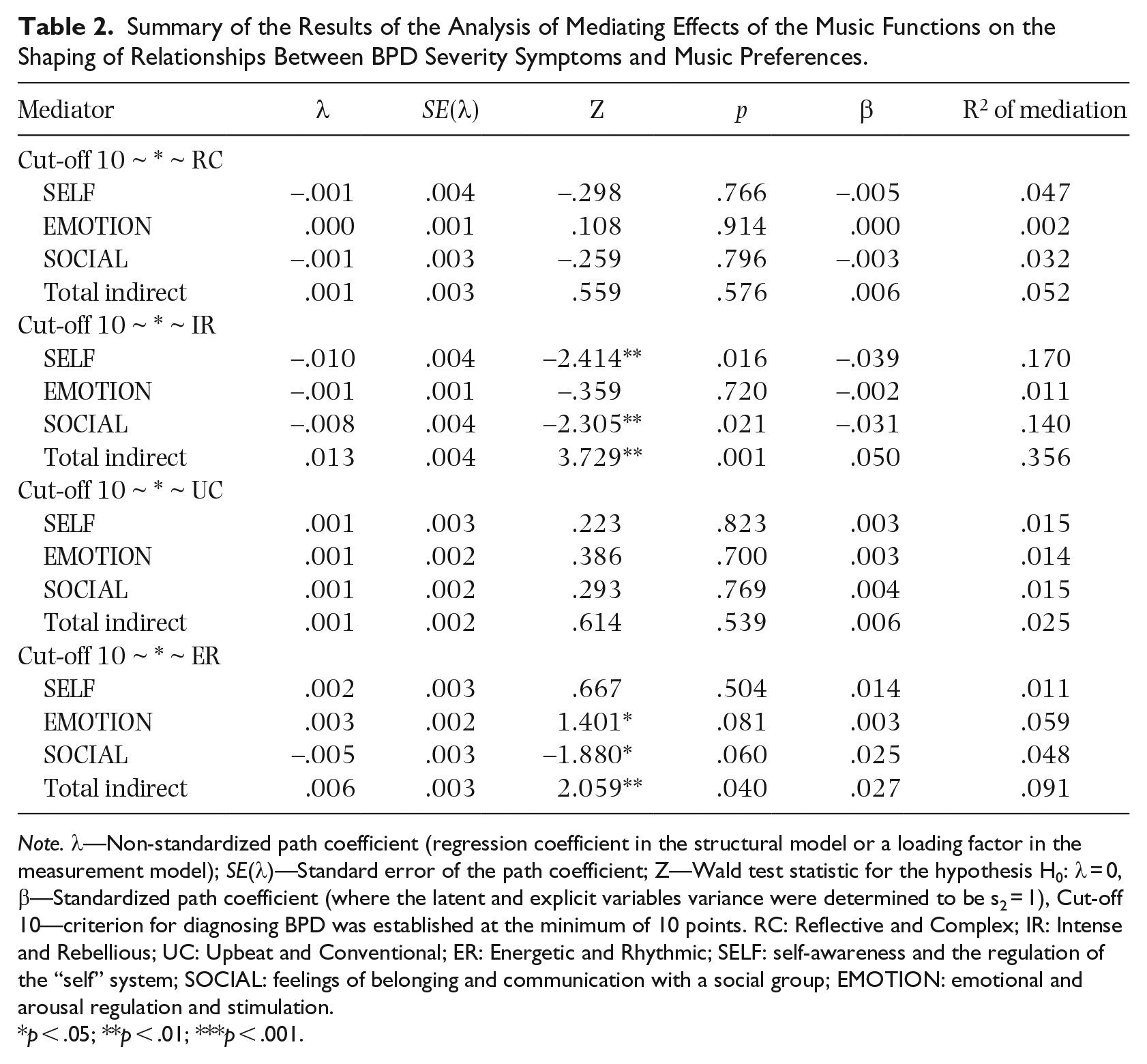
Note. λ—Non-standardized path coefficient (regression coefficient in the structural model or a loading factor in the measurement model); SE(λ)—Standard error of the path coefficient; Z—Wald test statistic for the hypothesis H0: λ = 0, β—Standardized path coefficient (where the latent and explicit variables variance were determined to be s2 = 1), Cut-off 10—criterion for diagnosing BPD was established at the minimum of 10 points. RC: Reflective and Complex; IR: Intense and Rebellious; UC: Upbeat and Conventional; ER: Energetic and Rhythmic; SELF: self-awareness and the regulation of the “self” system; SOCIAL: feelings of belonging and communication with a social group; EMOTION: emotional and arousal regulation and stimulation.
p < .05; **p < .01; ***p < .001.
Summary of Path Model.

Note. λ—Non-standardized path coefficient (regression coefficient in the structural model or a loading factor in the measurement model), SE(λ)—Standard error of the path coefficient, Z—Wald test statistic for the hypothesis H0: λ = 0, β—Standardized path coefficient (where the latent and explicit variables variance were determined to be s2 = 1), Cut-off 10—criterion for diagnosing BPD was established at the minimum of 10 points. RC: Reflective and Complex; IR: Intense and Rebellious; UC: Upbeat and Conventional; ER: Energetic and Rhythmic; SELF: self-awareness and the regulation of the “self” system; SOCIAL: feelings of belonging and communication with a social group; EMOTION: emotional and arousal regulation and stimulation.
p < .05; **p < .01; ***p < .001.
Detailed analysis of the path model indicates that BPD symptom severity is substantially related to the following functions of music: self-awareness (λ = –.069, β = –.294) and social relatedness (λ = –.051, β = –.22), where the more severe the BPD symptoms, the lower the score for the self-awareness and social relatedness functions (Table 3). BPD symptom severity accounts for about 8.5%–8.6% of the score differentiation within this domain.
At the same time, a direct effect of BPD symptom severity on all (except ER) music preferences was revealed, where the higher the BPD symptom severity, the more preferred the music for the following music factors: RC (λ = .026, β = .11) and UC (λ = .043, β = .227), whereas IR music was less preferred (λ = –.051, β = –.19). BPD symptom severity directly accounts for 1.2%–5.2% of the preference variability in these music factors.
In summary, the analysis partially supports the hypothesis that the functions of music mediate the relationship between BPD symptom severity and music preferences (Figure 2). Moreover, the functions of music mediate the relationship between BPD symptoms and IR music preference, where self-awareness and social relatedness functions are of crucial importance. In addition, the functions of music are a complete mediator of the relationship between BPD symptoms and ER music preference, with the special role of arousal and mood regulation and social relatedness functions being notable. In practice, this means that IR music preference depends only partly on BPD severity, and partly on how BPD affects the functions of music. In contrast, ER music preference depends entirely on the way BPD affects the functions of music, focusing, in particular, on arousal and mood regulation and social relatedness functions.

Final Model of the Relationship Between BPD Symptoms, Functions of Music, Music Preferences.
Discussion
The model of relationship presented in the study supports existing evidence that personality characteristics may shape listeners’ music preferences (Dunn et al., 2012; Greenberg et al., 2022; Rentfrow & Gosling, 2003; Schäfer & Mehlhorn, 2017). However, a novelty in the presented model is the assumption that the influence of the personality variables on shaping music preferences in the typical population may be mediated (i.e. accounted for) by the perception of the functions of music related to arousal and mood regulation, social relatedness and self-awareness. On one hand, these functions may be predicted based on personality variables, whereas on the other hand, they interact with the music preferences of the individual. This general assumption of this study was further extended to include specific personality factors related to the presence of personality disorder symptoms on the BPD spectrum. Nevertheless, it is assumed that the relationships under analysis may also pertain to personality in its broad sense (e.g. Samuel & Widiger, 2008).
The present results generally confirm the assumptions of the model presented here. At the level of simple correlation, the severity of BPD symptoms is significantly related to the music preferences for Intense and Rebellious, Upbeat and Conventional, and Reflective and Complex music genres, but not Energetic and Rhythmic. Individuals with higher severity of BPD-spectrum disorder symptoms manifest stronger preferences for Reflective and Complex and Upbeat and Conventional music, whereas, at the same time, displaying lower preference for Intense and Rebellious music. In contrast, direct connection between the severity of BPD symptoms and the preference for the music grouped under the ER music factor turned out to be negligible and statistically insignificant. This implies that music genres grouped under this factor are preferred (or not) irrespective of BPD symptoms severity. Thus, H1 has been partially supported.
Prior analyses (Samuel & Widiger, 2008; Widiger et al., 2002) using the five-factor personality model have consistently demonstrated that individuals with BPD display a high level of neuroticism and low levels of amicability and conscientiousness. Some studies have shown the relationship between neuroticism and the preference for pop music (e.g. Rawlings et al., 1995), which is supported by the present findings of simple correlations between personality traits and preference for Upbeat and Conventional music (including pop music). However, Langmeyer et al. (2012) have demonstrated that neuroticism can predict preference for Upbeat and Conventional music and lack of preference for Intense and Rebellious music, which is supported by the present findings.
The severity of BPD symptoms is clearly related to the perception of social relatedness and self-awareness functions of music, whereas the arousal and mood-regulation function seems independent of the severity of BPD symptoms (H2 partially supported). Moreover, a higher severity of BPD symptoms is related to lesser importance being attributed to the social relatedness and self-awareness functions of music. This means that individuals with high severity of BPD symptoms perceive music as a less useful means for expressing or exploring their self-awareness or shaping social interactions. Hence, perception of emotional functionality of music is poorly associated with BPD symptoms severity. Thus, the assumption, present in the literature, that one’s psychological condition determines the reasons for the use of music, is confirmed (Getz et al., 2012; Kuntsche et al., 2016; Randall et al., 2014; Vella & Mills, 2017).
The mediation analyses to assess the strength of the indirect relationship between BPD symptom severity and music preferences through perception of the functions of music indicate that the functions of music act as a partial mediator in shaping the formation of music preferences as based on personality predispositions (H3 partially supported). Thus, the studies conducted confirm the existence of the link between the preference for a particular type of music and the various psychological functions of listening to it (Schäfer & Sedlmeier, 2009).
This implies that psychological dimensions of the individuals with BPD symptoms in which their difficulties and deficits are diagnosed, may, through functions ascribed to music, be manifested in specific music preferences. Herein, self-awareness and social relatedness functions are particularly helpful in explaining this relationship. These results indicate that a higher severity of BPD symptoms is related to a lower preference for Intense and Rebellious music. This mechanism can be partly explained by the lower significance of the self-awareness and social relatedness functions of music among individuals with BPD, whereas such functions may directly favor Intense and Rebellious music preference (interestingly enough, with regard to arousal and mood-regulation function, this is a negative correlation). From a practical perspective, this result can be interpreted in that individuals displaying high severity of BPD symptoms tend to value Intense and Rebellious music less. This may be because BPD symptoms foster difficulty in perceiving the social relatedness and self-awareness functions of music that are essential to enjoy this kind of music.
The results also confirm the essential role of the functions of music in mediating between personality factors and preferences for Energetic and Rhythmic music, although, in this case, the functions of music act rather as a suppressor. In other words, they help reveal a genuine relationship that is difficult to observe directly due to non-specific interactions of mediating factors. One of these factors appears to be the functions of music, in particular, the functions of arousal and mood regulation and of social relatedness. This allows the observation that the relationship between BPD symptom severity and preference for Energetic and Rhythmic music (although insignificant at the level of simple correlations) turns out to be statistically significant after controlling for other variables.
Preference for Energetic and Rhythmic music may be because this music is perceived as facilitating social interactions (social relatedness function of music) and allows for tension relief and emotional release (arousal and mood-regulation function). However, the perception of these functions of music by individuals with high severity of BPD symptoms is hampered. Therefore, it can be assumed that the relationship between the severity of BPD symptoms and preference for Energetic and Rhythmic music is difficult to observe directly as the perception of the functions which are crucial in this type of music is distorted.
The results also confirm the significance of the functions of music in mediating between identity factors and Upbeat and Conventional music preference. In this case, the function of arousal and mood regulation acts as a mediator between the variables described. This means that emotional effects among individuals with BPD that are directly obtained through music may lead to preferences for Upbeat and Conventional music.
The results do not support the assumed model of relationship between BPD symptom severity and preference for Reflective and Complex music. While at a simple correlational level, the severity of the BPD symptoms may shape preferences for Reflective and Complex music (as individuals with high severity of symptoms are more apt to prefer this type of music), the functions of music fail to sufficiently account for this relationship. No empirical support has been found for the assumption that the self-identity function, arousal and mood-regulation function or social relatedness function of music may be crucial for Reflective and Complex music preference. Thus, it is possible that there is some other mechanism that has not been explored that goes beyond the functions of music may account for the relationship between BPD symptom severity and Reflective and Complex music preference.
Limitations and future research directions
It is possible that the measures used do not completely capture the picture of functioning of individuals with BPD. Furthermore, it is possible that the personality measure may not have been adequately sensitive regarding differences in the severity of particular disorders within BPD. In addition, we did not investigate if and at what stage of therapy the participants of the study were in, thus treating this as a homogeneous group despite the potential for further variation within the group.
The diversity of the results obtained may be accounted for by the fact that the BPD disorder has an extremely complicated structure and is composed of heterogeneous psychological states that should be further controlled in future work. The manner in which we approached the issue, however, enabled the forming of heterogeneous groups—similarly to the variables of the disorder under analysis. What is more, due to pandemic restrictions, it was difficult to test the participants in a more detailed way. In future, demographic variables, such as gender, age or music education which have also been shown to affect music preferences should also be taken into account. Moreover, although the pathology of personality organization and structure is relatively permanent and stable, its manifestations may change depending on the level of stress an individual is affected by (Cierpiałkowska & Marszał, 2013). Therefore, it is worth undertaking longitudinal studies that will allow (a) following the variability over time of the determinants of music preferences and functions of music in the course of BPD and (b) answering the question of how music functions may explain the effectiveness of music therapy (and thus, also the participants’ responsiveness to music therapy).
Knowing that music choices may be an expression of personality, we should still remember that it is not their only function. The search for mediators such as the functions of music as tested here is of essential importance. Even though the present evidence suggests that the above-mentioned relationship may be strong, it may not hold under all circumstances or for all types of people. To date, we lack knowledge as to the reasons why the functions of music are partial or full mediators of music preferences among individuals with BDP symptoms. While these relationships are still to be fully explored, this article presents a first step toward understanding them.
Conclusion
Past studies have shown that the relationships between music preferences (genres) and mental disorders have not generated sufficient evidence for causal relationships between variables. This study has demonstrated the existence of the bridge between music preferences and the personality characteristics of individuals with BPD symptoms through the fact that music preferences are rooted in personality characteristics. In this relationship, a mediating role is at least in part also played by the functions of music.
Diagnosing music preferences would facilitate a precise measurement of actual music preferences in specific samples and allow for creating scenarios that would find use in music therapy practice. Tapping into music preferences of individuals with different BPD symptoms severity, as well as discovering the psychological functions of music, may lead to quicker and more effective selections of therapeutic methods. The current results lead to the conclusion that the same types of music should not be used for the same goals, for example, relaxation, for individuals differing in terms of personality traits (especially those comprising BPD). In light of the current results, respecting individual differences at the level of personality traits seems to be a part of best music therapy practice. Without it, the entire therapeutic process may bring about undesirable effects. The applied significance of this study lies in the fact that personality traits may yield unique data about music preferences, which cannot be inferred elsewhere.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.