
Abstract
Trauma and related mental health disorders are common among incarcerated women, but empirically sound mental health interventions are lacking in prisons. Implementing such interventions is fraught with legal and logistical barriers. These barriers can be particularly detrimental for trauma-specific interventions given the unique needs of trauma survivors, yet there is little documentation of these issues or how to address them. This study describes a pilot study of an 8-week, strengths-based, trauma-focused intervention for 26 incarcerated women. Women reported considerable mental health problems and trauma. The study highlights the importance of adapting stringent research methodologies for prison-based trauma interventions. For instance, women with trauma were reluctant to participate in an intervention advertised as trauma-based. Moreover, a randomized wait list control design was unfeasible because women wanted the support of their friends when discussing trauma and could not control their schedules 9 weeks in advance. Ultimately, this work may inform future efforts to implement effective trauma-based interventions behind prison walls.
Women represent a growing proportion of the prison population, with incarceration rates climbing 48% between 1995 and 2004 (Political Research Associates, 2005). Trauma is common among incarcerated women; nearly 6 in 10 report physical or sexual abuse prior to incarceration (Covington, 2007; Green, Miranda, Daroowalla, & Siddique, 2005; Harlow, 1999). Women also exhibit significant mental health problems, many of which may be caused or exacerbated by trauma (Covington, 2007).
The combined influence of trauma and related mental health problems has negative consequences for women’s functioning, in prison and on release. Correctional settings have become a revolving door for women; two-thirds have a history of prior convictions (Greenfield & Snell, 1999). Research suggests that the failure to address women’s mental health needs may contribute to their high recidivism (Jordan et al., 2002). Indeed, clinicians and researchers agree that current approaches to services for incarcerated women are inadequate to address their complex mental health needs. Research suggests that females have very specific needs including self-esteem, relationships, and trauma that must be addressed for positive change to occur. As a result, clinicians, researchers, and numerous national organizations agree that holistic, gender-specific, trauma-based programs are needed (e.g., Office of Juvenile Justice and Delinquency Prevention; Alemagno, 2001; Bloom, Owen, & Covington, 2003; James & Glaze, 2006; Mahoney & Daniel, 2006; Marcus-Mendoza, 2010; Van Wormer & Kaplan, 2006). Specifically, in their 2010 report, the Girls Study Group notes that there is an urgent need for trauma-based intervention services that address self-esteem and peer influences among female offenders (Zahn et al., 2010). The current study introduces a novel intervention that answers this call for gender-informed programming.
For many, prison may represent a rare opportunity to receive mental health treatment that is not available in the community (Green et al., 2005; Hammett, Gaiter, & Crawford, 1998; Quina et al., 2007). Given the high rates of trauma among female inmates, trauma-focused interventions are critical. Yet, evidence-based, trauma-focused mental health interventions for incarcerated women are lacking (Osher & Steadman, 2007). One reason for this may be that implementing structured, evidence-based interventions in prison settings is fraught with legal and logistical barriers. Past research has noted the challenges of conducting treatment research in prisons (Patenaude, 2004; Quina et al., 2007; Wakai, Shelton, Trestman, & Kesten, 2009). For instance, effectiveness research within a prison setting requires compromising stringent methodologies, which limits the feasibility of conducting randomized controlled trials (RCTs; Blagden & Pemberton, 2010; Patenaude, 2004; Wakai et al., 2009). Furthermore, the highly controlled nature of the prison environment necessitates significant adaptations to the content and structure of the intervention, which, in turn, run the risk of compromising the integrity of evidence-based procedures (Miller, Koons-Witt, & Ventura, 2004; Wakai et al., 2009). Without these adaptations, most evidence-based programs are simply not feasible for a prison environment (Zlotnick, Johnson, & Kohn, 2006). As such, research aimed at establishing an evidence-base for new or adapted programs using rigorous RCT methodologies, particularly for treatment of trauma, is difficult.
Though this research base highlights many of the challenges of conducting research in a correctional setting generally, it addresses few of the obstacles to conducting trauma-based research specifically. Given the very specific needs of trauma survivors, it is likely that such research has many unique challenges that warrant documentation. For instance, individuals with trauma are notoriously difficult to recruit and retain in interventions in the general community, let alone within a prison setting where inmates’ freedom is restricted by prison regulations (Kinard, 2001). Survivors of trauma are often hesitant to pursue treatment because of avoidance and lack of resources. Within the prison environment, there may be additional safety concerns that prevent inmates from identifying themselves as trauma survivors. The strict prison regulations add additional hurdles to study design and participant confidentiality that can seriously compromise the study’s integrity. While these additional hurdles are expected when conducting trauma research in a prison setting, little work has been done to document or provide suggestions on how to manage them. Given the great need for evidence-based trauma programs in prison, a discussion of these issues and their impact on prison-based trauma intervention research is highly relevant and greatly overdue.
In an attempt to address this gap in the literature, this article describes our experience conducting a pilot study of a strengths-based, trauma-focused intervention geared toward the needs of incarcerated women. In doing so, we provide a description of the varied mental health profiles of women who chose to participate in this intervention, and describe the challenges involved in conducting an intervention study in a correctional facility. Last, we provide recommendations for future prison-based intervention research based on the obstacles we encountered. Ultimately, this work may inform future efforts to implement effective trauma-based interventions behind prison walls.
This study first set out to uncover some of the hurdles that may impede the dissemination of empirically validated interventions to prison populations. We aim to share some of the lessons learned along the way with the hope of guiding future intervention research in identifying the needs of women served by this type of programming. Therefore, the aims of the study were to
Explore the feasibility of conducting a trauma-focused intervention study within the prison walls.
Document the challenges involved in implementing trauma-based interventions in correctional facilities.
Mental Health Needs of Treatment-Seeking Incarcerated Women
Trauma-Related Mental Health Problems
Incarcerated women report high rates of violent victimization, childhood abuse, and other forms of trauma (Bloom et al., 2003). Symptoms related directly to trauma can persist into adulthood. Nearly half of women who have experienced a traumatic event in childhood seek or receive mental health treatment, and roughly a third continue to report high rates of trauma-related symptoms as adults (Messina & Grella, 2006). Trauma may also be associated with increased risk for other mental health problems. Research consistently links histories of violence with negative mental health outcomes, such as depression, substance abuse, and intimate partner violence among incarcerated women at rates higher than those in the general female population (Browne, Miller, & Maguin, 1999).
A growing literature suggests that treatment of trauma and its related mental health problems may help reduce future criminal behavior (Bloom et al., 2003; Singer, Bussey, Song, & Lunghofer, 1995). Few trauma-focused interventions are currently implemented in correctional settings, despite the vast research base indicating their importance for incarcerated women (Heckman, Cropsey, & Olds-Davis, 2007; Kinsler & Saxman, 2007; Osher & Steadman, 2007). Zlotnick, Najavits, Rohsenow, and Johnson (2003) conducted a pilot study investigating the utility of an evidence-based treatment, called Seeking Safety, that targets trauma and substance use disorders (SUDs) concurrently—issues that frequently co-occur in incarcerated women. Seventeen women participated in the program, which included twenty-five 90-min sessions held biweekly over the course of 12 weeks. Results indicated that Seeking Safety was successful at significantly decreasing posttraumatic stress disorder (PTSD) and SUD symptoms, with almost 50% of participants no longer meeting the criteria for the disorder and 65% reporting no substance use at the 3-month follow-up. In addition, the program was positively received by the women with 90% of women approached agreeing to participate in the study. As noted by the authors, results of this study are limited by the small sample size and the lack of a control group. Nonetheless, this study provides promising evidence that with modifications to the stringent methodologies typically required for intervention research, treatments geared specifically toward the needs of women can be successfully implemented and are positively received among incarcerated women.
Other Mental Health Issues
In addition to mental health issues that stem directly from trauma exposure, a significant percentage of incarcerated women have preexisting mental health conditions (Morash, Bynum, & Koons, 1998; Staton, Leukefeld, & Webster, 2003). Studies of psychiatric morbidity consistently find higher rates of mental illness among incarcerated females compared with the general population, with high rates of substance abuse or addiction (70%), and schizophrenia, mania, and major depression (19%; Warren et al., 2002). Early trauma histories combined with incarceration may not only cause but can also exacerbate mental health symptoms (Dirks, 2004; Marcus-Mendoza, 2010; Messina & Grella, 2006). Like trauma symptoms, these other mental health problems have also been linked with patterns of offending. In prisons, women with mental health problems are more likely than women without mental illness to have committed a violent offense (40% vs. 4%), to have three or more prior probations or incarcerations (35% vs. 9%), to have been homeless prior to arrest (16% vs. 6%), and to have a substance abuse problem (74% vs. 5%; James & Glaze, 2006).
Self-Esteem
One mechanism by which trauma may influence subsequent mental health problems is through self-esteem (Hubbard, 2006; Staton-Tindall et al., 2007). The high prevalence of sexual abuse and domestic violence among incarcerated women may contribute to low self-esteem (Castellano & Soderstrom, 1997; Dickow, Robinson, & Copeland, 2007; Schram & Morash, 2002). In turn, low self-esteem may perpetuate illegal behaviors such as violence, risk-taking, substance abuse, and other criminal activity (Oser, 2006; Toch, 1969). Given evidence of linkages between self-esteem and criminogenic risk factors, self-esteem could play an important role in interventions for incarcerated women.
Treatment of self-esteem holds promise among incarcerated women. A study of psychoeducational group-work with incarcerated females, focusing on self-esteem and empowerment, documented significantly lower trauma and depression symptoms post-intervention (Pomeroy, Kiam, & Abel, 1998). Other studies suggest that women in prison showed significant improvement in self-esteem when provided with programs focusing on their self-image (Samuelson, Carmody, Kabat-Zinn, & Bratt, 2007). Despite these initial encouraging findings, little research has been conducted to build on this foundation (Van Wormer & Kaplan, 2006).
Interpersonal relationships
In addition to focusing on self-esteem, interventions targeted at improving women’s relationships may also be important. In correctional settings, women present with unique relationship needs and communication patterns (Marcus-Mendoza, 2010; O’Brien, 2001). They have a strong need for a relational connection with others in correctional settings (Bloom et al., 2003; Marcus-Mendoza, 2010; O’Brien, 2001), possibly due to their separation from family and friends on the outside. Facilitating healthy, safe relationships with incarcerated peers may promote more positive mental health outcomes. Such connections, if used properly in the context of therapeutic interventions, can promote positive mental health outcomes in prison and may lower recidivism rates (O’Brien, 2001).
There is strong empirical support for gender-specific, trauma-focused treatments (Brown, 2004; Johnson & Johnson, 2006; Payne, 2005). This literature suggests that gender-specific group interventions in correctional settings are most effective when focused on participants’ intrapersonal and interpersonal strengths (Alyson, Anne, Judith, Dalton, & Catherine, 2007; Pomeroy et al., 1998; Van Wormer & Kaplan, 2006). Bloom and Covington (1998) described three necessary ingredients of a supportive group environment that form the foundation of any successful gender-specific treatment: (a) physical and emotional safety, (b) reciprocal disclosures, and (c) exchanges between the group members and facilitators to foster a sense of connectedness in the group, and an emphasis on empowerment over deficits or disease. Covington (2007) reviews three gender-specific models of group treatment for female offenders that have been implemented in correctional settings. All three programs implement a holistic approach to address the three important domains of (a) mental health/trauma histories, (b) self-esteem, and (c) interpersonal relationships. While these interventions have all been informally validated in that they were positively received by the women who participated in them, none of them, to our knowledge, have been evaluated via a RCT, leaving the question of their effectiveness from a statistical standpoint unanswered.
Purpose and Aims
To our knowledge, there are currently no empirically supported interventions that simultaneously address these three important domains of incarcerated women’s functioning (i.e., trauma, self-esteem, and interpersonal relationships), despite the fact that numerous mental health organizations worldwide have advocated for such a holistic, gender-specific approach (e.g., Office of Juvenile Justice and Delinquency Prevention, Canadian Task Force on Federally Sentenced Women; see Bloom & Covington, 1998). The rigid boundaries of the prison environment necessitate interventions that are flexible in structure (e.g., number and duration of sessions) and implementation (e.g., facilitator training and supervision). This study sought to explore the role of strength-based trauma-focused programming specific to women’s needs in improving self-esteem and mental health. Given the dearth of evidence-based programming in correctional settings, the present study was a first step to establishing an evidence base for a novel intervention geared toward the needs of female prisoners.
Method
Recruitment Strategy
This study used a convenience sample of 29 female inmates from a medium security prison in upstate New York. As this was a pilot study, there were no inclusion or exclusion criteria for participation. Women were recruited through fliers posted throughout the prison and all women were welcome to join. Fliers advertising the program described the program as an “explor[ation] of what I have survived and how it can make me an even stronger person.” In keeping with the strengths-based, narrative approach of the group, we chose to word the fliers vaguely so as to allow the women to self-identify as survivors rather than overtly advertising it as “trauma-focused.” We wanted women to identify with a personal narrative of trauma rather than being objectively labeled with one. We also felt that such flexibility in our recruitment was not only more consistent with an ecologically valid research design (Cicchetti & Toth, 2009) but also necessary to enhance buy in and maximize retention within this already difficult to reach population, as many women are afraid or uncomfortable publically disclosing that they were attending a trauma intervention.
Women interested in participating attended an informational meeting where they were provided with more detailed information about the content and requirements of the program. In all, 30 women attended the information session and all but one signed up for the group and were given the informed consent and baseline measures. The appropriate Human Subjects Review Boards for the prison and the university conducting the research approved this study.
Given the high rates of trauma among female inmates (Covington, 2007; Green et al., 2005; Harlow, 1999), we expected that very few participants would have no trauma history, and indeed descriptive data showed that only 3 of the 29 women reported that they had never experienced a traumatic event. Of those who did report a trauma history, many had experienced multiple events with the most commonly reported being rape, domestic violence, and death of a loved one. To remain consistent with our research aims, the 3 women who had no trauma history were removed from all analyses for a final sample of 26 participants.
Participants
Participants included 26 women recruited from a medium-security prison in upstate New York. Demographic characteristics are shown in Table 1. In cases where there were missing data, sample sizes for that item are shown in parentheses. The mean age of the sample was 35.8 (SD = 8.2, range = 19-50). The majority of women had only one charge (76%; or n = 19) that was the least severe classification (e.g., alcohol or drug-related offenses). Notably, only 3 women were incarcerated for the most serious possible charge in New York State (e.g., murder).
Sociodemographic Information (N = 26).
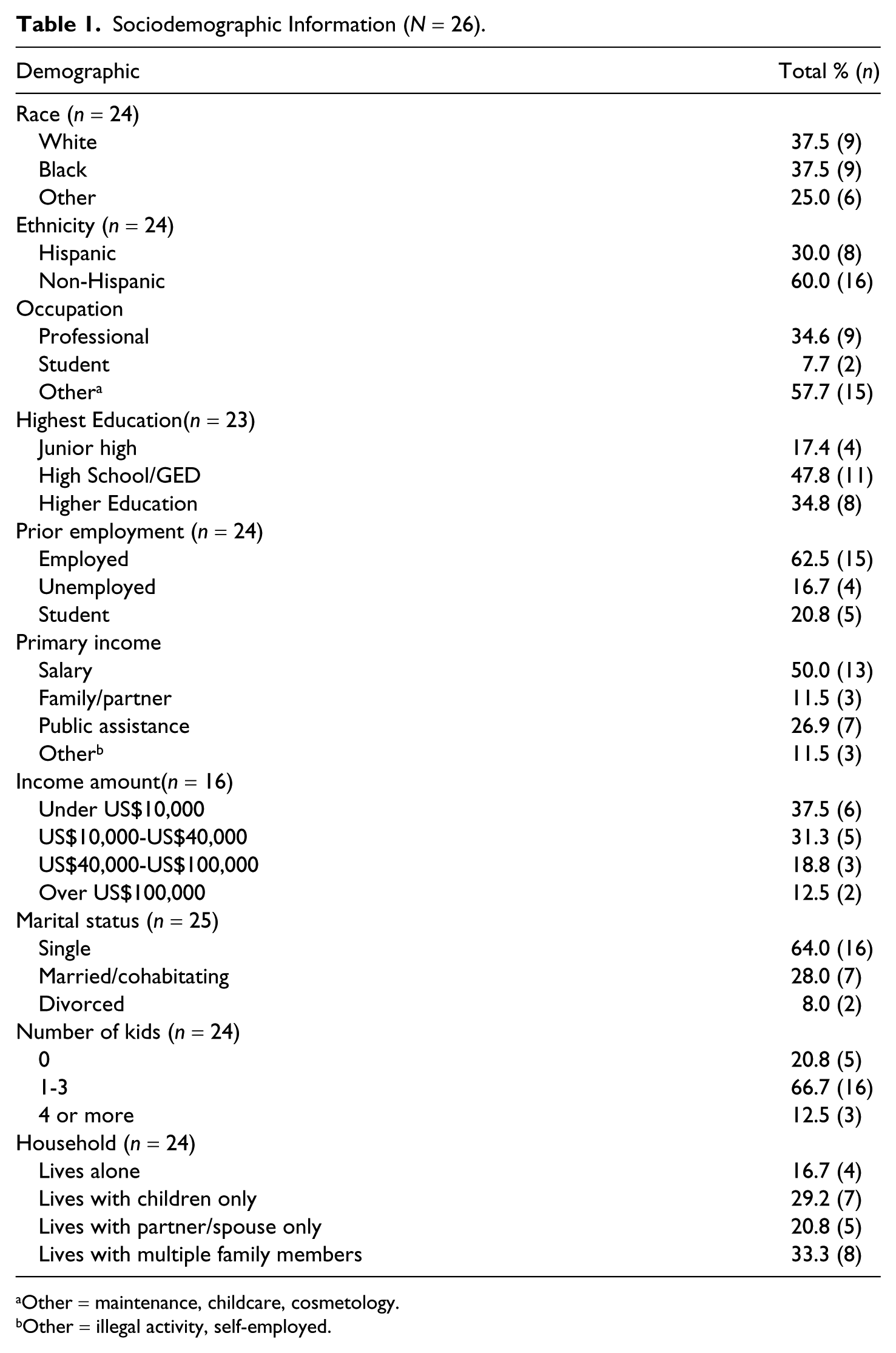
Other = maintenance, childcare, cosmetology.
Other = illegal activity, self-employed.
The sample comprised mostly Caucasian and African American participants (37.5% or n = 9 each). There was a larger percentage of Hispanic participants (43.3% or n = 8) than seen in the general population for New York State (17.8%; U.S. Census Bureau, 2010). Many of the women were professionals (e.g., sales, teaching, medical/legal service) prior to entering the prison system (34.6% or n = 9).
Research Design
To begin, we recruited a group of 14 women (Wave 1) in September of 2009. After providing informed consent, all participants were asked to complete baseline measures (T1) to assess mental health functioning (e.g., depression, positive and negative affect, trauma, PTSD, alcohol use), self-esteem, and general health. Participants in Wave 1 were randomized into an active treatment group (Intervention group, n = 8) and a waitlist control (WLC) group (n = 6). The Intervention group began the 8-week treatment immediately and ran from October to December of 2009, while the WLC was expected to begin the intervention in December, as soon as the Intervention group finished. In December (after the Intervention group completed treatment), both groups were asked to return to complete outcome measures (T2) to assess change in scores over time. Unfortunately, none of the Intervention or WLC participants returned to complete measures or begin the intervention. As a result, a second wave of 12 women (Wave 2) was recruited in January of 2010 once Wave 1 finished treatment. Wave 2 began treatment immediately after recruitment and ran from January to March of 2010.
Measures
Positive and Negative Affect Schedule (PANAS)
The PANAS (Watson, Clark, & Tellegen, 1988) is a self-report measure comprising two 10-item mood scales to assess positive and negative affectivity. Participants were asked to rate how they feel “in general, that is, on average” on a 5-point Likert-type scale ranging from “very slightly/not at all” (1) to “extremely” (5). High internal consistency of the scales has been demonstrated, and the positive and negative affect scales differentially relate to anxiety and depression in accord with Watson et al.’s (1988) conceptualization. This measure has been used internationally with incarcerated individuals (Hall, Benning, & Patrick, 2008; Van Harreveld, Van der Pligt, Claassen, & Van Dijk, 2007).
Self-Esteem Rating Scale (SERS)
The SERS (Nugent & Thomas, 1993) is a self-report measure of self-esteem that assesses problematic and positive levels of self-esteem. The measure includes 40 items that are rated on a 7-point Likert-type scale with half scored positively and half negatively. Total scores range from −120 to +120. The SERS has adequate convergent and concurrent validity and good internal consistency (Nugent & Thomas, 1993).
Trauma Symptom Checklist 40 (TSC-40)
The TSC-40 (Elliott & Briere, 1992) evaluates childhood and adult traumatic experiences. The measure includes six subscales (depression, anxiety, dissociation, sexual abuse trauma index, sexual problems, and sleep disturbances). Due to prison regulations, the sexual problems scale was not used. The items were answered on a 4-point Likert-type scale from “never” (0) to “very often” (3). The depression subscale has ten items, anxiety eight items, dissociation seven items, sleep six items, and the sexual abuse index five items. It is a reliable measure with alphas ranging from .66 to .77. Research exploring the impact of childhood traumatic events in a female prison population included the TSC-40 (Messina & Grella, 2006; Stein & Greenwall, 2007).
Drug Abuse Screening Test 10 (DAST-10)
The DAST-10 (Cocco & Carey, 1998) is a 10-item short form of the widely used DAST (Skinner, 1982) that provides a continuous self-report measure of drug use (nonalcohol) severity. It has excellent internal consistency (α =.92) and test−retest reliability (ICC = .78) in male and female substance abusers (Cocco & Carey, 1998). Items are scored as yes/no and the range is 0 to 10, with higher scores indicating more drug use.
Posttraumatic Stress Diagnostic Scale (PDS)
The PDS (Foa, 1995) is a self-report measure that determines the presence and severity of PTSD symptoms. The PDS first asks whether the person has experienced a trauma in the past year. Those who indicate yes are asked 17 questions that address three categories of symptoms associated with a diagnosis of PTSD: reexperience (5 questions), avoidance (7 questions), and hyper-arousal (5 questions). Questions ask how often respondents have been bothered by each symptoms on a scale from “never” (0) to “nearly always.” We defined a score of greater than or equal to 21 as having PTSD symptoms, as these scores have been found to reflect moderate to severe levels of PTSD symptoms.
Beck Depression Inventory (BDI-II)
The BDI (Beck, Steer, & Brown, 1996) is a 21-item self-report instrument designed to assess severity of depression. Items measure current affective, cognitive, motivational, and physiological symptoms. Each item is scored 0 to 3, with 3 indicating the most severe symptom. Coefficient alpha for the BDI-II in an outpatient sample was high (.92), and correlations ranging from .37 and .71 have been reported between the BDI-II and other self-report measures of depressive symptomatology (Beck et al., 1996). Total scores for the BDI-II indicated ranges of symptoms’ severity, and a cut score of 17 yields a 93% true positive rate for depression and an 18% false-positive rate in a clinical sample (Beck et al., 1996).
12-Item Short Form Health Survey Version 2 (SF12v2)
The SF12v2 (Ware, Kosinksi, & Keller, 1996) is a self-report scale derived from the SF36, a widely employed measure of physical and mental health. The instrument has two summary scales, the Physical Component Summary (PCS-12), which measures physical limitations or abilities, and the Mental Component Summary (MCS-12), an index of mental health and well-being. Higher scores indicated better functioning for both scales. The scale has strong psychometric properties and well-developed national norms (Garratt, Schmidt, Mackintosh, & Fitzpatrick, 2002; Turner-Bowker, Bartley, & Ware, 2002). The SF12v2 (Zaller et al., 2008) and the SF36 (Garratt et al., 2002; Turner-Bowker et al., 2002) have been utilized in prison studies among incarcerated people.
Treatment program: The Tree
The intervention in the current study, called The Tree, represents an integrated, strength-based, trauma-focused approach, aimed at addressing the complex relational needs of incarcerated women. The Tree is grounded in narrative theory, which places the client in the role of “expert” in her own life and the practitioner in a “not knowing” stance, empowering the client to direct the therapeutic relationship (Hutchinson, 2008; Payne, 2005). This perspective uses the individual’s subjective “life story,” as the touch point for meaningful change (Hutchinson, 2008; Payne, 2005). Narrative theory is culturally sensitive to the racial diversity of the prison population and the female gender. The strengths-based approach permits one to have connections to others while recognizing individual strengths and deficits. To maximize utility and generalizability, The Tree was designed so that community volunteers can implement it without advanced clinical training. Ex-inmates lead many groups, which provides the women with a positive role model. The two facilitators of the current group were a master’s level social worker and a volunteer who was an ex-inmate at the prison.
The intervention is structured around the book The Tree That Survived the Winter (Fahy, 1989), with each session’s theme taken from a section of the book (e.g., Session 1: Surviving; Session 2: Growing; Session 3: Disappointments; etc.). The aims of the intervention are to (a) help women identify strengths; (b) assist women in discovering, valuing, and sharing life stories; (c) model positive change through listening to other women (including co-facilitators) in the group who have moved from problems and weaknesses to strengths and gifts; and (d) help women make connections to each other.
The intervention consists of eight sessions, each roughly 1.5 to 2 hr long. In the first session, women participate in establishing ground rules, and the requirements, including active participation, completion of homework assignments, and no more than two absences, are explained. Sessions use a mixture of group and individual activities. The basic components of each session include an exercise related to the topic of the day, homework in the form of reading assignments and writing tasks, a reading from a daily meditation book related to the topic and feedback at the end of class regarding what was most helpful and what they would change. The last session includes a celebration. Each woman is given a book of all her work from the 8 weeks, a copy of The Tree That Survived the Winter, and a certificate of completion.
Results
Recruitment and Retention
The original study design involved half the participants from Wave 1 being randomized to an active treatment group that began at baseline and half to a WLC scheduled to begin 8 weeks after baseline (see Figure 1). In Wave 1 (n = 14), eight women were assigned to the Intervention group and six were assigned to the WLC group. While only four women from this group completed the intervention, attendance was exceptional; everyone attended at least six of the eight sessions. This suggests that the limiting factor to attendance had more to do with personal and logistical obstacles to enrollment rather than dropping out once enrolled. While none of the women returned for T2 assessments, two women came from the WLC group to meet with the investigators and share some insights. Two major themes emerged from these meetings: (a) A randomized WLC design is unfeasible in a prison environment and (b) the women who enrolled in the study have no control over their schedules and cannot predict their availability 9 weeks in advance. More information about each is provided below.
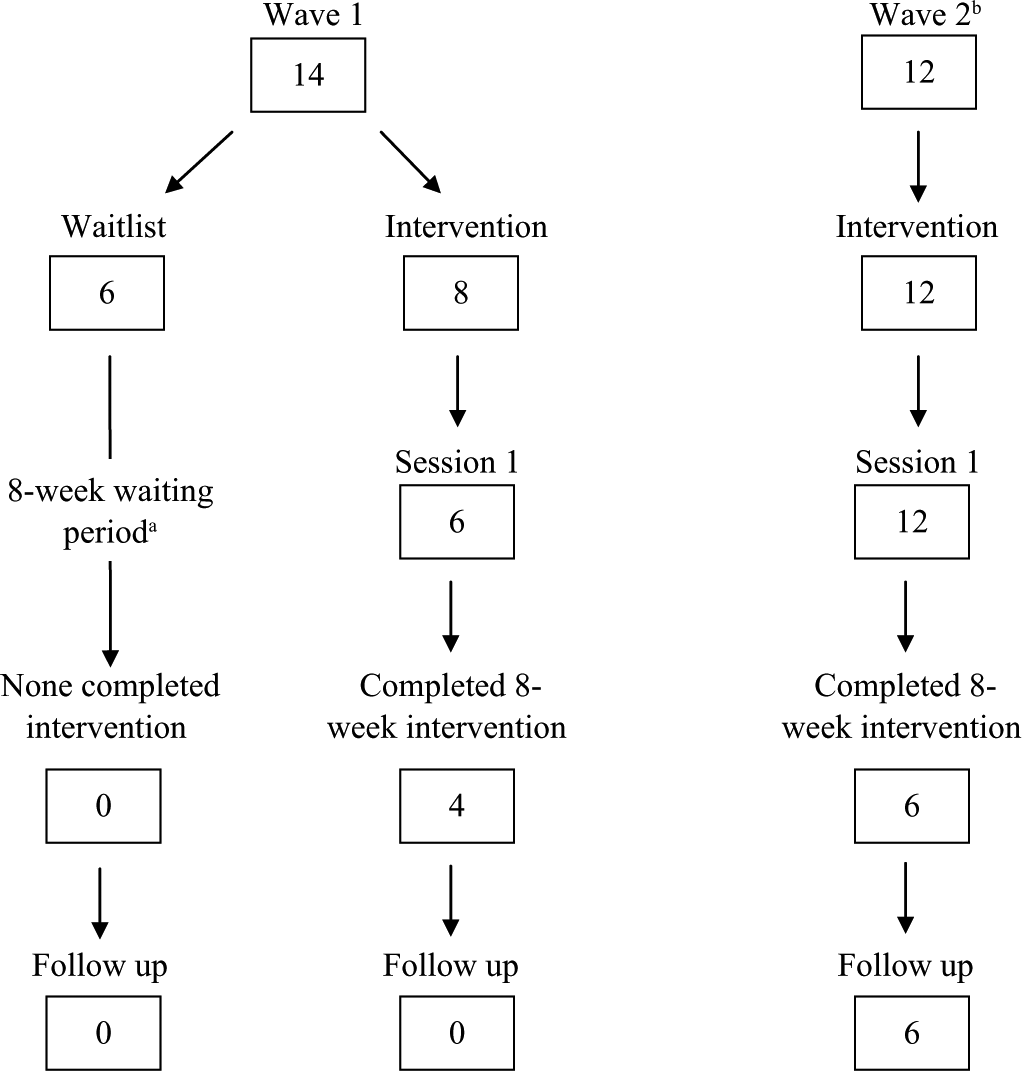
Recruitment and retention flowchart.
First, the women shared that prisoners have every aspect of their lives dictated to them. They were disappointed to volunteer for something out of their own volition, only to be told they could not start for another 8 weeks. Second, prison administrators change women’s schedules every few weeks to allow different individuals to participate in employment, physical activity, and school. This gave women very little control over their schedules. While participants were available on Wednesdays on enrollment, this could change in a short time period. When the intervention for the WLC started, many women were no longer free. Therefore, WLC designs appear to be unfeasible for the prison setting. Instead, an active control in which the intervention under investigation is compared with another commonly used treatment program may be more appropriate. If a WLC design is necessary, researchers must be prepared to carefully coordinate with prison administration to work around the prisoners’ schedules.
Relatedly, the women were excited about the prospect of participating in the intervention with their friends. They have very limited free time, and the group was scheduled during their recreational time, which meant that they were giving up one of their few opportunities to socialize to participate. Female inmates value personal connections, and the prospect of being separated by random assignment deterred participation. Furthermore, women with trauma are likely to be more guarded than a community population given their histories, not to mention the constant surveillance and prison politics inmates face. The prison environment is often not a safe place for women to share personal details of their lives, let alone identify themselves as trauma survivors, as doing so may put them at risk of being targeted by other inmates. Allowing women to stay with their friends helps to foster a safe, open-group atmosphere. For these reasons, random assignment may be inappropriate for trauma-focused group work within the prison setting. Instead, randomization methods that allow women to remain with their friends (e.g., block randomization, randomizing by ward) may result in better retention.
As shown in Figure 1, on our posting for Wave 2, 12 women attended the information session, and 6 completed the intervention and T2 assessments. Based on prison records, the women who did not return had many reasons, including release to community corrections, transfer to another prison, and being in disciplinary housing that prevented them from attending. Sentence length proved to be an additional barrier to recruitment. Out of the 30 women recruited from both waves, two thirds (66.2%, N = 20) had maximum sentences of 6 years or under, suggesting that this population is highly transient and, as a result, trauma treatment programs that require extended commitments may be inappropriate for a prison setting. Indeed, examining the status of women who did not complete the intervention and/or posttest assessments revealed that out of the 30 women, 7 had been released and 4 had been transferred.
Mental Health Functioning
Despite these hurdles and design challenges, we were able to successfully collect information on the initial mental health functioning for all 26 women who signed consent. Baseline mental health scores for the total sample (N = 26; see Table 2) suggest that this sample was suffering from moderate to severe symptoms across almost all domains. Specifically, according to national norms, participants reported high levels of negative affect and low positive affect equivalent to those seen among psychiatric inpatients (Watson & Clark, 1994), as well as moderate to severe depression (Beck et al., 1996). The women also reported lower than average self-esteem and physical and mental health functioning. The average level of drug use prior to incarceration passed the clinical cutoff for problematic drug abuse. Finally, trauma-related symptoms including dissociation, anxiety, and sexual abuse fell in the moderate range while average PTSD symptoms closely approached the clinical threshold for a diagnosis of PTSD.
Mental Health Functioning for the Sample at Baseline (N = 26).
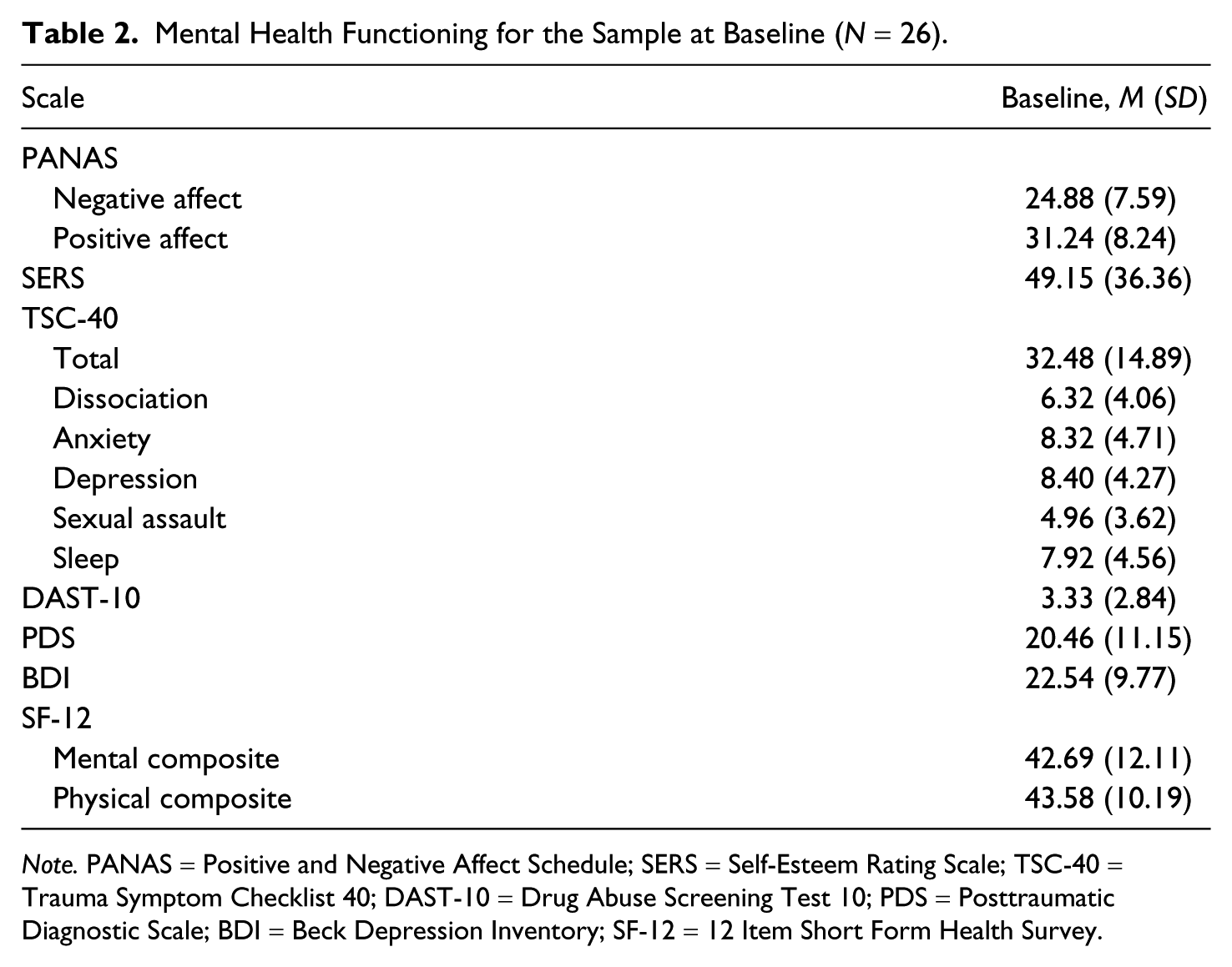
Note. PANAS = Positive and Negative Affect Schedule; SERS = Self-Esteem Rating Scale; TSC-40 = Trauma Symptom Checklist 40; DAST-10 = Drug Abuse Screening Test 10; PDS = Posttraumatic Diagnostic Scale; BDI = Beck Depression Inventory; SF-12 = 12 Item Short Form Health Survey.
Discussion and Recommendations
Given the high rates of trauma among incarcerated women, there is a great need for research on trauma-focused interventions in correctional settings. It is critical that these interventions address the unique needs of women including an emphasis on self-esteem and interpersonal connectedness (Zahn, et al., 2010; Bloom & Covington, 1998). As pointed out by Miller and colleagues (2004), hurdles to implementing evidence-based programs within prison walls include limits on the financial resources available to obtain, train, and supervise certified mental health therapists to facilitate the groups. These resources are particularly important for trauma work, which requires extreme sensitivity when talking about the trauma to ensure that the individual is not retraumatized in the process.
The current intervention includes several elements that appear to be conducive to the prison environment and may be useful additions to future prison-based intervention studies. Community volunteers without advanced mental health training facilitate the group, maximizing its utility in settings where resources for mental health programming are limited. The intervention is relatively short in duration, increasing the likelihood that this transient population will be able to complete the program before being transferred or released. The single group design also allows women to remain with their friends, which not only increases the chances that they will want to participate but also builds on preexisting relationships to encourage the development of a healthy social support system.
Lessons Learned
Our study emphasized the need to balance stringent methodology alongside ecologically valid research when adapting interventions for challenging settings (see Cicchetti & Toth, 2009; Rutter & Sroufe, 2000). This pilot study highlighted a number of challenges that accompany trauma-focused intervention research with incarcerated women (Morash et al., 1998). For example, we were forced to eliminate a randomized wait list control design and shorten the duration of treatment to maximize the likelihood that participants could complete the intervention before schedules changed or sentences were completed. Such changes may be required to match interventions to the prison environment.
Notably, the greatest challenges we encountered in designing and implementing this study were lengthy and numerous IRB (Institutional Review Board) applications limiting our ability to ask certain questions (e.g., posttreatment drug use, sexual problems), restrictions on bringing certain materials into the facility, and difficulty in conducting the group at times that did not conflict with other events at the facility (e.g., work, recreational activities). Interestingly, some of the requirements from the state, such as the prohibition of providing subject incentives, were in contrast with the university preference that participants be compensated for their time. Not only did these factors force us to adapt elements of our research protocol and intervention, but they also constrained our recruitment to only women who were willing to give up recreational time to come to the group.
An additional barrier to implementing the intervention involved poor communication between prison staff and administrative agencies in charge of granting us clearance to the prison. Although we obtained clearance to enter the prison for the duration of the intervention, it was not uncommon for our names to disappear from the visitor list on any given week, causing delays. Although all materials for the intervention had been approved by all appropriate agencies, at times we had difficulty bringing certain things into the prison because prison staff had not been notified. In many ways, these difficulties are part and parcel with any intervention research, let alone research conducted within a prison setting. However, it does highlight the importance of beginning the design phase well in advance of data collection as the current study was more than a year in the making from the time we began the IRB approval process to the time we began the intervention. In future studies, researchers may also need to familiarize themselves with state or institution-specific guidelines on participant compensation and recruitment incentives. As demonstrated by the administrative difficulties we encountered on a regular basis while conducting the intervention, this type of research requires good relations with prison staff to navigate the abundance of prison rules, regulations, and policies that must be addressed prior to study implementation.
Many of the challenges identified in the current study are consistent with those cited by past researchers (Trestman, 2005; Wakai et al., 2009). However, when compounded by the particular needs of women with trauma, these obstacles take on a new meaning. To be feasible, trauma treatment research must be adapted to fit the prison structure. For instance, in contrast to many trauma RCTs we chose not to exclude women who did not have a traumatic experience that meets the Diagnostic and Statistical Manual of Mental Disorders (DSM) diagnostic criteria. While allowing women to self-identify as trauma survivors may have resulted in a less rigorous test of the intervention, it may have been necessary for us to loosen this common inclusion criteria to encourage participation in a setting where disclosing one’s status as a trauma survivor could be stigmatizing or unsafe.
Conclusion
This study had a number of strengths and limitations. Clearly, the small sample size severely limited our ability to examine true effects of the intervention and/or conduct attrition analyses. As with all research in prison settings, our research design and implementation were restricted by the prison regulations against asking certain questions, bringing in certain materials, conducting groups at certain times, and so on. At the same time, attempting to implement and evaluate an intervention in a prison setting allowed us to learn from the roadblocks we encountered and elicit helpful suggestions from the women on how future studies could be more successfully employed. Hopefully, these findings will serve to inform future research on incarcerated women, aimed at developing services and programs that will best meet their needs, improve their functioning outside of prison, and reduce their chances of recidivating.
Footnotes
Acknowledgements
The authors wish to thank Hanna Monk for her assistance with data management, the staff at Step by Step for their generosity of time, and the incarcerated women who were brave enough to step forward and take part.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by NIMH K01MH75965-01.