
Abstract
This study examined two theoretical models on the interaction between psychopathy, traumatic exposure, and lifetime posttraumatic stress in a sample of 81 male detainees. In Model 1, the interpersonal and affective features of psychopathy were assumed to protect against posttraumatic stress. In Model 2, the lifestyle and antisocial traits of psychopathy were assumed to lead to a lifestyle that increases the risk of traumatic exposure and subsequent posttraumatic stress. The authors found significant negative bivariate associations between Psychopathy Checklist–Revised (PCL-R) total, Interpersonal and Affective facet scores, and posttraumatic stress. Model 1 was confirmed, as they found the interaction between the Affective facet and traumatic exposure had a significant negative effect on posttraumatic stress. Model 2 was rejected. The authors’ findings confirm that the interpersonal and affective features of psychopathy are associated with an emotional deficit and that the affective features of psychopathy are crucial for understanding the relationship between psychopathy and anxiety.
Psychopathy is a severe personality disorder that consists of interpersonal, affective, and behavioral features. On the interpersonal level, psychopaths are grandiose, arrogant, callous, dominant, superficial, and manipulative. Affectively, they are short tempered, unable to form strong emotional bonds with others, and lacking in guilt or anxiety. These interpersonal and affective features are associated with a socially deviant lifestyle characterised by irresponsible, impulsive, and rule-breaking behavior and a tendency to ignore or violate social conventions and mores (Cleckley, 1976; Hare, 2003, 2006; Hare & Neumann, 2005, 2008). The predominant instrument to assess this personality disorder is the Hare Psychopathy Checklist–Revised (PCL-R; Hare, 2003). Although the PCL-R has engendered a tremendous body of empirical research in the past, it has recently been argued that more theory-driven research is needed for the advancement of clinical psychology in general (Strauss & Smith, 2009) and our understanding of the psychopathy construct in particular (Skeem & Cooke, 2010). Our study adopted a theoretically driven approach to what has been identified as one of the key questions in the field of psychopathy, notably the relationship between psychopathy and anxiety (Hare & Neumann, 2008; Lilienfeld, 1994; Patrick, 2006; Skeem & Cooke, 2010). The aim of this study was to investigate the association between psychopathy, as defined by Hare (2003), and a specific form of anxiety, notably posttraumatic stress, by testing two theoretical models on the relationship between traumatic exposure, posttraumatic stress, and psychopathy.
Posttraumatic stress disorder (PTSD) is an anxiety disorder that potentially develops after exposure to an event in which the individual experienced, witnessed, or was confronted with either actual or threatened loss of life or serious injury invoking a response of fear, helplessness, or horror. According to the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association [APA], 1994), the diagnosis of PTSD requires that three clusters of symptoms (reexperiencing the traumatic event, numbing of affect and avoidance of trauma-related stimuli, and hyperarousal) are present for at least 1 month, causing significant distress or impairment (APA, 2000). However, there is considerable evidence that many individuals in reaction to a traumatic event display some symptoms of posttraumatic stress, without developing full PTSD (Helzer, Robins, & McEvoy, 1987; Stein, Walker, Hazen, & Forde, 1997). Such subthreshold posttraumatic stress is clinically relevant, as it appears to be associated with significant and long-standing impairment (Cukor, Wyka, Jayasinghe, & Difede, 2010). PTSD has been shown to be more prevalent in a sentenced prison population than in the general population, with different studies finding sentenced prison population–prevalence rates between 4% and 21% (Goff, Rose, Rose, & Purves, 2007). This high prevalence rate is not surprising, as prisoners appear to be exposed to more traumatic events during childhood and/or adulthood than individuals in the general population (Jordan, Schlenger, Fairbank, & Caddell, 1996; Urbaniok, Endrass, Noll, Vetter, & Rossegger, 2007; Weeks & Widom, 1998). Prison and general populations do not show differences in terms of the types of life events considered to be traumatic (Collins & Bailey, 1990; Gibson et al., 1999). However, there is emerging evidence for a traumatic event that is specific to offender populations, notably the commission of a violent crime. Some studies suggest that PTSD can directly arise from the commission of a violent or sexual offence, at least in forensic psychiatric patients (Gray et al., 2003; Papanastassiou, Waldron, Boyle, & Chesterman, 2004; Pham, 2012). However, the notion of offence-related PTSD remains equivocal regarding offenders in a general prison population (Payne, Watt, Rogers, & McMurran, 2008).
In the research literature, psychopathy has been linked in different ways to anxiety in general and to posttraumatic stress in particular, because psychopathy is a multifaceted concept. Hare (1991) originally proposed a two-factor model for the PCL-R, in which the core personality traits (“selfish, callous, and remorseless use of others”) and the behavioral features of psychopathy (“chronically unstable, antisocial, and socially deviant lifestyle”) are distinguished. There is considerable evidence that these two factors are differentially related to indications of internalising psychopathology. The personality factor is associated with lower anxiety (Blonigen et al., 2010; Harpur, Hare, & Hakstian, 1989; Hicks & Patrick, 2006) and greater psychological well-being (Verona, Patrick, & Joiner, 2001), whereas the behavioral factor is associated with higher anxiety (Blonigen et al., 2010; Hicks & Patrick, 2006) and risk of suicide (Verona et al., 2001). Later factor-analytical studies on the PCL-R (Cooke & Michie, 2001; Hare, 2003; Hare & Neumann, 2005) concur that the personality factor can be broken down into two facets: an Interpersonal and an Affective facet. Furthermore, there is general agreement that the behavioral factor also consists of two components—a Lifestyle and an Antisocial facet—although some authors (Cooke & Michie, 2001; Skeem & Cooke, 2010) have argued that the Antisocial facet should not be included in the PCL-R, as it is associated too strongly with criminal behavior.
One line of research posits a negative association between the interpersonal and affective personality features of psychopathy and posttraumatic stress. Proponents of this reasoning build on the proposition that psychopathy is marked by a lack of anxiety and/or fear (Cleckley, 1976; Lykken, 1995). In his seminal work The Mask of Sanity (1976), Cleckley stated that psychopathy is characterised by a fundamental emotional deficit, making it impossible to experience serious and deeply moving emotional states, and anxiety in particular. Some argue that this fundamental emotional deficit prevents the psychopathic individual from developing posttraumatic stress. Some of the factors advanced by cognitive and behavioral theories on the psychogenesis of PTSD are fear conditioning (neutral stimuli present during the traumatic event acquire fear-eliciting properties through association with the traumatic event), avoidance behavior (avoidance of conditioned stimuli prevents extinction of the association with the traumatic event; Keane, Zimering, & Caddell, 1985; Mowrer, 1960), and attentional bias (attention is abnormally sensitive to threat-related stimuli; Foa & Riggs, 1993). Indeed, evidence suggests that when exposed to reminders of traumatic events, trauma-exposed participants with PTSD exhibit greater physiological responses than trauma-exposed participants without PTSD (Blanchard, Hickling, Taylor, Loos, & Gerardi, 1994). Furthermore, individuals with PTSD develop stronger and more resistant conditioned physiological responses to aversive stimuli that are not related to the traumatic event than trauma-exposed individuals without PTSD (Orr et al., 2000). Finally, individuals with PTSD are more easily distracted by emotional cues when performing an experimental task (Bar-Haim, Lamy, Pergamin, Bakermans-Kranenburg, & van Ijzendoorn, 2007). However, psychopathy is associated with more difficulty in acquiring conditioned physiological fear responses (Birbaumer et al., 2005; Hare & Quinn, 1971; Lykken, 1957), less ability to learn to avoid responding to specific stimuli that lead to punishment (Blair et al., 2004; Lykken, 1957; Newman & Schmitt, 1998), and less distraction by emotional stimuli during experimental tasks (Christianson et al., 1996; Michell, Richell, Leonard, & Blair, 2006). These studies suggest that the psychophysiological functioning of highly psychopathic individuals and individuals with PTSD is exactly the inverse. Moreover, recent theoretical models have linked both the emotional deficit of psychopathy (Daversa, 2010; Fowles & Dindo, 2006; Patrick, 2007) and the psychogenesis of PTSD (Rauch, Shin, & Phelps, 2006) to a neurobiological deficit at the level of the amygdale. Psychopathy is associated with a hyporeactive amygdale, resulting in lower performance on functions that are known to recruit the amygdale, such as aversive conditioning and avoidance learning. However, PTSD is associated with a hyperreactive amygdale, making individuals more susceptible to fear conditioning, and thus more likely to develop posttraumatic stress symptoms after a traumatic event. Based on this line of reasoning, Blair and Mitchell (2009) conclude that psychopathy is in some functional respects the inverse of PTSD. Accordingly, we posit a first model in which the interpersonal and affective features of psychopathy are negatively associated with posttraumatic stress because these personality features protect individuals from the impact of traumatic exposure: As psychopathic individuals are less likely to develop conditioned fear, to avoid unpleasant stimuli, and to focus on threat stimuli, the impact of traumatic exposure may be less significant for them than nonpsychopathic individuals. This model is represented graphically in Figure 1.

Model 1: The interpersonal and affective traits of psychopathy as protector against posttraumatic stress
To our knowledge, this model has never been tested in scientific literature, although four studies have reported on the association between psychopathy and posttraumatic stress. Moeller and Hell (2003) studied a sample of 102 inmates and did not find a single case of PTSD in a group of psychopaths (defined as a score > 25 on the PCL-R), although PTSD could be diagnosed in a small proportion of the nonpsychopathic group. Similarly, Pham (2012) found a strong negative association between the PCL-R scores (in particular the affective features of psychopathy) and acute stress following a traumatic experience in forensic psychiatric patients. However, Blackburn, Logan, Donnelly, and Renwick (2003) found a significantly higher prevalence of PTSD in psychopaths (defined as a score > 25 on the PCL-R) in their sample of forensic psychiatric patients, and Kubak and Salekin (2009) found a significant positive association between ratings on the Psychopathy Checklist–Youth Version (Forth, Kosson, & Hare, 2003) and symptoms of PTSD in child and adolescent offenders.
A second line of research advances that the lifestyle and antisocial features of psychopathy are positively related to posttraumatic stress. According to this model, the impulsive and antisocial traits of psychopathy lead to a lifestyle that increases the risk of encountering stressful life events (e.g., a serious accident, being a victim of violence, incarceration, etc.; Frick, Lilienfeld, Ellis, Loney, & Silverthorn, 1999). The positive association between psychopathy and posttraumatic stress might therefore be explained by increased traumatic exposure. This model is represented graphically in Figure 2.

Model 2: The lifestyle and antisocial traits of psychopathy increase traumatic exposure and subsequent posttraumatic stress
The complete model as represented in Figure 2 has, as far as we know, never been tested. However, there has been previous research on the separate paths in this model. Indeed, some researchers have found a positive association between psychopathy and increased traumatic exposure (Dembo et al., 2007; Moeller & Hell, 2003; however not by Pham, 2012). Individuals from the general population with a history of behavioral problems before the age of 15 were more likely to have been beaten or mugged during the past 18 months and more likely to have seen combat if they served in Vietnam than those who reported little or no history of delinquency (Helzer et al., 1987), and childhood conduct disorder has also been shown to predict traumatic exposure (Koenen et al., 2002). Furthermore, a number of researches have established the positive association between criminal behavior, antisocial personality disorder, substance abuse, and PTSD, especially in men (Helzer et al., 1987; O’Toole, Marshall, Schureck, & Dobson, 1998; Sareen, Stein, Cox, & Hassard, 2004; Sierles, Chen, Messing, Besyner, & Taylor, 1986). This link has been established in community samples but scarcely in samples of incarcerated men (Gibson et al., 1999).
This study contributes to the literature on three points. First, we focused exclusively on traumatic exposure during adulthood. Most previous research does not distinguish between traumatic exposure during childhood or adolescence and traumatic exposure during adulthood, although their association to psychopathy is conceptually different. Some theoretical and empirical studies have suggested that early traumatic exposure plays a role in the aetiology of psychopathy, as it might alter the neurobiology of the brain and contribute to the core affective deficit of psychopathy (Daversa, 2010; Farrington, 2006; Lang, af Klinteberg, & Alm, 2002; Marshall & Cooke, 1999; Poythress, Skeem, & Lilienfeld, 2006; Weiler & Widom, 1996). However, in this study, we did not address the question of the aetiology of psychopathy but rather focused on the association between psychopathy and posttraumatic stress during adulthood. Although we acknowledge that early traumatic experiences might further complicate the precise relationship between psychopathy and posttraumatic stress, we preferred to test two clear-cut theoretical models. Our second contribution to the literature lies in the fact that the two models outlined above have never been tested before. By testing theoretical models instead of bivariate associations, this study responds to the recent call from more theory-driven research in the field of psychopathy (Skeem & Cooke, 2010). Third, we examine the association between psychopathy and posttraumatic stress on a more detailed level. All previously mentioned studies—except Pham (2012)—only provide information on the association between the PCL-R total scores and the categorical diagnosis of PTSD. We include the four facets of the PCL-R (Interpersonal, Affective, Lifestyle, and Antisocial) in our analyses (Hare & Neumann, 2005), and we consider posttraumatic stress as a dimensional variable by focussing on symptoms of posttraumatic stress rather than on categorical diagnoses of PTSD. In that way, we include clinically relevant levels of subthreshold posttraumatic stress in our analyses, and we avoid losing information by dichotomising a continuous variable.
Method
Participants
Participants were 81 male inmates recruited from the population of two prisons in Flanders (Belgium). The following inclusion criteria were applied: conventional competency in Dutch, no psychotic symptoms, not being on remand, and being declared fully responsible for one’s actions. Of the sample, 27% were convicted for (attempted) manslaughter or murder, 25% for a violent crime (robbery, assault, or battery), 41% for a sexual crime (indecent assault or rape of a minor or adult), and 7% for other crimes (drugs, fraud, or burglary). Inmates participated on a voluntary basis after supplying written informed consent. No incentive was given. The racial and ethnic composition of the sample was 84% White, 14% North Africans, and 2% other. The mean age of the sample at the time of the interview was 39.8 years (SD = 12.17, range = 20-73 years).
Instruments
Psychopathy
Psychopathy was assessed via ratings on the PCL-R (Hare, 2003). Ratings were based on information gathered from a semistructured clinical interview and review of file information. The interviewer was a clinical psychologist (first author) who received training in administering and scoring the PCL-R. To check the interrater reliability, PCL-R ratings made by clinical psychologists working in the prisons were made available to the authors. In that way, we obtained independent PCL-R ratings for 42% of the participants. Interrater reliability as determined by the intraclass correlation coefficient (absolute agreement) for a single rating, using a two-way random effects model, was .79 for the Interpersonal/Affective factor, .76 for the Lifestyle/Antisocial factor, and .82 for the PCL-R total score. Cronbach’s alpha as an index of internal consistency was good for the Interpersonal facet (.82), the Affective facet (.77), the Lifestyle facet (.78), the Antisocial facet (.69), and the total PCL-R scale (.83). The mean PCL-R total score in our sample was 22.9 (SD = 8.51, range = 1-36); 32% of the sample scored below 20 on the PCL-R, and 28% of the sample scored equal to or above the cutoff of 30. We tested mean differences on PCL-R scores as a function of the index offence and racial/ethnic origin. We found that the Lifestyle and Antisocial facets differed significantly as a function of index offence, Welch F(3, 22.75) = 4.99, p < .01 and Welch F(3, 17.05) = 9.08, p < .05, respectively. Post hoc analyses using the Games–Howell test indicated that the average score on the Lifestyle facet was significantly higher in detainees who were convicted for a violent crime (M = 7.87, SD = 1.27) than those who were convicted for a sexual crime (M = 5.94, SD = 3.40) or homicide (M = 5.60, SD = 3.14), and the average score on the Antisocial facet was significantly higher in detainees who were convicted for a violent crime (M = 7.13, SD = 1.63) than those who were convicted for a sexual crime (M = 4.04, SD = 2.78) or homicide (M = 4.74, SD = 3.27). No significant mean differences between PCL-R scores were found as a function of racial/ethnic origin. We also calculated Pearson correlations between age and PCL-R scores and found a significant negative correlation for the Lifestyle facet (r = −.40, p < .01) and the Antisocial facet (r = −.47, p < .01).
Lifetime symptoms of posttraumatic stress
The participants were interviewed regarding symptoms of reexperiencing, avoidance, and hyperarousal using the Structured Clinical Interview for DSM-IV-R Axis 1 Disorders (SCID-I). The presence of reexperiencing, avoidance, and hyperarousal symptoms was scored on a three-point scale from 0 (absent) to 1 (uncertain) to 2 (present). A Posttraumatic Stress Scale was calculated by adding up the scores on all 17 symptoms. This resulted in a scale with a mean of 3.6 (SD = 7.10, range = 0-23, skewness = 1.73 with SE = 0.27, and kurtosis = 1.48 with SE = 0.53) and that showed good internal consistency (Cronbach’s α = .94). Six of the 81 participants (7%) had a lifetime categorical diagnosis of PTSD.
Audiotapes of the SCID-I interviews were independently rated by a student with a bachelor’s degree in clinical psychology. For 46% of the sample, dual SCID-I ratings were made by the student. Interrater reliability of the individual symptoms as determined by the kappa coefficient ranged from .58 for the symptom “markedly diminished interest or participation in significant activities” to 1.00 for the symptoms “efforts to avoid thoughts, feelings, or conversations associated with the trauma,” “irritability or outbursts of anger,” and “hypervigilance.” The intraclass correlation coefficient (absolute agreement) was .96 for the Posttraumatic Stress Scale.
Traumatic exposure during adulthood
The first question of the section on PTSD in the SCID-I contains a list of critical incidents that one might have experienced or been aware that a loved one had experienced. In response to this question, the participants recited all the potentially traumatic events they had encountered during their lives. We only counted responses that were in accordance with the A1 criterion and that occurred after the age of 18. The responses could be classified into five categories: the index offence (violent or sexual offence; reported by 21% of the sample), accidents (traffic accident, fire, near drowning, climbing accident; reported by 9.9% of the sample), being a victim of aggression (being attacked or threatened; reported by 7.4% of the sample), witnessing the death or wounding of someone (witnessed murder, death, or dead body or saw person seriously hurt, see atrocities; reported by 13.6% of the sample), and serious illness or sudden death of relative (serious illness or death of child, unexpected death of family member or close friend; reported by 32.1% of the sample). A frequency score for traumatic exposure was calculated by totalling all potentially traumatic events reported. In our sample, 62% of the participants had experienced at least one potentially traumatic event in accordance with the A1 criterion, and the mean frequency score was 1.2 (SD = 1.83, range = 0-10, skewness = 3.15 with SE = 0.27, and kurtosis = 12.11 with SE = 0.53). A versatility score for traumatic exposure was calculated by adding the number of above-mentioned categories of traumatic events that were reported by participants. The mean versatility score was 0.84 (SD = 0.80, range = 0-3, skewness = 0.60 with SE = 0.27, and kurtosis = −0.31 with SE = 0.53).
Statistical Analysis
First, we calculated bivariate associations between the PCL-R scores, frequency, and versatility of traumatic exposure and posttraumatic stress. As posttraumatic stress are count data (number of symptoms) with overdispersion (the variance is greater than the mean), we used bivariate negative binomial regression analyses in which posttraumatic stress is regressed onto frequency of traumatic exposure, versatility of traumatic exposure, and the PCL-R total and facet scores separately (Coxe, West, & Aiken, 2009). We also tested the bivariate associations between frequency of traumatic exposure, versatility of traumatic exposure, and the PCL-R total and facet scores. Next, we tested the two models. The first model was tested as a moderator analysis. First, traumatic exposure (predictor) and the Interpersonal/Affective facets of the PCL-R (moderators) were entered in a multivariate negative binomial regression model with posttraumatic stress (outcome). Next, we entered the product of predictor and moderator and checked whether the moderator effect was significant. The second model was tested through a mediation analysis. First we tested whether there is a positive association between the Lifestyle and Antisocial facets of the PCL-R (predictors) and posttraumatic stress (outcome). If this were the case, we would then test whether this positive association could be explained by traumatic exposure (mediator). Significant moderator and/or mediator effects were further tested as recommended by Holmbeck (2002). We followed the recommendations made by Frazier, Tix, and Barron (2004) for conducting moderator and mediator analyses.
Results
The bivariate associations between PCL-R scores, frequency of traumatic exposure, versatility of traumatic exposure, and posttraumatic stress symptoms are reported in Table 1. There was a significant positive association between versatility of traumatic exposure and posttraumatic stress but not between frequency of traumatic exposure and posttraumatic stress. For each unit increase on the versatility of traumatic exposure scale (i.e., for each additional type of traumatic event reported), the number of posttraumatic symptoms increases with a factor of 1.46, exp(.377). There was a significant negative association between PCL-R total scores and posttraumatic stress. For each unit increase on the PCL-R total scale, the number of posttraumatic symptoms decreases with a factor of 0.97, exp(−.026). At the level of the facets of psychopathy, we see a significant negative association between the Interpersonal and the Affective facets and posttraumatic stress. For each unit increase on these facet scales, the number of posttraumatic symptoms decreases with a factor of 0.87, exp(−.142) and 0.88, exp(−.125), respectively. The Lifestyle and Antisocial facet were not significantly associated with posttraumatic stress. PCL-R total and facet scores were not related to frequency of traumatic exposure and versatility of traumatic exposure.
Bivariate Associations Between PCL-R Scores, Frequency of Traumatic Exposure, Versatility of Traumatic Exposure, and Posttraumatic Stress
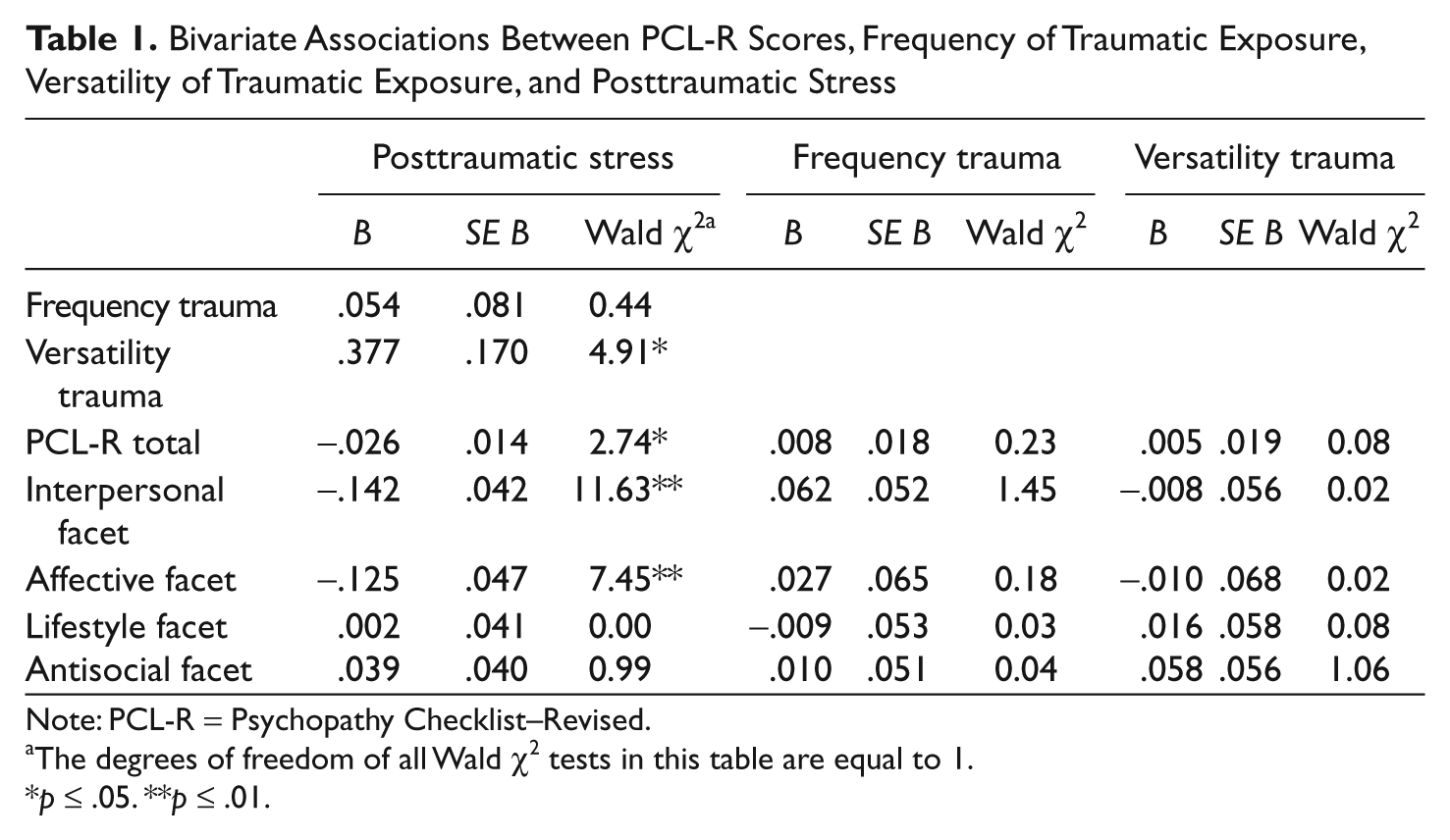
Note: PCL-R = Psychopathy Checklist–Revised.
The degrees of freedom of all Wald χ2 tests in this table are equal to 1.
p ≤ .05. **p ≤ .01.
We then proceeded to test the two models on the association between traumatic exposure, psychopathy, and posttraumatic stress. The first model stipulates that the interpersonal and affective traits of psychopathy function as protective factors against the development of posttraumatic stress. This means that the Interpersonal and Affective facets of psychopathy negatively moderate the association between traumatic exposure and the subsequent development of posttraumatic symptoms. As we previously found a significant positive association between versatility of traumatic exposure and posttraumatic stress, but not frequency of traumatic exposure, we use versatility of traumatic exposure as the predictor variable. The results from two negative binomial regression analyses are reported in Table 2.
Testing the Moderator Effects of Model 1 Using Negative Binomial Regression
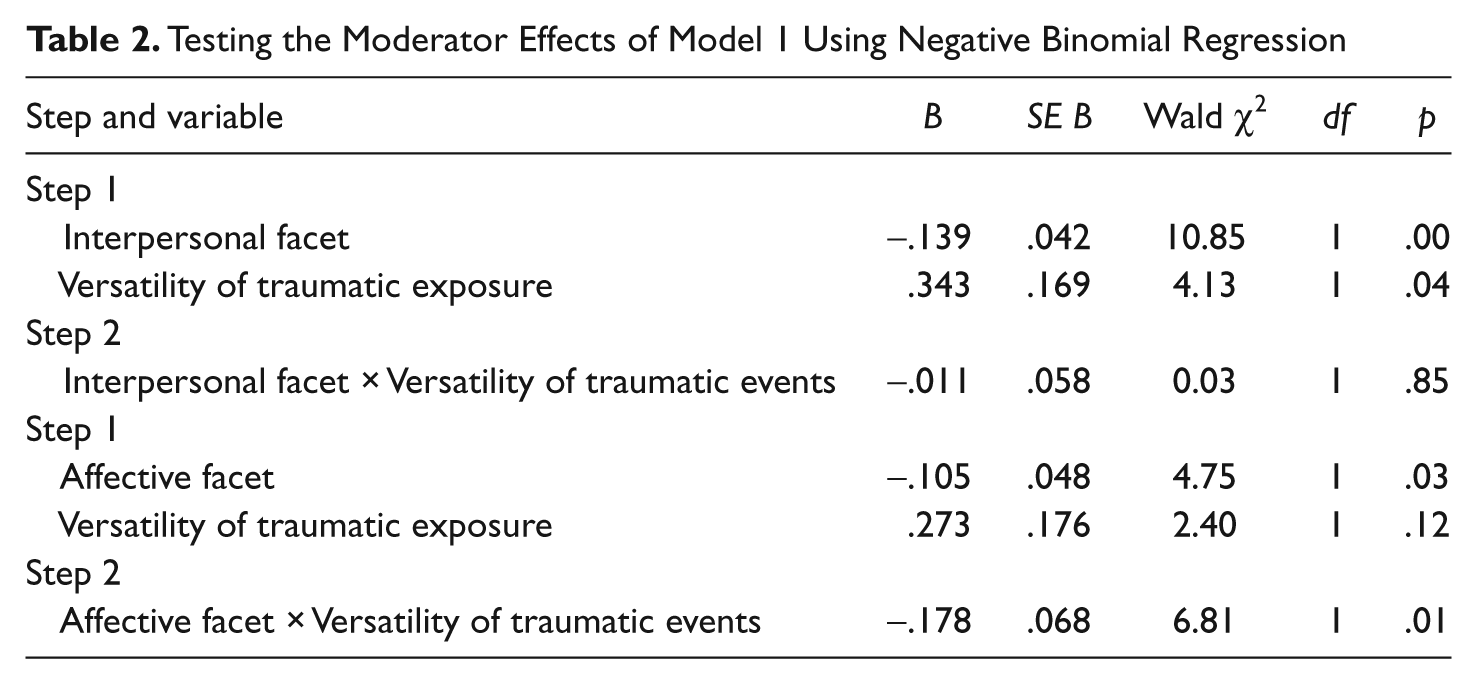
For the model with the Interpersonal facet and versatility of traumatic exposure, we found in Step 1 that both the predictor and the moderator had a significant main effect on posttraumatic stress. For each unit increase on the Interpersonal facet scale, the number of posttraumatic symptoms decreases with a factor of 0.87, exp(−.139), whereas for each unit increase on the Versatility of Traumatic Exposure scale, the number of posttraumatic symptoms increases with a factor of 1.41, exp(.343). This result parallels the bivariate associations found earlier. When the product term of the Interpersonal facet and versatility of traumatic exposure was entered in the model in Step 2, this interaction term appeared to have no significant effect on posttraumatic stress. So no evidence was found for an interaction effect. Similar analysis was done for the Affective facet. Step 1 resulted in a model whereby the Affective facet has a significantly negative main effect on posttraumatic stress. This means that for each unit increase on the Affective facet scale, the number of posttraumatic symptoms decreases with a factor of 0.90, exp(−.105). In this model, the versatility of traumatic events had no significant effect on posttraumatic stress. Step 2 resulted in a model that shows the interaction term has a significant negative effect on posttraumatic stress. Negative binomial regression does not allow for a direct comparison between nested models (i.e., the regression models with and without the interaction term) and does not allow for the calculation of a R2 statistic as index for the variance explained in the outcome variable by predictor, mediator, and interaction term (Coxe et al., 2009). However, the significant negative effect of the interaction term is evidence for the moderating effect of the Affective facet on the relationship between versatility of traumatic exposure and posttraumatic stress.
Following the procedure described by Holmbeck (2002), we conducted two post hoc regression analyses to probe this moderator effect. Prior to these analyses, we computed two conditional moderator variables by adding one standard deviation to the centered Affective facet (low Affective facet) and by subtracting one standard deviation from the centered Affective facet (high Affective facet). With these conditional variables, we conducted two negative binomial regression analyses, each of which included the main effect for versatility of traumatic exposure, the main effect for one conditional moderator variable, and the interaction effect of these two variables. The results of the regression analysis with low Affective facet as a conditional moderator indicated that there was a significant positive association between the degree of posttraumatic stress and versatility of traumatic exposure (B = .693, SE B = .243, p < .01); the results of the regression analysis with high Affective facet as a conditional moderator indicated that the degree of posttraumatic stress was not significantly associated with versatility of traumatic exposure (B = −.168, SE B = .237, p > .05). Regression lines depicting the relationship between versatility of traumatic exposure and posttraumatic stress as moderated by the Affective facet are plotted in Figure 3. These results demonstrate that at higher levels of the Affective facet, the impact of versatility of traumatic exposure on posttraumatic stress is mitigated.

Regression lines for relationships between versatility of traumatic exposure and posttraumatic stress as moderated by the PCL-R affective facet
The second model postulates that a positive association between the Lifestyle and Antisocial facets of the PCL-R and posttraumatic stress could be explained by the increased traumatic exposure in individuals with an impulsive-irresponsible and antisocial lifestyle.
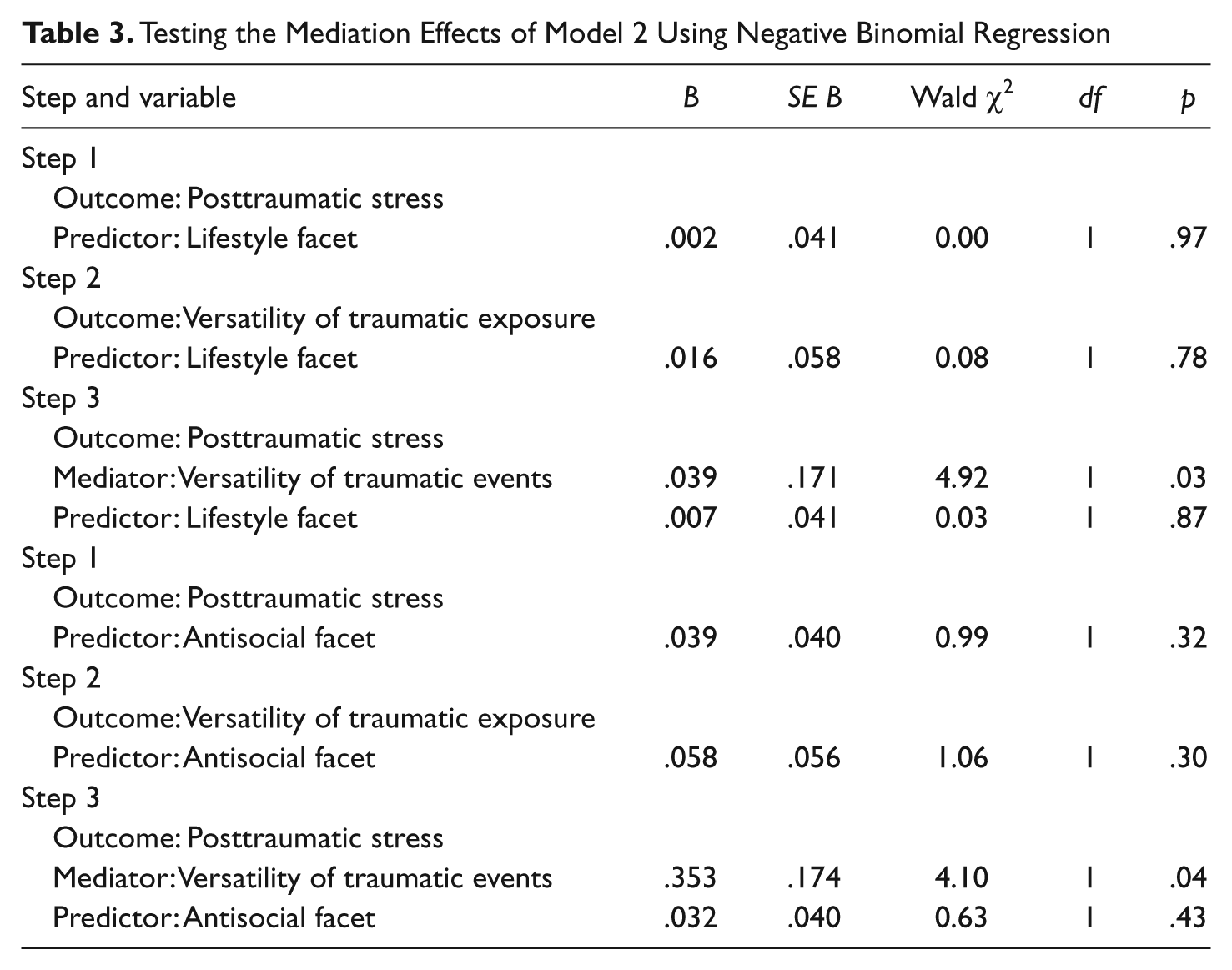
Table 3 contains the results necessary to examine Model 2. Following the procedure described by Frazier et al. (2004), we first tested the effect of the Lifestyle/Antisocial facet on posttraumatic stress through negative binomial regression (Step 1). The results were not statistically significant. To establish that the Lifestyle and Antisocial facets are related to versatility of traumatic exposure, we regressed the latter on the former variables (Step 2). Here again, we found no significant results. In Step 3, we regressed posttraumatic stress simultaneously on the Lifestyle/Antisocial facet and on versatility of traumatic exposure. The regression coefficients associated with the relationship between versatility of traumatic events and posttraumatic stress was significant in both cases, but the regression coefficients associated with the relationship between the Lifestyle/Antisocial facets and posttraumatic stress were not statistically significant. Although most of the results in Table 3 are not significant, this does not exclude a mediation effect. MacKinnon, Lockwood, Hoffman, West, and Sheets (2002) have demonstrated that the requirement that results are significant in Step 1, 2, and 3 decreases the ability to test for mediation effects, especially in small samples. They advise that a formal test (Sobel test) of the indirect effect be performed, and Preacher and Leonardelli (2010) provide an online calculator to perform this test. The Sobel test indicated that the indirect effect of the Lifestyle facet on posttraumatic stress through versatility of traumatic exposure is not significant, Sobel test (z) = .274, p = .78. Likewise, the indirect effect of the Antisocial facet on posttraumatic stress through versatility of traumatic exposure is not significant, Sobel test (z) = .845, p = .40. This means that there is no evidence for Model 2, according to which a positive relationship between the Lifestyle/Antisocial facet of the PCL-R and posttraumatic stress is mediated by versatility of traumatic exposure.
Testing the Mediation Effects of Model 2 Using Negative Binomial Regression
Conclusion
It has long been postulated by clinicians and researchers that psychopathy is characterised by a lack of anxiety and/or fear (Cleckley, 1976; Lykken, 1957), and this idea is the basis for several of the most recent theories on psychopathy (Daversa, 2010; Fowles & Dindo, 2006; Lykken, 1995; Patrick, 2007). However, results from empirical studies on this topic have been inconsistent (Hare, 2003; Schmitt & Newman, 1999), and the role of anxiety in the psychopathy construct remains unclear (Hare & Neumann, 2008). The primary aim of this study was to investigate the association between psychopathy and posttraumatic stress by testing two theoretical models that specify differing relationships between traumatic exposure, posttraumatic stress, and psychopathy. First, we found through bivariate negative binomial regression analyses that the Interpersonal and Affective facets of the PCL-R are negatively associated with posttraumatic stress. This implies that the core personality features of psychopathy are protective factors against the development of posttraumatic stress. This finding contributes to the view that an essential affective deficit underlies the interpersonal and affective features of psychopathy and that these personality features are crucial for understanding the relationship between psychopathy and anxiety (Cleckley, 1976; Daversa, 2010; Fowles & Dindo, 2006; Patrick, 2007).
To find more specific indications for the protective role of psychopathy, we tested whether the interpersonal and affective traits moderate the effect of traumatic exposure on posttraumatic stress (Model 1). We found that the Affective facet of the PCL-R, but not the Interpersonal facet, and traumatic exposure had a significant interaction effect on posttraumatic stress. This finding confirms the construct validity of the distinction made by factor-analytical studies between interpersonal and affective features within the psychopathic personality (Cooke & Michie, 2001; Hare, 2003; Hare & Neumann, 2005).
From the perspective that the development of posttraumatic stress can be conceptualized as a fear-conditioning process (Mowrer, 1960; Rauch et al., 2006), this finding confirms the theory that the affective features of psychopathy are characterised by low fear conditionability (Fowles & Dindo, 2006; Lykken, 1995; Patrick, 2007). A number of experimental studies have established this theory (Birbaumer et al., 2005; Blair et al., 2004; Hare & Quinn, 1971; Lykken, 1957; Newman & Schmitt, 1998), but our research replicates this finding with real-life unconditioned stimuli (traumatic exposure) and clinically relevant conditioned response (posttraumatic stress). Furthermore, our finding lends support to the assertion that psychopathy is characterised by a deficient cognitive processing of emotional information (Blair & Mitchell, 2009). Traumatic events might have less psychopathological consequences for high-psychopathic individuals because they are less inclined to interpret these events as threatening and horrifying. There is considerable experimental evidence for deficits in the cognitive processing of emotional information by psychopathic individuals (Christianson et al., 1996; Michell et al., 2006). For instance, Christianson et al. (1996) presented neutral slides (e.g., a woman bicycling on the street in front of a car) and negative emotional slides (e.g., a woman lying beside her bicycle on the street in front of a car bleeding from a head injury) to high- and low-psychopathic offenders. During a subsequent memory test, nonpsychopathic offenders recalled more central than peripheral details of emotional slides, whereas the psychopathic offenders recalled equally well the central and peripheral details of emotional slides. Apparently, the process of focussing on emotional information typically found in nonpsychopathic individuals is less operative in psychopathic individuals. However, when the offenders were asked to consciously evaluate the emotional valence of the slides, both psychopathic and nonpsychopathic offenders were able to rate the emotional slides as being more negative than the neutral slides. Christianson et al. conclude that there is a discrepancy between the conscious verbal rating of negative emotional events and the automatic processing of emotional information. In a similar vein, we found in our study that participants who score high on the Affective facet of the PCL-R were able to enumerate a number of emotional (i.e., traumatic) events when asked to do so (see Table 1: the nonsignificant correlation between the Affective facet and frequency and versatility of traumatic exposure) but that the impact of these events is mitigated by the Affective facet (possibly because of different cognitive processing of these emotional events).
Consistent with previous research in offender samples (Jordan et al., 1996; Urbaniok et al., 2007; Weeks & Widom, 1998), the degree of exposure to traumatic events during adulthood was quite high in our sample. Serious illness or sudden death of a relative was the most common type of traumatic event reported. Inspection of the individual cases that reported this type of traumatic event revealed that 60% involved the accidental death of a family member or friend, 33% involved the suicide of a family member or friend, and only 7% of the cases involved the violent death of a family member or friend through crime. The second most-commonly reported type of traumatic event was the index offence, suggesting that a violent or sexual offence can be experienced as traumatic by the offender himself or herself. However, previous research on offenders from general prison populations has indicated that higher levels of traumatic exposure prior to the offence increases the degree of offence-related PTSD, which makes the direct relationship between the offence and PTSD more complex (Payne et al., 2008). Some authors have claimed that an impulsive, irresponsible, and antisocial lifestyle would be associated with an elevated risk for traumatic exposure during adulthood (Frick et al., 1999). However, we found no significantly positive relationship between the Lifestyle and Antisocial facet of the PCL-R and frequency or versatility of traumatic experiences. This finding is in contradiction with Dembo et al. (2007) and Moeller and Hell (2003; but in line with Pham, 2012). However, these studies did not distinguish between traumatic exposure during adulthood and childhood. It is possible that the Lifestyle and Antisocial facets are positively related to stressful life events, such as familial and marital discord, financial and professional problems, and so on, rather than with traumatic events in terms of the DSM-IV A1 criterion. Such stressful life events might very well induce general maladaptive functioning, stress and negative emotions, rather than posttraumatic stress. Further research might focus on this topic. However, in this study, we found no evidence that the behavioral features of psychopathy have an indirect effect on posttraumatic stress through the mediating factor of traumatic exposure. Therefore, Model 2 on the association between psychopathy and posttraumatic stress was rejected.
Several limitations of the present study should be noted. First, we did not include traumatic exposure during childhood or adolescence in this study. Although there are theoretical and empirical indications that early traumatic exposure plays a role in the aetiology of psychopathy (Daversa, 2010; Farrington, 2006; Lang et al., 2002; Marshall & Cooke, 1999; Poythress et al., 2006; Weiler & Widom, 1996), and that traumatic exposure at a younger age increases sensitization to the effects of later traumatic events (Koenen et al., 2002), the focus of this study was not on the aetiology of psychopathy and posttraumatic stress. Our aim was to investigate the relationship between psychopathy and posttraumatic stress, and restricting traumatic exposure to adulthood made it possible to test two clear-cut conceptual models. Second, the reliability of our measurement of traumatic events might be impeded by the retrospective design and reliance on primarily self-report information. We tried to minimize the impact of this design by using (semi)structured interview formats. Third, the mean PCL-R total score of 22.9 in our sample is considerably higher than generally found in European samples (e.g., Coid et al., 2009; Hare, 2003), which indicates that our sample is not representative for the population of European or even Belgian detainees. However, in our opinion, the marked presence of psychopathy in our sample is not a threat to the validity of our results. To study a clinical phenomenon, it is important that this phenomenon is present in a considerable portion of the sample. Furthermore, the range in PCL-R scores in our sample was very large. Future research might focus on which of the above-mentioned mechanisms determine the moderating role of the emotional deficit in psychopathy (deficient fear conditioning, avoidance learning, or attentional bias) or investigate other psychopathological consequences of traumatic exposure, such as agoraphobia and depression (Gabriel et al., 2007). It seems to us that the topic of traumatic exposure and posttraumatic stress offers a theoretically and clinically relevant field of research outside the laboratory for studying psychopathic personality traits as a factor of robustness against internalising psychopathology.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.