
Abstract
The effect of music therapy on anger management and coping skills is an innovative subject in the field of forensic psychiatry. This study explores the following research question: Can music therapy treatment contribute to positive changes in coping skills, anger management, and dysfunctional behavior of forensic psychiatric patients? To investigate this question, first a literature review is offered on music therapy and anger management in forensic psychiatry. Then, an explorative study is presented. In the study, a pre- and post-test design was used with a random assignment of patients to either treatment or control condition. Fourteen participants’ complete datasets were collected. All participants received “treatment as usual.” Nine of the participants received a standardized, music therapy anger management program; the five controls received, unplanned, an aggression management program. Results suggested that anger management skills improved for all participants. The improvement of positive coping skills and diminishing of avoidance as a coping skill were measured to show greater changes in music therapy participants. When controlling for the exact number of treatment hours, the outcomes suggested that music therapy might accelerate the process of behavioral changes.
Although there is growing research in the field of forensic psychiatry, greater improvements and increased scientific understanding of specific treatment modalities for forensic psychiatric patients are necessary, especially regarding less conventional treatment modalities. Music therapy is an example of such a treatment modality; however, it is rarely researched scientifically in the forensic psychiatric field. Music therapy in this study is defined as the use of musical intervention grounded in cognitive-behavioral therapy (CBT) and based on best practice used to accomplish individualized goals of change or development in emotional, behavioral, cognitive, and social functioning within a therapeutic relationship (ArtEZ, 2009, based on the definition given by the American Music Therapy Association definition, 2005, and the Dutch Music Therapy Association, NVvMT, 2009). The objective of this study is to explore whether and which behavioral improvement occurs in inpatient forensic psychiatric patients due to music therapy.
Music Therapy in Forensic Psychiatry: Treatment and Research
As with the majority of the treatment programs within international forensic psychiatry, music therapy focuses on overt behavior and is assumed to affect a patient’s (re)actions in a well-defined and structured situation (Codding, 2002; Crimmins, 2010; Smeijsters & Cleven, 2004).
Music
Why and how could music be an effective treatment intervention for forensic psychiatric patients? The core assumption in the theoretical literature on the functions of music is that music is generally composed, or played, to express emotion (whether it be love, anxiety, sadness, fear, aggression, or anger), to trigger cognitions or to contain behaviors. Saarikallio and Erkkilä (2007) found that, beside entertainment, healthy adolescents use music to enforce relaxation, distract from certain emotions, energize a person, offer solace, or discharge emotions. Music can provoke sensory images within us, whether these are mild or strong. Music can help people to express, recognize, or sense inner (emotional, cognitive, physical, or psychological) motions that influence our daily life (Juslin, 2009). When making music, it can help express specific emotions and contain these emotions at the same moment. This we call the containing power of music.
Music can also be a vehicle to express or contain quite different personal emotions or social issues. Tentative issues in society can be conveyed through music. For example, in society the (verbal) expression of certain emotions (such as anger through aggression) is often condemned and perceived as negative—or even destructive (Lorber, 2004; Lowenstein, 2004). Music has the strength to help people experience and express feelings without acting them out in reality. The psychobiological strength of music stimulates human beings to apply music in their daily life to cope with emotional situations (Ter Bogt, Mulder, Raaijmakers, & Gabhainn, 2011; Thaut, 2005). So music can influence people, yet it has no therapeutic value by itself.
Music Therapy
Music therapy is the profession that systematically applies music’s psychobiological and containing power to influence people (Hakvoort & Dijkstra, 2012; Wigram, Pedersen, & Bonde, 2002). Insights from emerging scientific fields such as neurology suggest the effectiveness of music applied in therapy—as well as an explanation for these effects (Lin et al., 2011; Thaut, 2005; Thaut, Nickel, & Hömberg, 2004). If implemented therapeutically and systematically, music is a promising method to influence the neurological processes of human beings.
Promising are the results of Blood and Zatorre (2001), Esch and Stefano (2004), and Nistri, Ostroumov, Sharifullina, and Taccola (2006), who demonstrate neurological pathways that could be applicable in music therapy treatment for people who suffer from addiction problems. The explanation is that music stimulates brain processes that influence the production of specific endorphins in receptors (DRD2), a process that is severely impaired and damaged by, for example, the long-term use of psychedelic substances (Feltenstein & See, 2008; Stansfield & Kirstein, 2005). An average of about 70% of the forensic psychiatric patients in the Netherlands has a problem with substance abuse (Van Gemmert & Van Schijndel, 2011)
Cognitive-behavioral music therapy (Hakvoort & Bogaerts, 2013) is meant to help facilitate emotion regulation, which is a skill that is often taught in CBT with offenders and psychiatric patients. The music is used as a training situation. Skills, such as improving selective attention or asking for help that need to be developed, are trained and rehearsed, first under musical circumstances and subsequently in everyday life. The music is applied as training facilitator and as reinforce, as well as motivator. If the patient has sufficient cognitive skills, cognitive adaptations are stimulated through insight in (musical) functioning.
Cognitive-behavioral-based music therapy in forensic psychiatry centers on the basic principles as outlined in Bonta and Andrew’s (2007) “What Works” framework: the risk-need-responsivity model. Music therapy, here, focuses on minimizing risk principles and addressing the (treatment) needs of forensic psychiatric patients, although often this framework is implicit. Music therapy can specifically address the responsivity of the patients by becoming attuned to their musical interest. Treatment is based on need principles, such as building problem-solving, self-management, anger management, and coping skills, as well as reducing substance abuse behavior (Andrews, Bonta, & Wormith, 2006; Brand & Nijman, 2007; De Vogel, De Ruiter, & Bouman, 2007; Van Nieuwenhuizen et al., 2011).
A qualified and competent music therapist has the ability to create a specific stressful situation for a patient in a safe environment. This component is one of the major strengths of music therapy (Dijkstra & Hakvoort, 2010; Hakvoort & Smeijsters, 2006; Kluck-Walpot & Vink-Brouwer, 2006; Laansma & Riemke, 2006). During music therapy, a patient is confronted with several musical assignments that provoke his reactions. These assignments may mimic situations in real life. These situations can be everyday situations or very specific (stress-enhancing) situations (such as being rejected or having to meet one’s own or another person’s impossible expectations). Patients are placed in musical situations that demand a modification of their behavior. This condition enables patients to experience and demonstrate their capabilities and limitations to adjust to a new or stressful situation. A music therapist actively intervenes in this process and controls the music condition. During the music therapy, the music therapist addresses positive psychosocial and executive functions and enables the patient to apply and practice newly acquired skills.
Because patients perceive the music therapy situation to be “just about playing music,” they can reveal their typical coping and impulse regulation skills but do not become traumatized or engage in violent acts. Therefore, music therapy creates musical situations that are realistic and can be manipulated to evoke stress but do not threaten or harm the patient or the therapist. Especially when working on treatment goals directed toward anger management—a major problem for most forensic psychiatric patients—the act of making music can help forensic psychiatric patients practice new skills before they have to practice them in daily life (Hakvoort, 2002; Rickson & Watkins, 2003).
Case Example
In this section, an example of music therapy anger management in forensic psychiatry is presented to clarify some details in a treatment process.
Keith 1 is a 25-year-old man suffering from a Cluster B personality disorder, addicted to cannabis, with a verbal IQ of 74 and a performal IQ of 78. He was convicted for manslaughter of a drug-dealer whom he seemed to have stabbed in rage after a decline. Keith was sentenced to prison followed by treatment under the Entrustment Act (see “Participants” in the “Method” section). He has extreme aggression outbursts in which he destroys furniture in his room or at the unit or attacks staff members. He was referred to music therapy to work on his anger management skills. Keith was motivated to join, as the music therapist promised to help him write his own rap-text.
In the therapy, they first start searching for his favorite music and the ideal music to relax when he is agitated or angry. The music therapist places the music in an order from fitting angry states to fitting relaxation. She burns the music to a CD that Keith can listen to during music therapy. Consecutively, Keith receives psycho-education about stages in anger, aggression, and regulation. Due to his limited intelligence, this education is kept very simple, mainly consisting of rehearsing, cognitions like: “If I feel irritated, I have to leave the conversation.”
Second, the music therapist and Keith train relaxation skills during a number of sessions, while listening to, moving to and making music. If Keith is tense, head-banging and jumping (he calls it dancing) to music works well to regulate some of his extreme tension. When dancing, he often feels the urge to scream as well, so they compose his own rap-text for that moment. Rap music therapy is a specific treatment approach that addresses both the musical aspects (rhythm, dynamics) and expressive aspects, as well as lyrics (Hakvoort, 2008). The music therapist assists Keith in defining the content of his rap. It should match the situation he is in (tense, angry) and it should match his own accountability for the situation. The rap should be personalized to Keith to support his identity, but also simple enough to let him memorize it easily. In addition, they work on rhyme and rhythm. He is proud to write his own two-sentence text (translated from Dutch):
My name is Keith and through my own deed, I’m condemned to TBS,
2
which gives me a lot of stress.
They practice dancing and rapping the text to the music that best matches Keith’s angry state. After about 2 min of dancing and rapping, he gets tired. At that moment, he sits down and uses relaxation-to-music-breathing-skills to unwind. The next sessions they continue practicing, with the music therapist progressively withdrawing from the process.
The music therapist and Keith practice applying the CD, first during music therapy. After a number of run-throughs, the music therapist creates musical situations that trigger Keith’s anger. She encourages him to imitate her (too difficult) piano riffs. Every time he does not match her riffs exactly, she repeats the pattern a little louder and faster. She observes Keith’s anger rising during the musical assignment. Just before she estimates that he is about to lose control she reminds him of what he should do when angered. She assists him in putting on the music and dances along with him, initiates the rap-phase and is surprised to see Keith apply the relaxation-to-music-breathing-skill by himself. They repeat this pattern during a number of music therapy sessions, then let Keith practice it in his room (first supervised by the music therapist and then more and more independently). A large sheet of paper is taped to the inside of Keith’s door saying: Angry → shut the door → turn on the music → dance, rap → sit down on your bed → breath with the music → ring the bell if you are relaxed again.
On the unit, Keith first needs hints from the socio-therapists to apply his newly learned skills, but more and more often he withdraws to his room as soon as he becomes angry or extremely agitated and applies his anger management skills all by himself. His violent outburst has disappeared.
Anger
Anger is perceived as one of the dynamic risk factors for forensic psychiatric patients (Douglas & Skeem, 2005). Anger is thought to be an aversive emotion that can involve active approaches (Potegal & Stemmler, 2010) as well as passive resistance (Fernandez, 2013). According to Novaco (2010), “the central characteristic of anger in the broad context of clinical disorders is deregulation—its activation, expression, and experience occur without appropriate controls” (p. 485). Anger has paradoxical effects on the physical, cognitive, and emotional functioning of people (Lowenstein, 2004; Potegal & Stemmler, 2010). It arises as a “cognitive appraisal of wrongdoing and a tendency to counter or redress the wrongdoing” (Fernandez, 2013, p. 3). The emotion of anger is evoked in specific situations, which differ across individuals. Anger can have a physiological impact, both positive and negative, on cognition and behavior (Potegal & Stemmler, 2010). Under certain circumstances, impulses and tempers triggered by anger overrule cognitive functioning (Potegal & Stemmler, 2010). Probably all forensic patients have disturbed anger coping mechanisms. These mechanisms have developed over many years of disturbed anger management and susceptibility to feelings of wrongdoing (Fernandez, 2013). The way the forensic psychiatric patients handle their anger might then cause them to victimize others.
A cognitive understanding of the factors contributing to the offense of the patient alone is not enough to prevent relapse (Mann, Hanson, & Thronton, 2010), because a number of risk factors contribute to a violent act. Aggression might be a behavioral reaction fueled by anger, but it can also be thrill-seeking behavior (Averill, 1983). The patient has to come to the realization that he lacks coping skills that are common among his peers and that he often overestimates his ability to handle stressful situations (Bouman, De Ruiter, & Schene, 2003). Coping skills refer to a person’s cognitive, behavioral, and emotional adjustment to (changing) situations (e.g., Folkman & Lazarus, 1984; Folkman & Moskowitz, 2004). Negative coping skills (such as violent behavior) show a positive correlation with relapse into criminal behavior (Brand & Nijman, 2007). Subsequently, the patient has to practice and train newly acquired (coping) skills to master and apply them in real-life situations.
Music Therapy in Correctional Settings
Dijkstra and Hakvoort (2006) and Gallagher and Steele (2002) designed and implemented specific addiction treatment programs for forensic psychiatric patients and offenders with substance abuse problems. Music therapy is applied in the programs to trigger emotions and build both interpersonal and coping skills. Music assists the process of rehearsing and repeating the newly acquired skills. Rickson and Watkins (2003) designed a specific music therapy program to promote pro-social behaviors in aggressive patients, whereas Watson (2002) used drumming to improve social skills, pro-social behavior, and the ability to become aware of and manage emotions of sexual offenders. Hakvoort (2002) designed a specific music therapy anger management program tailored to the possibilities and limitations of forensic psychiatric patients.
Although music therapy is applied internationally to correctional settings, research on the influences of music therapy on inpatient forensic psychiatric patients is rare. The few research articles available are sometimes more than 20 years old or focus on qualitative case descriptions. These studies tend to explore emotional reactions (such as anxiety, anger, and tension as rated by the patients themselves) and rarely examine aspects such as coping skills or anger management as observed by staff. For example, Hoskyns (1995) observed an increase in positive self-perception and in the expression of emotions through music therapy in forensic patients. Thaut’s (1989) music therapy research indicated that patients expanded their coping skills after music therapy treatment. Patients showed improvements in the ways in which they reacted to fear and tension-arousing situations.
In a self-report research design, female inmates indicated that they felt more relaxed, experienced less stress, and could express themselves better after 12 music therapy sessions (Daveson & Edwards, 2001). Patients indicated that music therapy led to a decrease in stress, anger, and frustration. That research study suggests that music therapy can shift coping skills from mainly aggressive behavior to general acceptance.
Drieschner (1997) performed one of the few quantitative research studies of music therapy using forensic psychiatric patients in the Netherlands. He demonstrated that percussion improvisations had a positive physical effect on the anger management skills of forensic psychiatric patients. He compared percussion improvisations with the effects of solving a tangram puzzle.
At present, a number of research on music therapy with offenders have been initiated or completed. Gold et al. (2013) examined the influence of music therapy on the mental well-being of prisoners. Due to a very short average period of incarceration (62% of participants stayed less than 1 month), the positive results can only be met with caution. Currently, Chen, Hannibal, Xu, and Gold (2013) are repeating Gold et al.’s (2013) research in China. Even a Cochrane systematic data review on music therapy with offenders is in preparation (Protocol by Chen, Leith, Aarø, Manger, & Gold, 2014).
Objectives and Hypotheses
The objective of this study is to explore whether behavioral improvement occurs in forensic psychiatric patients due to music therapy by focusing on need factors: coping skills, and anger and aggression management. The study was conducted within four forensic psychiatric clinics in the Netherlands using five certified music therapists.
The research question was as follows:
The alternative hypothesis was formulated as follows: Music therapy interventions affect coping skills in a positive way (increasing positive reactions and decreasing avoidance coping reactions) and improve the anger management skills of forensic psychiatric patients.
Method
Participants
The Dutch forensic system is different from most forensic psychiatric systems in the world. If a suspect is found guilty but not—or only partially—accountable or culpable, a judicial court can pass a sentence of imprisonment followed by treatment under the Dutch Entrustment Act (TBS). The Dutch Entrustment Act is a judicial instrument embedded in the Criminal Code. It combines a prison sentence with confinement in a TBS-maximum security hospital (Van Marle, 2002, p. 83). 3 The idea behind this system is that a severe psychiatric disorder might influence the suspect to commit a crime. The main goals of the Dutch Entrustment Act are to protect society from these dangerous or psychologically disturbed offenders and to prevent the offender from relapse into violent criminal behavior.
The participants of this study were male forensic psychiatric patients. They were enrolled in the Dutch forensic system between August 2008 and December 2011. Of the 13 subjects who participated, 14 datasets where gathered, as one of them completed both control and subsequent treatment conditions. The average age of the 13 participants who completed the study was 35.6 years (ranging from 25 to 49, with a standard deviation of 8.9 years). They were selected if they had overall IQs over 75 and were within their first one and a half years of forensic hospitalization in the Netherlands. The severity of crimes ranged from armed robberies (with extreme violence), to (extreme) sexual assaults of women or children, to manslaughter. Participants were included if they did not suffer from schizophrenia or acute psychosis and had not been previously sentenced to TBS treatment. Twelve participants suffered from at least one personality disorder, more than 60% of whom suffered from Cluster B personality disorders (Diagnostic and Statistical Manual of Mental Disorders [4th ed., text rev.; DSM-IV-TR]; American Psychiatric Association [APA], 2000). One participant suffered from Asperger syndrome. Five of the participants did not come from Dutch cultural backgrounds. Eight of the participants had been addicted to psychedelic drugs (at least one; see Table 1).
Characteristics of the Participants.

Note. PD = personality disorder.
Of 21 persons who were invited to take part in the study, 6 refused to participate (3 of whom wanted to have music therapy treatment and made sure not to end up as controls on the waiting list). One experimental participant refused to participate in the post-test due to conflicts with unit staff. Treatment of one experimental participant was terminated early due to safety risks of the music therapist. Five participants completed the control condition and nine the experimental condition. As mentioned, one of the participants completed both conditions; see Figure 1. The only key difference found between the dropouts and those who completed the study was found in the participant who was rejected early from the study. He showed an extreme high score on the Psychopathy Check List–Revised (Hare, 2003).
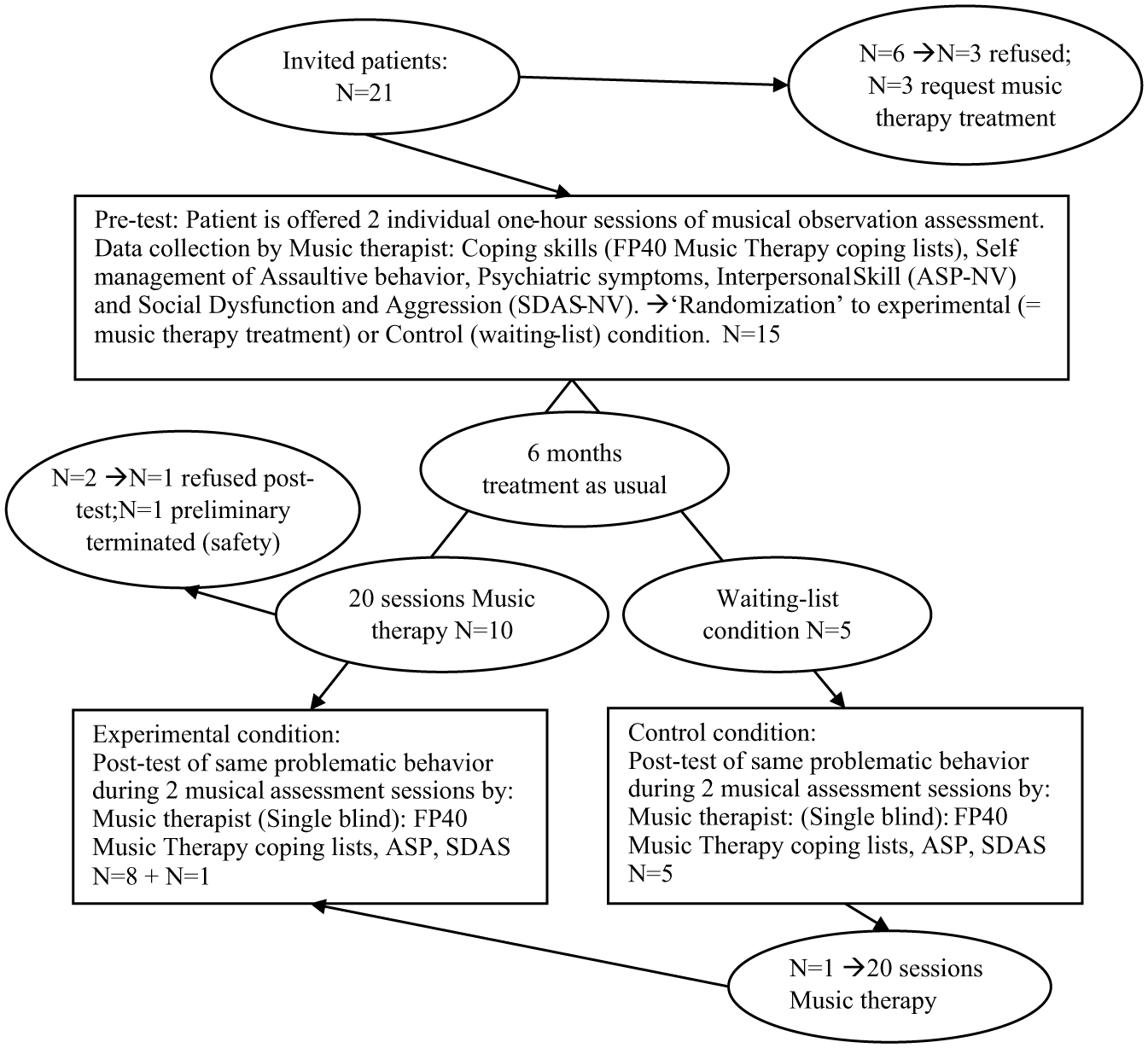
Research design per participant.
Experimental Design
This study was initially set up as a Randomized Controlled Trial (RCT; as approved by the Medical Ethical Committee of the University Medical Center of Groningen; Trial number METc 2008.099 ABR 20688). Due to major set-back (such as a huge decrease of newly enrolling forensic psychiatric patients in the Dutch TBS and the allocation of trained music therapist), only a small number of patients enrolled in the research. Although it might look therefore exaggerated, we nevertheless tend to meet the CONSORT statement (Schulz, Altman, & Moher, 2010) for clarity of the treatment procedure. In the study, a multi-center approach was introduced to prevent biases in the data resulting from a specific music therapist or a specific clinic. Music therapists in forensic psychiatry were selected based on their education, skills, and experience with cognitive-behavioral music therapy. They were trained on a standard protocol to assure similar interventions (see Standardized music therapy anger management program for more details). At the end, five music therapists from four forensic psychiatric clinics took part in the research.
A pre- and post-test design was conducted to measure coping skills, anger management and dysfunctional behavior. Figure 1 provides a schematic overview of the research design per participant. All participants took part in two musical observation sessions (Hakvoort, 2007). They were offered a standardized assessment including coping-exercises for the drum-set and piano by the music therapist. After these two sessions, the music therapist who led the sessions conducted an assessment of coping skills, anger (aggression), and dysfunctional behavior using different assessment tools: the pre-test.
After the pre-test, participants were randomly assigned to either the experimental or waiting list (control) condition by an independent researcher. This independent researcher was offered the birthdate of the participant. The last number of the day of birth would resemble music therapy (even) or control (uneven); music therapists were unaware of the randomization criteria and the researchers unaware of the date of birth. A patient who was assigned to the experimental condition was offered a standardized music therapy anger management program for twenty 1-hr-a-week individual sessions (see “Procedures”). Control participants (CS) received “treatment as usual” (without music therapy). Treatment as usual contains medical treatment, occupational therapy, recreational activities, and therapies (such as psychotherapy, art therapy, and addiction treatment). After their post-assessment, they could participate in the experimental condition, which one participant did.
After the 20-session treatment (equaling 6 months) or 6-month waiting-list period, a post-test that replicated the pre-test was conducted. Again participants were offered a standardized assessment including coping-exercises for the drum-set and piano by the music therapist. After these two sessions, the music therapist who led the sessions conducted an assessment of coping skills, anger (aggression), and dysfunctional behavior using the same assessment tools. These two musical observation assessments were videotaped and rated by the principle researcher (see results for inter- and intra-rater reliability). This person was not aware of whether a participant was assigned to the treatment or control condition (single blind data gathering), but was able to identify nine of the 14 participants correctly for their treatment condition after observing the videos. The principle researcher trained the music therapists how to score the observation lists, using video-excerpts of participants who were not involved in the study, whose video had been scored already by the observer or from participants who had withdrawn from the study (but who had agreed to the use their video for training purposes). Pre-set standards were formulated in a codebook. The number of reactions on a certain assignment was scored in percentages. Standards and criteria were set beforehand and refined during regular supervised meetings between the music therapists and the principle researcher.
Observation assessment tools were applied during pre- and post-tests (no self-reports). The tools included the Coping Skills List from the Forensic Psychiatric Profiles 40 (FP40), the Social Dysfunction and Aggression Scale (SDAS), and three of the Atascadero Skills Profiles.
The coping skills list from the FP40 (Brand, 2006) was applied to measure coping skills. The FP40 coping list measures positive coping (acceptance, humor, asking for help, positive actions), avoidance coping (ignoring, withdrawing, denying), and negative coping (threatening, violent acts). The scale ranges from one to three (1 representing “never” and 3 representing “during at least 50% of the displayed reactions”). The FP40 includes an observation scale for coping skills within forensic psychiatry. The inter-rater reliability was measured via Intra-Class Correlation Coefficient (ICC; Shrout & Fleiss, 1979). The inter-rater reliability varied between ICC .64 and .86 (Brand, 2006). The items of the FP40 were adjusted by the researcher to be able to observe coping behavior in music therapy. This adjusted score list uses the same scales as the FP40 coping list, but within different situational contexts (e.g., “handling failures at the unit” is replaced by “handling failures during music therapy”). The music therapist and the researcher who scored videos filled out the FP40 coping list for Music Therapy independently for both conditions.
Two lists were applied to measure anger management skills. First, the music therapist and principle researcher filled in three scales from the Dutch Version of the Atascadero Skills Profiles (ASP-NV; Vess, 2001; translated by researchers of the FPC dr. S. van Mesdag, 2004). Scale 1 measures self-management of psychiatric symptoms, Scale 4 measures the self-management of assaultive behavior, and Scale 9 measures Interpersonal Skills. The scales range from 0 to 4 (with 0 representing this skill is non-existing; 4 representing this skill is completely adequate). In the FSA-R-version created by Neville and Vess (2001), the Atascadero Skills Profile was determined to be reliable and valid for rehabilitation therapy (including music therapy), with reliability coefficients ranging from .87 to .98 for the entire instrument.
The second list to assess anger management skills was the SDAS (by Wistedt et al., 1990; Dutch translation by B. van der Werf, 1997). The SDAS includes 11 items of dysfunctional or aggressive behavior (such as scolding, suicidal thoughts, or threatening behavior). Each item is scored between 0 (= not present) and 4 (= severely present). The scores are added to determine a level of dysfunctional or aggressive behavior. The ICC of the SDAS was reported to be .97 (Wistedt et al., 1990).
The pre- and post-test included the same tests that were completed after the first musical observation sessions. The post-test was completed 6 months after the pre-test. To garner general information about the participants, we gathered background information from the Historical Clinical Risk–20 (HCR-20, developed by Webster, Eaves, Douglas, & Wintrup, 1995; translated by Philipse, de Ruiter, Hildebrand, & Bouman, 1999) and the HKT-30 (Werkgroep Risicotaxatie Forensische Psychiatrie, 2003) and a list for “Additional Treatments” (De Jonge, De Spa, & De Vos, 2006). Harte and Breukink (2010) calculated the HCR-20 reliability ICC score as varying between .49 and .82 (De Vogel & De Ruiter, 2005; Hildebrand, Hesper, Spreen, & Nijman, 2005). HKT 30 stands for the Dutch variation Historisch Klinisch Toekomst–30, as created by the Werkgroep Risicotaxatie Forensische Psychiatrie (2003). Its reliability ICC (Harte & Breukink, 2010) varied between .61 and .87 (Canton, van der Veer, van Panhuis, Verheul, & van den Brink, 2004; Hildebrand et al., 2005; Schönberger, Hildebrand, Spreen & Bloem, 2008).
Standardized Music Therapy Anger Management Program
In the treatment condition, patients were offered a standardized cognitive-behavioral music therapy anger management program tailored to the needs of forensic psychiatric patients. This program was created using a literature review and a forensic-psychiatric-music-therapist’s peer review (Hakvoort, 2002). The general goal of the music therapy anger management program is to train a patient to regulate and control his reactions to irritation or anger. The evaluative goal of the program is twofold. The program is considered to be completed successfully (a) if the patient is aware of and can manage at least two situations that trigger his anger and (b) if the patient can apply at least one new coping technique to diminish his anger. A number of sessions contain homework assignments to enhance the transfer of learned skills from music therapy to daily life.
The music therapy contains four stages. During the first stage, the patient is introduced to different aspects of anger management and relaxation, while making music and listening to different styles of music. In addition to becoming familiar with the music therapy environment, the patient’s therapy also focuses on treatment conditions (security and safety; in the case of Keith, he listened to music and is asked for (style) favorites). During the second stage, the patient learns techniques to reduce tension and receives psycho-education on discerning the different phases of anger (Keith practiced dancing, rap, and relaxation exercises). During the third stage, the patient’s awareness of specific stressors is enhanced. He discovers at least two specific situations that arouse anger/aggression and is able to label at least one “explosive” condition. During this phase, he is instructed to use techniques from the second phase to reduce tension (in the case example, the music therapist triggers Keith’s anger in this third stage by provoking Keith’s feelings of failure; she then assists him in using the newly trained skills). During the last stage, the patient learns to apply personalized techniques independently to manage stressful situations and alleviate his anger (Hakvoort, 2002). Patients participated in assignments such as imitating the drum patterns of the music therapist (which got too difficult to repeat after a while), improvising while the music therapist provides a boring accompaniment or one without any structure.
The anger management program is offered on an individual basis. All sessions take place in a music therapy room, equipped with a variety of instruments, including drums, piano, keyboard, computer with music programs, (bass) e-guitar, at least one drum-set, microphones, a PA system and a high quality stereo-set.
The music therapy program is outlined in a music therapist’s manual. The manual describes each session’s objectives, the mandatory and suggested assignments and the musical attitude or roles of the music therapist during each session. Music therapists underwent a specific training course that focused on the assessment of coping skills as well as executing this anger management program. In addition to this training program, music therapists were supervised to provide uniformity during the treatment program and scoring procedures.
Statistical Analysis
Only 14 participants were included in our study due to the low enrollment of newly admitted patients. The mean values found between the pre- and post-tests were plotted on graphs. Outcome measures in this study represent the outcome scores of the pre-test subtracted from the post-test of the SDAS, ASP-NV, and the FP40 coping list for music therapy. A nonparametric Wilcoxon matched-pairs signed-ranks test was performed on the mean change scores of each condition to look for differences. This action can be justified because we used a standardized intervention, implemented a randomization of data, and aimed for single blind data. A t-test was used to calculate the means and standard deviations of the changes in the CS and the participants in the music therapy treatment condition (MTC). The outcomes are presented in the following figures. We did not expect significant changes (p < .05), and hoped for positive tendencies (as formulated in the alternative hypothesis).
To offer more insight into the individual responses of patient, the treatment was also tested employing an additional N = 1 statistical approach as discussed in Spreen, Timmerman, Horst, and Schuringa (2010). This specific N = 1 approach is developed to support decisions about an individual patient’s progress during treatment and can also be employed to test the effect of an individual therapy. In this approach, a team of observers rate different relevant behavioral indicators. Depending on the treatment situation, a patient can be observed by a team of therapists. Each observer assigns a value on indicator “Anger.” The statistical decision test is as follows: for each indicator (or item or scale), all given values of the observers are joined between two measurement moments. For instance, observer X gives a 6 on “Anger” and observer Y a 7 at the first measurement. At the second measurement, observer X gives a 7 and Y an 8. To decide whether the patient has improved, all combinations of values of both observers between the two measurements are subtracted from each other. All positive differences are summed and divided by all combinations. This way the percentage positive and negative change according to the observers is computed. From a simulation study, 4 where this percentage positive change was compared with simulated RCTs, cases with a positive change percentage of 67% or more had a high probability (.95) to be classified in the experimental group of the RCTs. The results for each patient are plotted. Above the axis is the number of increased behaviors, below the axis the number of decreased behaviors. Small rectangles imply hardly any changes. The significant level for change is calculated to be 67% or higher for N = 1.
Results
The sessions were scored by the music therapist and the principal researcher to check for inter-rater reliability (watching video registrations). The overall inter-rater reliability was good (Cronbach’s α = .80, with a range from .23 to .95). The intra-rater reliability after a 2-week interval was satisfactory (Cronbach’s α = .78, with a range from .24 to .92).
Coping Skills
Avoidance coping skills
As presented in Figure 2a, the mean (M) scores of CS for avoidance coping skills did not differ significantly from the mean scores of participants in the MTC during pre-test (control: M = 1.96 and treatment: M = 1.86). During the post-test, the participants from the treatment group showed a larger mean decline in avoidance coping skills than the CS (control: M = 1.94 and treatment: M = 1.52).
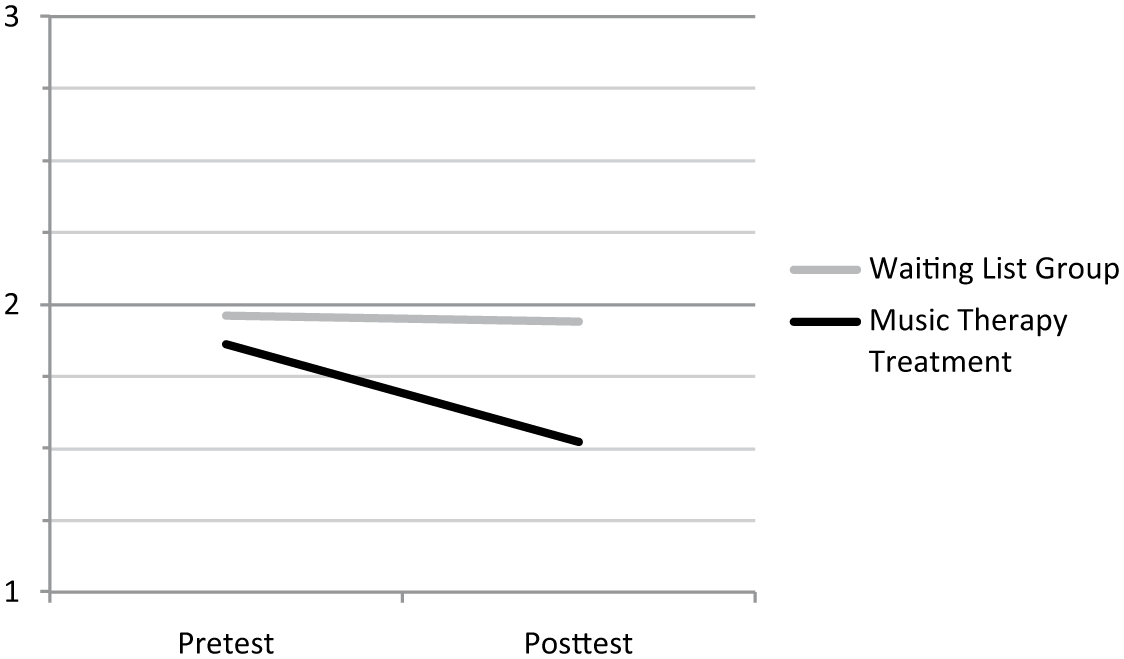
FP40 avoiding coping skills.
The mean outcomes show quite a distinct pattern (of decreased avoidance for the music therapy condition), which does not show up in the Wilcoxon. To enable the reader to better compare the outcomes, a N = 1 graph was added for each single participant in Figure 2b. The letters assigned to each participant are randomly picked. Most patients seem to show a decrease in the number of applied avoidance skills. For most patients, it is a positive sign. However, for some patients it is positive if they learn to apply more avoidance skills. Therefore, it is hard to judge the exact outcome.
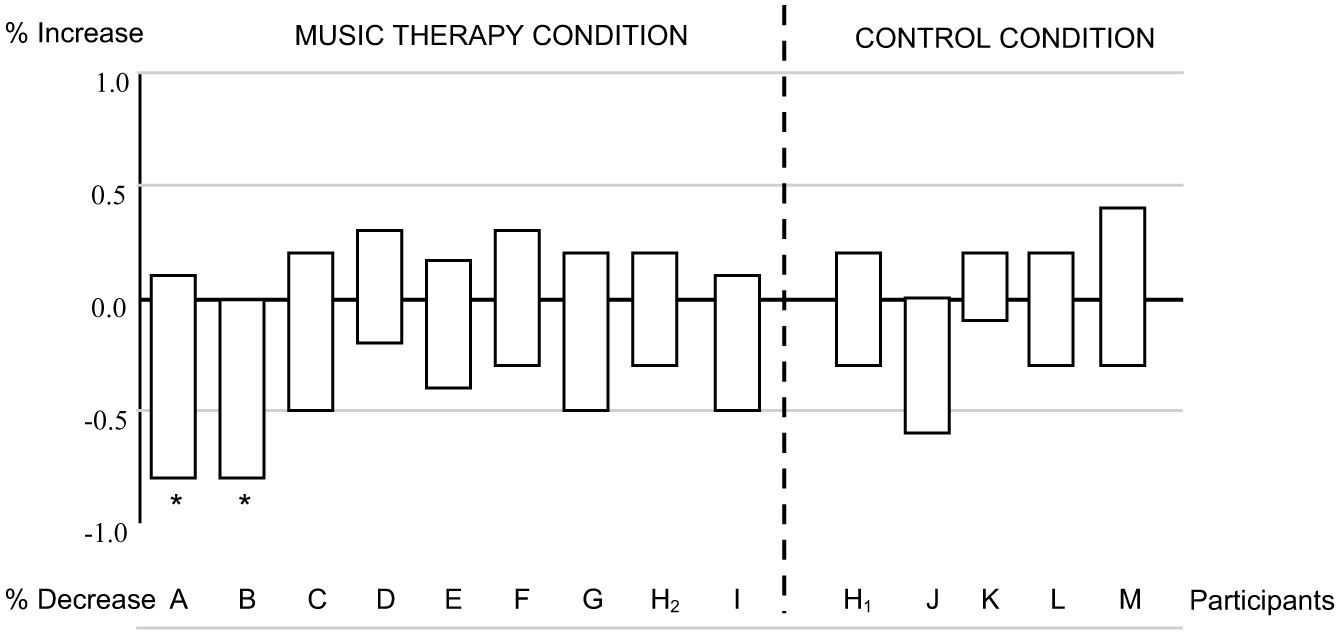
N = 1 of FP40 avoiding coping skills.
Positive Coping Skills
The mean values of positive coping skills for the participants in both the control and treatment conditions did not differ significantly at the pre-test (control: M = 1.76 and treatment: M = 1.68). Only the MTC showed a substantial increase in the use of positive coping skills (control: M = 1.77 and treatment: M = 2.13), as shown in Figure 3a.

FP40 positive coping skill.
To investigate whether this result could be subscribed to specific outliers, an additional N = 1 boxplot for each single patient was added in Figure 3b. Here, we can see that Participant B (and A probably too) seems to influence the significance level. Other participants show quite similar patterns of change under both conditions.

N = 1 of FP40 positive coping skills.
Negative Coping Skills
No changes occurred in terms of negative coping for all participants, as very few participants demonstrated negative coping behavior during music therapy. Therefore, the results are not displayed in a figure.
Anger Management Results
Social dysfunction and aggression
The SDAS reflected a similar pattern of no change for both CS and music therapy treatment participants (see Figure 4). Average dysfunctional behavior and aggression were from the start extremely low (control: M = 2.6 and treatment: M = 2.56 at pre-test; on a scale of 0 to 22) and changed little during the post-test (control: M = 2.4 and treatment: M = 2.56). On an average, we can assume that participants who volunteered to enroll in the study showed little dysfunctional or aggressive behavior or negative coping skills during music therapy.
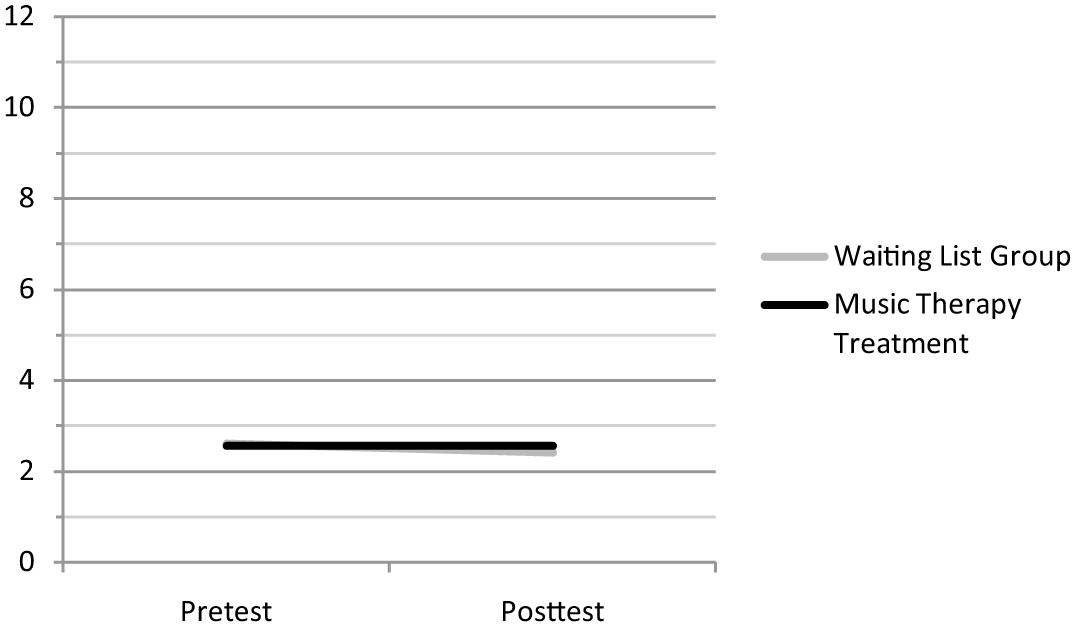
Social dysfunction and aggression.
Self-Management of Assaultive Behavior
If one examines the Atascadero Skills Profile and focuses on the skills needed to manage assaultive, aggressive behavior (Figure 5a), participants in the control and the MTC showed low ratings on these skills in the pre-test (control: M = 1.31 and treatment: M = 1.78). Both the controls and the music therapy participants seemed to have improved those skills at post-test (control: M = 2.01 and treatment: M = 2.51).
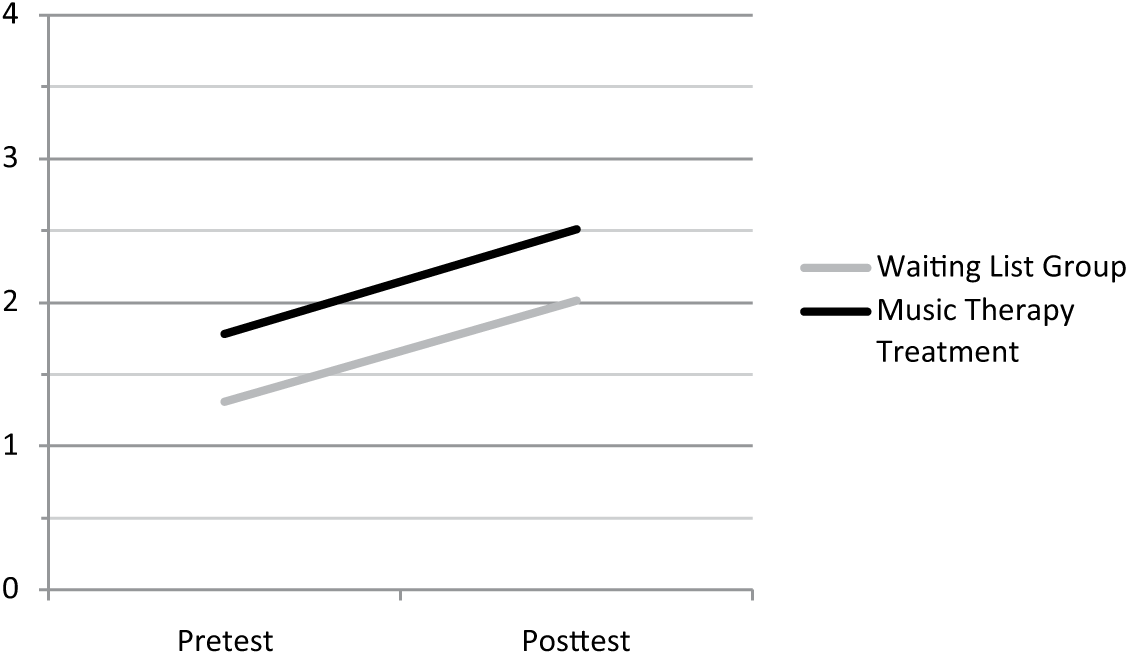
Self-management of Assaultive Behavior (ASP, Scale 4).
The difference in pre-test score is a coincidence in random assignment. Due to the small N, it is not possible to tell whether the differences have a specific meaning. The fact that the participants enrolled in music therapy condition showed fewer interpersonal skills might have been compensated by the higher management skills of assaultive behavior. As the scores of all other observations start pretty much on the same level, this difference can be due to one outlier as can be seen in Figure 5b.
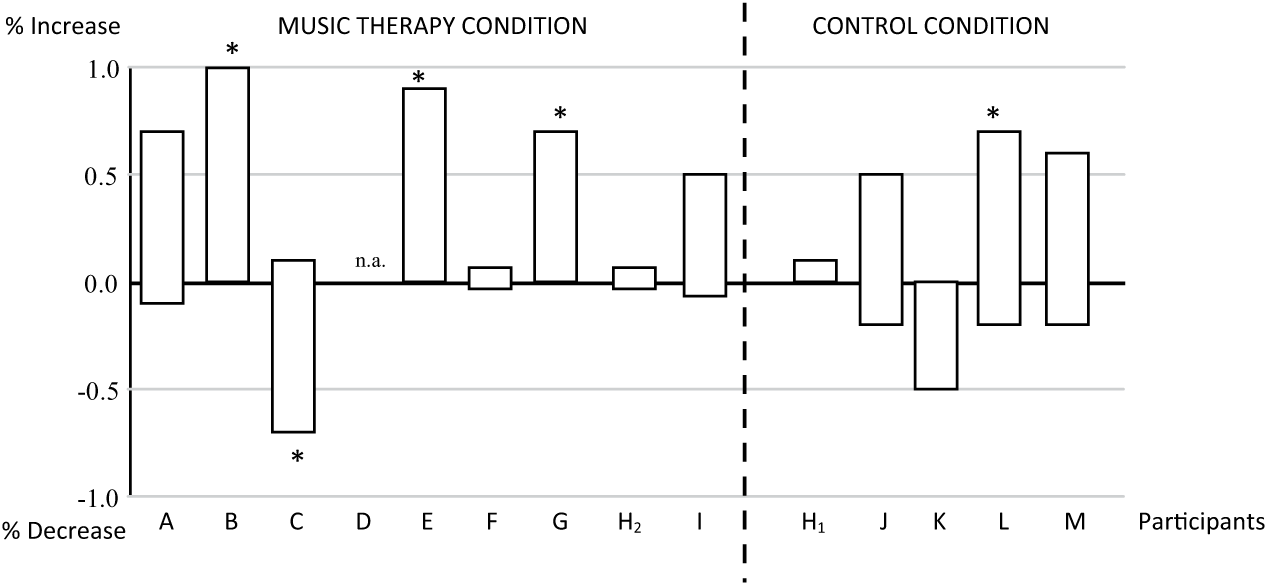
N = 1 of Self-management of Assaultive Behavior (ASP, Scale 4)
Figure 5b provides us with some insight into the changes that occur per participant. Some participants show (significant) improvement and others became significantly less capable of managing their assaultive behavior.
Other Results
Self-management of psychiatric symptoms seems to increase after 20 music therapy sessions (treatment: pre-test M = 1.76, post-test M = 2.42) compared with the stagnation as observed in the CS (control: pre-test M = 1.87, post-test M = 1.87). Figure 6 shows a graphic representation. This result merely reflects a general tendency of more cognitive understanding, and is not a significant result.
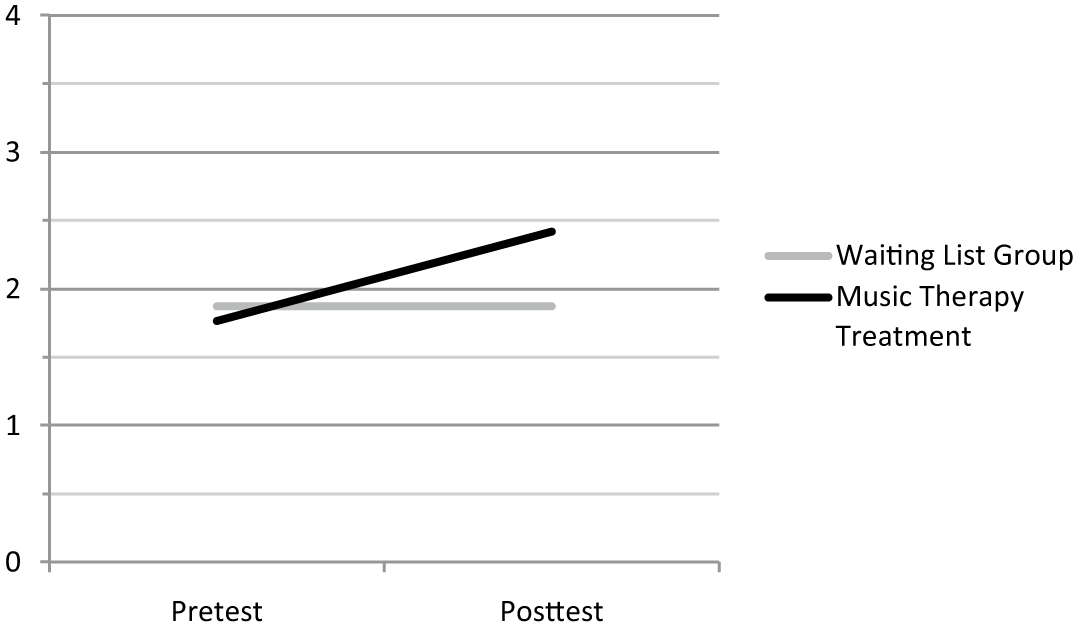
Self-management of Psychiatric Symptoms (ASP, Scale 1).
As shown in Figure 7, music therapy also had a positive influence on the mean outcome of the participants who completed the Atascadero Interpersonal Skills profile. CS hardly improved their skills (control pre-test M = 2.57, post-test M = 2.62), while those in the music therapy treatment group showed an improvement of interpersonal skills (Treatment Pre-test M = 2.35, Post-test M = 2.76).
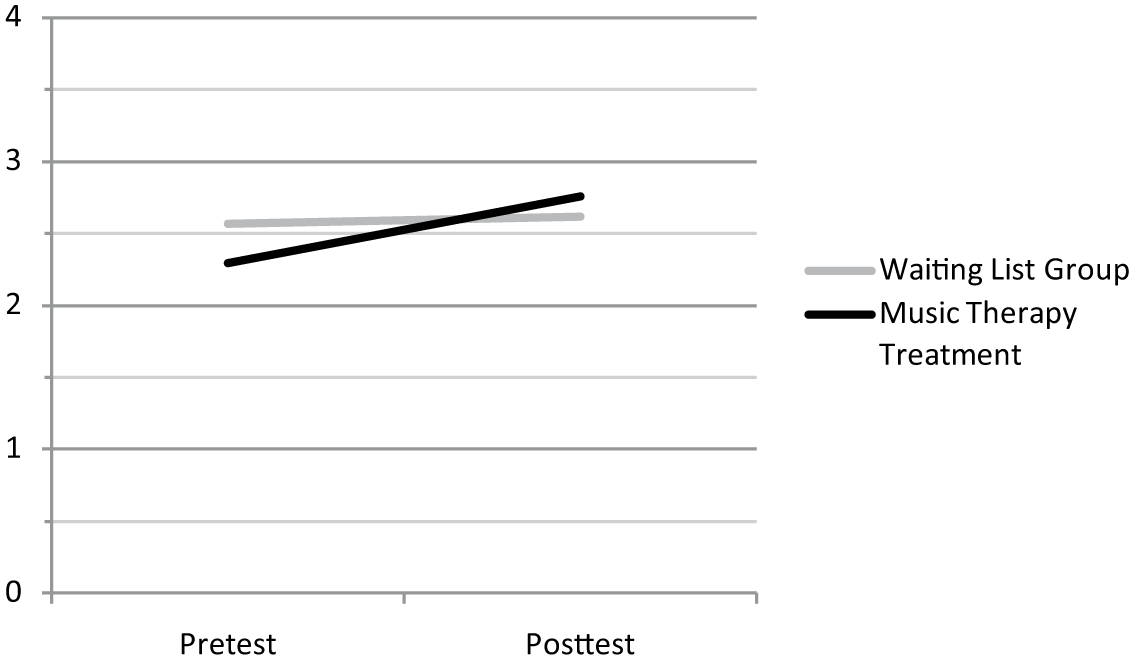
Interpersonal skills (ASP, Scale 9).
As the N of the study is small, the statistical power of the research is weak (for the N = 14), and a low effect size (d = 0.3) the statistical power = 0.12, with a higher effect size (d = 0.8) the statistical power is still small = 0.53). All results therefore have to be treated with the highest probable caution.
A remarkable difference was observed when participants were controlled for their exact number of treatment hours (excluding leisure or occupational activities). Those in the music therapy condition received an average of 4.1 therapy sessions (including 1 hr of music therapy) per week, with an average of 4 hr and 45 min. CS received an average of 4.4 therapy sessions a week, with an equivalent of more than 6 hr, thus considerably more hours of treatment per week than those in the experimental condition. The reason for the difference in hours is that most participants in the control condition coincidently received Aggression Management Group Therapy (including psychomotor therapy and verbal psychotherapy with two therapists in a group of three to four patients) for 3 hr a week, while the music therapy participants received individual Music Therapy Anger Management training for 1 hr a week. So, the number of treatment hours differed. Music therapy participants received almost 1.5 hr less therapy than the controls.
Discussion
Changing a disturbed anger coping mechanism consists of hard work and repetition of newly acquired skills, especially when dealing with personality disordered offenders and offenders with severe mental illness. This conclusion furnishes an important critique on the effectiveness of anger management programs in general (Glancy & Saini, 2005; Howells et al., 2002; Koerner, 1999).
The primary, tentative results of this study may help determine whether a specific music therapy treatment could improve coping skills and anger and aggression management in a small group of forensic psychiatric inpatients. The following hypothesis was formulated: Music therapy interventions can affect coping skills in a positive way (increasing positive reactions and decreasing avoidance coping reactions) and can improve anger management skills of forensic psychiatric patients. This explorative study shows no hints that the hypothesis should be rejected, but there is no statistical evidence to support it either. From the Wilcoxon test, one significant change score for positive coping skills was found. With multiple testing on a single, very small dataset, however, Type I error might have occurred here as well.
Cognitive-behavioral music therapy could have a positive effect on coping skills. Participants who were assigned to the music therapy experimental condition tended to use more positive coping skills when compared with those in the control condition, although this differed among participants. This could mean that the music therapy participants more often accepted a situation, asked for help, or demonstrated appropriate behaviors.
Changes in avoidance coping skills differed slightly among control and experimental groups. The latter seemed to have less of a need to withdraw from social situations or deny that something difficult was happening. These are important skills to learn when examining the “need” principles of Bonta and Andrew (2007). Brand (2006) and Brand and Nijman (2007) argued that need factors, such as coping skills, can prevent relapses into violence.
One interesting side effect was observed. Participants who enrolled in music therapy had the tendency to improve their insight into their psychiatric symptoms and how to cope with their limitations, although they received fewer actual hours of treatment. Music therapy seems to increase the insight and cognitive awareness of forensic psychiatric patients regarding how to cope with their psychiatric problems under stressful situations.
For all participants, there was a small growth in management of assaultive behavior; treatment seems to influence their management skills. Descriptive differences in means were compared checking against randomness, to measure a tendency for improvement in coping and anger or aggression management behavior. These findings support the findings in the previous literature about behavioral improvements of forensic psychiatric patients who participated in treatment programs (e.g., Andrews & Bonta, 2010; for the Netherlands: Brand & Nijman, 2007, Chakhssi, De Ruiter, & Bernstein, 2010; De Jonge, Nijman, & Lammers, 2009).
Most of the CS received a 3-hr per week aggression management training session. The experimental participants received fewer hours of treatment and yet made the same progress (or on individual bases even better). The difference in treatment (music therapy vs. aggression management therapy) was not intended but arose spontaneously (the staff most likely decided that if participants received music therapy, they did not yet have to enroll in the aggression management group). Only one treatment participant (H) received both—first aggression management training and later the music therapy. Yet, he showed hardly any changes during both conditions. Because almost all participants had a low score on social dysfunction and aggressive behavior, we might be dealing here with a “floor effect.”
Changing years of inadequate anger management is difficult with forensic psychiatric patients. Getting enough participants enrolled in a clinical setting is even more difficult. But those are certainly not the only limitation of this study. The number of patients enrolled in this study was too small for a statistically significant answer to the research question. Although numerous efforts were placed upon enhancing the number of enrolled participants, many (mostly external) factors influenced the fact that only five music therapists could deliver the complete 14 datasets from a total of 13 participants (for details, see Hakvoort et al., 2011). Due to this small N, the results of individual participants are not compared with their background information, such as the type of offense, impulsivity, substance abuse, aggressive behavior, concurrent or former (medical or psychological) treatment, intelligence, personality disorder, and other information. The offenses for which the participants were sentenced do not prove an origin in anger-provoked behavior for all of them; we are not sure whether their risk principles were anger-related behaviors.
There is no validated music therapy observation instrument for forensic psychiatric patients, let alone one that measures coping skills. The Atascadero Skills Profile has never been tested for its separate lists. Validity is therefore probably weak. The research design was intended to test the FP40 coping lists for Music Therapy for reliability using the data from the FP40 coping lists for socio-therapy. However, the data collected at the living unit by socio-therapy for coping skills were too often incomplete or even lacking to use for a reliability check. Inter-coder reliabilities for socio-therapy even showed negative results. So, the data gathered for comparison were all from the music therapy assessment situation. In the post-test, the participants in the experimental condition had 20 sessions of music therapy experience. They knew the music therapist better and might have been more relaxed for a camera videotaping them. Results can be influenced through that procedure.
To find out whether music therapy might have a positive effect, further research has to be carried out. The music therapy anger management program could be more cost-efficient compared with the group aggression management treatment, depending on the number of patients and therapists enrolled in, for example, group aggression management treatment. Whether it could increase forensic patients’ positive coping skills, decrease avoidance coping skills, or offer them a better understanding of how to manage their psychiatric symptoms has to be explored in further research. Other tests might be applied to screen patients beforehand for anger management problems; selecting those with higher scores on dysfunctional behavior (higher risk factors) might influence the results as well.
We are dealing here with a selection effect as well. Not all invited patients were willing to participate. Those patients interested in treatment might be more eager to participate in research than those who are completely unmotivated or suffer from anger-provoked passive resistance. All the participants volunteered; therefore, it could be likely that no difference between treatment and control groups was found. Music therapy seemed to appeal to the responsivity of the patients (as three of them refused to partake in the study to ensure not ending up as controls).
This exploratory study offers a starting point or can function as a pilot for future, larger scaled research studies on the influence of music therapy on coping and anger management skills in forensic psychiatric patients.
Footnotes
Acknowledgements
The authors would like to acknowledge M. Groen (FPC Oldenkotte), D. Kruidhof (FPC Oostvaarderskliniek), G. Roefs (FPC Kijvelanden), E. Smit, and M. van Veen (FPC Veldzicht) for their knowledge, skills, time, and effort as music therapists in this study.
Authors’ Note
This study is part of PhD research at Tilburg University, The Netherlands.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors are grateful for the research funds provided by ArtEZ, the Institute of the Arts, Enschede and Forensic Psychiatric Center Oostvaarderskliniek, Almere, The Netherlands.