
Abstract
This study reports an evaluation of the Drink-Impaired Drivers program in the English and Welsh probation service. Participants were adult male offenders who had been convicted of a drink-driving offence and were serving community sentences. The 1-year drink-drive reconviction rates were compared for offenders who completed the program, offenders who started but did not complete the program, and a comparison group who were not allocated to the program. At 1-year follow-up, there was no reconviction among offenders who had completed the program. Multivariate analysis showed that the noncompleters had a significantly higher rate of reconviction than the completers and comparison group.
Driving under the influence of alcohol is an offence that occurs at a high frequency. In 2006, there were more than 101,000 arrests for drink-driving in England and Wales, with 92,671 convictions (Ministry of Justice, 2008a). Of the 140,361 traffic accidents in Great Britain in 2007, 6.9% (9,620) were alcohol related (Department for Transport [DfT], 2008). In the United States, a similar percentage (7%) of automobile accidents is alcohol related (National Highway Traffic Safety Administration, 2005, as cited in Moore, Harrison, Young, & Ochshorn, 2008). The human cost of drink-driving is severe: In alcohol-related traffic accidents in 2007 in Great Britain, there were 14,480 casualties, of which 460 were fatal and 1,760 resulted in serious injuries (DfT, 2008). The financial cost of alcohol-related traffic accidents in 2007 was estimated at £1,250 million (DfT, 2008).
There is much to be gained from reducing levels of drink-driving, and a range of strategies have been used to achieve this: punitive sanctions such as fines and prison sentences, alcohol ignition interlock devices, driving under the influence (DUI) courts similar to drug courts, and interventions that either address the offender’s problematic drinking or psychoeducational programs that aim to change offenders’ thinking about their drink-driving (Nochajski & Stasiewicz, 2006). The only published meta-analysis of interventions with drink-drive offenders examined 215 studies with sample sizes between 60 and 1,145 conducted between 1955 and 1992 (Wells-Parker, Bangert-Drowns, McMillen, & Williams, 1995). Educational interventions were the most common, often delivered in combination with other approaches, such as psychotherapy/counselling and probation supervision. For officially recorded DUI recidivism, there was a mean effect size of 0.19, although for better quality studies the effect size was 0.08 to 0.10, which equates to an 8% to 9% reduction in drink-driving recidivism for intervention groups. The effect size was slightly higher for medium-risk offenders than low- or high-risk offenders, although risk level was associated with the type of intervention received. Wells-Parker et al. (1995) noted that it was difficult to draw any firm conclusions about the most-effective treatment type because of the low numbers of each type of intervention combination. Nevertheless, educational interventions appeared to be most effective, particularly in combination with psychotherapy/counselling (effect size = 0.13); education alone had an effect size of 0.04, whereas probation supervision alone had an effect size of –0.01.
Since this meta-analysis, a number of studies have been published that evaluate the different approaches to DUI noted above. There is generally little support for fines and prison sentences in reducing DUI reconviction (Taxman & Piquero, 1998; Yu, 2000). Alcohol ignition interlock devices have a positive effect while on the vehicle, but this disappears once it is removed (Voas, Blackman, Tippetts, & Marques, 2002; Voas, Marques, Tippetts, & Beirness, 1999). There have been recent attempts in North America to replicate the success of drug courts (Wilson, Mitchell, & MacKenzie, 2006) by setting up “DUI courts” that combine treatment with close supervision by the courts. However, evaluations have reported little effectiveness of these courts with respect to DUI rearrests and self-reported drink-driving (Bouffard & Richardson, 2007; Bouffard, Richardson, & Franklin, 2010; MacDonald, Morral, Raymond, & Eibner, 2007; Ronan, Collins, & Rosky, 2009).
Interventions with offenders that focus on treating their alcohol use and/or take a psychoeducational approach to reduce drink-driving have shown a greater level of success in reducing DUI recidivism. As noted by Wells-Parker et al. (1995), many interventions use a combination of methods to address offenders’ alcohol use, education about drink-driving, and psychological treatments, making it difficult to disentangle exactly the approaches that are most effective. However, there are a small number of studies that report positive effects for interventions using predominately educational methods, although these studies have methodological flaws regarding control groups. Robertson, Gardner, Xu, and Costello (2009) reported that a court-mandated educational intervention with motivational enhancement for first-time DUI offenders in Mississippi, USA, had significantly lower DUI reconviction among completers (21.1%, n = 21,102) as compared with noncompleters (35.82%, n = 8,843) and nonstarters (29.46%, n = 17,937).
Another study, this time in Great Britain, reported an evaluation of a DfT Drink/Drive Rehabilitation (DDR) scheme (Smith, Buckle, Keigan, Buttress, & Stone, 2004), although again with no true comparison group. The DDR scheme allowed courts to refer drink-drivers to organizations—such as the probation service, specialist alcohol-service providers, and private companies—that provided DfT-approved rehabilitation courses. Attendance at these courses was voluntary and subject to a fee, but completion made offenders eligible for a reduction in their period of disqualification from driving. At a 2-year follow-up, 1.4% of offenders who had attended a course had been convicted of a further drink-drive offence, as compared with 3.7% of those who had not attended a course. Survival analysis also showed that time to reconviction was longer among completers. Inwood, Buckle, Keigan, and Borrill (2007) reported a 5-year follow-up of these participants, and once again, completers were significantly less likely to be reconvicted of a further drink-drive offence.
More complex interventions that combine education with other approaches such as psychosocial interventions, license sanctions, and supervision have shown the greatest effect sizes with respect to DUI recidivism (Wells-Parker et al., 1995). An early project was the Turning Point project in Ohio, USA, for chronic drink-drivers with three or more previous DUI offences and a jail sentence of 30 days or more (Langworthy & Latessa, 1993). This intervention was a 28-day, residential chemical-dependency program for offenders serving sentences for multiple DUI offences. Alcohol addiction was addressed through educational work, group and individual counselling, and attendance at Alcoholics Anonymous and/or Narcotics Anonymous. Although the admission criteria for the program were not always followed—a not unfamiliar occurrence (see Palmer et al., 2008)—those program participants who met the Turning Point criteria (n = 352) had significantly fewer new charges for an alcohol-related offence (not specifically DUI) than a comparison group (n = 193) at an average follow-up period of 13 months. Further follow-ups at 4 and 10 years (average follow-up time) corroborated these findings, with significantly lower recidivism rates for Turning Point participants for all offences, alcohol-related offences, and DUI offences (Langworthy & Latessa, 1996; Pratt, Holsinger, & Latessa, 2000).
More recently, Moore et al. (2008) reported an evaluation of community-based cognitive-therapy program in Florida, USA, for offenders with two or more DUI convictions (but without a drink problem). Using a combination of psychoeducational group work and individual counselling, this program targeted the cognitive distortions that support drink-driving. Out of 62 offenders who were court mandated to attend, 54 (87%) completed the intervention. At 21-month follow-up, 7 (12.9%) completers had been arrested for a DUI offence as compared with 6 (75.0%) of 8 noncompleters.
Lapham, Kapitula, C’de Baca, and McMillan (2006) reported an evaluation of the more complex 3-year DUI Intensive Supervision Program (DISP) for repeat drink-impaired drivers (DID) in Oregon, USA. This intervention addressed both problematic drinking and the drink-driving offence itself, with group sessions to change offenders’ thinking about drink-driving, electronic monitoring (EM), mandatory sale of vehicles, breath testing, weekly attendance at Alcoholics Anonymous (AA), polygraph tests, and supervision by a probation officer. The program participants (n = 460) and a matched comparison group (n = 497) were followed up from the date of conviction (i.e., for the intervention group, the follow-up period included their time in the intervention) for between 3 and 5 years. Lapham et al. reported that compared with the control group, the intervention group had a 48% reduction in rearrests for drink-driving offences, a 54% reduction in rearrests for driving without a license, and a 39% reduction in rearrests for other traffic offences.
One problem when evaluating multicomponent interventions is understanding exactly the components that are most effective. In a study subsequent to the one described above, Lapham, C’de Baca, Lapidus, and McMillan (2007) attempted to examine the relative effectiveness of the components of the DISP. Participants were randomly assigned to four groups: intensive supervision program with EM and forced sale of vehicles (n = 118), intensive supervision program and EM but no sale of vehicles (n = 116), intensive supervision and forced sale of vehicles but no EM (n = 118), and intensive supervision program alone (n = 120). Where EM formed part of the intervention, this lasted between 45 and 120 days depending on sentence requirements. Drink-driving reconviction data were collected at between 1 and 4 years follow-up, starting from the date at which participants entered the intervention. Hazard analysis showed that there was a short-term effect of EM, probably reflecting the shorter-term nature of this sanction, which has parallels with the short-term effect of alcohol ignition interlock devices (Voas et al., 1999, 2002). In contrast, the impact of forced vehicle sale was less clear. Because of the length of the intervention (3 years), only one third of the participants had actually completed the intervention at the point at which reconviction data were collected, and so these results should be treated with some caution.
A number of interventions for drink-driving reported in the literature had a motivational enhancement component, typically using motivational interviewing (MI). MI is a client-centred approach that aims to enhance motivation to change through the expression of empathy and development of a feeling of discrepancy between the client’s current attitudes/behavior and the behavior that is targeted for change (Miller & Rollnick, 1991). Only one study has reported a drink-driving reconviction outcome, with no significant difference in the MI group compared with a no-treatment control group among a sample of incarcerated prisoners, the majority of who were American Indian (Woodhall, Delaney, Kunitz, Westerberg, & Zhao, 2007). Other evaluations have reported more positive effects of MI compared with no treatment or standard care with a range of samples (incarcerated alcohol- or drug-using adolescents, incarcerated DUI/DWI offenders, repeat DUI offenders from the local community) and using intermediate outcomes such as level of drinking, biomarkers of alcohol abuse, and self-reported DUI behaviors (Brown et al., 2010; Stein et al., 2006; Stein & Lebeau-Craven, 2002; Woodhall et al., 2007). Therefore, although MI appears to have a positive effect on short-term behaviors, there is little evidence available to judge its long-term impact on drink-drive recidivism.
DID Program
Until recently, there was no provision in England and Wales for interventions with DUI offenders in prison or community settings. The DID program was developed to address this gap for DUI offenders serving community sentences; to date there are no interventions for those offenders in prison. Drawing on the research base, the DID program uses a combined cognitive-behavioral and educational approach, and addresses the attitudes and behavior of DID. Specifically, the program aims to improve offenders’ knowledge about alcohol and driving, to improve their planning skills and ability to generate alternatives with respect to their drink-driving behavior, and to change their attitudes that are supportive of drink-driving. The program is delivered to groups and comprises 14 sessions of 2-hr duration. In addition to direct training methods, use is also made of motivational enhancement approaches.
To date, there are no published independent evaluations of the DID program. A Home Office evaluation reported by Hollis (2007) presented reconviction data for DID-program completers, noncompleters, and nonstarters; however, there was no comparison group or examination of reconviction for the target offence of drink-driving. Therefore, the current study examines the impact of the DID program on reconviction for drink-driving offences. Reconviction rates are compared between offenders who completed the DID program, those offenders who started but did not complete the DID program, and a comparison group of offenders convicted of a drink-driving offence who were not referred to the DID program.
Method
Participants
The participants were 375 male offenders serving community sentences who had been convicted of a drink-driving offence. The age of the offenders at the time of their sentence ranged from 18 to 71, with a mean of 35.43 years (SD = 10.77), and the number of previous convictions ranged from 0 to 118, with a mean of 5.42 (SD = 8.65). Of these offenders, 144 had a requirement to attend a DID program as part of their sentence. The remaining 231 offenders formed the comparison group; they had received similar sentences without a requirement to attend an offending-behavior program as there was a limited availability of the DID program.
Offenders who did not attend the first session or who missed two sessions of the program for acceptable reasons were allowed a second attempt at the program. If they failed to complete the program at the second attempt, or they missed program sessions for unacceptable reasons, then they were sent back to court for breaching their order, although their offender manager had discretion over this decision. When an offender was breached for nonattendance at the program, this typically resulted in additional hours of unpaid work or other community sanctions being added to their sentence.
Study Design
As with previous studies evaluating program outcomes (Hollin et al., 2008; Palmer et al., 2007), it was planned to use a quasiexperimental design to compare reconviction outcome. Rather than matching the samples on key variables, it was decided to use multivariate statistics to control statistically for sample differences during analyses.
Data Collection
The data for offenders allocated to the program were gathered by a team of field researchers employed to work alongside staff in the probation areas. The comparison group was assembled from two sources: the Probation Index database, which is a national database of offenders serving community sentences, and several probation areas. The data drawn from the Probation Index and probation areas provided information on the offender’s name, gender, date of birth, index offence, date of sentence, and type of probation order.
Reconviction data for all offenders were gathered from the Offenders’ Index, a national government database that records reconvictions. These reconviction data included reconviction offence type, date of reconviction, and Offender Group Recon-viction Scale–2 score (OGRS2; Taylor, 1999). The OGRS2 is a scale that uses nine demographic and criminal-history variables to produce an estimate of an individual offender’s risk of reconviction within 2 years. It was developed by analysing patterns of convictions in a large sample of offenders serving prison and community sentences in England and Wales. Research with the OGRS2 shows a high level of predictive validity (Coid et al., 2009; Howard, Francis, Soothill, & Humphreys, 2009) and that it is comparable with other similar measures (Coid et al., 2009). OGRS2 scores can range from 0 to 100, with higher scores indicating a higher risk of reconviction. All reconviction data were collected at a 1-year follow-up. For offenders allocated to the DID program, the starting point of the follow-up period was taken from the date of the last session attended on the program, whereas for the comparison group the starting point was taken as date of sentence.
Results
Of the 144 offenders allocated to the program, 85 completed the program, giving a completion rate of 59.0%. The descriptive statistics for the two groups of offenders allocated to the DID program (i.e., completers and noncompleters) and their comparison group are shown in Table 1. Univariate analyses were performed to compare these variables across the three groups: There were significant differences between completers, noncompleters, and the comparison group for age, F(2, 372) = 6.86, p < .01, and OGRS2 score, F(2, 372) = 4.66, p < .05. Post hoc Scheffé tests were used to examine differences between the groups. These comparisons showed that the noncompleters group was significantly younger than the completers and the comparison group, and the completers group had a significantly lower risk of reconviction (as measured by OGRS2) than the noncompleters. There were no significant differences between the groups for number of previous convictions.
Descriptive Statistics for Three Groups (N = 375)
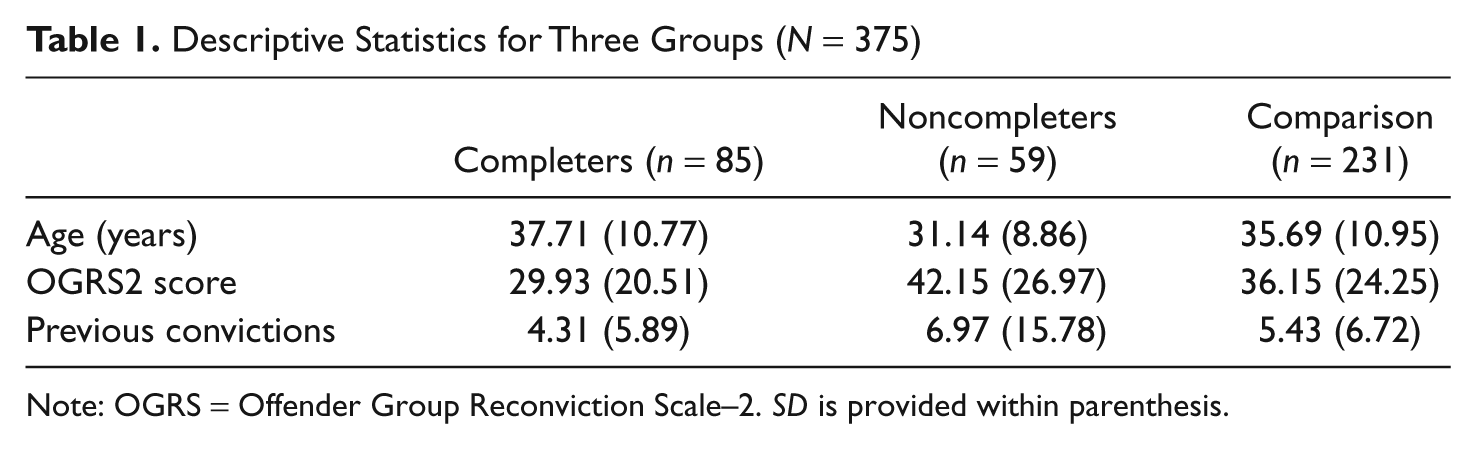
Note: OGRS = Offender Group Reconviction Scale–2. SD is provided within parenthesis.
Reconviction for Drink-Driving Offence
At 1-year follow-up, 17 (4.53%) offenders were reconvicted specifically for a drink-driving offence, with a mean time to reconviction of 159.53 days (SD = 83.29). During the follow-up period, none of the offenders in the completer groups was reconvicted as compared with 8 (13.6%) in the noncompleter group and 9 (3.9%) in the comparison group (see Table 2). An exact logistic regression was conducted to examine the impact of treatment group on drink-drive reconviction using Statistical Analysis Software Version 9.1. This technique is suitable for small numbers and sparse/empty cells (Derr, 2009). In line with previous research (Hollin et al., 2008; Palmer et al., 2007), age, OGRS2 score, and number of previous convictions were entered as control variables. Treatment group was the only significant predictor of reconviction (exact p = .008; see Table 3). It was not possible to run an exact logistic regression with all four variables in the model due to insufficient memory, 1 so after removing all the covariates using a backward stepwise procedure, further exact analyses were run to examine group differences. These post hoc analyses showed that the noncompleter group was significantly more likely to be reconvicted than the completer (p < .01, odds ration [OR] > 999 2 ) and comparison groups (p < .001; OR = 3.869). There was no difference in rate of reconviction between the completers and comparison group.
Reconviction for Drink-Driving Offence by Group (N = 375)

Note: Numbers in parentheses are column percentages.
Predictors of Reconviction for Drink-Driving Offence Using Backward Stepwise Regression
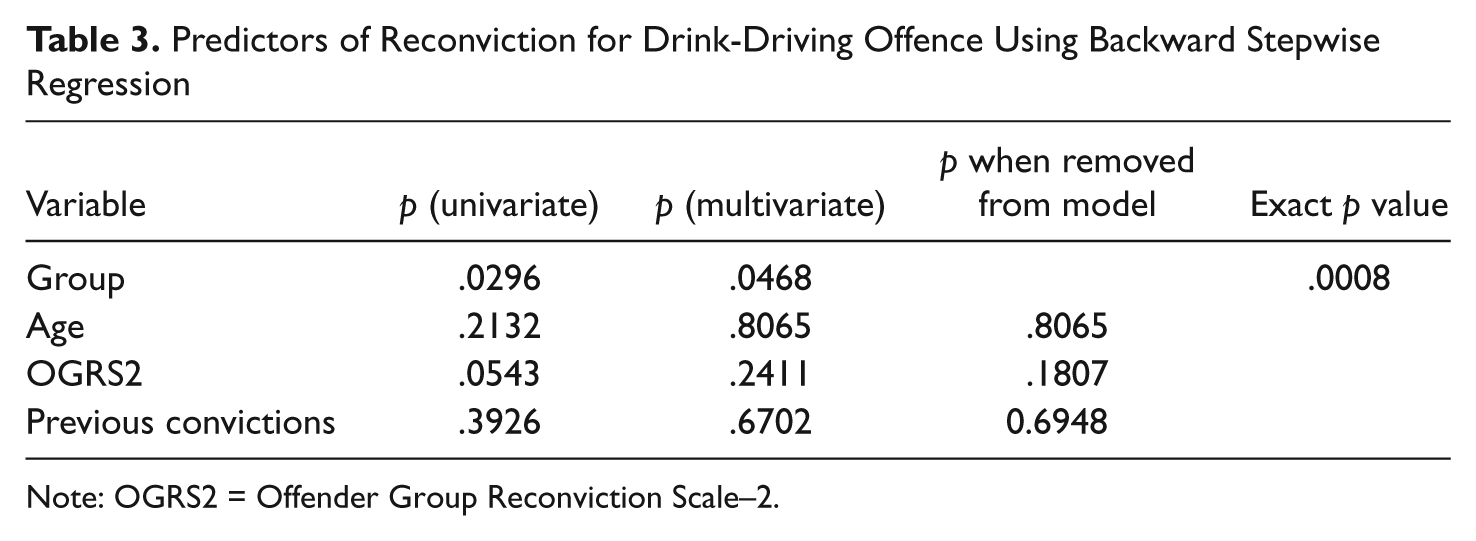
Note: OGRS2 = Offender Group Reconviction Scale–2.
Discussion
Official statistics show that nationally, 4.03% of drink-drive offenders are reconvicted of another drink-drive offence within 1 year in England and Wales (Ministry of Justice, 2008b). At 4.53%, the rate of drink-drive reconvictions for all offenders in the sample is in line with these statistics. Among offenders who completed the DID program, there was zero reconviction at a 1-year follow-up; however, the reconviction rate for completers was not significantly different to that of the comparison group. This finding is in contrast to other evaluations of drink-drive interventions, in which program completers have had significantly lower rates of drink-drive reoffending than control groups (Inwood et al., 2007; Lapham et al., 2006; Pratt et al., 2000). This discrepancy may be due to a floor effect in the data as seen with the very low rate of reconviction at follow-up for all offenders. This study had a shorter follow-up period than other studies—the three studies cited above had follow-up periods of 3 or more years—and it may be that a longer follow-up period would yield different results. The Lapham et al. (2006) and Pratt et al. (2000) studies were also conducted with samples of more serious drink-drive offenders, as evidenced by the length and setting of these interventions.
The program noncompleters had the highest level of drink-drive reconvictions (13.9%) and were significantly more likely to be reconvicted than the completer and comparison groups. This finding is in keeping with the results reported by Robertson et al. (2009) and Moore et al. (2008) in their evaluations of interventions for drink-drivers. A similar adverse “noncompletion effect” has also been reported in evaluation of other cognitive-behavioral programs addressing general offending behavior (e.g., Hollin et al., 2008; Palmer et al., 2007; Van Voorhis, Spruance, Ritchey, Listwan, & Seabrook, 2004). The evidence suggests that noncompleters are typically younger, have a higher risk of reconviction, have more previous convictions, and are more likely to have few academic qualifications. A similar pattern was found here, with noncompleters being younger and at higher risk of reconviction than the completers group. There are various explanations for why noncompleters do worse, ranging through levels of motivation (Debidin & Lovbakke, 2005), study design (Hollin, 2008), and that the predictors of noncompletion are similar to those for reconviction, hence, the close relationship between the two (Wormith & Olver, 2002).
The DID completion rate of 51% was lower than that reported in other court-mandated interventions with drink-drivers. Two studies in the Unites States reported completion rates of above 85% (Moore et al., 2008; Nochajski, Miller, Wieczorek, & Whitney, 1993), whereas a Canadian study by Rootman et al. (2005) showed a completion rate of 97.3%. However, the completion rate for the DID program was higher than that found in other offending-behavior programs run in the community in England and Wales. Two evaluations of cognitive-skills programs for general offender groups being delivered at the same time as the data in the current study were collected and reported completion rates of around 30% (Hollin et al., 2008; Palmer et al., 2007), although recent data suggests completion rates have improved across all programs National Offender Management Services Interventions and Substance Abuse Unit [NOMS ISAU], 2007. As all the programs are offered by the same national organization, it seems plausible that the higher completion rate for the DID program may be explained by the characteristics of drink-drive offenders. Thus, compared with offenders allocated to general offender programs (Hollin et al., 2008; Palmer et al., 2007), the drink-drive offenders allocated to the DID program were about 8 years older, had one half the risk of reconviction, and one half the number of previous convictions. Rootman et al. reported similar predictors of noncompletion of drink-drive programs, also noting that noncompleters drank more frequently than completers. Furthermore, in keeping with the literature (Inwood et al., 2007; Nochajski et al., 1993), the DID-program completers were older, had lower risk, and had fewer previous convictions than both the noncompleters and controls.
Although this study reports the first evaluation of the DID program, it is not without its limitations. The overall sample size is reasonable; however, once the intervention group is split into completers and noncompleters, the cell numbers decrease. As with other offence-specific interventions (e.g., Hatcher et al., 2008), the number of offenders eligible for the DID program was lower than for the general offending-behavior programs. However, the size of the sample in the current study compares favourably with other evaluations of drink-drive programs and is unlikely to mask a program effect (see Moore et al., 2008; Nochajski et al., 1993). With such a low base rate of reconviction for drunk-driving offences, using reconviction as an outcome may not have been sensitive enough a measure. An alternative outcome, such as rearrest data, may have provided a more meaningful comparison. A further limitation is the lack of randomization and potential pretreatment differences between groups on variables that data were not available for and so could not be controlled for in the analyses.
Although this study does not provide evidence that completing the DID program reduces drink-drive reconvictions, it supports previous research in highlighting worse reconviction outcomes for noncompleters. Given the low base rate of reconviction for drink-driving (Ministry of Justice, 2008b), it can be argued that the targeting strategy for the DID program is working against itself: Those who complete the DID program are—as judged by their age, risk level, and previous convictions—at a very low risk of reconviction. It is also the case that, as a group, DUI offenders sentenced to community disposals are likely to be low-risk offenders, with more serious offenders receiving prison sentences. As Wells-Parker et al. (1995) have pointed out specifically for drink-drivers, program effects are diminished with low-risk offenders. In this light, the outcome from the DID effect is an excellent example of the risk principle, that is, the level of service delivery should be commensurate with the offender’s level of risk (Andrews & Dowden, 2006).
Given this analysis of the current findings, there are several recommendations that can be made. First, the program-allocation criteria should be reconsidered to eliminate very low-risk offenders and to emphasise the factors associated with noncompletion and higher rates of reconviction. Indeed, it may well be that the low risk of reconviction among DUI offenders in the community is such that, in line with the risk principle, resources would be spent better elsewhere with other groups of higher risk offenders. Second, a reduction in rates of dropout may be beneficial in reducing reconvictions among the higher risk offenders. Various techniques can be employed to increase the likelihood of an offender completing a program, including preparatory work before commencing a program and the use of techniques such as MI to enhance engagement in treatment both before and during the course of a program (Miller & Rollnick, 1991; Serin, Kennedy, Mailloux, & Hanby, 2010). Third, several similar programs in other jurisdictions explicitly target the offender’s drinking (Langworthy & Latessa, 1993; Lapham et al., 2006), and there may be gains in similarly addressing this factor with a higher risk group of offenders.
Footnotes
Acknowledgements
The authors would like to thank Dr. John Bankart of the University of Leicester, United Kingdom, for his expert advice on the multivariate statistics, and Rebecca Daw and Maxine Richards for assistance with data collection.
Any views or opinions expressed within this article are those of the authors and not that of the Home Office.
The author(s) declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) disclosed that they received the following support for their research and/or authorship of this article: This study was supported by a grant from the Research Development and Statistics Directorate of the Home Office, United Kingdom.