
Abstract
This study examined the New Perspectives Aftercare Program (NPAP) for serious juvenile and young adult offenders in The Netherlands. Participants (n = 127) were randomly assigned to NPAP (n = 66) or existing aftercare services (“treatment as usual” [TAU], n = 61). The aim was to determine whether NPAP was effective in decreasing cognitive distortions and criminal thinking patterns and increasing prosocial skills of the juveniles compared with TAU. No direct intervention effects were found on any of the outcome measures. Moderator analyses, however, showed several interaction effects of ethnicity and coping skills for both NPAP and TAU youths. Furthermore, NPAP dropouts displayed significantly more indirect aggression at posttest compared with youths dropping out from TAU. Possible explanations for the mostly null effects are discussed, including implications for further research, policy, and practice.
Young people who reenter society after release from a correctional facility are confronted with many problems, often resulting in a relapse to delinquent behavior. It appears difficult for juveniles and young adults to reenter society after a period of detention and to change their lives of crime and become responsible, law-abiding citizens (Snyder & Sickmund, 2006). Work, schooling, and the support that family, friends, and other important persons provide often have ended during detention, which makes successful rehabilitation difficult (Mears & Travis, 2004). The challenge of changing life is even more difficult for juveniles and young adults, as they are facing both the transition from their detention facility to the community and, simultaneously, the transition from adolescence to adulthood, which has its own specific challenges (Travis, Solomon, & Waul, 2001). The cognitive capacity and life skills of adolescents and young adults differ from those of adults, and they are still going through the developmental stages of identity, moral, and social development until approximately the age of 25 (Arnett, 2000; Grisso & Schwartz, 2000; Zimmerman, 2005).
How juveniles and young adults fare post-release has become a critical criminal justice policy issue (Ministry of Justice, 2003; Office of Justice Programs, 2002). Consequently, interest in aftercare for juvenile and young adult offenders has grown remarkably over the past two decades, and more reentry and aftercare programs have been developed and provided for offenders released from detention (Altschuler & Armstrong, 1994, 2002; Mears et al., 2004; Ministry of Justice, 2003). Research has shown that chances of successful reintegration improve when the transition from correctional facilities to the community is directed and supervised (Fagan, 1990; Goodstein & Sontheimer, 1997). Jarjoura (2000) argued that if youths stay out of trouble in the first few months after release, their chances of maintaining work, reaching their academic goals, and developing an independent lifestyle increase. A reentry or aftercare intervention could therefore promote successful community reintegration and reduce repeated offending by youths released from juvenile correctional facilities, according to Altschuler and Armstrong (1994).
A recent meta-analytic review on aftercare programs for juvenile and young adult offenders (James, Stams, Asscher, De Roo, & Van der Laan, 2013) showed that relatively few aftercare programs have been accompanied by robust scientific research and most studies focus on recidivism outcomes only, while improvement in criminogenic needs and psychosocial functioning seem equally important, as those factors need to be changed to prevent future relapse (Andrews & Bonta, 2010). Aftercare programs aim to address criminogenic needs at different levels of the juvenile’s functioning, with a focus on the individual and/or family. The meta-analytic review further showed that aftercare programs for juvenile and young adult offenders are most effective if they are well-implemented and consist of individual instead of group treatment, and if they are aimed at older and high-risk youth.
The New Perspectives Aftercare Program (NPAP) seems to be a promising aftercare intervention in The Netherlands, because it includes all the characteristics (multifaceted, community-based, and offender-focused) that are generally recognized as features of effective interventions aimed at positive behavioral change and recidivism reduction in juveniles and young adults (Altschuler et al., 1994; Lipsey, 1992). First, NPAP is based on the risk–needs–responsivity (RNR) model, focusing on moderate- to high-risk juveniles, targeting their criminogenic needs and responsivity, that is, tailoring the intervention to the learning style, motivation, abilities, and strengths of the individual offender (Andrews, Bonta, & Hoge, 1990). Second, Crick and Dodge (1994) developed a social information processing model explaining aggressive and delinquent behavior. By systematically challenging distorted social information processing, further aggressive behavior can be prevented. In addition, the coping-relapse model (Brown, St. Amand, & Zamble, 2009) is applied. All the youths’ personal and contextual factors influencing their delinquent behavior are carefully mapped, and functional behavior assessments provide the youth insights in their cognitions and behavior, ultimately intended to lead to positive behavioral change. Furthermore, NPAP incorporates general treatment principles, by stimulating the therapeutic alliance and treatment motivation of the offenders (Wampold & Brown, 2005).
In short, NPAP targets specific criminogenic needs, such as criminal thinking patterns, cognitive distortions, prosocial (coping) skills, which have been shown to have a significant impact on delinquency (Andrews & Bonta, 2010; Lösel & Beelmann, 2003; Nas, Brugman, & Koops, 2008; Philips & Lindsay, 2011; Rokach, 1997, 2000) and will be briefly described below. First, a pro-criminal attitude toward committing crime is one of the most important predictors of delinquency and recidivism (Andrews & Bonta, 2010). Pro-criminal attitudes are thoughts, feelings, and beliefs that promote criminal and aggressive behavior, and which are characterized by distrust of authorities (e.g., police and judges), perceptions of the world as hostile and unsafe, adoption of aggressive behavior, and identification with criminal peers (Andrews et al., 2010; Golden, 2002; Granic & Butler, 1998).
Second, an important focal point of NPAP is cognitive distortions. Barriga and Gibbs (1996) distinguished primary cognitive distortions, referring to self-centered attitudes and beliefs, from secondary cognitive distortions, which can preserve the self-image of the juvenile after an antisocial act and can be split up in three categories, that is, blaming others, minimizing/mislabeling, and assuming the worst. Research shows that both types of cognitive distortions are related to aggressive and delinquent behavior (e.g., Helmond, Overbeek, Brugman, & Gibbs, 2015; Lardén, Melin, Holst, & Långström, 2006; Wallinius, Johansson, Larden, & Dernevik, 2011). Studies show that juvenile delinquents tend to have more cognitive distortions than their non-delinquent peers (e.g., Barriga, Landau, Stinson, Liau, & Gibbs, 2000; Liau, Barriga, & Gibbs, 1998; Wallinius et al., 2011).
Third, NPAP focuses on coping strategies. There is evidence showing that individuals who commit crimes underuse healthy and effective coping strategies when they face demands (Quinsey, Harris, Rice, & Cormier, 1998; Rokach, 1997, 2000; Rokach, & Cripps, 1998; Zamble & Porporino, 1988, 1990). This has also become apparent in individuals who reenter society after a period of incarceration (Philips & Lindsay, 2011). Therefore, the development of healthy coping strategies, a goal of NPAP, may decrease an individual’s odds of returning to a life of crime.
Fourth, a focus of NPAP is the development of social skills, which includes the ability to “execute verbal and nonverbal behaviors that maximize the likelihood of goal attainment and the maintenance of good relations with others” (Bedell & Lennox, 1997, p. 9). Studies have shown that poor social skills are related to antisocial behavior (Beauchamp & Anderson, 2010; Lösel & Beelmann, 2003). Improving social skills can therefore steer one away from incremental involvement in delinquent behavior.
It is remarkable that most studies into aftercare programs only examine recidivism data. To be able to determine whether aftercare indeed successfully targets those factors that are associated with delinquent behavior, it is important to also address criminogenic needs in effectiveness studies (Andrews et al., 2010; Bergseth & McDonald, 2007). Although changed knowledge and attitudes do not necessarily lead to changes in behavior, there is some evidence that it can have an impact on subsequent criminal behavior (Friendship, Blud, Erikson, Travers, & Thornton, 2003).
Therefore, the present study seeks to fill a gap in the research literature on secondary outcomes of aftercare and examined conditions for changing a delinquent lifestyle, such as criminal thinking patterns, cognitive distortions, aggressive behavior, and prosocial and coping skills to evaluate the effectiveness of an aftercare program for juveniles and young adult offenders. Hence, the aim of the study was to examine whether NPAP produces outcomes that are superior to the existing services (“treatment as usual” [TAU]) by means of a randomized controlled trial (RCT). The primary outcomes were the criminogenic needs targeted by NPAP measured before and immediately after NPAP or TAU (short-term effectiveness), because all are supposed to be related to the risk of recidivism. A second aim was to examine the moderators of the effectiveness of NPAP, because the aftercare program might work for some participants, but not for others (Kraemer, Wilson, Fairburn, & Agras, 2002). The choice of moderator variables that were added a priori was guided by prior literature on moderators of intervention outcomes and risk factors for recidivism of juvenile and young adult offenders after release from a secure care or detention facility (Altschuler & Armstrong, 2004; Andrews & Bonta, 2010).
First of all, the number of prior offenses and the distinction between the number of violent and non-violent prior offenses were included as potential moderators of program effectiveness, given that history of criminal offending is one of the most important (static) risk factors for reoffending in delinquent youth (Andrews & Bonta, 2010; Grieger & Hosser, 2014).
Second, an important static risk factor for recidivism is age at first arrest (Loeber & Farrington, 1998), which was therefore included as a moderator. Various studies have shown that offenders with an early onset of antisocial behavior are more likely to continue with their delinquent behavior into (young) adulthood and turn into serious and chronic offenders than offenders with a late onset of offending behavior (Nagin, Farrington, & Moffitt, 1995; Tolan & Thomas, 1995).
Third, ethnic minority status might influence program effectiveness. There is empirical evidence showing that ethnic minority groups are over-represented in the population of juvenile delinquents and youth care globally (Blom & Van der Laan, 2006; Junger, 1990; Snyder et al., 2006). Whether clients of ethnic minority groups should be treated with the same methods and interventions as the majority population of a particular country has been much discussed, and studies have shown equivocal results (De Anda, 1997; van der Put, Stams, Deković, Hoeve, & van der Laan, 2013; Wilson, Lipsey, & Soydan, 2003). By including ethnic minority status as a moderator, we can establish whether the aftercare program can be offered to both groups regardless of their ethnic background.
In addition, age of the offenders was included as a moderator, because prior research on aftercare programs has shown that interventions are more effective when aimed at older youths (James et al., 2013), likely because of their readiness for change connected to their moral, social, and identity development, which continues into young adulthood (Arnett, 2000).
Another possible moderator of the effectiveness of NPAP was whether or not the aftercare program was provided on a voluntary of mandatory basis, because some researchers have argued that little benefit can be derived from criminal justice interventions when individuals are forced into treatment (Hartjen, Mitchell, & Washburne, 1981; Parhar, Wormith, Derkzen, & Beauregard, 2008; Platt, Buhringer, Kaplan, Brown, & Taube, 1988). According to this view, it is a poor investment to devote resources to youths who are unlikely to change because they are only externally motivated to change by the possible negative consequences of non-compliance.
Finally, treatment retention was included as a potential moderator, as prior research has shown that whether participants dropped out of treatment is a good predictor of their individual’s long-term success (Hubbard, Craddock, Flynn, Anderson, & Etheridge, 1997; Simpson, Joe, & Brown, 1997).
Method
Participants
Participants were juveniles who were referred to NPAP between January 2010 and July 2012 and who met the inclusion criteria for NPAP according to the team manager and/or behavioral scientist (Vogelvang & Schut, 2008). A total of N = 163 were recruited for the study at baseline and randomly assigned to the intervention NPAP group (n = 79) or the control group (n = 84). We were unable to complete a first assessment for 36 participants (NPAP, n = 13; TAU, n = 23) because they were unwilling to cooperate with the assessment or because they were untraceable, resulting in an attrition of 22.1% and 127 participants (NPAP, n = 66; TAU, n = 61) who completed the first assessment. Despite extensive tracing efforts, 20 participants (NPAP, n = 12; TAU, n = 8) were lost to post-intervention assessment and two had yet to complete the assessment at the time of writing, resulting an attrition of another 12.2% of the original sample and in 107 juvenile and young adult offenders (NPAP, n = 54; TAU, n = 53) who completed both the pre- and posttest measurements.
Participants lost to post-intervention assessment did not differ significantly on any assessed variable from those retained. Little’s (1998) missing completely at random (MCAR) test indicated that data were MCAR, χ2(32) = 31.161, p = .509. As differences were unrelated to attrition, all 127 remaining participants (NPAP, n = 66; TAU, n = 61) were included in the analyses, correcting for the attrition on the posttest. A flow diagram on inclusion and drop out per measurement wave is provided in Figure 1. We did not use listwise deletion as it can result in discarding a large proportion of the data, which can lead to biased results, because the power of the study decreases. Multiple imputation is currently recommended as a modern missing data handling technique (Baraldi & Enders, 2010). Using LISREL 8.8, the multiple imputation was carried out by means of the expectation maximization algorithm (Graham, 2009).
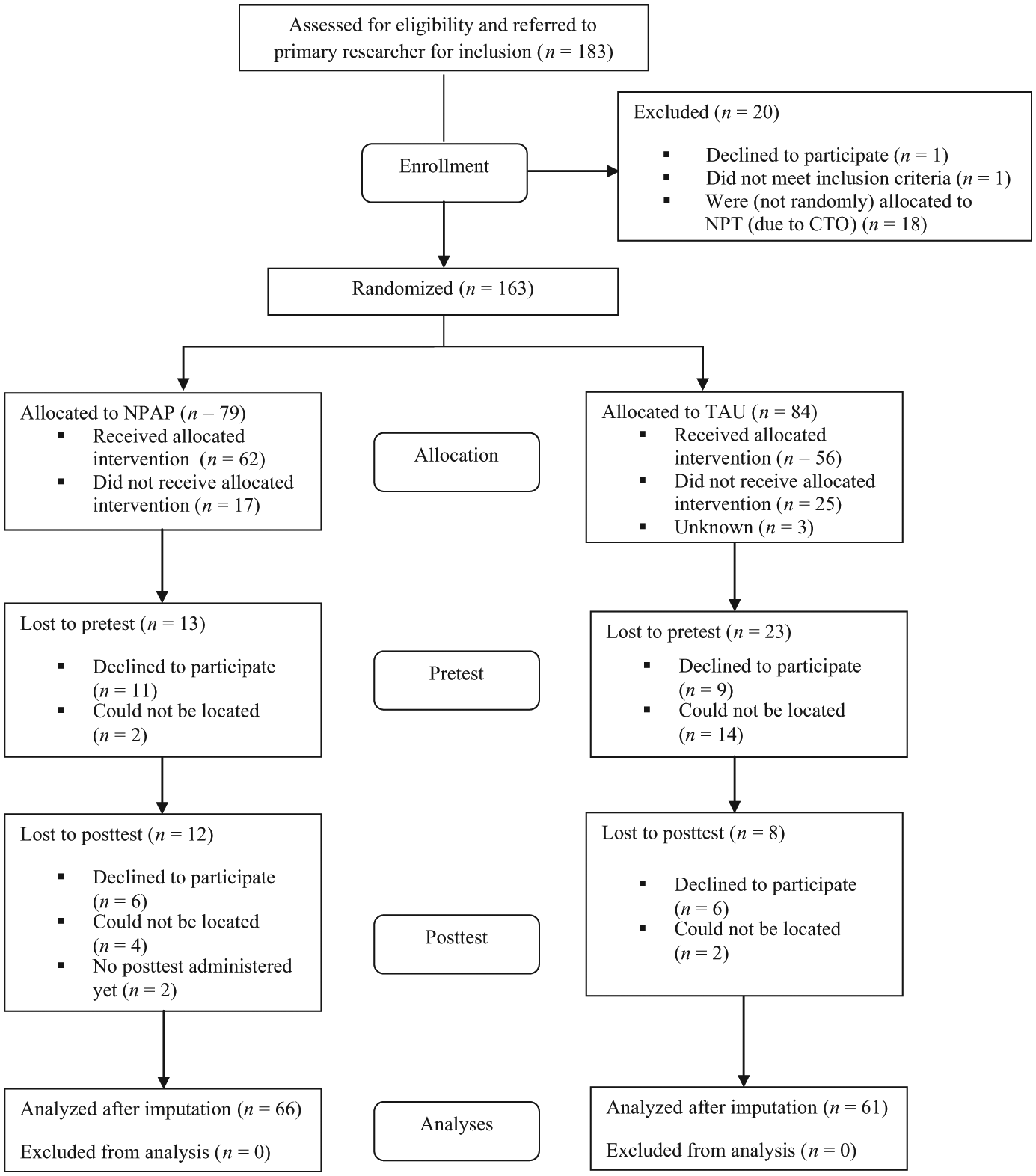
Flow diagram.
The majority of the sample was male (n = 123). The sample ranged in age from 15 to 26 years old (M = 19.54, SD = 2.38). In this study, 85% had an ethnic minority status, meaning that at least one of the youth’s parents was born outside of The Netherlands. 1 The largest ethnic minority group (35.4%) consisted of second-generation non-Western immigrant workers (from Moroccan and Turkish descent). Of the participants, 26.8% was detained in an adult or juvenile detention facility at the first measurement wave. Just over a third of the participants who were not detained at T1 lived with one or both of their parents (39.4%) and more than half of them had debts (55.9%), ranging from 0 to 1,000 euro (11.8%) to more than 5,000 euro (14.2%). Participants were on average 13.43 years old (SD = 2.42) when they first came into contact with the police. Of the juveniles and young adults, 42.5% admitted using cannabis on a regular basis, smoking an average of 2.98 (SD = 2.18) joints a day. An overview of the key background variables of the experimental and control group is shown in Table 1.
Descriptives of the Intervention (NPAP) Group and Control (TAU) Group at Pretest.
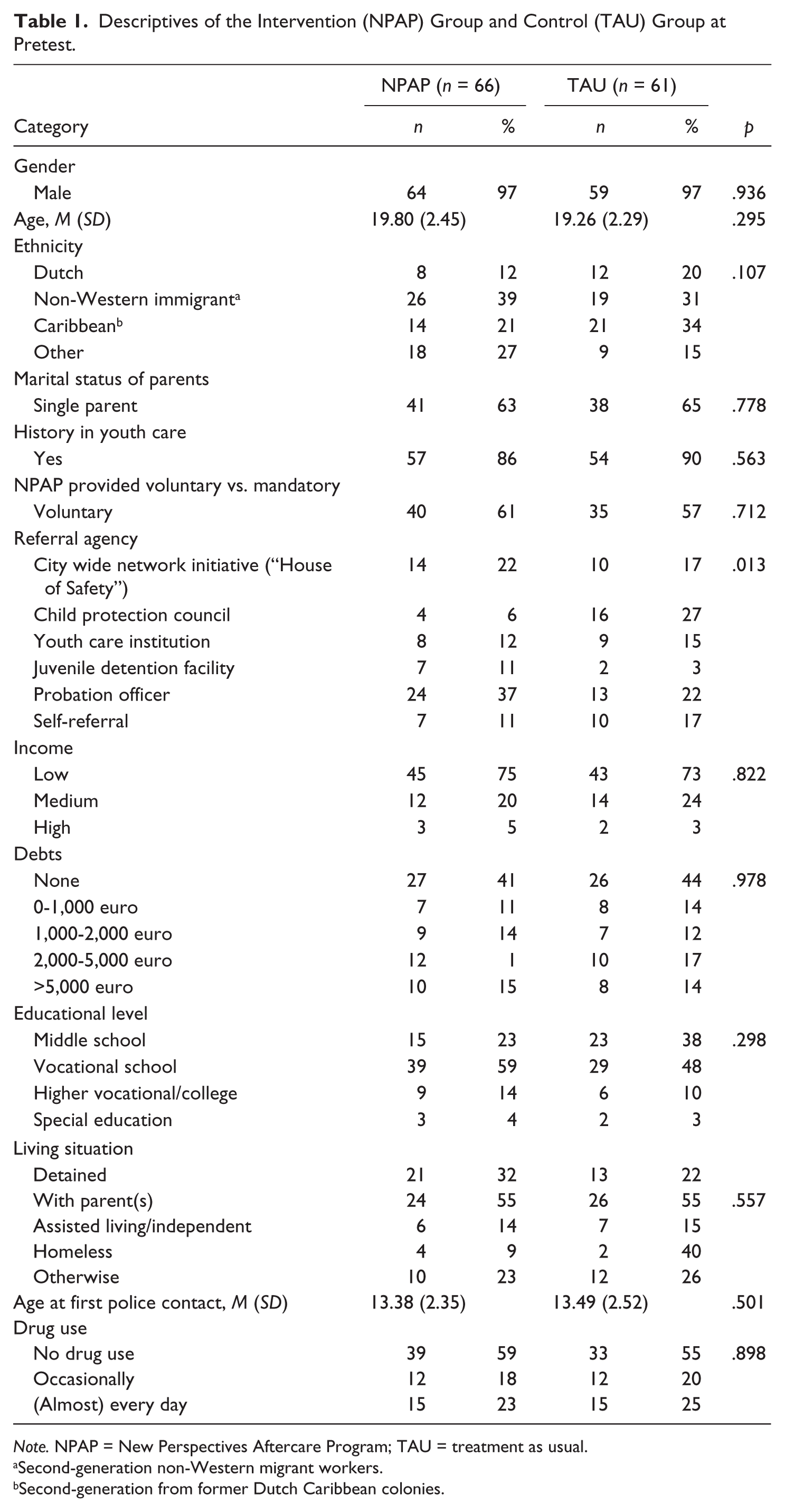
Note. NPAP = New Perspectives Aftercare Program; TAU = treatment as usual.
Second-generation non-Western migrant workers.
Second-generation from former Dutch Caribbean colonies.
Independent-sample t tests for continuous variables and chi-square analyses for categorical variables were used to examine differences between treatment conditions at pretest on demographic and outcome variables. With the exception of referral agency, χ2(5, n = 107) = 13.537, p < .05, which showed that in the NPAP group, most referrals came from probation officers, whereas in the control group, most referrals came from the child protection councils, no significant differences were found on any of these variables, suggesting that randomization was successful.
Procedure
The study involved random assignment of individuals referred to NPAP, equally divided into an experimental (NPAP) condition and control condition (“TAU”).
Individuals were recruited after being referred to NPAP by one of various possible referral agencies, such as a youth care institution or probation officer. 2 After a client was referred to NPAP, he or she was screened by the NPAP’s team manager and/or behavioral scientist based on an intake form and the available case file. Juveniles and young adults aged 16 to 24 were eligible for the aftercare program and inclusion in the study if they (a) had spent a minimum of 4 weeks in detention; (b) had committed a minimum of three criminal acts, including one serious offense; (c) moderate to serious problems regarding social skills, criminal thinking patterns, and behavior; and (d) had a medium to high recidivism risk, based on a recent risk assessment by the RISc 3 (Adviesbureau Van Montfoort & Reclassering Nederland, 2004) or the Structured Assessment for Violence Risk in Youth (SAVRY 4 ; Lodewijks, Doreleijers, de Ruiter, & de Wit-Grouls, 2006).
Exclusion criteria for the NPAP program were a low IQ (<75), severe psychiatric problems, and/or substance abuse problems and lack of motivation (Vogelvang & Schut, 2008). If a client was found eligible for enrolment in NPAP (based on the inclusion and exclusion criteria for the program), he or she was informed about the trial by the referral agency. When informed consent was obtained, computerized randomization took place. Subsequently, juveniles and young adults were approached by the researchers for completion of a set of questionnaires prior to the start of NPAP or TAU (T1) and at posttest (T3), 9 months later. Data were collected by the first author and several trained research assistants. The majority of the research assistants who conducted the assessments were not informed about the participant’s randomly assigned condition (blinding). A range of standardized questionnaires was used at each measurement wave to identify an individual’s cognitive and behavioral problems, skills, motivation, and changes over time. The participants received 20 euros for each completed assessment as a token of gratitude. 5 The medical ethical committee of the University of Amsterdam approved the design of the study (number 10.17.1193).
Conditions
NPAP
The NPAP is an intensive aftercare program for serious juvenile and young adult offenders, aged 16 to 24 years, reentering society after a period of detention or secure care, with a moderate to high recidivism risk. The goals of the treatment are the prevention of recidivism (new convictions) by modifying cognitive distortions and behavior and improving social skills. The intervention is intensive, vigorous, and highly individualized; combining reintegration in the neighborhood, work or school, and focusing on the network of the juvenile or young adult as a whole. The intervention strategies include coordinated case management, motivational interviewing, and cognitive behavioral interventions focused on controlling impulses, problem solving, and criminogenic thinking patterns (Vogelvang & Schut, 2008).
NPAP is divided into three phases and it is typically delivered for 9 months, with a 3-month follow-up period. The first (reentry) phase commences during the last 3 months of detention to ensure a smooth transition from the closed environment back into the community, followed by an intensive phase of 3 months and a consolidating phase. During the intensive phase, the youth care workers have 6 to 8 hr a week per client. In addition, they have low caseloads (six to seven clients maximum), are available 24 hr a day, are outreaching, invest in a therapeutic relationship with their clients, and aim to build a prosocial network that the juveniles and young adults can rely on beyond the intervention period.
TAU
The participants assigned to the control group were offered the usual services for this target group, a broad array of social and mental health interventions, including juvenile and adult justice services, child welfare services, and youth care services. Predominantly, these services included individual treatment, with 68.0% of the TAU group youths receiving individual counseling and case management through a secondary prevention program, and 20.8% through a community-based intervention. Some youths were referred to family-based interventions (Functional Family Therapy [FFT] or Multidimensional Family Therapy [MDFT], 11.3%) and treatment in a residential setting (2.5%). Most of the interventions provided as TAU consisted of components that are also present in NPAP and focused on similar risk factors. Of the control group youths, 20.4% eventually received no treatment, mostly due to a lack of motivation, versus 11.1% of the NPAP group (see Table 1).
Measures
Aggressive behavior
The Buss–Durkee Hostility Inventory–Dutch (BDHI-D) is used to assess aggressive behavior in adolescents. The questionnaire consists of 35 items on a 2-point Likert-type scale, with response options true and false. The BDHI-D consists of two scales, measuring Direct Aggression (16 items, for example, “I almost never hit someone, even if the other gives the first blow”) and Indirect Aggression (19 items, for example, “I never get so angry that I’ll throw stuff around’). The reliability of both scales was sufficient, with Cronbach’s α = .740 (pretest) and .773 (posttest) on the Direct Aggression scale and Cronbach’s α = .811 (pretest) and .823 (posttest) on the Indirect Aggression scale.
Cognitive distortions
To assess Self-Serving Cognitive Distortions, the Dutch translation of the How I Think (HIT) Questionnaire for adolescents (Brugman, Nas, & Van der Velden, 2011; Gibbs, Barriga, & Potter, 2001) was used. The HIT consists of 54 items, of which 8 are anomalous response items designed to screen for socially desirable responses and 7 positive filler items to encourage full use of the scale. Participants indicate how much they agree with statements representing Self-Serving Cognitive Distortions, for example, “If someone gets beat up, it’s usually his or her own fault.” The juvenile is asked to indicate his or her degree of agreement along a 6-point Likert-type scale, ranging from strongly disagree (1) to strongly agree (6). The HIT consists of four different Self-Serving Cognitive Distortions: “Self-Centeredness” (9 items), “Blaming Others” (10 items), “Minimizing/Mislabeling” (9 items), and “Assuming the Worst” (11 items). Nas et al. (2008) found satisfactory reliability and validity (convergent and divergent) in a Dutch sample. The internal consistency of the HIT in this study was excellent, with Cronbach’s α = .938 (pretest) and .939 (posttest), and Cronbach’s α = .954 (pretest) and α = .953 (posttest) for Self-Serving Cognitive Distortions. The subscales of Self-Serving Cognitive Distortions also had good reliabilities ranging from α = .813 to α = .865 (pretest) and α = .797 to α = .870 (posttest).
Coping
The use of different coping strategies is measured by the Utrecht Coping List for Adolescents (UCL-A; Schreurs, Willige, van de Brosschot, Tellegen, & Graus, 1993). The UCL-A gives an indication of the psychosocial functioning and preference for certain coping styles in different situations. The self-assessment questionnaire UCL-A consists of 47 items (e.g., “I share my concerns with someone”), of which 3 are positive filler items and 44 of the items can be divided into seven subscales: Confrontation (7 items), Palliative Reaction Pattern: engaging in other activities trying to relax (8 items), Avoidance (8 items), Seeking Social Support (6 items), Depressed (Passive) Response Pattern (7 items), Expression of Emotions (3 items), and Reassuring Thoughts (5 items). The items are scored along a 4-point Likert-type scale with the response categories rarely or never, sometimes, often, or very often. The seven subscales can be divided into two new scales, for example, Active Coping (with the scales Confrontation, Seeking Social Support, Expression of Emotions, and Reassuring Thoughts) and Passive Coping (with the scales Palliative Reaction Pattern, Avoidance, and Depressed [Passive] Response Pattern). The internal consistency for the scales was good, with Cronbach’s α = .828 (pretest) and α = .868 (posttest) for Passive Coping and Cronbach’s α = .818 (pretest) and α = .836 (posttest) for Active Coping. In addition, the reliability of most subscales was sufficient, with reliabilities ranging from α = .677 (pretest “reassuring thoughts”) to α = .840 (pretest “seeking social support”) and α = .619 (posttest “reassuring thoughts”) to α = .795 (pretest “seeking social support”).
Pro-criminal attitude
A possible pro-criminal attitude toward crime was measured with the Crime Pics II (Frude, Honess, & Maguire, 1994). This questionnaire for adolescents consists of 20 items along a 5-point Likert-type scale ranging from strongly disagree (0) to strongly agree (4). A higher score on the scale means that there is more of a pro-criminal attitude. The Crime Pics II consists of the subscales General Attitude Toward Crime (17 items, for example, “Crime does pay”), Anticipation of Recidivism (6 items, for example, “Committing offenses has become a way of life for me”), and Denial of the Victim’s Suffering (3 items, for example, “There are no victims from my offense(s)”). According to Frude et al. (1994), the Crime Pics II has a good face and criterion validity. The scales demonstrated adequate reliability with, respectively, an internal consistency of Cronbach’s α = .801 (pretest) and α = .822 (posttest) for “General Attitude Toward Crime,” Cronbach’s α = .702 (pretest) and α = .788 (posttest) for “Anticipation of Recidivism,” and Cronbach’s α = .718 (pretest) and α = .718 (posttest) for “Denial of the Victim’s Suffering.”
Prosocial skills
The Dutch Questionnaire Social Skills of Youths (VSVJ) is used to measure prosocial skills (Hulstijn et al., 2008). The VSVJ is a self-report questionnaire consisting of 28 items measured along a 5-point Likert-type scale, ranging from not at all (1), sometimes (2), regularly (3), and often (4) to very often (5). The VSVJ considers a social person as someone who can communicate with others, can adapt to its environment, knows how to prevent or adequately resolve peer conflicts. The VSVJ consists of the scales, Prosocial Behavior (16 items, for example, “I show my emotions”) and Socially Inappropriate Behavior (12 items, for example, “I threaten others”). Juveniles scoring high on Socially Inappropriate Behavior and/or low on Prosocial Behavior are considered to have social skill problems. The internal consistency of the VSVJ in the current study was good, with Cronbach’s α = .901 (pretest) and α = .837 (posttest) for Prosocial Behavior, and Cronbach’s α = .821 (pretest) and α = .785 (posttest) for Socially Inappropriate Behavior.
Response style
To assess response style, the anomalous response scale from the HIT was used (8 items, for example, “sometimes I get bored”; Gibbs et al., 2001), together with a social desirability measure (Crowne & Marlowe, 1960). The Dutch translation of the Social Desirability Scale (SDS) consists of 15 items measured on a 2-point Likert-type scale: 1 (true) or 2 (false). Participants indicate whether they agree with improbable statements (e.g., “I always tell the truth”). The higher the score on the SDS, the more likely someone is to respond in a socially desirable manner (Rutten et al., 2007). The internal consistencies were good, with Cronbach’s α = .762 (pretest) and α = .791 (posttest) for the anomalous response scale of the HIT Prosocial Behavior, and Cronbach’s α = .841 (pretest) and α = .853 (posttest) for the SDS. Furthermore, anomalous responding correlated with social desirability, r = .514, p < .001.
Analyses
The present study incorporated an intention to treat (ITT) design (Bergseth & Bouffard, 2013; Sherman & Strang, 2004) to eliminate potential confounding effects of treatment motivation (or offending propensity) that occurs when cases are analyzed based on the treatment actually delivered. Individuals were retained in treatment (NPAP) and comparison (TAU) groups based on referral to those interventions, regardless of their level of attendance to the assigned intervention.
First, overall effectiveness of NPAP was examined for all outcome measures using ANCOVA with IBM SPSS version 20. The intervention outcomes (cognitive distortions, criminal thinking patterns, prosocial skills, and aggressive behavior) at posttest served as dependent variables, treatment condition as the between-subjects factor (i.e., experimental vs. TAU) and the pre-intervention scores of the outcome variables as a covariate. The achieved sample size was n = 127 (NPAP, n = 66; TAU, n = 61), which is sufficient to test the hypotheses in a series of ANCOVAs assuming .80 power, an alpha of .05, and a large effect size (Cohen, 1992).
For the moderator analyses, the same ANCOVAs were conducted, with the moderators as factor. Post hoc analyses for moderator effects were conducted by splitting the file according to the moderator and again conducting an ANCOVA and calculating effect sizes separately for each group. Effect size estimates were computed as Cohen’s d, and were calculated through a formula from Lipsey and Wilson (2001), based on the F values of the ANCOVA’s used to examine differences between pre- and posttest scores for the NPAP and TAU groups regarding the outcome variables, controlling for pretest scores. Effect sizes were coded such that positive values indicated a positive outcome for the NPAP group compared with the control group.
Results
Intervention Effects
One-way between-subjects ANCOVAs were carried out to assess the impact of the NPAP on the various cognitive and behavioral outcome measures. Tests were carried out to confirm homogeneity of regression and linear relationship between the covariate and each dependent variable. Table 2 shows that no significant main effects were found with regard to any of the outcome measures (i.e., aggressive behavior, cognitive distortions, pro-criminal attitude, coping, and prosocial skills).
Means, Standard Deviations, and Intervention Effects of NPAP Versus TAU.
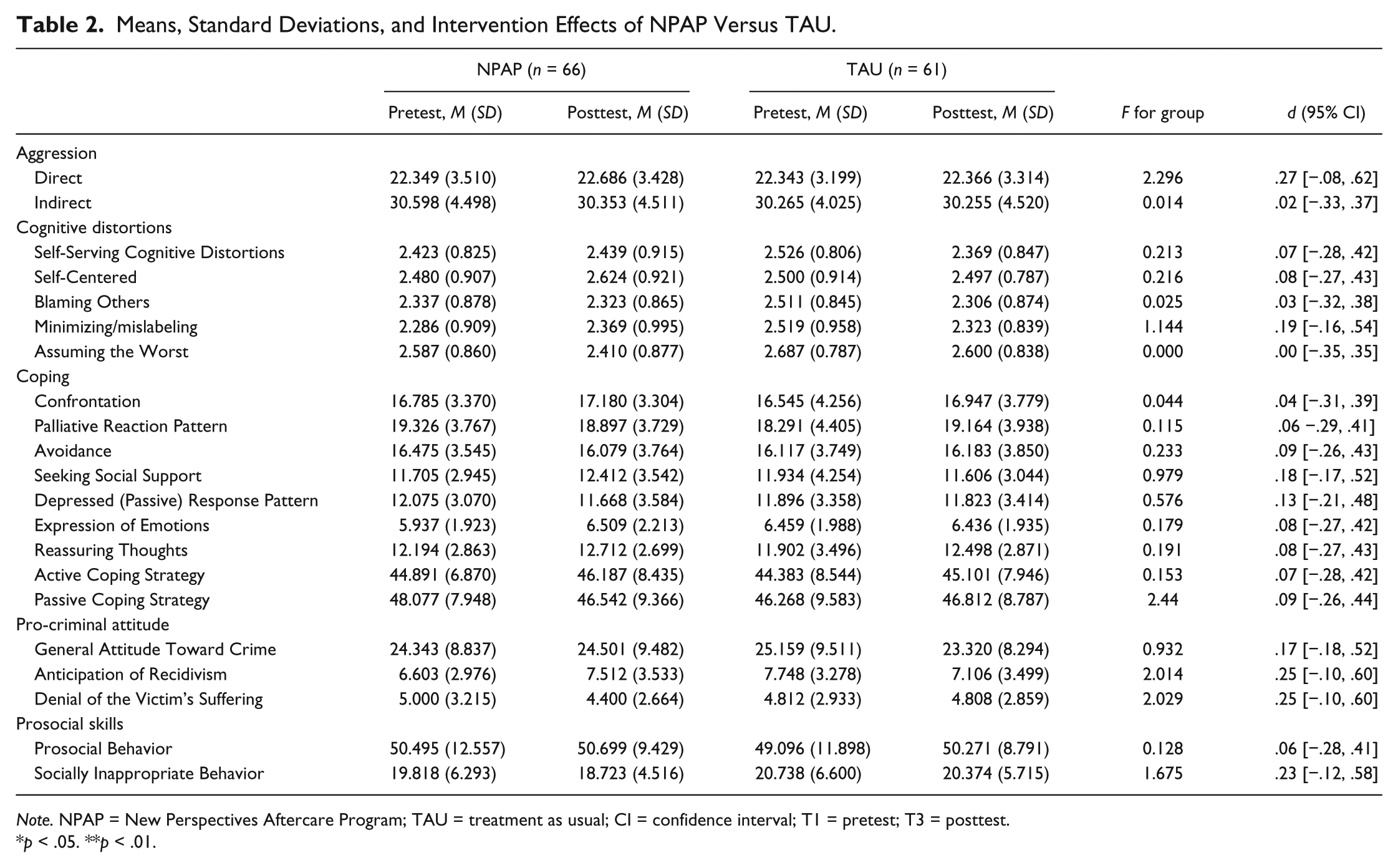
Note. NPAP = New Perspectives Aftercare Program; TAU = treatment as usual; CI = confidence interval; T1 = pretest; T3 = posttest.
p < .05. **p < .01.
Moderators of Effectiveness
To examine whether demographic characteristics, legal framework, and moment of commencing aftercare affected the effectiveness of NPAP, five potential moderator effects were tested.
Ethnic minority status
Moderator analyses of ethnicity revealed significant interaction effects with condition and several coping strategies. A significant Ethnicity × Condition interaction was found for palliative reaction pattern, F(3, 118) = 6.30, p < .01. Post hoc analyses showed significant intervention effects for native Dutch juveniles, F(1, 17) = 20.42, p < .01, d = 2.06: Dutch juveniles in the NPAP group adopted a palliative reaction pattern more often, whereas Dutch juveniles in the control group showed a decrease in the use of palliative reactions over time. The intervention effect was also significant for Caribbean youths, F(1, 32) = 6.82, p < .05, d = −.90, but the direction of this effect was different than for Dutch juveniles: between pre- and posttest Caribbean youths in the TAU group increased their use of palliative reactions when faced with a difficult situation, whereas it decreased in the NPAP group. No differences in the use of palliative reactions were found for the other ethnic minority groups.
In addition, a significant interaction between ethnicity and condition was found for the use of reassuring thoughts as a coping strategy, F(3, 118) = 3.00, p < .05. Post hoc analyses revealed a significant intervention effect for Dutch juveniles, F(1, 17) = 8.93, p < .01, d = 1.36, indicating that Dutch juveniles from the NPAP group significantly increased the use of reassuring thoughts following aftercare, whereas Dutch juveniles who were referred to TAU did not. For the ethnic minority groups, no significant differences were found.
Age
To examine whether adolescents or young adults would benefit more from NPAP, the sample was divided in a group that was 18 years of age or younger (n = 52) and a group of 19 years and older (n = 75). Results show that age was a significant moderator, interacting with the intervention status in predicting the use of the coping skill seeking social support. Post hoc analyses showed that there was no change in the use of this coping skill in younger youths, F(1, 49) = 1.23, p = .27, d = .20, whereas a large and negative intervention effect was found for older NPAP youths, F(1, 72) = 8.36, p < .01, d = −.51, indicating that, at posttest, older youths referred to TAU did seek social support when faced with a difficult situation more often, whereas NPAP youths sought social support significantly less.
Voluntary or mandatory treatment
No interaction effects were found for the group of young offenders who were referred to aftercare on a voluntary basis (n = 75) and who were referred to aftercare on a mandatory basis (n = 52), including a mandatory treatment order (Community Treatment Orders [CTO]). As no intervention effects were found for voluntary versus mandatory treatment, youths who receive aftercare within a legal framework are just as likely to do well following aftercare as those who receive NPAP on a voluntary basis.
Start of aftercare
With the aim of establishing whether it matters if juveniles and young adults are referred to aftercare during (n = 34) or after detention (n = 91), we analyzed if there were interaction effects. We found no significant Moderator × Intervention effects, indicating that there is no difference in effectiveness of the intervention between youths who start receiving the aftercare intervention during the last phase of their detention or after being released.
Completing aftercare
Moderator analyses showed that whether juveniles successfully completed the intervention (n = 68), dropped out (n = 35), or did not even start with the intervention (n = 24) significantly interacted with condition regarding the use of indirect aggression at posttest, F(2, 120) = 3.20, p < .05. Post hoc analyses revealed a larger and significant intervention effect for juveniles and young adults who dropped out from aftercare, F(1, 32) = 4.55, p < .05, d = .73, than for youths who did not commence aftercare, F(1, 21) = .31, p = .58, d = .10, or completed the intervention, F(1, 65) = .496, p = .48, d = .13. NPAP youths who dropped out from the intervention displayed significantly more indirect aggression at posttest compared with youths dropping out from TAU and who showed a slight decrease in indirect aggression. NPAP youths who completed the intervention showed somewhat less indirect aggression, whereas TAU group youths increased their use of indirect aggression. Youths who eventually did not receive aftercare showed hardly any change in the use of indirect aggression.
Discussion
This study is one of the first to analyze the impact of an aftercare program for juvenile and young adult offenders on criminogenic needs. We intended to determine whether the NPAP managed to establish changes in aggressive behavior, cognitive distortions, and criminal thinking patterns, and to increase the social and problem-solving skills of adolescents or young adults immediately after NPAP or TAU.
The findings from this RCT study do not support the overall short-term effectiveness of NPAP on any of the outcome measures relative to the services usually available for delinquent youths leaving a secure care or (juvenile) detention facility. Although this outcome is not in line with what was expected, perhaps this is not so surprising. It most likely took many years and an accumulation of problems to become the adolescents and young adults they now were (Lane, Turner, Fain, & Sehgal, 2005). Therefore, it may take more time to establish significant changes than is possible within the 9 months of the intervention. As NPAP targets the most difficult young offenders (high risk, with lengthy criminal records and numerous criminogenic needs), the expected short-term impact might be low. A recent meta-analysis showed that the overall effect size of aftercare programs is relatively small (James et al., 2013). In addition, the null effects from this study are consistent with the scarce prior research on intermediate outcomes of aftercare programs, in which the expected positive impact of aftercare was not found (Barton, Jarjoura, & Rosay, 2008; Greenwood, Deschenes, & Adams, 1993). To make lasting changes, continuation of care beyond the relatively short period of aftercare might be necessary, especially for particular vulnerable subgroups. However, the question remains as to how long aftercare should last in these cases.
To examine whether subgroups of youngsters benefited more or less from the intervention and if other factors were related to the program’s outcomes, moderator analyses were performed. We found that ethnicity moderated the intervention effects of several coping strategies. Most remarkable was the finding that Dutch and Caribbean NPAP youths did benefit from the intervention in that they were more able to use healthy coping strategies when they were confronted with a challenging or difficult situation. After NPAP, Dutch NPAP youths more often used reassuring thoughts as a coping strategy, whereas Caribbean NPAP youths showed a decrease in their palliative reaction pattern compared with control group youths. No differences in intervention effects were found for the various ethnic groups on other outcomes, such as cognitive distortions and aggressive behavior, showing that NPAP can be used for all delinquent juveniles and young adult offenders, regardless of their ethnicity, corresponding with what prior research suggests (Wilson et al., 2003).
Furthermore, mixed results were found for the impact of age on the use of the active coping skill to seek social support. Although there was no significant difference between younger NPAP and TAU group youths, older NPAP youths sought social support significantly less over time than youths who were referred to TAU. Generally speaking, one would expect that youngsters would seek less social support as they mature, because their autonomy increases during adolescence and the impact of parental supervision diminishes as youngsters come of age (Van der Put et al., 2011). Yet, our findings are contrary to our expectations, because NPAP seeks to stimulate the development of healthy coping strategies to prevent a relapse into antisocial behavioral patterns. Potentially, we can speculate that NPAP youths sought less social support elsewhere, because they felt that they received sufficient support from their NPAP youth care worker during the critical period post-release in which they were faced with the challenges of reentry.
Although some prior research suggests that participants benefit more from aftercare if the program starts during detention (Altschuler et al., 2004), our results showed that the moment of starting the aftercare intervention is not related to the aftercare program’s effectiveness, as was also shown by the meta-analytic study by James et al. (2013). These findings suggest that NPAP would have been just as effective when started upon reentry compared with when the intervention starts during the last phase of secure care or detention, if any significant changes on the criminogenic needs would have been found. In practice, it appears to be difficult to commence with the aftercare program prior to release of the offender, because many stakeholders are involved and offenders are sometimes unexpectedly released at an earlier stage. Therefore, the findings from our moderator analyses are of practical importance in that they highlight that whether aftercare is started before or immediately after release is irrelevant. Instead, based on our findings, it seems to be more important that youths complete the aftercare program, once they have commenced.
Another remarkable finding from the moderator analyses is that it does not matter whether NPAP is provided on a mandatory or voluntary basis. This finding indicates that NPAP can be just as effective for offenders who are forced into aftercare, for example, as part of their parole conditions, as for offenders who are referred to aftercare without a legal framework, and who are likely to be more intrinsically motivated to change. Traditional views on therapy outcomes assume that clients must have a genuine motivation to change, whereas more current research suggests that motivation is a more dynamic process (Wormith et al., 2007). Readiness for treatment appears to be more complex, incorporating aspects of willingness, readiness, and ability, among other things (Lösel, 2012). Our findings are in line with research on substance abuse treatment and sexual offender treatment, in which no clear outcome differences were found between mandatory and voluntary participation (Schmucker & Lösel, 2009; Shearer & Ogan, 2002). It seems to be more important that participants enroll in the program than whether program participation is coerced, which is important for referral agents who enroll juvenile and young adult offenders in aftercare programs such as NPAP.
Finally, the results point out the importance of completing the NPAP. NPAP youths who completed the intervention showed a decrease in indirect aggression, whereas NPAP youths dropping out from the program showed significantly more indirect aggression than youths who received TAU. These results show that the NPAP intervention has a significant impact on the use of indirect aggression, which is a risk factor for (violent) recidivism (Card, Stucky, Sawalani, & Little, 2008; Nagin & Tremblay, 1999). As is shown by prior research, treatment dropouts often do even worse than the control group (Lösel, 2012).
Why did this study on the effectiveness of NPAP not produce more positive results? One consideration is that standards for services traditionally provided for youngsters reentering society are already relatively high in The Netherlands. Considering that the majority of the TAU group received some form of established and often theoretically based intervention, one can expect to find smaller effect sizes, if any at all. Based on recent studies, Lösel (2012, p. 83) pointed out that “more positive control conditions and the transfer of ‘what works’ knowledge into routine practice seem to contribute to lower effects in some more recent studies” (Sundell et al., 2008; Tong & Farrington, 2006). However, when the two groups are considered separately, no significant changes on any of the expected outcome variables were found for the TAU group either.
Finally, our largely null findings could also be ascribed to the methodological rigor of the study design that we used. As is shown by previous studies, RCTs, such as ours, show less favorable results in terms of effect sizes as compared with weaker research designs, which is attributable to the internal validity (Lipsey & Wilson, 1998; Weisburd, Lum, & Petrosino, 2001; Welsh, Peel, Farrington, Elffers, & Braga, 2011). Weaker research designs include a control group (if any) that is matched on several of the offenders’ background characteristics at best, resulting in a comparison group that tends to differ from the intervention group, at least more than is possible in an RCT, the golden standard in which these differences are controlled for by means of randomization. Group differences in weaker research designs result in a greater likelihood to find positive differences on any of the outcome measures, which is therefore less likely in our current RCT study.
This study has a number of strengths. The study is the first RCT of an aftercare program for juvenile and young adult offenders in The Netherlands, and one of few RCT studies into the effectiveness of aftercare programs conducted worldwide (James et al., 2013). Another strong point of the study is its ecological validity, as the study was carried out as a field trial in a “real world” forensic youth care practice setting (Barkham & Mellor-Clark, 2000; Cape & Barkham, 2002; Weisz, Jensen-Doss, & Hawley, 2006). Therefore, the findings of this study provide important information for policy makers and clinicians, and can be applied directly in practice to improve the effectiveness of aftercare services provided for juvenile and young adult offenders. Furthermore, the sample consisted of a group of very serious offenders, who tend to have a high attrition rate in studies such as these that rely solely on self-report measures. Yet, due to relentless and extensive tracing efforts, we were able to limit the attrition rate to only 34.3%.
There are also several limitations to this study and issues that should be addressed in future research. First, the study suffered from considerable attrition of study participants. Yet, these participants did not differ significantly on any assessed variable from those retained. However, it is always possible that dropouts differed on other, untested measures. Moreover, sizable attrition is to be expected given that the sample consisted of a group of very serious young offenders who tend to have a high attrition rate in studies that rely on self-report measures. Attrition rates among this population are generally high, given that the young offenders have recently been released from secure confinement and are often without stable living arrangements and income and therefore difficult to trace (Crisanti, Case, Isakson, & Steadman, 2014).
Second, the final sample was relatively small in size (n = 127) resulting in our study being underpowered to detect small intervention effects. However, it seems highly questionable whether the observed (very) small effects have clinical significance. Furthermore, the sample size is comparable with many other RCTs of aftercare programs for juvenile and/or young adult offenders (Bergseth & McDonald, 2007; Greenwood et al., 1993; Sontheimer & Goodstein, 1993). Because of the sample size and even smaller subgroups, for example, with regard to ethnicity, we need to be cautious when interpreting the findings from the moderator analyses. However, there is also the possibility that the study was underpowered for detecting moderator effects that would otherwise have become apparent if the sample size had been larger (Asscher, Deković, van der Laan, Prins, & Van Arum, 2007; Gardner, Hutchings, Bywater, & Whitaker, 2010). Furthermore, only few moderators were tested in the current study. Additional potential moderators and mediators of the intervention should be analyzed in the future to study their impact on treatment outcomes.
Despite the limitations, this study makes a valuable contribution to the small and growing body of literature on the effectiveness on aftercare programs for juvenile and young adult offenders, especially because it incorporates criminogenic needs as a measure of program effectiveness, of which very little is known thus far. A possible interpretation of the largely null effects is that NPAP is generally not successful in producing positive outcomes and that it is therefore not worthwhile to continue with this intervention and similar aftercare programs. However, one should be careful not to accept the null hypothesis, because not finding any clear-cut treatment effects in terms of changing criminogenic factors does not mean NPAP is unsuccessful, as results regarding delinquency and recidivism are yet to come. While the results of this study do not provide compelling evidence that NPAP was effective in altering criminogenic needs, it does not warrant dismissal of the program.
Several research and policy recommendations can be made. Perhaps, the focus should not be on specific treatment principles (e.g., altering cognitive distortions) to measure the success of NPAP on the long term. There are also other measures of success that can result from successful case management and should be included in a subsequent study, such as whether a juvenile managed to establish (and maintain) meaningful education and employment activities. Literature shows that these factors should also be considered as criminogenic needs and the target of aftercare interventions. Altschuler and Armstrong (2004) stated that outcomes refer not only to observable changes in program participants regarding knowledge, attitudes, beliefs and behavior but should also include environmental factors (e.g., whether the aftercare program has helped create new job opportunities or qualifications for youth). This is often a weakness of many leaving detention who experience a gap between income (work, benefits) and spend. Research indicates that this gap is often filled by crime (Shapland, Bottoms, & Muir, 2012) and should therefore be closed during aftercare to prevent recidivism (Welsh et al., 2012). “Soft measures,” such as employment, schooling, housing, and establishing a meaningful relationship, are perhaps the most important measures of success for the offenders themselves, who struggle to get their lives back on track. If asked directly, they are likely to value these practical issues more than whether their dysfunctional cognitions have changed. Research on desistance confirms this belief (Blokland & Nieuwbeerta, 2005; Horney, Tolan, & Weisburd, 2012).
In addition, subsequent research should also focus on the working mechanisms of more general treatment principles, such as client–therapist relationship, which is an important factor of influence on the effectiveness of an intervention (Wampold & Brown, 2005).
Continuous quality control procedures should be developed and used to improve treatment adherence and staff competence, as treatment effects are larger when staff is well selected, trained, and supervised (Antonowicz & Ross, 1994; Gendreau et al., 1999). Moreover, a longer follow-up period of the study might show delayed or so-called “sleeper” effects, in which changes in cognitions might only become visible over a longer period of time, because they need time to sink in. Therefore, future research is needed to include a longer follow-up period and examine other relevant risk and protective factors to draw a more definite conclusion on the effectiveness of the NPAP.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.