
Abstract
When mothers of preterm infants are unable to produce sufficient volumes of breastmilk, neonatologists in many Western countries prescribe pasteurized donor breastmilk. Breastmilk has a paradoxical presence in the neonatal intensive care unit: while it has therapeutic properties, it also has the potential to transmit disease. National health authorities and local neonatal intensive care unit policies each delimit the safety of donor milk by focusing on the presence or absence of pathogens. It is in this light that breastmilk from the human milk bank is both sought and legitimated to minimize safety concerns. This research uses data arising from an ethnographic study of two human milk banks and two neonatal intensive care units in the United States, and 73 interviews with milk donors, neonatal intensive care unit parents and clinicians. The primary research question framing the study was ‘What are the underlying processes and practices that have enabled donor milk to be endorsed as a safe and legitimate feeding option in neonatal intensive care units?’ This study is framed using three key principles of Latour’s ‘new critique’, namely, adding to reality rather than debunking it, getting closer to data rather than turning away from fact and creating arenas in which to assemble. As a result, conceptions of donor milk’s safety are expanded. This case study of donor milk demonstrates how Latour’s new critique can inform science and technology studies approaches to the study of safety in health care.
Introducing donor breastmilk
The contradictions and politics of breastmilk transactions come to the fore in neonatal intensive care units (NICUs), where care is provided to the most fragile, preterm and acutely sick infants. Breastmilk is promoted as the best and safest food for preterm infants (American Academy of Pediatrics (AAP), 2012). Human milk, not bovine-derived infant formula, is most easily digested and has bioactive factors that assist in gastrointestinal development and provide immunity to infections (Ewer et al., 1994; Wight et al., 2008: 14). Breastmilk also offers protection against a severe, sometimes fatal, gastrointestinal condition called necrotizing enterocolitis (NEC) (Schanler, 2007; Sullivan et al., 2010), which has an incidence of approximately 7 percent in preterm infants (Neu and Walker, 2011). For these reasons, ‘best practice’ stipulates that NICU health professionals should assist mothers in providing their own breastmilk to their hospitalized preterm infants (Meier et al., 2010; Rodriguez et al., 2005). However, as a result of premature delivery, maternal illness and physical separation from their infants, it is not uncommon for NICU mothers to experience a delay in breastmilk production or difficulty in providing sufficient volumes (Arnold, 2010: 130–131; Schanler et al., 1999). In situations where preterm infants are unable to suckle, their mothers can express their own breastmilk and then feed them via a gavage or bottle. Expressing sufficient breastmilk can be difficult and time-consuming (Hurst et al., 2013; Swanson et al., 2012), because every 3–5 hours, day and night, for weeks or even months, the NICU mother must mimic a ‘normal’ term newborn’s suckling pattern by using an electric breast pump to stimulate the breast to produce milk, and then extract it into a bottle for storage. If a mother is unable to provide sufficient volumes of breastmilk to her NICU infant, the World Health Organization (WHO) and the AAP recommend that donor breastmilk (DBM) be sourced from a human milk bank (HMB) in preference to the use of artificial infant formula (AAP, 2012; WHO United Nations Children’s Fund (UNICEF), 2003).
The safety of breastmilk transactions in the NICU
This article analyses a set of safety-constructing practices that legitimate donor milk transactions. There is significant debate about safety in infant feeding (see Gribble and Hausman (2012), Wolf (2011)). Such discourses are symbolic of how breastmilk is positioned in Western society (Boyer, 2010; Gribble and Hausman, 2012). Notwithstanding the powerful social symbolism and ubiquitous health promotion message of ‘breast is best’ (Wolf, 2011), breastmilk as a female bodily fluid is also constructed as indeterminate and suspicious (Benn and Phibbs, 2007; Bramwell, 2001). Breastmilk can harbour viruses and is seen by some as a risky fluid and a ‘conveyor of contamination’ (Hausman, 2011: 120). Thus, it shares ‘an ontological status with other substances that cross the body boundary and have been vilified to a greater or lesser extent’ (Boyer, 2010: 10). In sum, breastmilk occupies a paradoxical position in the NICU (Bartle, 2010), of which donor milk is a prime case study; it is prescribed due to its therapeutic and preventative effects but with simultaneous concern about its potential for harbouring pathogens.
The use of DBM is on the rise in North American NICUs (Miracle et al., 2011; Perrine and Scanlon, 2013). Yet, feeding any mother’s milk to an unrelated infant is not always encouraged by the presiding health authorities (AAP, 2012; Centers for Disease Control and Prevention, 2009; US Food and Drug Administration (USFDA), 2010) or in policies that guide local NICU clinical practice (Geraghty et al., 2013). The USFDA, for example, advises against obtaining breastmilk from the Internet, suggesting instead that ‘there are human milk banks that take voluntary steps to screen milk donors, and safely collect, process, handle, test, and store milk’ (USFDA, 2010). Further evidence of concern about breastmilk transactions can be found within the hospital policies that govern episodes of ‘misappropriated breastmilk’. Typically, these errors in breastmilk feedings occur as a result of poor milk labelling or storage systems, staff fatigue, and/or two infants having similar surnames. Breastmilk misappropriation errors occur at a rate of 0.07–0.14 per 1000 NICU feedings, although the rate is probably higher, as not all errors are detected or reported (Rinke et al., 2011). In the event of misappropriated breastmilk, the affected baby, her mother and the mother whose milk was accidentally administered are all tested for viruses that are transmissible by breastmilk (Rinke et al., 2011). In the vast majority of cases, viral tests are returned with a negative result, and no harm is caused to the baby (Gabrielski and Lessen, 2011; Rinke et al., 2011; Zeilhofer et al., 2009). Still, misappropriation produces staff stress, a loss of families’ trust in the hospital system (Gabrielski and Lessen, 2011; Rinke et al., 2011), and ‘enormous psychic stress to the mother whose baby received the milk of another woman’ (Zeilhofer et al., 2009: 1277). Put simply, misappropriated breastmilk is considered a hospital error and a threat to patient safety (Rinke et al., 2011).
A mother’s own milk, DBM, breastmilk sourced from the Internet and misappropriated breastmilk are each classified as human milk, yet each is accorded a different status, ranging from the ‘liquid gold’ of mothers’ own milk to the ‘potentially dangerous’ classification assigned to both misappropriated breastmilk and breastmilk procured through the Internet. Donor milk and misappropriated breastmilk are positioned as unlikely to provide substantial risk to an infant’s health, yet they hold contrasting positions in relation to the use of a mother’s own milk. Of relevance to safety, concern about breastmilk transactions erupts when flows of breastmilk go ‘against’ the normative direction, that is, from the mother to her biological or gestational infant (Shaw, 2007, 2010b). 1 Despite a mother’s own expressed breastmilk potentially harbouring pathogens (Dahaban et al., 2013; Jeurink et al., 2013), only when breastmilk is fed to a ‘biologically unrelated infant’ is it ‘subjected to stringent microbiological standards’ (Cossey et al., 2011: 834–836). This suggests that the fear of disease transmission or risk to the infants’ health is not the sole factor underlying the safety and risk management practices uncovered in this research. In this article, I ask, ‘What are the practices that have enabled donor milk to be endorsed as the safest and most legitimate feeding option when mother’s own milk is unavailable?’ To answer this question, I reveal previously unrecognized labours that contribute to and re-describe donor milk’s safety. Importantly, these practices do not only occur in the HMB, but in the homes of donors, and in the NICU. I argue that the definitions of safety need to be expanded away from being solely about medical risk and the presence or absence of pathogens, and be more inclusive of the diverse institutions, actors and practices involved in the attainment of safety.
A ‘new critique’ of safety in health care
To broaden understandings of how the safety of DBM is constructed so that it may be legitimately used in the NICU, I draw upon three principles of Latour’s (2004) ‘new critique’ and link them to recent developments in science and technology studies (STS) research on safety in health care.
First, rather than subtracting from reality by deconstructing or debunking fragile beliefs and practices in which the participants are invested, the new critique respects the fragility of the ‘matters of concern’ and proceeds with care and caution through a process of adding to reality (Latour, 2004: 232). Thus, the agent of the new critique is ‘not one who debunks, but the one who assembles’, or ‘detects how many participants are gathered in a thing to make it exist and to maintain its existence’ (Latour, 2004: 246). Although not explicitly labelled as such, the same spirit is found in the work of some STS researchers of safety in health care (Jerak-Zuiderent, 2012; Lopez et al., 2010; Mesman, 2007, 2009; Zuiderent-Jerak et al., 2009). For example, in a study of the accomplishment of safety in a telecare service for the community-dwelling elderly population, Lopez et al. (2010) emphasized the contribution and delicate balance of various technologies, practices and care. Similarly, Mesman’s (2007, 2009) work on infection control in NICUs also finds that safety-generating practices are diverse and stretch far beyond technical interventions. She highlights clinical staff’s investment in reasoning, legitimizing, speaking and interpreting practices to produce safe care (Mesman, 2008). Latour’s ‘new critique’ is encapsulated by such approaches to safety in health care for they ‘add to’ dominant techno-centric and risk-oriented approaches. Both Lopez et al. (2010) and Mesman (2007, 2009), for example, argue for a wider analytical scope for patient safety research, one that is not based singularly on technology, or error identification and deficits, but one that includes care and attention to the deliberate production of safe practice. Rather than pursuing a deficit focus through the deconstruction of safety errors, the practices that generate safety can be assembled and ‘re-described’ so that a more diverse, inclusive and arguably more ‘safe’ model of care is brought into existence (Bruun Jensen, 2010: 7–8). In this article, I seek to add to predominant notions of safety in the study of DBM. Rather than merely challenging the pathogen-centric notion of safety and the technical interventions involved, I argue that this is only part of the labour of producing safety. Therefore, I move beyond the walls of the HMB to see how donor milk safety is brought into existence in other institutions.
Second, Latour’s (2004) ‘new critique’ advises researchers to ‘get closer’ to the highly situated, complex and messy ‘matter of concern’ (p. 231). To get closer to the production of safety as a matter of concern requires ‘intimate understandings of actions and situations that enhance or undermine safety in the everyday’ (Jerak-Zuiderent, 2012: 734). This is important not only for researchers but also for clinicians and clinician-participants who can then ‘engage with, and learn from, the messiness of everyday work’ (Iedema, 2009) and increase their awareness of their own ‘resources of resilience’ (Mesman, 2007). One means through which to achieve this is by adopting an ethnographic approach to examine the complexity of practice and multiple ontologies that comprise safe health care (Hor et al., 2013; Iedema, 2009; Iedema et al., 2013; Jerak-Zuiderent, 2012; Lopez et al., 2010; Mol, 2002; Mol and Mesman, 1996). Ethnographic approaches to the study of safety in health care aid the ‘new critic’ by providing data that resist privileging abstracted representations and avoid positioning these as something that can be considered separately from the practices from which they arise (Bruun Jensen, 2010; Mol, 2002; Zuiderent-Jerak et al., 2009). For example, one ethnographic study found that the practices that constitute ‘fact’ in everyday hospital life, such as the tests and decision-making invested in the making of a definitive diagnosis, can be ‘bracketed’ such that the diagnosis becomes a ‘referent in pre-existing reality’ (Mol, 2002: 163). This serves to enhance credibility, enable efficiency and ensure that treatment planning progresses (Mol, 2002: 163). Similarly, a doctor’s statement that ‘donor milk is safe’ provides credibility to an ‘unknown substance’ and therefore reassures anxious parents and enables an infant to be fed. However, the predominance of such statements of fact can also unintentionally sacrifice the disclosure of the safety-generating practices to the very audiences that may need to know about them. Therefore, by ‘getting closer to data’ through the use of ethnography, I assemble the various and previously unrecognized safety labours that accompany donor milk on its journey into and through the NICU and bring them to the attention of safety scholars, STS academics and the practitioners involved in milk donation.
Third, the new critique offers participants ‘arenas in which to gather’ (Latour, 2004: 246). Some health-care safety researchers enact this through ‘forums of engagement’ (Carroll et al., 2008; Iedema and Carroll, 2013; Iedema et al., 2013; Mesman, 2007) or ‘artful contamination’ (Zuiderent-Jerak and Bruun Jensen, 2007) with participants. In one interventionist ethnographic NICU study, Mesman (2007) actively involved herself in various patient safety committees. By assembling those who strove to improve patient safety in their own hospital, alongside the ‘doing’ of her own research, Mesman (2007) literally offered ‘participants arenas in which to gather’ (Latour, 2004: 246). Throughout the fieldwork conducted for this research, I used the methodology of ‘video reflexive ethnography’ to create forums of engagement (Iedema and Carroll, 2011) between myself and the NICU clinician-participants in which to discuss various issues associated with using donor milk in the NICU. I also returned to the field sites to engage in a dialogue about aspects of my research ‘findings’ with the NICU staff and broader community. However, in these forums of engagement, I did not have the opportunity to harness and communicate the multiplication (Mol, 2002: 82) of the realities that contribute to, and define, donor milk’s safety. Therefore, I use this article to speak at length to a broader audience, and to foreground diverse practices both as new information and as a new frame of safety. This forum honours those involved in producing, pasteurizing and prescribing breastmilk, and those who choose to research, read and write about it. Therefore, I deliberately write in a way that transcends disciplinary boundaries so that different parts of this article may each appeal to the diverse participants that are called forth in the analysis of the safety of donor milk. It is in this way that I hope to create a transdisciplinary arena so that we, a transdisciplinary community, can gather, learn and discuss the safety of breastmilk transactions.
Sites of engagement: an account of the methodology used
Ethnography enables observation of work practices and rituals in the organizational environment that (re)creates order (Law and Lien, 2012). With the assumption that safety was one such paramount ‘order’, my aim was to trace the flow of breastmilk from the providers of DBM, through the HMB, and then into the NICU to examine how safety was constituted through practice. Data arising from two ethnographies in two HMBs and two NICUs and 73 interviews conducted during 2011 and early 2012 form the basis of this account. Fieldwork was conducted over a 6-month period in mid-western and western states of the United States. Conducting fieldwork across multiple institutions in two different states enabled immediate comparison between the practices and discourses enacted in each location, and strengthened the transferability of expanded notions of safety to other NICUs in advanced, capitalist, Western countries that use DBM from an HMB, such as the United Kingdom, Canada, Italy and Australia. The two study NICUs were selected because they each used DBM and were accredited as Level III NICUs. This accreditation means that they have the appropriate staff expertise and substantial medical technologies to care for the sickest and most premature of newborn infants (AAP, 2004). These infants have the greatest medical necessity for DBM because they are most vulnerable to the negative effects of bovine-based artificial infant formula and are at the highest risk of NEC (Neu and Walker, 2011). The two HMBs were purposively selected, as they provided DBM to the study NICUs. 2 This enabled a thorough investigation of the practices that enabled the ‘flow’ of milk from donor to recipient.
The institutional practices and discourses of those involved in donating, processing and prescribing breastmilk were systematically observed. This revealed how DBM was transformed or ordered – materially and discursively – into a ‘safe’ product for use in the NICU. In the HMB, I observed the recruitment and screening of donors; the handling, testing and pasteurization of donated breastmilk; and the processes involved in distribution of breastmilk to hospitals. I assisted staff with washing bottles, pasteurization and sorting frozen incoming donations of milk. This provided an embodied understanding of the significant labour undertaken by HMB staff. In the NICU, my observations focused on clinical activities, decision-making and communications associated with infant feeding, and the handling or use of DBM. Due to the primacy of growth and nutrition to neonatal care, a large portion of talk and tasks in the NICU are either directly or indirectly dedicated to feeding, from the practical task of nurses ‘doing’ infant feeding through to neonatologists’ decision-making about feed volume, fortification, or the interpretation of test results (Mol and Mesman, 1996). Consequently, I observed a wide variety of practices, including doctors’ prescribing decisions, nurses establishing an infant’s feed tolerance, and lactation consultants establishing whether or not mothers were expressing their milk effectively. All participants were provided with written and verbal information about the research and signed a consent form. 3 Additionally, verbal consent was obtained from participants before each session of observation. The ethnography or ‘praxiography’ (Mol, 2002) provided insights into how DBM, as a scarce resource, is utilized, framed and accepted by clinicians and parents, and in which conditions or in what situations it is prescribed for infants. 4
All interview participants (Table 1) were recruited during ethnographic fieldwork in the NICUs and HMBs, except for the donor cohort. Instead, 65 donors were identified from one HMB’s donor database and were sent a research package that included an introductory letter about the research and a ‘consent for contact’ letter. In all, 25 (38%) donors returned their consent forms and participated in a semi-structured interview, which was audio recorded, and then transcribed by a professional transcriber. The transcripts were checked by the author and imported into HyperResearch coding software (HyperRESEARCH 3.0.2 Computer Software, ResearchWare, Inc., 2011) for thematic analysis. The diversity of practices required that the data from NICU parents, NICU clinicians, HMB staff and milk donors be coded separately.
Semi-structured interviews.
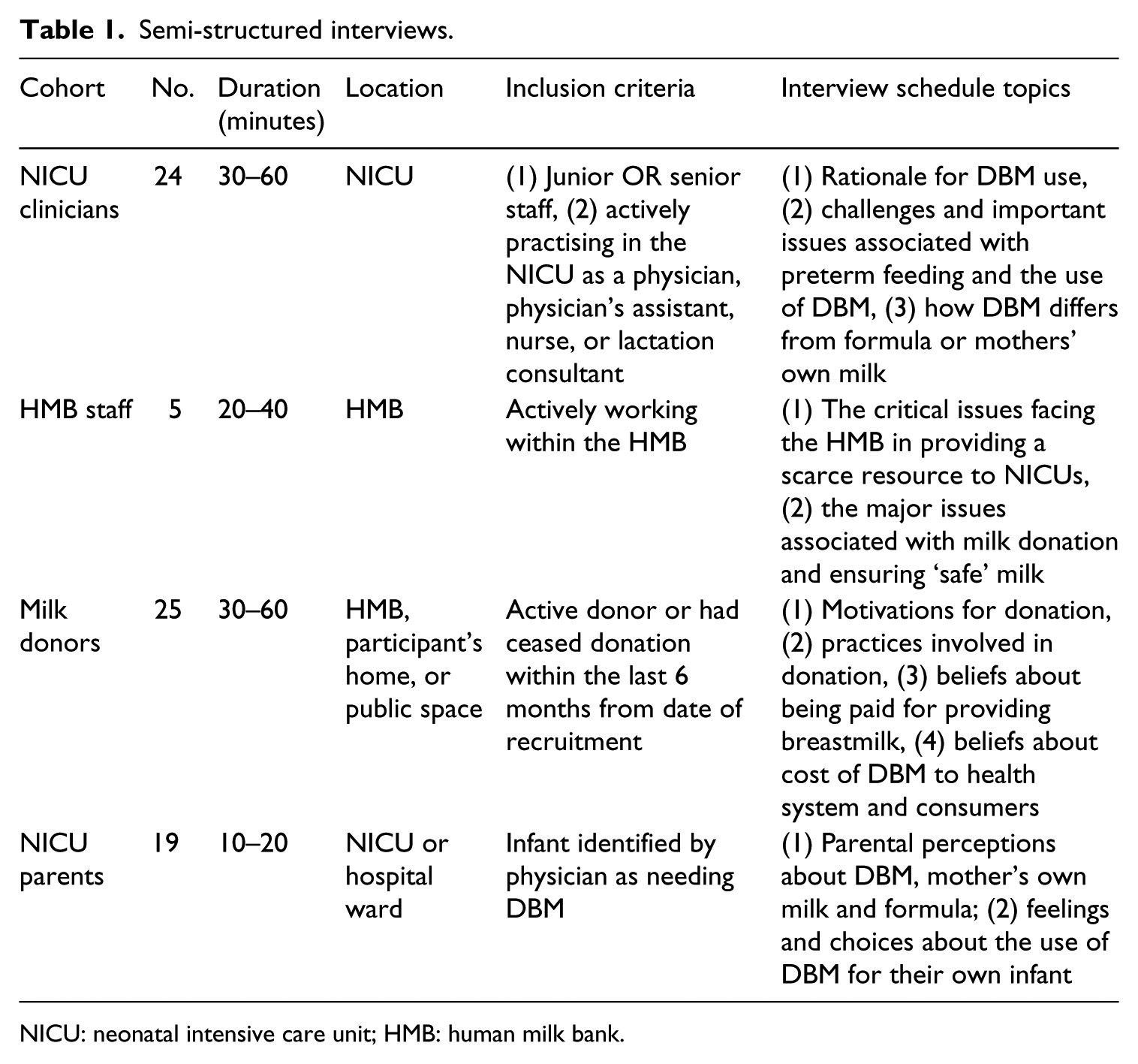
NICU: neonatal intensive care unit; HMB: human milk bank.
Constructing safety: the HMB, donor and neonatologist
The HMB: material labour, material transformations
Breastmilk that has not been produced by the infant’s mother must be deemed to be safe before it is fed to preterm infants in NICUs. In the majority of cases, DBM will be ordered (via a doctor’s prescription) from an HMB. In the United States, the DBM used in NICUs has been donated anonymously by lactating women who may have a store of frozen breastmilk that they cannot use (Arnold and Lockhardt-Borman, 1996). Alternatively, some women choose to deliberately pump extra breastmilk with the sole purpose of donation (Arnold and Lockhardt-Borman, 1996). The early 1980s saw the peak of human milk banking, with 30 active HMBs in the United States. The crisis of HIV/AIDS in the mid-1980s and the discovery that the virus could be transmitted through breastmilk saw the closure of HMBs (Jones, 2003: 315). Also in the 1980s, laboratory techniques were developed for detecting HIV in serum and the scientific verification of the benefits of human milk for infant health expanded (Miracle et al., 2011). This led to a revival of the human milk banking industry (Miracle et al., 2011) in addition to the establishment of the Human Milk Banking Association of North America (HMBANA), under whose auspices, with guidance from the USFDA and the AAP, the standards for operating an HMB were developed in 1990 (Jones, 2003; Tully, 2000). These standards include guidelines for donor screening. Should the donor pass the initial lifestyle and lactation screening questionnaire, she is then required to provide a blood sample and pass a test for HIV/AIDS, Hepatitis B and C, HTLV 1 and 2 and syphilis (HMBANA, 2011). The safety records of HMBANA HMBs are flawless. An early review of the donor data of HMBANA milk banks found that
the donor screening process appears to be sufficiently thorough to protect both recipients and donors … Out of the entire population, less than 1% (0.52%) of potential donors received positive serum test results, all of which proved to be false positives. (Tully, 2000: 236)
Such statements of safety are typical of HMBANA and its members. For HMBANA HMB staff, who usually frame safety in terms of donor screening, pasteurization and microbial testing of breastmilk, the provision of safe milk to the NICU is paramount:
The critical issue is making sure that our milk is safe. Which we obviously do with having it checked for cultures and making sure our processes are what they are so that everything stays medically appropriate for those babies. (HMB #2 Community Outreach Worker)
DBM from HMBs is distinguished from breastmilk obtained through Internet-facilitated milk sharing by the safety processes of the HMBs (Geraghty et al., 2013; Keim et al., 2013) and their flawless track record (Cohen, 2007). Evidence gathered through my research interviews substantiates this view. For example, the directors of each HMB state,
I think it’s just plain dangerous. I know too much about transmission of diseases and medications and all of those kinds of things. There are all these new diseases, there are medications, there are illicit street drugs, and people don’t have your best interests at heart, even though they might tell you they do. So I think you’d be taking a big chance to receive milk from somebody who isn’t carefully screened and the milk was pasteurized. Milk banking takes the variable out of it. Never in the history of milk banking has there been an incidence of disease transmission, or a negative outcome with a baby. I mean, sure they [Internet sites] talked about, ‘Oh, screen your donors,’ and stuff like that, but it’s not the same screening, I’m sorry! (HMB #1 Director) when you buy milk over the Internet or you find someone through a friend of a friend, you don’t know anything about that person. The USFDA has come out and said, ‘informal milk sharing is not safe. (HMB #2 Director)
The HMB model of safety is similar to that of the blood banking system; it has multiple levels of screening based on social, psychological and technical protocols (HMBANA, 2011; Martucci, 2010). When a potential milk donor first contacts an HMB, she will be asked lifestyle and lactation screening questions and will only progress to the next stage of screening if she declares herself to be healthy, not taking regular medications or herbal supplements, a non-smoker, abstainer from regular alcohol consumption and a non-drug-user (HMBANA, 2011). This is deemed important because the infants receiving the milk are premature, immunologically fragile and receiving many medications in the NICU:
When I’m talking to a new donor on the phone, and we’re discussing if she’s taking any meds or had any alcohol or things like that, we tell them that our patients who are receiving it are usually in pretty critical and compromised medical conditions and we don’t know what other medicine that they could be getting or that their mother might be getting, if they’re getting some partial feedings from their own mom, and we just don’t want to have any drug interactions. (HMB #1 Donor Coordinator)
In an effort to ensure minimal chances of bacterial contamination of the milk donated, HMB staff provide detailed written and verbal education to all donors. Topics covered include optimal milk expressing techniques, safe milk storage and labelling methods. Donation guidelines are also discussed and include circumstances where donation should not occur. For example, donors are advised that they should not donate milk when taking certain medications, herbal teas, excess caffeine, any alcohol and if the donor or someone else in the household is infectious or unwell (HMBANA, 2011).
When the HMB receives the donated frozen breastmilk, the staff need to engage in administrative, classificatory and tracking procedures so that milk is traceable at all times from donor to recipient. The donor screening and education denotes the beginning of the classification work in HMBs that determines which breastmilk is suitable for donation to, and consumption by, sick preterm infants. A mere moment of this work is depicted in the fieldnotes recorded during the handling of incoming donor milk:
Dozens of little bags and bottles of donated breastmilk arrive in insulated coolers, packed with dry ice to keep the milk frozen. Staff immediately make an inventory of the milk with exclamations of glee such as ‘it’s like Christmas!’ as they cut open the boxes with a Stanley knife to gain access to the milk. Staff carefully and systematically record the name of the milk donor, the amount she has donated, and the month she has expressed each bottle of milk. I immediately begin sorting the donor’s milk into baskets for storage according to the month the milk was expressed: the white basket is for May, blue for June, yellow for July, red for August and green for September. One staff member expresses further excitement as she determines that one shipment contains preterm milk – milk that has been expressed during the first 4 weeks of a preterm infant’s life. This milk is scarce and is separated from the ‘term’ milk because it is higher in protein. It will be pasteurized separately. These details are recorded on the computer and the milk is provided with a specific shelf in the pre-pasteurization freezer for storage. (Fieldnotes, HMB #2)
Pasteurization and bacteriological testing are the final procedures for ensuring safety. Given the focus on manipulating the physicality of the breastmilk, the work HMB staff enact can be deemed ‘material labour’ (Dyer-Witheford, 2001). For any one batch of milk produced by the HMB, the staff commence by opening the dozens of bags arising from individual women’s milk donations, then pouring these into large glass flasks and thoroughly mixing the milk. This pooling process, which typically involves milk from between two and five different donors, achieves a more standardized product for the hospital system (Arnold, 2010). HMB staff then rebottle milk into purpose-specific containers, heat seal them and then load bottles into the pasteurizing machine, which destroys bacteria and viruses (Andersson et al., 2007; Van Gysel et al., 2012). The milk is then unloaded from the machine and refrozen while HMB staff await the outcomes of microbiological testing. Testing ensures the eradication of bacteria, pathogens and abnormal levels of skin flora (Kennaugh and Lockhart-Borman, 2011). If the batch fails microbiology testing, then staff at the HMB have to discard dozens of bottles of frozen milk. The amount of work involved in these processes is significant, and HMB staff at all levels of the organization recognize the labour involved:
The preparation of milk is very labour intense. It’s all done by hand. (HMB #2 Director) It’s really very physical. I’ve had a couple of accidents. I try to be careful. There’s a lot of lifting. I have carpal tunnel from doing 200 bottles a day by myself. (HMB #2 Pasteurizing Coordinator)
The account given thus far reveals that HMB staff enact significant amounts of interpersonal and ‘material labour’, and that this safety-generating labour can be obfuscated when health authorities and HMBs frame the safety of donor milk only as the presence or absence of any pathogens in the pasteurized DBM. It is the material labour enacted by staff within the HMB that converts some material constituents of the DBM and, as a result, transforms it from a ‘risky biosubstance’ (Boyer, 2010) with a ‘potentially’ pathogenic status into a known and ‘safe’ product whose ‘biovalue’ (Waldby and Mitchell, 2006) is deemed safe and ready for use in the NICU.
Constructing safety through the reproductive labour of milk donors
The non-pathogenic status of DBM is not simply a result of the technical intervention of pasteurization or the numeric indicators inscribed in the microbiology report. Many of the practices that contribute to the construction of donor milk as ‘safe’ occur prior to the pasteurization and microbiologic testing of breastmilk, including in the homes of donors. The following account of a milk donor’s investment in producing breastmilk for her own infant is typical of the relatively invisible and unacknowledged reproductive labour work enacted by women in the domestic sphere:
I was dedicated, even though I was exhausted, [I pumped] every two hours. So I pumped twelve times a day until my milk came in, and then we went home with eighty bags of milk! I’m a tiny person but I am a very good milk-maker! (Donor)
‘Reproductive labor’, a term coined by second-wave feminists, refers to the domestic work and childrearing that contributes to society’s national economy and reproduction (Mulford, 2012; Waring, 1988). The concept has been applied to women’s bodily labour invested in the donation of eggs and embryos for regenerative medicine (Waldby and Cooper, 2010) and to donors of other reproductive body tissues such as eggs and sperm (Almeling, 2011). The health-care cost savings as a result of breastfeeding are often promoted, but they regularly ignore the maternal labour, time and opportunity cost involved (Bartick and Reinhold, 2010; Mulford, 2012; Smith, 2007; Smith and Forrester, 2013; Smith et al., 2002). Unlike the United States, Norway values the labour of breastmilk production monetarily by including breastmilk in food production statistics. It is possible to make the work involved in providing ‘safe’ breastmilk to an HMB visible by reframing it in economic or labour terms such as ‘reproductive labour’ or ‘care work’. Such terminology attends to the reproductive labour involved in providing milk for one’s own infant, and the additional self-regulatory work milk donors enact to actively comply with milk donation standards provided by the HMB:
I’m pretty uptight, so … I keep a pretty close tab on everything. The first month I was reading the guidelines all the time, every day or two before I pumped, just to make sure that I hadn’t done anything, that I hadn’t had a cup of tea or something and not thought about it. Just to make sure that it was like a habit of ‘Okay, make sure you wash, make sure you wipe down the breast’ and all these things, until it really became a habit. Because if I was just pumping for my own baby, I wouldn’t worry about, like obviously I’d wash my hands, but I wouldn’t worry about, like, sort of wiping down the area, and all that stuff. And if my husband has the sniffles I’ll still pump for my own baby, but I don’t pump for the bank. (Donor) It’s a little bit of effort to be mindful, ‘Oh, yeah, I have a headache. Do I want to take something for it, or not? But I need to take something for it. So when can I donate again?’ You have to be a little bit more mindful, but it’s not bad. I understand why the regulations are there: because you’re dealing with little, itty-bitty, fragile babies that have no immune system, and they need … how can I say it … the purest possible milk that you can get. (Donor)
During their interviews, donors explained and sometimes demonstrated how they separated their breastmilk into differently coloured bags, or separate sections of the freezer so that it was clear which milk would be given to the HMB, and which milk would be fed to their own infant. Donors justified that the ‘purer’ milk would be donated to the HMB because it complied with HMB donation guidelines; the milk was not infused with traces of alcohol, excess caffeine, medications, herbal tea, or expressed during a time when the donor or her family were sick. When asked whether providing the ‘purer’ milk to the HMB was somewhat paradoxical, most donors reiterated that due to fragility of the NICU babies, such milk was more suitable to the sick preterm than to their own robust, healthy and community-dwelling infants:
The babies that are getting it are ones that are more fragile, more sensitive, and there needs to be limits and safeguards to really take care of those little babies. (Donor)
Clearly, milk donors’ deliberate self-regulation and compliance with donation guidelines, coupled with the material work and reproductive labour invested in pumping, labelling and storing breastmilk, are practices which both align with the discourses of risk and also contribute to the safety of DBM even before it arrives in the HMB for pasteurization and testing for the presence of pathogens.
Medical decision-making, prescription and informed consent
Despite the flawless safety track record of donor milk obtained through HMBs (Cohen, 2007), disease transmission and safety of DBM is a common concern among many American NICU clinicians (Carroll and Herrmann, 2012; Harris et al., 2005). However, in the NICUs where this research was conducted and where donor milk was commonly used, safety was largely of no concern among neonatologists who prescribe it on a daily basis (Carroll and Herrmann, 2012). The absence of pathogens and the work of the HMB had transformed milk into a highly medicalized, industrial and somewhat uniform product that reassured neonatologists and NICU parents alike:
The donor has been screened and the milk has been heat-treated and kept in sterile containers that have been analysed for safety prior to use, and then it is recorded and treated like any other medicine. In that sense it becomes like the right medication, right dose, right patient, assuming they do everything correctly. There is a mental transformation of the substance as a consequence of the process. (Neonatologist, NICU #2) They do all the testing so that makes you feel a little bit better of course. (NICU mother) I believe it’s even pasteurized, and they go to the extremes to make sure that it’s ok. (NICU mother)
This is not to say that through the medicalization and medical endorsement of donor milk, all traces of the donor’s distant presence are removed along with any microscopic pathogens. For many NICU mothers, the ‘imagined’ presence of the milk donor is keenly felt and can be perceived by some to interrupt the sanctity of the normative mother–baby dyadic feeding relationship. Moreover, the perception of DBM’s safety by the majority of NICU parents is in stark contrast to the perceived dangers of sourcing DBM from the Internet, where an ‘unknown’ and unscreened donor would provide breastmilk for the hospitalized infant:
I wouldn’t trust it. I wouldn’t even drink milk that I’d just bought from some random person that hadn’t been tested and not pasteurized, so I definitely would not let my baby drink it! (NICU mother) Oh, gosh! I would not, there’s too many crazies out there! (NICU mother) Oh! I don’t feel comfortable with that. No, I would not! (NICU mother)
The daily NICU ward round is a time where, among other aspects of care, neonatologists make infant feeding decisions, including the prescription of DBM. After assessing the baby’s status, weight, growth progress and feed tolerance, neonatologists calculate feed volume and fortification needs and examine these requirements in relation to the mother’s own breastmilk supply. Once it has been determined that an infant needs DBM due to low maternal milk supply or maternal choice not to provide breastmilk, neonatologists will initiate the use of DBM through a written feeding order or prescription. Parental consent is also necessary. During informed consent, a neonatologist will provide written information and verbal education about the screening and processing of DBM and will outline the medical reasons that have resulted in the need for DBM prescription. The neonatologist will also encourage the mother to provide the ‘gold standard’ of care, her own breastmilk.
5
A comprehensive explanation by the neonatologist of the medical reasons for and the processing of DBM can ‘make or break’ parents’ decisions to consent to the use of DBM:
The doctor discussed [donor milk] with me, they did tell me everything about it. It is pasteurized, you know … And so it made me feel a little bit more comfortable than just saying, ‘Do you want to do this or do you want to do that?’ Had I had no information behind it or anything like that, then I might have stuck with my original decision, where once she discussed the background of it and that it is pasteurized, it is going through a screening process and everything like that, it did make the decision change. (NICU mother)
DBM poses no biomedical risk to an infant, yet feeding DBM to a preterm hospitalized infant without physician prescription and parental consent would, like misappropriated breastmilk, also be considered an error in hospital practices. DBM in the United States is considered a prescribed treatment that serves as an alternative to mother’s own milk (Miracle et al., 2011). It involves the administration of food, but also a bodily fluid from another person, and therefore in most hospitals it requires informed consent. Not mentioning DBM to NICU parents as an infant feeding alternative to infant formula for their preterm infants is in violation of the ethical foundations of informed consent processes surrounding infant feeding decision-making (Miracle et al., 2011). This reveals the cultural importance of communications processes and medical prescription surrounding the safe administration of DBM. Some neonatologists recognized the significance of their role and influence and actively used it to promote DBM ahead of formula for small or particularly at-risk babies:
In a large part, my choice and my suggestion is very, very influential when the babies are very, very small. I think when everybody can look from across the room and say ‘Man, how can a baby be that small and survive?’ and when parents are really nervous about survival, then they tend to listen to the doctor more, be more concerned that there might be a problem that will take the baby’s life, and they will do whatever it takes. (Neonatologist, NICU #2) More than half the parents are receptive to it. And by us talking about it, usually if they’re kind of on the fence, if you explain the better tolerance and just again, that we’re not trying to replace their milk, it’s just a bridge, a lot of them are more receptive to it. (Neonatologist, NICU #1)
These interview extracts reveal that when education and consent narratives are comprehensive in detail, they too, like the HMB, can transform donor milk from a largely unknown and feared substance into a safe and life-giving fluid.
Food for the NICU infant has ‘multiple orders’ (Mol and Mesman, 1996); it is a series of numbers, an outcome of calculation, an instruction to act, a weight, an infusion and a composition (Mol and Mesman, 1996). Rather than being simply cast as a food source, neonatologists reposition breastmilk as akin to a medicine. This informational, communicational and affective work in support of DBM is ‘immaterial labor’ (Dyer-Witheford, 2001). Physicians’ attendance to specific terminology in critical care environments can reposition tissue donation (Miracle et al., 2011; Shaw, 2010a), and in the NICU, it is perceived by many NICU parents as critical to the legitimation and perceived safety of DBM.
Safety-constructing practices for donor milk in neonatal intensive care
This article set out to answer the following question: ‘what are the practices that enable DBM to legitimately and safely cross kinship lines in the NICU?’ Through an ethnographic approach framed by three principles of Latour’s (2004) new critique and existing STS research on safety in health care, I traced the flow of DBM from the donor to the recipient. In doing so, I have assembled an array of socio-material safety-constructing practices and proposed a more inclusive understanding of DBM’s safety. Moreover, DBM has provided a case study that demonstrates how Latour’s new critique can inform STS approaches to the study of safety in health care.
The more diverse and inclusive understanding of DBM’s safety offered in this article is timely. Current debates about the safety and legitimacy of breastmilk transactions centre on the material constituents that are present or absent in donor milk (Geraghty et al., 2013; Keim et al., 2013). Moreover, understandings about safety are dominated by the work enacted within the HMB, namely, pasteurization and microbiological testing of donated breastmilk, and donor screening and education programmes (Geraghty et al., 2013; Keim et al., 2013). Collectively, these practices minimize the risk that fragile premature infants will ingest any harmful pathogens when they are fed DBM. Consequently, the work of making DBM safe is invariably attributed solely to the work of a singular institution, albeit an important one.
Microbial agents powerfully engage us in shaping our health practices and health policies (Latour, 1998), yet what is considered clean or dirty goes beyond the presence or absence of pathogens (Douglas, 1966). Other infant feeding options, despite also harbouring risk, do not carry safety burdens comparable to those confronting the many forms of breastmilk transactions (Gribble and Hausman, 2012). For example, bovine-based artificial formula is regulated as a food by the USFDA and is monitored for its composition, manufacturing standards and quality control procedures (USFDA, 2011). However, leading authorities such as the AAP, the neonatology profession at large and NICU parents do not routinely question formula’s risk in terms of its association with feeding intolerance, bovine milk allergy and increased incidence of NEC in the preterm infant (Abdelhamid et al., 2011; Schanler et al., 2005; Sullivan et al., 2010). It is ironic, therefore, that the cultural consensus surrounding the safety of bovine-based formula (Hausman, 2011: 81) means that for preterm infants in NICU, the practice of obtaining parental consent for formula use remains outside the routine practice of consent and parental education on the safety and efficacy of DBM. 6
By focusing solely on the microbial actors, there is a risk of ignoring human actors situated within the HMB and across other institutions, who materially and discursively transform DBM into ‘liquid gold’ for use in NICUs. A more inclusive approach to the safety of donor milk draws attention to the important safety-generating ‘material labour’ of HMB staff, the ‘reproductive labour’ of milk donors and the ‘immaterial labour’ of NICU clinicians. Different but simultaneous ontologies are collectively enacted through these practices, and operate to produce different consequences (Zuiderent-Jerak et al., 2009). This ‘multiplication’ (Mol, 2002) of the safety-generating practices that legitimate breastmilk transactions in the cultural setting of neonatal intensive care is not singularly positioned. Rather, safety-generating practices can be viewed by researchers, experts on safety in health care and by NICU clinicians and parents as multiple orderings of safety that are produced across multiple spatiotemporal locales (Law and Lien, 2012). Thus, this multiplication stretches beyond the Pasteurian binaries of absence/presence, before/after, living/dead and pure/impure (Latour, 1998: 85–86), which have typically characterized pronouncements of DBM’s safety and have been solely located in the HMB. Instead, by attending to the assembly of people, practices and institutions that constitute the safety of DBM, I have attributed important safety-generating work to the practices within and beyond the walls of the home, HMB and NICU. These practices are critical to identify and recognize, particularly for the purposes of educating anxious NICU parents and clinicians who may be new to DBM, but also for informing hospital administrators and policy makers, all of whom make decisions about DBM based on notions of safety.
Footnotes
Acknowledgements
An Endeavour Fellowship (2091_2011) enabled ethnographic fieldwork to be conducted in the United States. The author would like to thank Kerry Warner, the members of the University of Technology (UTS) Communication Studies Writing Group and the three anonymous reviewers for their invaluable feedback and contributions to this publication.
Funding
This research was funded by the Australian Research Council (Discovery Grant DP110103025, Chief Investigator Katherine Carroll).