
Abstract
This study measured the prevalence of current, severe symptoms of a mental health problem in an adult population of inmates in Ontario, Canada. The Resident Assessment Instrument–Mental Health was used to measure the prevalence of symptoms among a sample of 522 inmates. Propensity score weighting was used to adjust for nonrandom selection into the sample. Prevalence estimates were derived for the total inmate population, remand and sentenced, males and females, and Aboriginal and non-Aboriginal inmates. It is estimated that 41.1% of Ontario inmates will have at least one current, severe symptom of a mental health problem; of this group, 13.0%, will evidence two or more symptoms. The number of symptoms is strongly associated with presence of a psychiatric diagnosis and level of mental health care needs. Female (35.1%) and Aboriginal (18.7%) inmates are more likely to demonstrate two or more current, severe symptoms. Greater efforts must be made to bridge the gap between correctional and mental health care systems to ensure inmates in correctional facilities can access and receive appropriate mental health care services.
Introduction
Responsibility for the treatment of inmates with a mental health problem falls somewhere between the correctional system and the mental health care system (Constantine et al., 2010; Floyd, Scheyett, & Vaughn, 2009; Olley, Nicholls, & Brink, 2009). Nevertheless, confronted by reports that as many as two thirds of jail inmates and one half of prison inmates have symptoms of a mental health problem (Brink, Doherty, & Boer, 2001; James & Glaze, 2006; Lafortune, 2010; Steadman, Osher, Robbins, Case, & Samuels, 2009), correctional services in Canada, the United States, and other Western countries have made important strides in recent years to improve mental health services they provide to inmates, albeit still within a context where security, administration of punishment, and reduction of recidivism—not treatment—are the mandated purposes (Brandt, 2012; Floyd et al., 2009; Lamberti & Weisman, 2004; Lurigio, 2011; Olley et al., 2009; Ontario Ministry of Community Safety and Correctional Services, 2008). Measurement of the prevalence of inmates with current, severe mental health problems continues to have important treatment, cost, and policy implications for both correctional and mental health care systems (Lamb, 2009; Lurigio, 2011; Soderstrom, 2007; Sung, Mellow, & Mahoney, 2010).
Fazel and Danesh (2002) conducted a systematic international review of 62 studies of severe mental disorder in prisoners conducted between the years 1996 and 1999, comprising nearly 23,000 inmates in jails and prisons. On average, 3.7% of male inmates and 4.0% of females demonstrated a psychotic illness; 10% of males and 12% of female inmates demonstrated major depression. The prevalence of severe mental disorder was almost equal for jail detainees (inmates held awaiting trial) and sentenced inmates in prison. Fazel and Danesh reported that the prevalence of severe mental disorder (psychosis, depression) among inmates was two to four times greater than in the general population. In a 2012 update of the original review, Fazel and Seewald (2012) extended the analysis to include a total of 81 studies of the prevalence of severe mental disorder among prisoners spanning the years 1966 to 2010, comprising 109 different samples totaling 33,588 inmates. Fazel and Seewald reported pooled prevalence rates for psychosis of 3.6% among male prisoners and 3.9% among female prisoners, and prevalence rates for major depression of 10.2% and 14.1% for male and female prisoners, respectively, with no significant differences in prevalence observed between jail detainees and sentenced prisoners. Rates of comorbidity with substance misuse ranged from 13.6% to 95%. Despite growing international attention to the high rates of mental illness among inmates in jails and prisons, Fazel and Seewald (2012) observed that the prevalence rates of psychosis and depression among inmates remained virtually unchanged since their 2002 review. At the same time, as research on the prevalence of severe mental disorder among inmates continues to accumulate, it is apparent that correctional systems remain ill-equipped to deal with the growing evidence and demand to provide adequate mental health services (Morgan et al., 2012; Steadman et al., 2009).
In Canada, few studies of the prevalence of mental disorder among inmates have been undertaken, and almost all exclusively with male inmates. Motiuk and Porporino (1991) conducted 2,185 mental health assessments with male federal inmates, and reported current (within 1 year) prevalence rates of 5.0% for psychotic disorders, and 9.9% for depressive disorders. Bland, Newman, Thompson, and Dyck (1998) compared the prevalence of mental disorders in a random sample of male community residents in Edmonton, Alberta, with a random sample of male inmates incarcerated in an Edmonton provincial correctional facility. The 6-month prevalence rate for schizophrenia among inmates was 2.2%; for major depression, 13.9%; mania, 3.3%; and for cognitive impairment, 1.1% (Bland et al., 1998). Prevalence rates for male inmates were on average five times those observed in the community sample of males. Corrado, Cohen, Hart, and Roesch (2000) studied 790 male detainees at a pretrial detention center in Vancouver, British Columbia, and reported prevalence rates for schizophrenia of 4.9%, for major depression 6.0%, and bipolar disorder 4.1%. Brink et al. (2001) studied 267 male offenders sentenced to federal prison and found prevalence rates of 8.4% for mood disorders and 3.5% for schizophrenia/psychotic disorders, with rates for mood disorders four times greater among inmates compared with a community comparison sample, and three times greater for schizophrenia. A 2004 report on the health care needs of Canadian federal inmates reported that approximately 3% of male inmates are found to be “mentally disordered” at intake, and 7% have emotional/mental health symptoms requiring immediate attention (Canadian Journal of Public Health, 2004).
Though most international research demonstrates a greater prevalence of severe mental disorder among female inmates, their small numbers (6% of federal inmates, 11.5% of provincial inmates; Landry & Sinha, 2008) and disbursement across a multitude of facilities means that very little Canadian research has been carried out on their mental health status and care needs (Canadian Journal of Public Health, 2004). In a recent study, Lafortune (2010) examined the prevalence of mental disorder among 671 male and female inmates admitted to provincial correctional facilities in Quebec, and found that 6.4% of male inmates and female inmates had a diagnosis of schizophrenia in their medical file; 19.8% of males and 26.3% of female inmates had a diagnosis of depressive disorder. Similarly, despite their significant overrepresentation in the Canadian correctional system (4% of the Canadian population, but 18% of federal and 22% of provincial inmates; Landry & Sinha, 2008), very little research has been conducted on the mental health status and care needs of Aboriginal inmates, though studies from Australia (Butler, Allnutt, Kariminia, & Cain, 2007; Heffernan, Andersen, & Kinner, 2009) suggest higher rates of mental illness among Aboriginal inmates.
Despite calls for action from the Canadian Medical Association (MacDonald, Hucker, & Hebert, 2010) and Canadian Psychiatric Association (Chaimowitz, 2012), and appeals from the Correctional Investigator of Canada (2012) for more resources and capacity to address the mental health needs of correctional inmates, still to date there is relatively little known about the number of inmates with severe mental disorder currently incarcerated in Canadian jails and prisons, and their needs for mental health services and treatment.
Setting and Background
With an average daily count of approximately 8,600 inmates, the Ontario correctional services system is the largest provincial system in Canada. Remand inmates held in jails and detention centers awaiting trial account for 63% of inmates. Provincial sentence inmates serve a maximum period of incarceration of 2 years less a day, and are held in correctional centers or in the case of short sentences, jails and detention centers, and account for another 32% of inmates. The remainder of “other” inmates is made up of those held on immigration warrants, parole violations, youth warrants, and custody transfers (Ontario Ministry of Community Safety and Correctional Services, Program Effectiveness, Statistics and Applied Research Unit, 2008; Porter & Calverley, 2011).
In January 2005, the Ontario Ministry of Health and Long-Term Care announced $50 million to expand services for persons with a mental illness who come into contact with the law. A priority was placed on estimating the number of inmates in Ontario jails, detention centers and correctional centers with current, severe symptoms of mental health problems as an important first step in determining the need for additional resources.
The study reported here describes the use of the Resident Assessment Instrument–Mental Health (RAI-MH), a standardized mental health status assessment instrument mandated for use in all Ontario psychiatric facilities, to assess the mental health status of a volunteer sample of 522 inmates, and to estimate the prevalence of current, severe symptoms of mental health problems in the general inmate population, excluding substance abuse problems, which are now commonly viewed as a separate disorder requiring a different set of treatment responses (Brandt, 2012; Fazel & Danesh, 2002; Fazel & Seewald, 2012; Steadman et al., 2009). Prevalence rates for the general inmate population, and subgroups by correctional status (remand, sentenced), gender, and Aboriginal status are presented.
The results from the current study remain the most comprehensive assessment of inmate mental health symptoms reported to date in Canada, and compare favorably with recent pilot results from the Correctional Service of Canada’s CoMHISS (Computerized Mental Health Intake Screening System) project (Correctional Investigator of Canada, 2012; Correctional Service of Canada, 2010a, 2010b).
Method
Sample
The study universe included all general population adult inmates of Ontario correctional facilities during the period May 2005 to September 2007. Inmates held in specialized mental health treatment units (approximately 250 province-wide, or 3% of total) were not included in the study due to concerns about security and informed consent. As remand and sentenced inmate groups are reported to have a different prevalence of mental health problems (Butler, Allnutt, Cain, Owens, & Muller, 2005; James & Glaze, 2006; Trestman, Ford, Zhang, & Wiesbrock, 2007), both were included in the research. The Ontario Correctional Services Offender Tracking and Information System (OTIS) database was used to identify an initial June 2005 sample of seven jails, detention centers and correctional centers that had large enough inmate populations to ensure representation by correctional status, gender, and Aboriginal status. Later, in June 2006 and again in June 2007, additional correctional facilities were included in the study to increase the number of female and Aboriginal inmates, and to achieve an adequate sample size for comparing subpopulations of interest.
OTIS is an administrative database that contains detailed demographic, criminal offence and custody history on all past and current inmates in jails and detention and correctional centers in Ontario, along with Level of Service–Ontario Revision (LSI-OR) assessments of offenders. The LSI-OR (Andrews, Bonta, & Wormith, 1995) is a well-researched and validated risk/need correctional assessment instrument composed of 45 binary risk and criminogenic need items grouped into eight domains encompassing history of criminal behavior, antisocial personality pattern, antisocial attitudes and beliefs, antisocial associates, education/employment, family/marital, and leisure/recreation experiences and history of substance abuse. The LSI-OR is used to classify level of security and risk for reoffending, and to plan rehabilitation programs targeting criminogenic needs (Andrews & Bonta, 2010; Andrews et al., 2012).
In accordance with the ethical principles established by the Canadian Tri-Council Policy Statement on Ethical Conduct for Research Involving Humans (Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans, 1998, 2010), and research guidelines established by the Ontario Adult Corrections/Youth Justice Research Committee (Ontario Ministry of Community Safety and Correctional Services, 2004, 2010), it was not possible to conduct random sampling of inmates for participation in the research. Instead, at each study site, research staff were given access to inmates to make a brief presentation about the research, and request volunteers to participate. Volunteers were asked to sign an informed consent form that detailed the purpose of the research and the terms of participation, including completion of the RAI-MH instrument and permission for the researchers to access both correctional and medical files, and to obtain staff input. In total, 522 volunteers across 14 different jails and detention and correctional centers participated in the research between June 2005 and September 2007, representing 6% of the average daily inmate count during the period 2005-2007 and 14 out of 32 or 44% of all correctional facilities in the province which combined account for 68% of the total inmate population. There were no significant differences in the inmate population structures of the participating institutions versus nonparticipating institutions, save for the greater likelihood of including larger jails more likely to have larger female populations (5 jails combined accounting for 1,015 male and 55 female inmates) versus smaller jails having largely male populations (10 jails accounting for 651 male and 42 female inmates).
Instrument
The RAI-MH is “a comprehensive, standardized instrument for evaluating the needs, strengths, and preferences of adult psychiatric patients in institutional settings” (Hirdes et al., 2005, pp. 2-4). Mandated in 2005 for use in all Ontario inpatient psychiatric facilities, the RAI-MH was chosen for the current study to ensure a common understanding of mental health problems between the Ontario correctional and mental health care systems.
The RAI-MH does not produce a formal diagnosis of a mental illness. Completed by clinical staff, including psychiatrists, family physicians, nurses, social workers, and therapists, the RAI-MH is comprised of more than 400 items that describe patient demographic characteristics, mental and physical health symptoms, functional status, substance abuse, risk of violence to others and self-injury, experience of traumatic life events, diagnostic history, social support, medication compliance, service use, and discharge readiness (Jones, Perlman, Hirdes, & Scott, 2010). The information derived from the RAI-MH is used to identify patients in need of further assessment and diagnosis and to support treatment planning in the form of clinical assessment protocols (CAPs), 18 different patient treatment need domains ranging from needs for safety (self-harm, harm to others, self-care) and social functioning (social relationships, informal support, supports for discharge, conflict with others, traumatic events, criminal involvement) through economic issues (personal finances, education and employment), autonomy (control interventions, medication, risk for rehospitalization), and health promotion (smoking, substance use, weight management, and others; Hirdes et al., 2005, 2011).
The RAI-MH items demonstrate good reliability and validity in inpatient settings (Gibbons et al., 2008; Seto, Harris, & Rice, 2004; Urbanoski, Mulsant, Willett, Ehtesham, & Rush, 2012), with interrater agreement averaging in excess of 80%, weighted kappa values of .70 across all items, and Cronbach’s alpha coefficients of .77 through .95 (Hirdes et al., 2002, 2008; Jones et al., 2010).
Within the RAI-MH instrument, 38 mental state indicators are devoted to describing mental health symptoms, ranging from hallucinations and delusions through reduced social interaction and sleep problems. Each is scored as 0 = (not present), 1 = (present but not exhibited in last 3 days), 2 = (exhibited on 1-2 of last 3 days), and 3 = (exhibited daily in last 3 days; Hirdes et al., 2001). The individual mental state indicator scores are combined into five symptom scales.
Positive Symptoms Scale (PSS): combines scores for four indicators of positive psychotic symptoms, including hallucinations, command hallucinations, delusions and abnormal thought process. Scores on the PSS range from 0 to 12, with a threshold score of 3 or above indicating current, severe positive symptoms of psychosis.
Depression Rating Scale (DRS): combines scores for seven mental state indicators, including facial expressions (sad, pained), tearfulness, negative comments, anxious complaints, fears/phobia, persistent health complaints and persistent anger. DRS scores range from 0 to 14, with scores 6 or above indicating current, severe symptoms of depression.
Negative Symptoms Scale (NSS): measure of negative psychotic symptoms combining four indicators: anhedonia, withdrawal, lack of motivation and reduced interaction. Scores on the NSS range from 0 to 12, with a threshold score of 6 or more indicating current, severe negative symptoms of psychosis.
Mania Symptoms Scale (MSS): composed of six mental state indicators, including inflated self-worth, hyperarousal, irritability, increased sociability/hypersexuality, pressured speech and labile affect. Scores range from 0 to 12, with scores of 5 or greater indicating current, severe symptoms of mania.
Cognitive Performance Scale (CPS): measures the level of cognitive functioning. The CPS combines indicators of short-term memory, cognitive skills for daily decision making, communication skills, and self-performance in eating. CPS scores range from 0 to 7, with scores of 2 or more indicating current, moderate to severe symptoms of cognitive impairment.
The PSS and NSS scales have been validated in inpatient psychiatry settings against the Positive and Negative Syndrome Scale (PANSS), the most widely used measure for the assessment of symptoms of schizophrenia (Kay, Fiszbein, & Opler, 1987; Kelley, White, Compton, & Harvey, 2013). The DRS has been validated in long-term care and inpatient psychiatry settings against both the Hamilton and Calgary depression scales (Burrows, Morris, Simon, Hirdes, & Phillips, 2000; Frederiksen, Tariot, & De Jonghe, 1996), and the CPS has been validated against the Mini Mental State Examination and the Test for Severe Impairment (Hartmaier et al., 1995; Jones et al., 2010).
Instrument Training
Research staff attended a 1-day educational session on the administration of the RAI-MH, under the supervision of the training supervisor. Completion of the RAI-MH involves both face-to-face interviews with the patient as well as additional fact-checking and data collection from files and clinical staff, and possibly family members and other agencies involved with the patient (Hirdes et al., 2001). The training session included a number of detailed sample cases for assessment, against which the validity of the assessments completed by the individual trainees was evaluated by the training supervisor. A pilot analysis (n = 5) of the interrater reliability of the RAI-MH as administered by members of the research team in the early stages of the data collection suggests a close concordance between assessments, with an average kappa value of .41.
Data Collection
To ensure that assessments were completed reliably and for security reasons, two research staff members were present at each administration of the RAI-MH, and scoring of the instrument was later reviewed to produce a final consensus on any item that caused disagreement. Research staff members were rotated through the different RAI-MH assessment teams to guard against systematic bias in completion of the assessments. The data acquired from the face-to-face assessments were fact-checked and supplemented with information from on-site medical and correctional files, from nursing and correctional staff, and the OTIS database. The in-person administration of the RAI-MH instrument with inmates required between 1 and 1.5 hr to complete, with an additional 2 hr devoted to collection of information from correctional and nursing staff and from file reviews, and for final review for consensus. All of the inmates who volunteered to participate in the study completed the RAI-MH assessment instrument.
Data Analyses
The IBM–SPSS Statistics 20 program (IBM Corporation, 2012) was used to compute propensity score weights to correct for nonrandom selection bias in the data, and to perform the statistical analyses.
Results
Propensity Score Weighting
Voluntary, nonrandom selection of inmates can introduce selection bias into a study sample, with the result that estimated prevalence rates and other statistical measures may be inaccurate (Austin, 2011; Bruce, Pope, & Stanistreet, 2008). In a previous study comparing the recidivism of San Francisco jail inmates who attended a mental health court program with inmates who did not receive the program, McNiel and Binder (2007) used a propensity score weighting technique to correct for potential selection biases in the treatment sample. Their approach combined the treatment and nontreatment groups into one sample and, using a set of possibly selection-biasing background variables, estimated the differential probability that a given inmate would be found in the treatment or nontreatment group. Following the approach recommended by Hirano and Imbens (2001), McNiel and Binder (2007) then used the inverse of the estimated differential probability to derive a weighting score for each case, such that inmates with a given set of characteristics who have too high a probability of being included in the treatment group are down-weighted in influence in the analysis, while those with too small a probability of selection are now weighted more heavily in the analysis (McNiel & Binder, 2007).
Following this approach in the current study, the volunteer sample of 522 inmates was combined with a random sample of 1,200 inmates drawn from the OTIS database covering the 2005-2007 period of the study. Eight potentially selection-biasing variables including gender, age, history of abuse and psychiatric treatment, Aboriginal status, correctional status, total LSI-OR score and current offence severity, as ranked on a 26-point index ranging from the least serious types of offences (e.g., unclassified offences, municipal bylaw infractions, traffic offences) to the most severe including violent sexual offences, attempted murder and homicide (Ontario Ministry of Community Safety and Correctional Services, Program Effectiveness, Statistics and Applied Research Unit, 1995) were included in a logistic regression model predicting the probability of selection into either the sample group or the randomly drawn comparison group. As almost half (48.7%) of the inmates held on remand did not have an LSI-OR completed, separate logistic regression analyses were conducted for inmates with and without the LSI-OR. The results of the logistic regressions are shown in Table 1.
Logistic Regression Model Coefficients and Test Statistics—Estimated Probability of Selection Into Volunteer Sample or Random Comparison Sample, Separate Analyses for Inmates With or Without LSI-OR Scores.
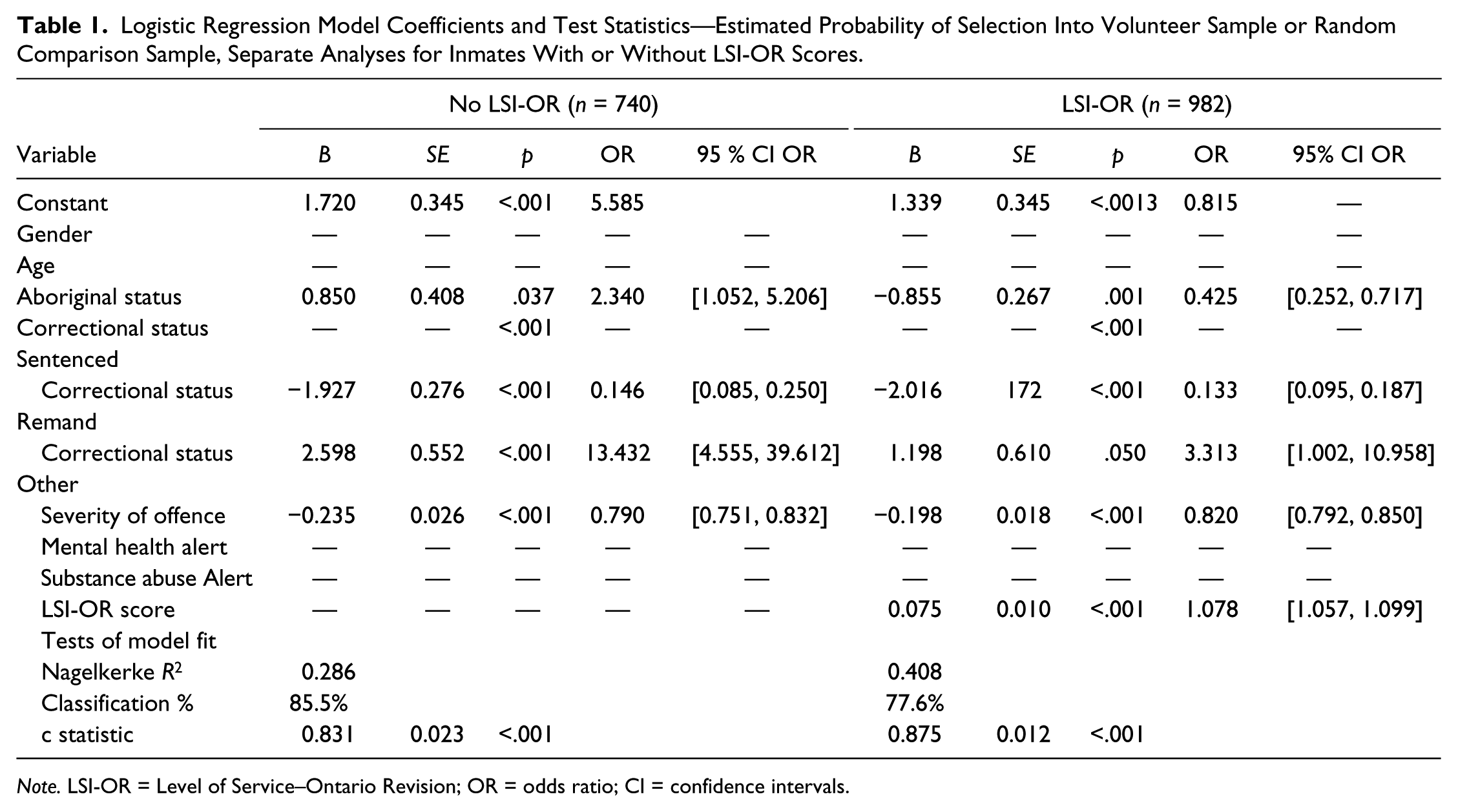
Note. LSI-OR = Level of Service–Ontario Revision; OR = odds ratio; CI = confidence intervals.
The “No LSI-OR” (n = 740) and “LSI-OR” (n = 982) models performed adequately, correctly classifying 85.5% and 77.6% of cases, respectively, as members of the treatment sample or comparison sample. The c statistics for the logistic regression models derived from the Receiver Operating Characteristic (ROC) curve analysis were .831 (p < .001) and .875 (p < .001.) respectively, demonstrating a high degree of accuracy in classifying sample membership (Norusis, 2005; Pintea & Moldovan, 2009). The estimated logistic regression coefficients and odds ratios were in the expected direction, with inmates held on remand underrepresented in the treatment sample (ORnoLSI = 0.146; ORLSI = 0.133) while the category of other inmates (e.g., immigration warrants, parole violations, etc.) was overrepresented (ORnoLSI = 13.432; ORLSI = 3.313) when compared with the group of sentenced inmates. Inmates held in custody for minor offences were underrepresented in the treatment sample (ORnoLSI = 0.790; ORLSI = 0.820), and there was a slight overrepresentation based on the magnitude of the LSI-OR score (ORLSI = 1.078). Inmates with an Aboriginal background were overrepresented in the No LSI-O model (ORnoLSI = 2.340) and underrepresented in the LSI-OR model (ORLSI = 0.425), a consequence of a higher proportion of Aboriginals in the treatment sample without a completed LSI-OR assessment.
The logistic regression predicted values for group membership were inverted to construct standardized by sample-size propensity score weights to be applied to the sample data (Guo & Fraser, 2010; Hirano & Imbens, 2001; McNiel & Binder, 2007). An additional term was added to the weighting equation to further adjust for the substantial oversampling of female inmates in the raw data. The results of the propensity score weighting procedure are shown in Table 2.
Characteristics of Total Inmate Population 2006/2007, Volunteer Inmate Mental Health Assessment Sample (N = 522) and Propensity Weighted Sample (NW = 522), Number, (Percent) and Pearson Chi-Square Goodness of Fit Test with Total Inmate Population Distribution.
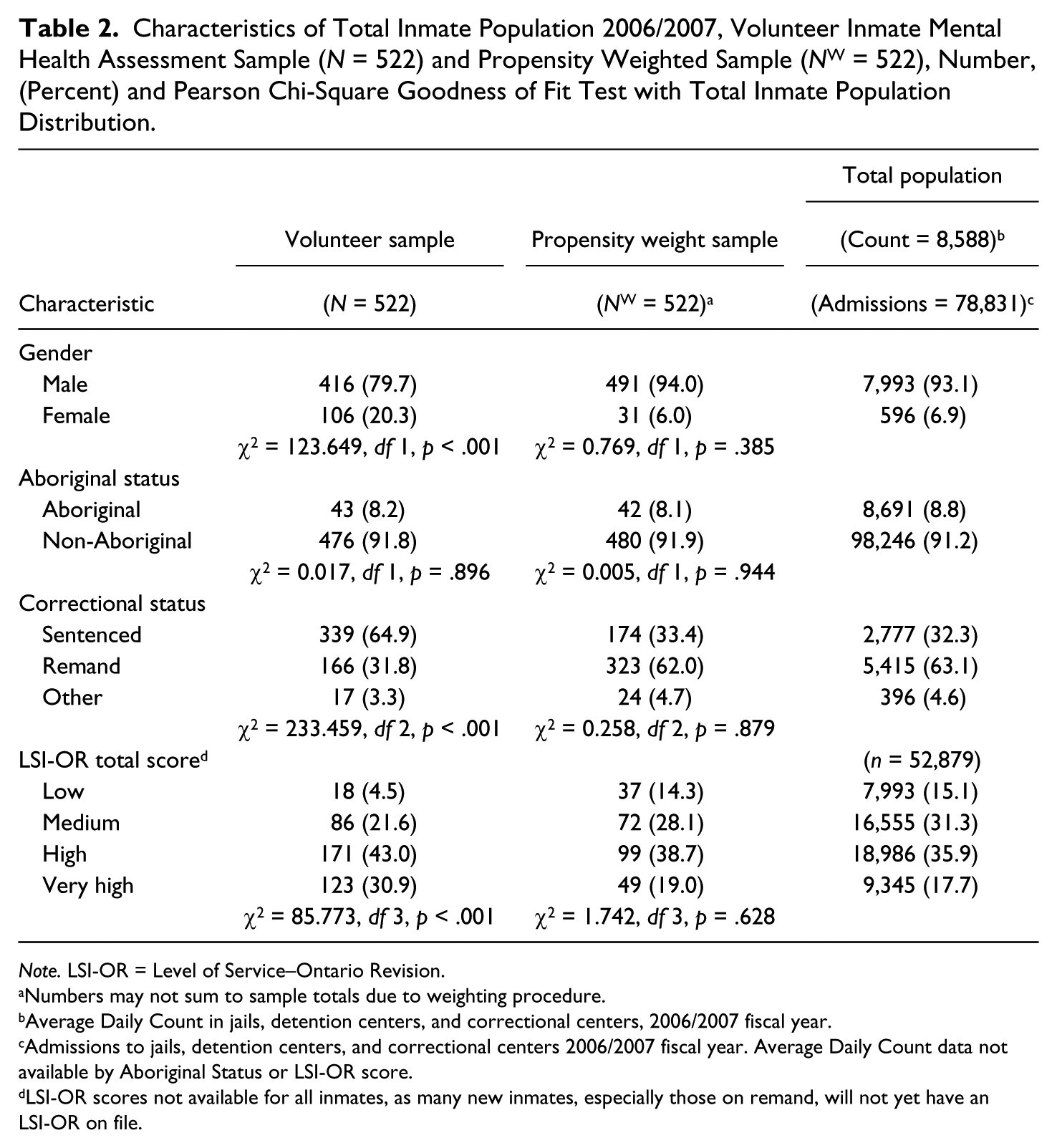
Note. LSI-OR = Level of Service–Ontario Revision.
Numbers may not sum to sample totals due to weighting procedure.
Average Daily Count in jails, detention centers, and correctional centers, 2006/2007 fiscal year.
Admissions to jails, detention centers, and correctional centers 2006/2007 fiscal year. Average Daily Count data not available by Aboriginal Status or LSI-OR score.
LSI-OR scores not available for all inmates, as many new inmates, especially those on remand, will not yet have an LSI-OR on file.
Compared with the raw data sample, the distribution of gender, Aboriginal status, correctional status and LSI-OR scores in the propensity score weighted sample NW = 522 closely mirrored the total inmate population distributions. The chi-square distributional tests showed no statistically significant differences between the NW = 522 and total inmate population distributions. Consequently, the NW = 522 propensity score weighted sample distributions were used to construct the estimates of prevalence of current, severe symptoms of a mental health problem in the general population of inmates in Ontario correctional facilities.
Prevalence of Symptoms of a Mental Health Problem in the Propensity Score Weighted Sample
The proportions of inmates measured as having no symptoms, or symptoms assessed as below or above the scale cut-off scores are shown in Table 3, for both the propensity score weighted sample (NW = 522) and, for comparison purposes, the original volunteer sample (N = 522).
Proportion of Inmates Assessed With the RAI-MH Instrument With No Symptoms, One or More Symptoms Below Scale Cut-Off Scores, and One or More Symptoms Above Scale Cut-Off Scores, Propensity Score Weighted Sample (NW = 522) and Volunteer Sample (N = 522), Number and (Percent).
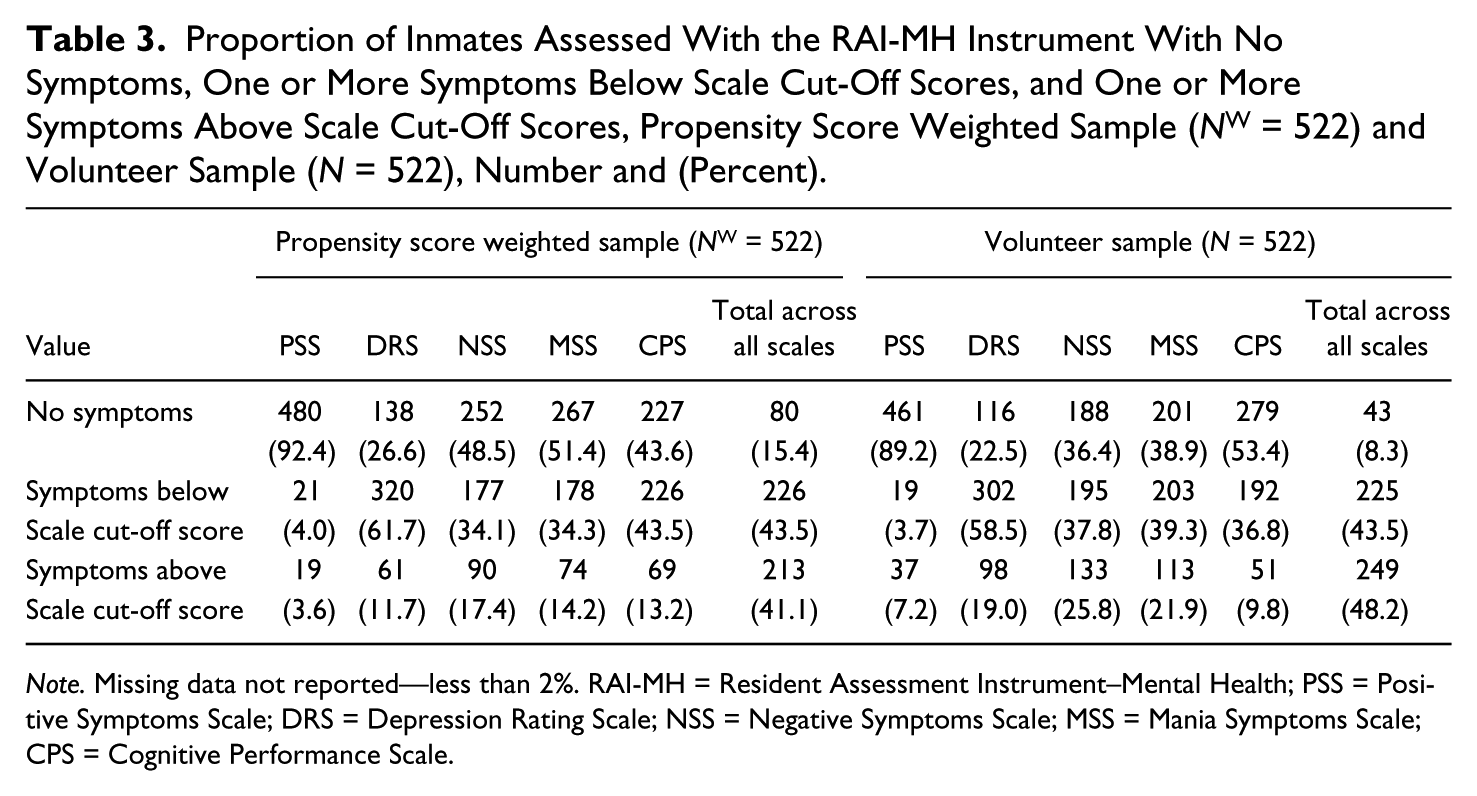
Note. Missing data not reported—less than 2%. RAI-MH = Resident Assessment Instrument–Mental Health; PSS = Positive Symptoms Scale; DRS = Depression Rating Scale; NSS = Negative Symptoms Scale; MSS = Mania Symptoms Scale; CPS = Cognitive Performance Scale.
Eighty of the inmates in the propensity score weighted sample (15.4%) showed no current symptoms of a mental health problem. Another 226 inmates (43.5%) demonstrated at least one mild to moderate symptom of a mental health problem, as measured by values below the cut-off score for the five different symptom scales. Current, severe symptoms of a mental health problem were seen in 41.1% (213/522) of inmates, as indicated by values exceeding the cut-off score on at least one of the five symptom scales. Compared with the distribution of symptom scale cut-off scores in the volunteer sample, the effect of the propensity score weighting procedure was to generally reduce the frequency of scores above the scale cut-off values for the PSS, DRS, NSS, and MSS scales, with only a modest increase (9.8%-13.2%) in the frequency of CPS scores above the scale cut-off.
Table 4 displays the distribution of inmates in the propensity score weighted sample, by number of current, severe symptoms of a mental health problem measured as exceeding the cut-off scores on any of the five symptom scales, and gender, Aboriginal status, and correctional status.
Number of Current, Severe Symptoms of a Mental Health Problem—Propensity Score Weighted Sample NW = 522, by Total, Correctional Status, Gender and Aboriginal Status.
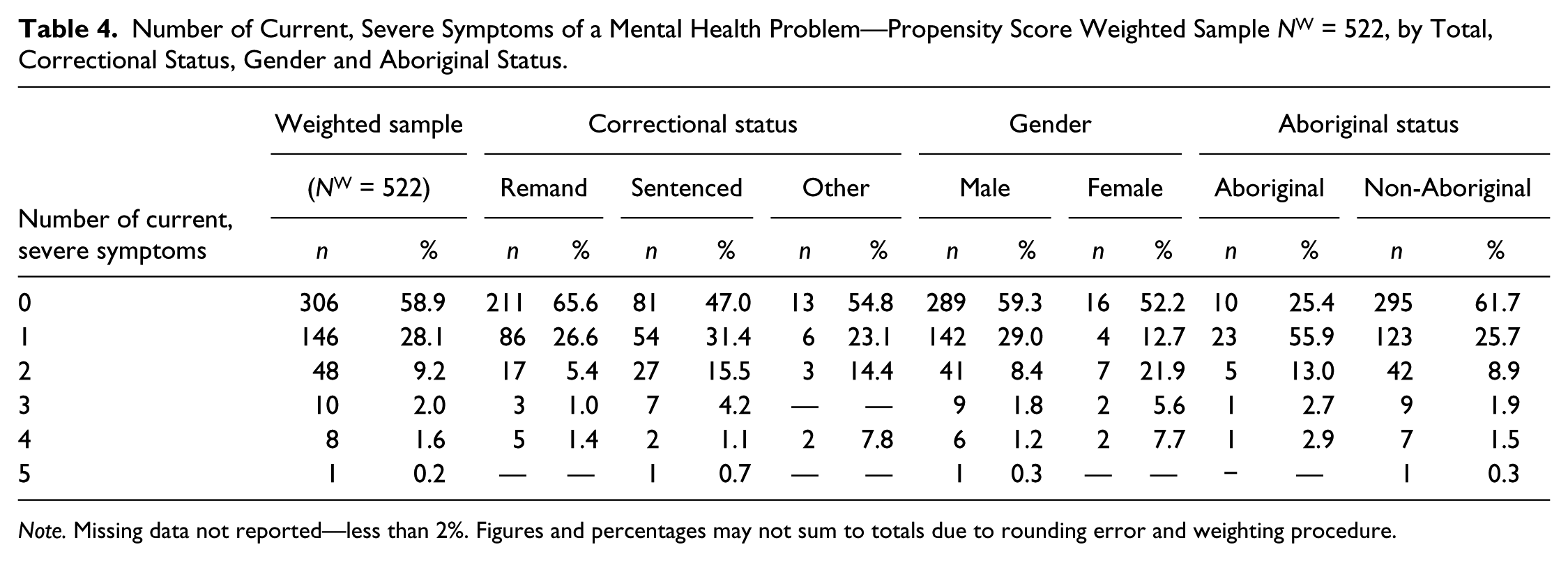
Note. Missing data not reported—less than 2%. Figures and percentages may not sum to totals due to rounding error and weighting procedure.
Overall, 58.9% of inmates showed no current, severe symptoms of a mental health problem. More than one quarter (28.1%) of inmates demonstrated at least one current, severe symptom, of which cognitive impairment (33.2%) and negative symptoms (28.2%) accounted for nearly two thirds of all cases. Another 13.0% of inmates showed two or more current, severe symptoms, with depression (64.5%) and negative symptoms (71.9%) most common.
Sentenced and other inmates were significantly more likely to have current, severe symptoms of a mental health problem compared with inmates held on remand, χ2(10, nW = 518) = 35.884, p < .001, with the sentenced group showing the highest proportion of inmates with two or more severe symptoms. Other studies (Butler et al., 2005; Fotiadou, Livaditis, Manou, Kaniotou, & Xenitidis, 2006; James & Glaze, 2006; Wilper et al., 2009) have reported a higher prevalence of mental health problems among remand inmates or, more recently (Fazel & Seewald, 2012) no difference. Still other research suggests that, independent of correctional status, symptoms of mental health problems will be most current and severe among the most recently incarcerated offenders, and will decline in intensity as adjustment to incarceration takes place (Blaauw, Roozen, & van Marle, 2007; Brandt, 2012; Hassan et al., 2011).
In the current study, average time spent in jail held on remand (M = 162.4, median = 108.0) actually exceeded the average time incarcerated for sentenced inmates (M = 158.2, median = 92.4) and other inmates (M = 75.0, median = 48.5), due in large part to practical and legal barriers to interviewing inmates held on short-term remand warrants, coupled with a small number of inmates in the study sample being held on remand who are facing serious criminal charges requiring considerable case preparation time and multiple court appearances, as well as out of jurisdiction/federal inmates being held pending transfer, and the trend to increasing remand hold times across the Canadian correctional system generally (Weinrath, 2009). With shorter average times between admission and RAI-MH assessment for both sentenced (M = 84.9, median = 37.0) and other inmates (M = 50.3, median = 33.0) compared with inmates held on remand (M = 111.7, median = 59.5), and negative zero-order correlations between length of time to assessment and severity of symptoms across the five mental health symptoms scales (PSS = −0.017, p = .707, DRS = −0.203, p < .001, NSS = −0.122, p = .005, MSS = −0.057, p = .193, CPS = −0.088, p = .043), the lesser severity of symptoms among remand inmates probably stemmed from their longer average time of incarceration and longer period of time before assessment on the RAI-MH (Blaauw et al., 2007; Hassan et al., 2011).
As in previous studies (Binswanger et al., 2010; Drapalski, Youman, Stuewig, & Tangney, 2009; Floyd et al., 2009; James & Glaze, 2006; McCorkle, 1995), female inmates were significantly more likely to demonstrate current, severe symptoms compared with male inmates, χ2(5, nW = 519) = 17.481, p = .004, with female inmates (35.2%) evidencing a higher proportion of two or more current, severe symptoms compared to males (11.7%).
Aboriginal inmates were significantly more likely to demonstrate any current, severe symptoms (74.6%) compared with non-Aboriginal inmates (38.3%), χ2(5, nW = 517) = 22.600, p < .001, echoing the findings in other research (Brink et al., 2001; Butler et al., 2007; Heffernan et al., 2009; Trevethan, Moore, & Rastin, 2002).
Though an on-file DSM Axis I diagnosis was available for only a small proportion of inmates in the sample (N = 114; nW = 70), the number of severe symptoms (0, 1, 2-5) was statistically significantly related to the presence or absence of a diagnosis, χ2(5, nW = 517) = 20.649, p = .001, with inmates with two or more symptoms significantly more likely to have a DSM Axis I diagnosis on file, most often depression. The number of severe symptoms was strongly correlated (r = .328, p < .001) with a summary index score across all of the 18 different RAI-MH CAP measures of mental health care needs, and was significantly associated, χ2(4, nW = 517) = 91.709, p < .001, with a subset of eight RAI-MH CAPs measuring safety, social functioning and autonomy, with 31% of inmates exhibiting two or more current, severe symptoms scoring as “high risk/immediate need” compared with 8.2% for inmates with only one current severe symptom and 9.8% for inmates with no symptoms.
Prevalence of Symptoms of a Mental Health Problem in the General Inmate Population
For reporting the prevalence of current, severe symptoms of a mental health problem in the total Ontario general inmate population, symptoms were grouped into three categories with 0 = no current, severe symptoms, 1 = one current, severe symptom, and 2 = two or more current, severe symptoms. The calculated proportions derived from the propensity score weighted sample were applied to the total average daily inmate count 2006/2007 (n = 8,588) and subgroups by correctional status, gender, and Aboriginal status to arrive at estimates of the prevalence of current, severe symptoms of mental health problems in the general population of inmates in Ontario correctional facilities, as shown in Table 5. Ninety-five percent confidence intervals are reported for the prevalence estimates.
Prevalence Rates in Ontario Inmate Population Derived From Propensity Score Weighted Sample Estimates, by Number of Current, Severe Symptoms and Total, Correctional Status, Gender, and Aboriginal Status.
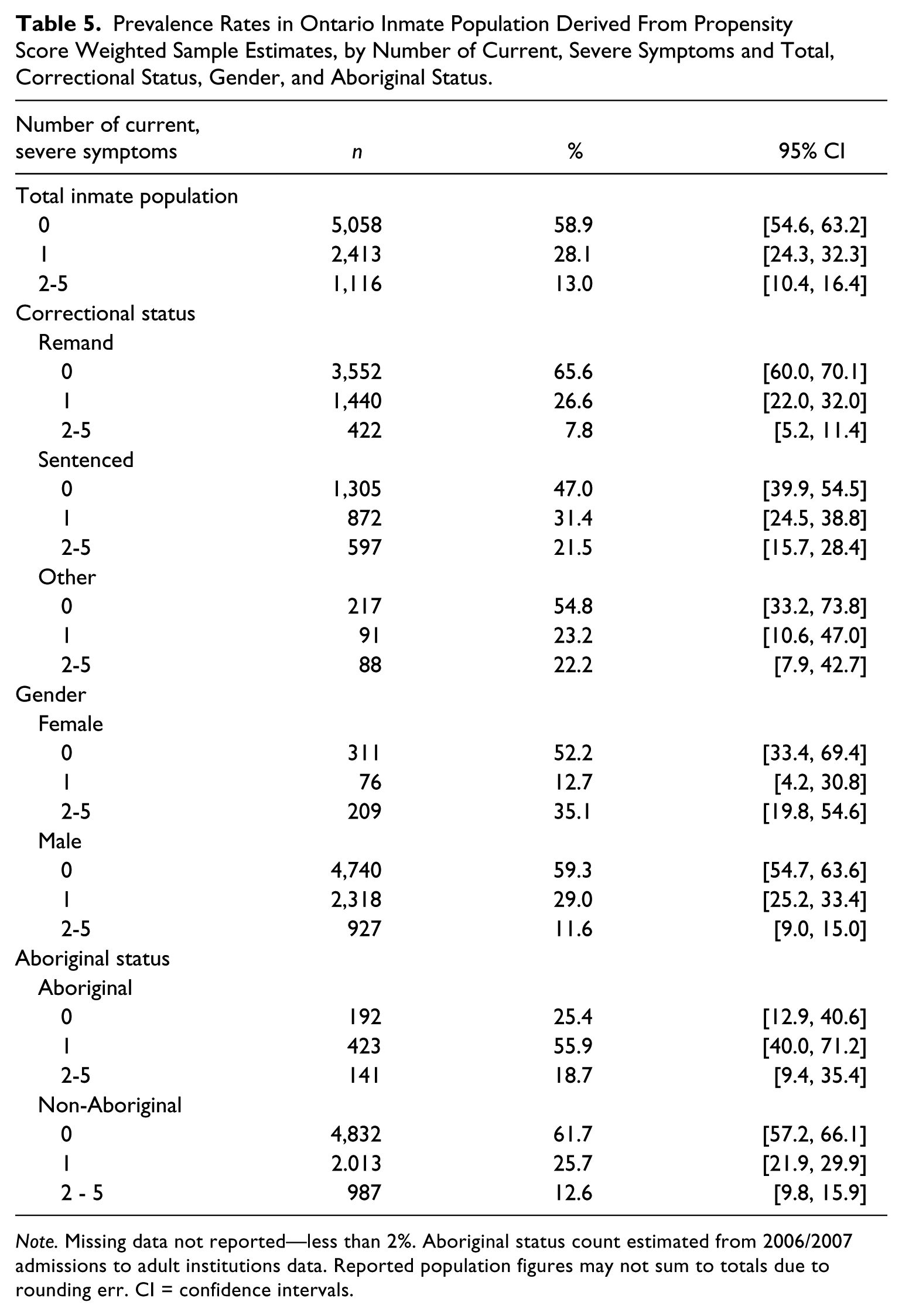
Note. Missing data not reported—less than 2%. Aboriginal status count estimated from 2006/2007 admissions to adult institutions data. Reported population figures may not sum to totals due to rounding err. CI = confidence intervals.
These calculations project that as many as 2,413 inmates (28.1%: 95% CI = [24.3, 32.3]) in the general population during the 2006/2007 period demonstrated at least one current, severe symptom of a mental health problem. Another 1,116 inmates (13.0%; 95% CI = [10.4, 16.4]) in custody showed two or more current, severe symptoms. Cognitive impairment, negative symptoms, and depression were most common of these problems. The majority of inmates 5,058 (58.9%, 95% CI = [54.6, 63.2]) showed no current, severe symptoms of a mental health problem.
More than half of sentenced and other inmates evidenced at least one current, severe symptom of a mental health problem, along with nearly one half (47.8%) of female inmates and almost three quarters (74.6%) of Aboriginal inmates.
Discussion
Based on the RAI-MH assessments, it is estimated that as many as 3,529 inmates or about 41.1% of the general population in Ontario correctional facilities, evidence current, severe symptoms of a mental health problem. The majority of inmates with a mental health problem showed one current, severe symptom (28.1%, n = 2,413), most often cognitive impairment or negative symptoms. A smaller number of inmates (13.0%, n = 1,116) showed two or more current, severe symptoms, with depression and negative symptoms most common. Other research (Andersen, 2004; Binswanger et al., 2010; Brink et al., 2001; Butler et al., 2006; Trestman et al., 2007) reports similar estimates of the overall prevalence of mental health problems in the inmate general population, in the range of 30% to 40%, or an even greater prevalence (James & Glaze, 2006; Lafortune, 2010). In the current study, the estimated prevalence of current, severe positive symptoms (3.6%) and depression (11.2%) is comparable with the findings reported by Fazel and Seewald in their 2012 international review.
Sentenced and other inmates were estimated to have a greater prevalence of any current, severe mental problem compared with remand inmates, though this result was complicated by the fact that in the Ontario correctional system sentenced and other inmates evidenced a shorter average time incarcerated compared to remand inmates; typically, the longer the period of time inmates are incarcerated before being assessed the less severe the symptoms, as they have had more time to adapt to imprisonment (Hassan et al., 2011).
Female inmates demonstrated a greater prevalence of current, severe mental health problems, and a higher number of severe symptoms compared to male inmates. Given the relatively small number of female inmates in Ontario’s jails and detention and correctional centers (596, or 6.9% of the total) spread across 16 facilities, the mental health assessment and treatment services provided to female inmates are likely to be “generic” mental health programs based on the needs of male inmates that ignore the unique circumstances of female inmates, and the greater severity of their mental health symptoms (Schizophrenia Society of Ontario, 2012). In Canada, the need for mental health services that address the problems of female inmates far outstrips the resources available (Leschied, 2011).
Aboriginal inmates were more likely to show more current, severe symptoms compared with non-Aboriginals. The lack of culturally appropriate assessment instruments and treatment programs, and general lack of knowledge about mental health problems among Aboriginal inmates (Butler et al., 2007; Daigle, 2007; Schizophrenia Society of Ontario, 2012) means that, like many disadvantaged minority groups in other countries (Brandt, 2012; Prins, Osher, Steadman, Robbins, & Case, 2012; Simpson, Brinded, Fairley, Laidlaw, & Malcolm, 2003), Aboriginal inmates are unlikely to have ready access to services that could be important in reducing their high rates of overrepresentation and recidivism in the Canadian correctional system (LaPrairie, 1996; Public Safety Canada, 2003).
Limitations of the Study
The current study employed a volunteer, nonrandom sampling strategy and inferences drawn from the sample data about the prevalence of symptoms of mental illness in the total population of inmates should be made with caution. Though the propensity weighting technique (Hirano & Imbens, 2001; McNiel & Binder, 2007) employed in the current study is considered a well-researched and widely-accepted statistical approach for estimating and adjusting samples for nonprobability bias of selection, still, estimates derived from the current study should be regarded with caution, and interpreted in light of findings from other studies. The estimate of the prevalence of inmates with current, severe symptoms of a mental health problem may also be negatively biased (too low) as the researchers were unable to access and assess the population of inmates (approximately 250) considered by correctional staff to be too physically or mentally ill, or too dangerous, to be safely assessed.
Although numerous studies have demonstrated the reliability and validity of the RAI-MH assessment tool, still self-report measures of psychiatric history and symptoms may inflate estimates of the symptoms of mental illness; however, in the current study, information obtained from the RAI-MH assessments was verified wherever possible against correctional and medical files of inmates, and attempts were made (n = 5) to assess interrater reliability in the current study.
At the same time, while a useful tool for assessing symptoms and estimating the prevalence of symptoms of mental illness in the population of inmates, a number of questions on the RAI-MH instrument proved difficult, if not impossible, to answer reliably in the correctional setting (e.g., meal preparation, shopping, wandering, misuse of medication, etc.). As a result, the researchers are pursuing an adaptation of the RAI-MH instrument tailored specifically for the correctional environment.
Conclusion
The substantial prevalence of current, severe symptoms of a mental health problem in the general population of inmates in Ontario correctional facilities is strong reason for public concern (Chaimowitz, 2012; Office of the Auditor General of Ontario, 2008, 2010). Although specialized mental health treatment units housing inmates with severe mental health problems are available within the Ontario correctional system, these units are already at or near capacity. Special Needs Units and infirmary beds located within larger jails, detention centers, and correctional centers are likewise already at or near capacity in addressing the needs of inmates with severe mental health problems, physical health needs, and other types of problems (Office of the Auditor General of Ontario, 2008). Though other forms of basic physical and mental health care are available in all correctional facilities, still more than 30% of the estimated 1,116 general population inmates demonstrating two or more current, severe symptoms scored “high risk/immediate need” on RAI-MH CAPs for mental health care, evidence of an urgent need for intervention (Hirdes et al., 2011). Given the proportionately higher number of severe symptoms among both female and Aboriginal inmates, and their lesser access to mental health services, there is all the more urgency to put in place appropriate mental health services for these inmates (Schizophrenia Society of Ontario, 2012).
Although correctional services in the province of Ontario, and more broadly throughout Canada, the United States and in other Western countries have made important strides in recent years to improve mental health services they provide to inmates, there remains a striking gap in the financial resources, and treatment programs and professional expertise required to address the needs of correctional inmates with severe symptoms of a mental health problem. Greater efforts must be made to bridge the gap between the correctional and mental health care systems to ensure that inmates in correctional facilities can access and receive appropriate mental health care services while incarcerated. Further research on the prevalence and mental health care treatment needs of inmates with severe mental health problems, including identification of specialized strategies to address the needs of female and Aboriginal inmates and other distinctive groups, will be important in supporting these efforts.
Footnotes
Authors’ Note
The conclusions expressed in this article are solely those of the authors, and do not represent the policies of the Ontario Ministry of Community Safety and Correctional Services or the Ontario Ministry of Health and Long-Term Care.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported with funding provided by the Ontario Ministry of Community Safety and Correctional Services and the Ontario Ministry of Health and Long-Term Care, and with data provided by the Program Evaluation and Applied Research (PESAR) Unit of the Ontario Ministry of Community Safety and Correctional Services. Hirdes’s participation was supported in part through the Ontario Home Care Research and Knowledge Exchange Chair funded by the Ontario Ministry of Health and Long Term Care.