
Abstract
The pilot study presented in this article investigated the role of moral-cognitive features in understanding aggressive and rule-breaking behaviours in adolescents with Disruptive Behaviour Disorder (DBD). We collected two samples. The community sample was composed of 85 adolescents, whereas the DBD sample was composed of 30 adolescents. Compared with a community sample, adolescents with DBD are more inclined to use moral disengagement (MD) to legitimize their aggressive and rule-breaking behaviours. Moreover, regression models showed that self-enhancement values and MD foster externalizing behaviours taking into account both gender and the group they belonged to, that is, either clinical or community sample. Instead, self-transcendence values could prevent externalizing problems by inhibiting MD. Implications of these findings for assessment and therapeutic interventions are discussed.
Disruptive Behaviour Disorders (DBDs), including Oppositional Defiant Disorder (ODD) and Conduct Disorder (CD), are among the most common reasons for referring children and adolescents to outpatient clinics in Italy (Frigerio et al., 2006) as well as in other countries (Steiner & Remsing, 2007). Children with ODD and CD comprise a heterogeneous group of patients who engage in a broad array of problem behaviours, ranging from relatively minor defiance and temper tantrums to more serious violations such as physical aggression, destructiveness, and stealing (American Psychiatric Association, 2000). Children with ODD or CD are at risk of developing a variety of problems such as peer rejection, school failure, substance abuse, and criminality (Burke, Arkowitz, & Dunn, 2002; Odgers et al., 2008) with high costs for communities (Kolko et al., 2009). The persistence of child behavioural problems and their role in the development of later clinical problems highlight the need for further studies in the field of DBD risk factors (Martens, 2000; Simonoff et al., 2004).
A variety of contextual and personal risk factors associated with children’s aggressive behaviour have been examined, including risks in family and peer relationships, children’s neurobiological functioning, and children’s abilities to cope with their anger and frustration, solve social problems, and use social skills (Krol, Morton, & De Bruyn, 2004; Matthys & Lochman, 2010). However, few studies have focused on one type of personal risk factors: moral-cognitive processes. Moral cognitions could be related to causal models underlying severe aggressive behaviours or rule-breaking behaviours (Arsenio, Adams, & Gold, 2009). Moreover, the change in moral cognitions is a major focus of treatment programs in juvenile corrections aimed at reducing delinquent and later criminal behaviour (Kim & Jurg Gerber, 2012).
Dodge and Godwin (2013) indicated that social-cognitive processes are major psychological mechanisms through which life experiences are stored and represented internally to guide our own behaviour. In line with this finding, personal values (PVs) and moral disengagement (MD) can identify a mind-set that promotes aggressive or rule-breaking behaviours. From this theoretical point of view, these disruptive behaviours can be regulated and maintained by personal beliefs (i.e., other or self-oriented PVs) and by cognitive processes (i.e., MD mechanisms; Bandura, 1991; Patrick & Gibbs, 2011). Moreover, it is likely that MD can become crystallized over time, for some adolescents, when dealing with antisocial and transgressive behaviours in the pursuit of self-interests (Paciello, Fida, Tramontano, Lupinetti, & Caprara, 2008). Thus, the exploration of PVs and MD in a clinical setting could be useful, because they represent factors influencing the severity of patients’ externalizing problems and could also be important for defining important targets for intervention.
Despite the possible implications in designing clinical interventions, to the best of our knowledge no studies have investigated how PVs and MD are related to aggressive and rule-breaking behaviours in adolescents with DBD.
PVs and Antisocial Behaviours
In Schwartz’s theory, PVs are conceived as trans-situational concepts or beliefs concerning desirable goals. PVs refer to motivational determinants of behaviour transcending specific situations and serve as general criteria to select and evaluate one’s decisions and actions. They vary in importance and serve as guiding principles in people’s lives. The importance of different PVs in selecting and evaluating one’s own behaviour across situations depends on how they are incorporated into self-concept during adolescence. Moral experiences and expertise gained in adolescence form the foundation of adult moral character, identity, and agency (Blasi, 2005), as well as the sense of responsibility toward community and society. Moreover, cross-cultural studies have confirmed the basic structure hypothesized by Schwartz’s value theory in adolescents’ samples (Bubeck & Bilsky, 2004; Schwartz, Melech, Lehmann, Burgess, & Harris, 2001). With respect to their content, PVs can be distinguished on the basis of the motivational goals they express (Schwartz, 1992). In the case of harmful behaviour, two opposite typologies of PVs can influence the selection and evaluation of aggressive behaviour: self-enhancement and self-transcendence. Self-enhancement PVs direct attention to one’s own needs and legitimize selfish and aggressive behaviours, whereas self-transcendence PVs direct attention to others’ needs and prevent harmful behaviour promoting other-oriented behaviours as helping (Schwartz, 2010; Schwartz & Howard, 1984). More specifically, self-enhancement values include power and achievement, which represent the pursuit of self-interests; instead, self-transcendence values comprise benevolence and universalism and emphasise concern for the welfare and interests of others.
Previous studies, delivered in community or at-risk samples, have linked PVs to problem behaviours (Goff & Goddard, 1999; Grube, Ames, & Delaney, 1994), to having deviant peers (Simons, Whitbeck, Conger, & Conger, 1991) and to become more reactively aggressive (McDonald & Lochman, 2011). Moreover, adolescents who prioritize self-oriented PVs are more likely to use self-serving mechanisms as MD to transform harmful behaviour in an acceptable way to interact with others. Differently, adolescents who prioritize other-oriented PVs are less likely to use MD and to adopt harmful behaviours (Menesini, Nocentini, & Camodeca, 2013; Paciello, Fida, Tramontano, Colli, & Cerniglia, 2013).
MD and Antisocial Behaviour
Bandura (1991) has introduced the construct of MD to explain the determinants and mechanisms governing aggressive behaviours. MD refers to the moral-cognitive process by which individuals explain their own aggressive behaviour and its negative consequences in a socially and morally favourable light. In this regard, MD explains the eight mechanisms through which self-sanctions can be deactivated and affective self-evaluative reactions are avoided, leading to different types of harmful conduct, while preserving moral ideals and standards (Bandura, 1991). Overall, MD may be viewed as a type of “rationalization” of antisocial, wrongful, and harmful behaviours that are considered in light of a desired goal.
A number of findings have shown that the above-mentioned eight mechanisms can be traced back to a common latent variable that makes people more or less inclined to use mechanisms of MD (Bandura, Barbaranelli, Caprara, & Pastorelli, 1996; Bandura, Caprara, Barbaranelli, Pastorelli, & Regalia, 2001; Gini, Pozzoli, & Hymel, 2014). The development of MD is influenced, especially during adolescence, by the interactions between individual characteristics and social context in which one operates (Fontaine, Fida, Paciello, Tisak, & Caprara, 2012; Hyde, Shaw, & Moilanen, 2010). A growing body of literature has recently demonstrated the predictive power of MD on deviant and criminal careers and its associations with a variety of manifestation of antisocial behaviours during adolescence (Bandura et al., 2001; Cardwell et al., 2015; Fontaine et al., 2012; Gini et al., 2014; Hyde et al., 2010; Menesini et al., 2003; Mulder, Brand, Bullens, & van Marle, 2011; Pelton, Gound, Forehand, & Brody, 2004; Shulman, Cauffman, Piquero, & Fagan, 2011). Yet, almost all of these evidences derived from studies delivered in community samples. For this reason, the research in clinical settings on the association between adolescents’ MD and their problematic behaviours may provide important information for the development of interventions aimed at reducing adolescents’ problematic behaviours.
Aims and Hypotheses
The pilot study presented in this article aims to explore the role of self-enhancement and self-transcendence, respectively, “self-oriented” and “others-oriented” PVs, and MD, in understanding moral-cognitive processes leading to aggressive and rule-breaking behaviours, both in a community sample and in a clinical sample of adolescents with DBD diagnosis. More specifically, we first examined the differences in self-enhancement, self-transcendence, and MD by comparing profiles of both clinical and community samples, controlling for gender differences. To this regard, we expected that adolescents with DBD would give more importance to self-enhancement PVs such as success and power, and would be more inclined than others to use MD to legitimize their aggressive and rule-breaking behaviours. Moreover, we hypothesized that clinical adolescents would give less importance to self-transcendence PVs in light of their relational difficulties (Barker & Salekin, 2012). Second, we also examined if and how PVs affect MD, and if these moral dimensions promote antisocial and harmful behaviours, taking into account both gender and group belonging, that is, either clinical or community sample. The explanatory value of MD and PVs in respect to aggressive behaviours had been already empirically tested on community adolescents’ samples in previous studies with the same or a similar construct (Barriga, Morrison, Liau, & Gibbs, 2001; Beerthuizen & Brugman, 2013; Paciello et al., 2013). Nevertheless, previous studies have not investigated the relation among PVs, MD, and harmful behaviours considering a clinical context. More specifically, controlling for gender and belonging to the clinical group, we hypothesized the following:
Self-enhancement fosters the recourse to mechanisms of MD and rule-breaking and aggressive behaviours. As self-enhancement values prioritize an individual’s own interest, consequently they may foster cognitive processes legitimizing the recourse to harmful and antisocial behaviour to achieve one’s own goals.
Self-transcendence holds back the recourse to mechanisms of MD and prevents rule-breaking and aggressive behaviours. As self-transcendence values prioritize the sense of responsibility and belonging, it is more difficult to activate self-serving mechanisms and avoid self-sanctioning feelings related to adoption of behaviours damaging others, and violating social and moral norms.
The importance of analysing these relations in adolescence is becoming more and more evident to inhibit crystallisation of beliefs and cognitive processes that sustain antisocial careers. In the long run, research on PVs, MD, and other cognitive factors involved in antisocial behaviours might contribute to the development of treatment models aimed at reducing these risk factors related to moral functioning, and thus preventing antisocial problems.
Method
Participants
Total sample was composed of 115 Italian adolescents (44.3% girls) with a mean age of 14.87 (SD = 1.31). Specifically, 85 adolescents constituted the community sample (55% girls; Mage = 15.01 years; SD = .41), whereas 30 adolescents were included in the clinical sample (13.3% girls; Mage = 14.56; SD = 2.28). Age and gender differences between groups were previously tested: Age differences were found to be non-significant, whereas a significantly higher proportion of girls was found in the community sample, χ2(1) = 18.09, p < .001. All participants did not vary in terms of ethnicity, and most of them lived with their parents. The participation rate was high during data collection, with 90% participation from adolescents of the possible community sample (n = 94) and 93% for the clinical sample (n = 32).
Procedures
The community sample was recruited from a high school in Naples. A stringent consent procedure for the research was followed, including at various stages, parents’ consent and approval from school councils, while letting children decline their participation if they so chose. Adolescents were administered a set of scales tapping into different types of behaviours in their classrooms by two trained female experimenters and asked to complete paper-and-pencil tests individually (time to complete tests: 60 min). Before starting, the experimenter explained that their responses to the questionnaire would be absolutely confidential. When necessary, the experimenter offered clarifications on the behaviours being measured.
The clinical sample included children referred to our Outpatients Clinic (Pisa-Italy) and diagnosed as DBD on the basis of a clinical interview, the Kiddie Schedule for Affective Disorder and Schizophrenia for School-Age Present Lifetime Version (K-SADS-PL; Kaufman et al., 1997) administered to patients and parents by trained child psychiatrists. Sixteen of the patients presented an ODD, and 14 had CD, 6 (20%) had attention-deficit hyperactivity disorder (ADHD) comorbidity. Two patients dropped out and were excluded from the sample. Inclusion criteria for the participation in the current study were as follows: (a) Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) diagnosis of CD or ODD according to K-SADS-PL; (b) a total Wechsler Intelligence Scale for Children, 3rd ed. (WISC-III) IQ score above 85; (c) a Child Behavior Checklist (CBCL) externalizing score above 63; and (d) no psychotic status or associated neurological disorders. The study has received approval from the institutional review board of Stella Maris Scientific Institute of Child Neurology and Psychiatry (Pisa-Italy), and all participants and their parents provided an informed written consent.
Measures
The anonymous self-report survey included measures of PVs, MD, aggressive and rule-breaking behaviours.
PVs
We used the Portrait Values Questionnaire (PVsQ; Schwartz, 1992), which includes 23 items, each portraying a person (his or her aspirations, goals, and important aspects of his or her life). Participants were asked to rate how similar to the described person they felt to be, using a 6-point Likert-type (from 6 = very similar to 1 = very dissimilar) scale. For the present study, we took into account items related to self-transcendence and self-enhancement values. These dimensions were used in several developmental studies demonstrating the influence that these PVs have on harmful and unethical behaviour (Frimer & Walker, 2009; Menesini et al., 2013). In the present study, the Cronbach reliability coefficients of the above-mentioned dimensions are acceptable (.64 for self-transcendence and .70 for self-enhancement), albeit lower than those reported in literature (Paciello et al., 2013).
MD
We used the original scale created by Bandura and colleagues to study MD in adolescence (Bandura et al., 1996). The scale assesses proneness to MD from different forms of detrimental conduct in diverse contexts and interpersonal relationships. The full set of 32 items tap the eight different mechanisms by which moral self-sanctions can be disengaged from transgressive conduct. For each of the 32 items, adolescents rated on a 5-point Likert-type scale their degree of acceptance of moral exonerations for such conduct on an agree–disagree continuum (from 1 = strongly disagree to 5 = strongly agree). The MD scale was used in several developmental studies that have attested the predictive power of MD in fostering aggression, violence, and crime career during adolescence (Fontaine et al., 2012; Hyde et al., 2010; Shulman et al. 2011). In the present study, the Cronbach reliability coefficient was very high (.91), in line with previous studies (Gini et al., 2014).
Aggression and Rule-Breaking Behaviours
We used the Youth Self-Report (YSR; Achenbach & Rescorla, 2000). This checklist belongs to one of the most comprehensive evaluation systems for childhood and adolescence psychopathology. It is composed of 112 items; for each one, ratings were provided on a 3-point scale (from 2 = sometimes true to 0 = never true). The instrument targets to identify problems connected with Internalizing and Externalizing problems. Aggression and rule-breaking behaviours refer to the externalizing area, which is a tendency to express the problems outwards. The YSR is a well-known instrument in clinical and developmental literature; several studies have used YSR in the examination of aggressive and disruptive behaviours in community and clinical adolescent samples (Tackett, Krueger, Sawyer, & Graetz, 2003; van Lier, van der Ende, Koo, & Verhulst, 2007). In the present study, the Cronbach reliability coefficients of aggression and rule-breaking behaviours were acceptable (.77 and .68), albeit slightly lower than those reported in previous studies (Achenbach & Rescorla, 2000).
See Table 1 for measurement details and item examples.
Measurement Details.
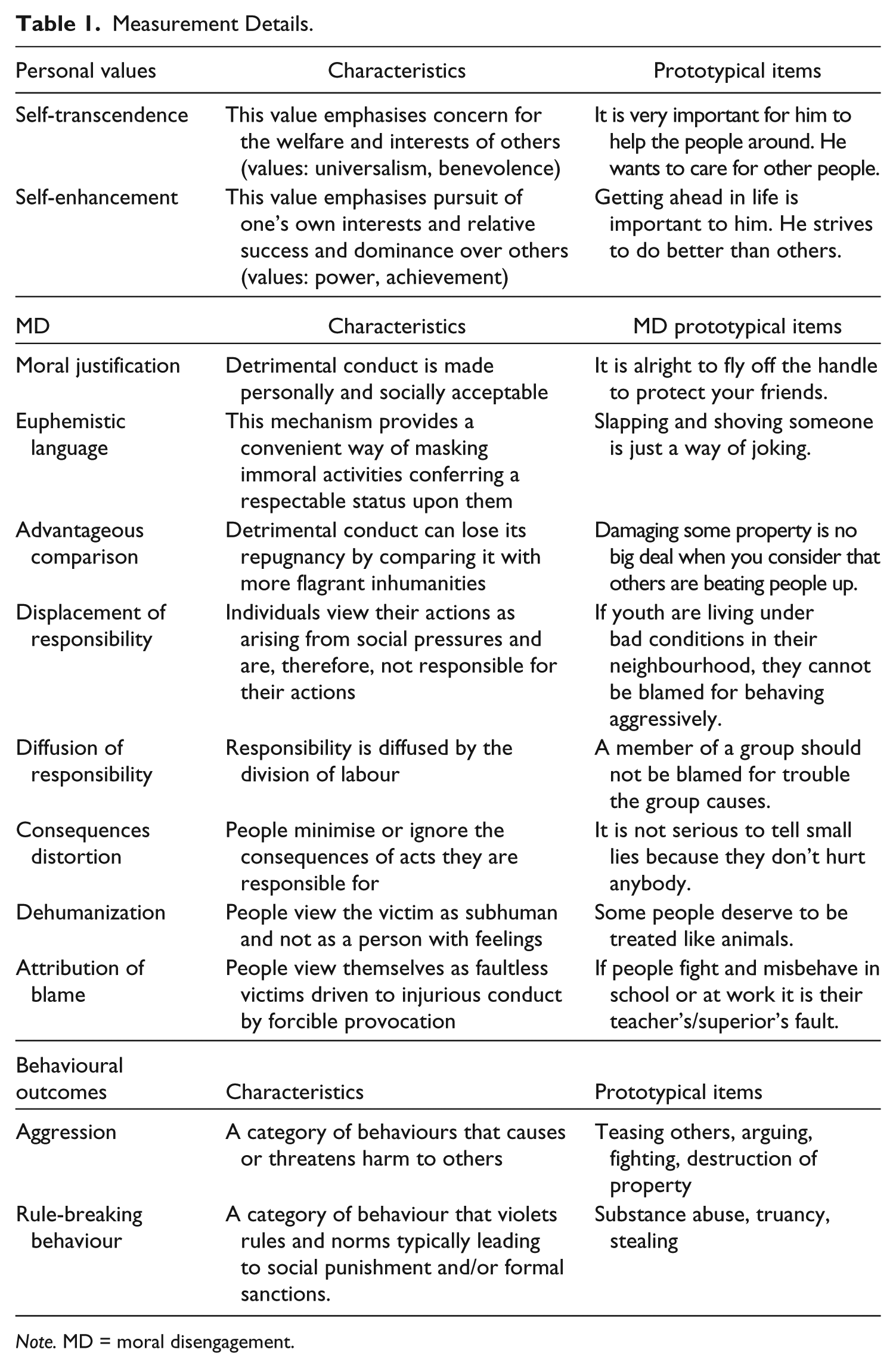
Note. MD = moral disengagement.
Data Analysis
Preliminary, descriptive, and correlational analyses were performed, and gender differences were examined. Subsequently, MANCOVA was used to determine if the clinical and community group presented significantly different levels for PVs, MD, aggressive and rule-breaking behaviours, using gender as the control variable in the analysis. Following the MANCOVA, individual ANCOVAs were used to examine more specifically group differences in each dimension. The profile analysis results were presented using T scores. Finally, to test our hypotheses, three hierarchical regression models were conducted. In the first model, we tested the influence of PVs on MD controlling for gender (1 = male; 2 = female) and group belonging (1 = community sample; 2 = clinical sample). In the other two regression models, we examined the contribution of PVs and MD to aggressive and rule-breaking behaviours. In particular, in the regression models, gender and group belonging were entered at Step 1, self-transcendence and self-enhancement were entered at Step 2, and MD was entered at Step 3. We also evaluated the influence of the interaction of PVs and group and MD and group on externalizing problems by entering at Step 4 the product of variables (Group × PVs and Group × MD). However, these analyses revealed no statistically significant interactions.
All statistical analyses were performed using SPSS v.15.0. Moreover, as there were less than 4% missing data, the analyses were performed on listwise covariance matrices.
Results
Preliminary Analyses
Observed means, standard deviations for all the study variables in the total sample are presented in Table 2. Before proceeding with the analysis, the normality of the variables was ascertained. Due to the non-normality of rule-breaking behaviour, we computed the root square of this variable to normalize it, as suggested by Tabachnick and Fidell (1989).
Descriptive Analyses.
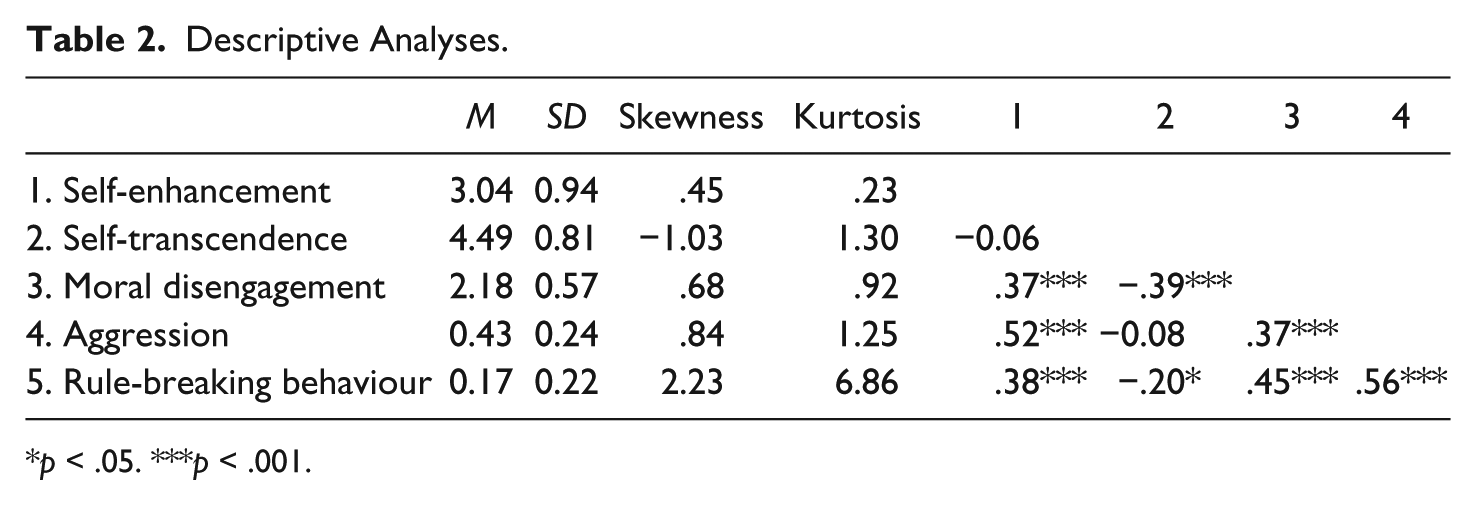
p < .05. ***p < .001.
Correlational analysis shows that (a) aggression is significantly and positively associated with self-enhancement and MD, (b) rule-breaking behaviours are significantly and positively linked to MD, (c) MD is significantly and positively associated with self-enhancement and negatively linked to self-transcendence, and finally (d) aggression and rule-breaking behaviours are significantly and positively associated (Table 2).
With regard to gender differences, males and females significantly differed on self-transcendence, F(1, 108) = 10.33, p < .01, η2 = .08; self-enhancement, F(1, 108) = 4.29, p < .05, η2 = .04; MD, F(1, 107) = 20.78, p < .000, η 2 = .16; and rule-breaking behaviour, F(1, 107) = 10.78, p < .000, η2 = .07. More specifically, females show higher levels of self-transcendence than males. However, males show higher levels of self-enhancement, MD, and rule-breaking behaviour than females.
Profile Analyses
With regard to group differences, the MANCOVA revealed a significant difference in PVs, MD, aggressive and rule-breaking behaviours between subject groups (Wilks’s λ = .58), F(5, 99) = 14.10, p < .001. Post hoc analyses of the separate ANCOVAs revealed significant differences in MD, F(1, 106) = 4.17, p = .04; aggression, F(1, 106) = 6.56, p = .01; and rule-breaking behaviour, F(1, 106) = 66.57, p < .001.
In particular, as shown in Figure 1, the clinical group shows significantly higher levels of MD (clinical T score: M = 54.43, SD = 9.77; community T score: M = 47.84, SD = 8.06), rule-breaking behaviour (clinical T score: M = 61.31, SD = 12.89; community T score: M = 46.27, SD = 4.81), and aggressive behaviour (clinical T score: M = 53.34, SD = 12.87; community T score: M = 48.89, DS = 8.66), compared with the community sample. Finally, the ANCOVAs showed a significant effect of gender for self-transcendence, F(1, 106) = 10.07, p = .01, and for MD, F(1, 106) = 4.17, p = .05.
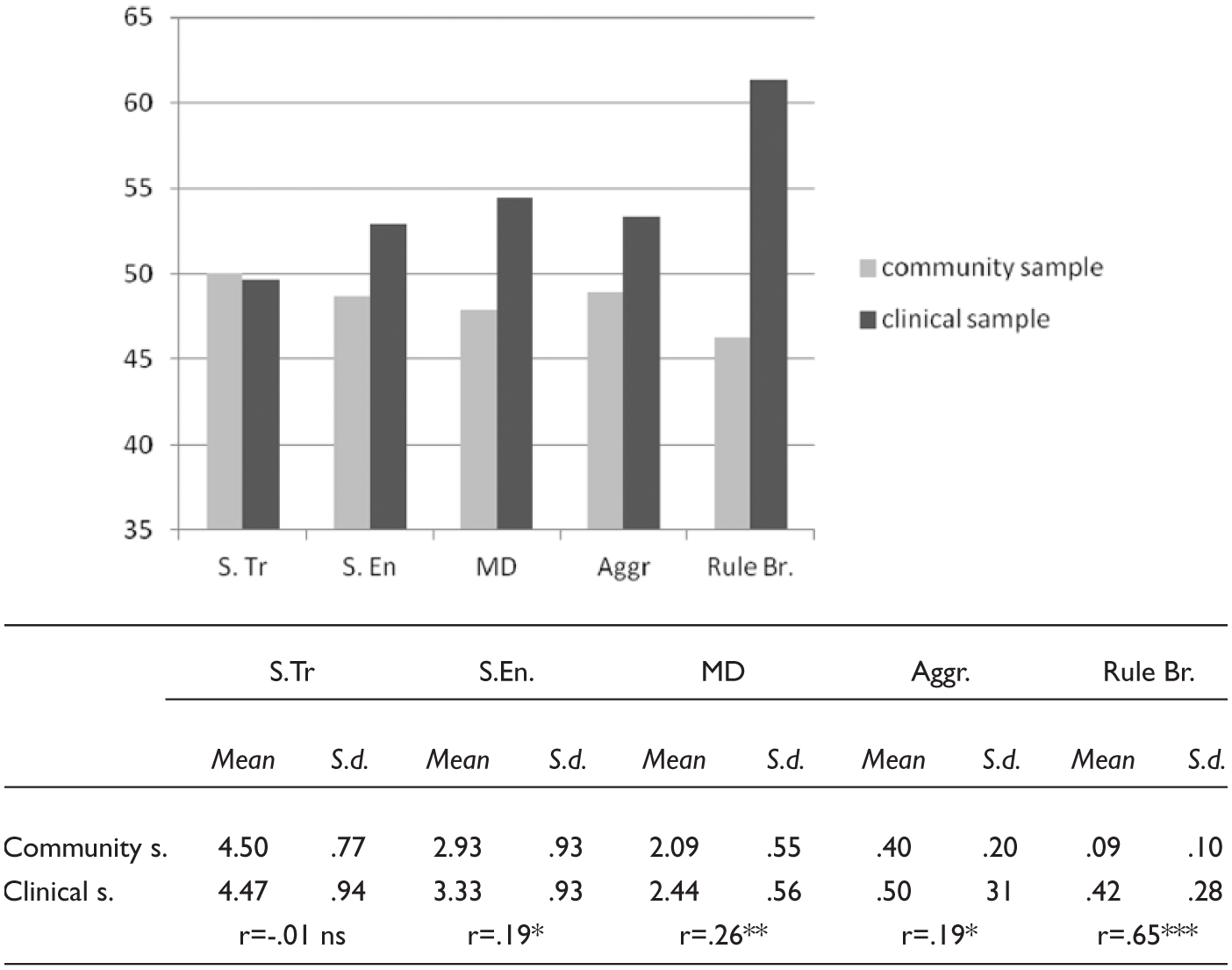
Clinical and community profile.
Regression Models
The first hierarchical regression model examined the influence of PVs on MD controlling for gender and group belonging. The results attested that in addition to the contribution of gender and group belonging (19% of explained variance), PVs significantly predicted MD, that is, self-transcendence hinders the recourse to MD mechanisms, whereas self-enhancement fosters it. The second and third regression models examined the contribution of PVs and MD to aggressive and rule-breaking behaviours, respectively, controlling for gender and group belonging. The results attested that in addition to the contribution of gender and group belonging (06% of the variance in the case of aggression and 45% of the variance in the case of rule-breaking behaviour) in both models, self-enhancement significantly predicted behavioural outcomes. Moreover, in addition to the contribution of PVs (22% of the variance in the case of aggression and 05% of the variance in the case of rule-breaking behaviour) MD significantly fosters adolescents’ externalizing behaviours (Table 3).
Hierarchical Regression Models.
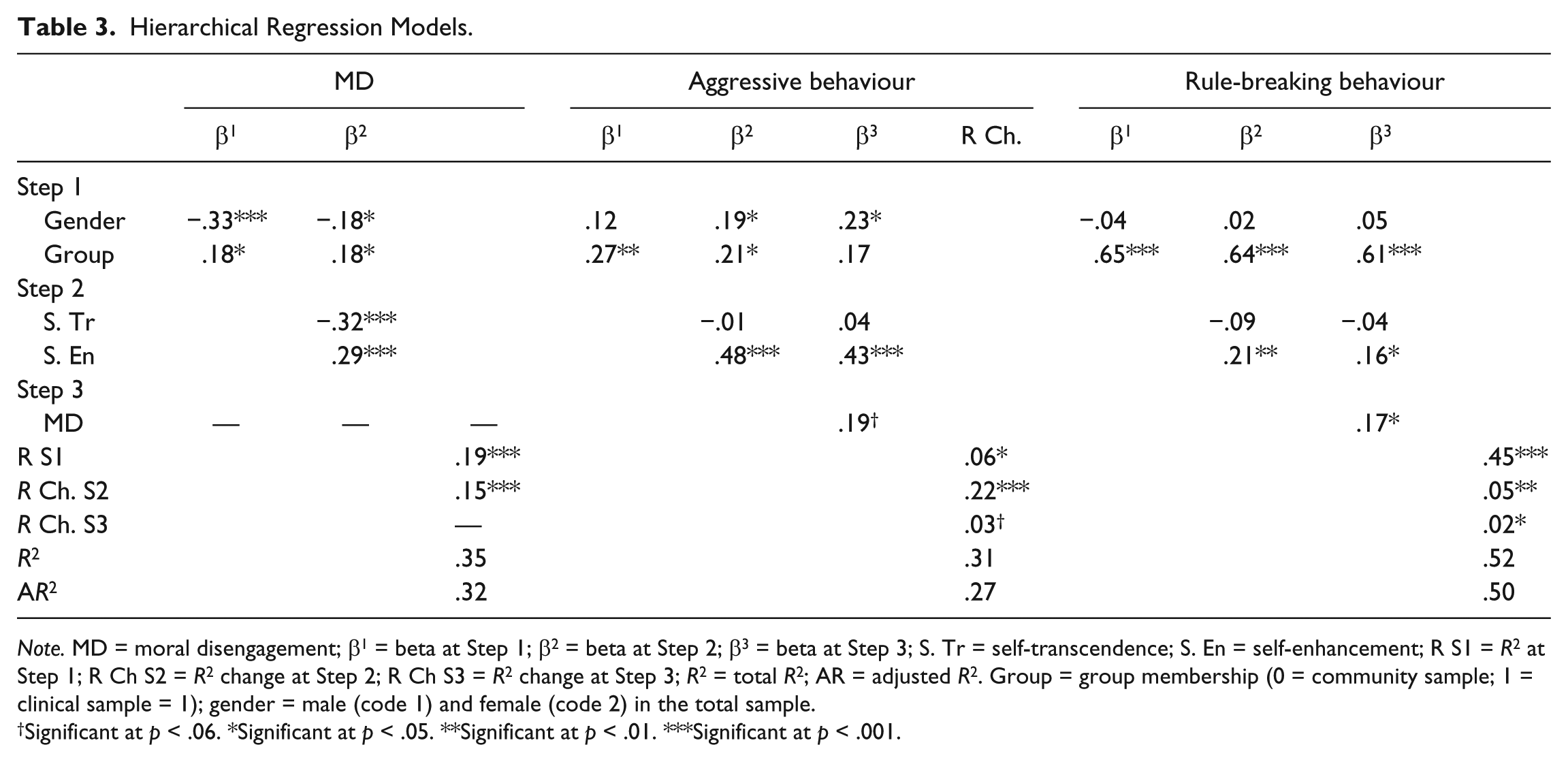
Note. MD = moral disengagement; β1 = beta at Step 1; β2 = beta at Step 2; β3 = beta at Step 3; S. Tr = self-transcendence; S. En = self-enhancement; R S1 = R2 at Step 1; R Ch S2 = R2 change at Step 2; R Ch S3 = R2 change at Step 3; R2 = total R2; AR = adjusted R2. Group = group membership (0 = community sample; 1 = clinical sample = 1); gender = male (code 1) and female (code 2) in the total sample.
Significant at p < .06. *Significant at p < .05. **Significant at p < .01. ***Significant at p < .001.
Discussion
The current study has supported the role of self-oriented values and MD in promoting and legitimizing harmful and rule-breaking behaviours in both clinical and community adolescent samples. Overall, the study showed that PVs and MD could be relevant to understanding the real-world behaviour of aggressive adolescents. The first interesting finding concerns the comparison between clinical and community samples on PVs and MD. With respect to the moral-cognitive variables, the most relevant difference between the two groups regards MD: The DBD adolescents showed significantly higher level of MD. No differences between these two groups are found on self-transcendence, although in adolescents with DBD the levels of self-enhancement are generally higher. The second interesting finding concerns the role of values and MD in accounting for the externalizing problems, in line with other studies (Barriga et al., 2001, Beerthuizen & Brugman, 2013; Paciello et al., 2013; Visconti, Ladd, & Kochenderfer-Ladd, 2015), self-enhancement values seem to be motivational determinants particularly relevant to the understanding of antisocial phenomena and MD could mediate the relation between self-interested goals and aggressive behaviour. With regard to self-enhancement values, the question regarding why some individuals give particular or exclusive weight to PVs such as power and achievement is a very challenging one. These PVs, indeed, are highly related to aggressive, rule-breaking attitudes and behaviours, and are consistent with aggressive youth’s high value for social goals of dominance and revenge (Lochman, Wayland, & White, 1993; McDonald & Lochman, 2011). High self-enhancement can make the individual give little importance to cooperation and sense of collectivity and community (Teisl, Rogosch, Oshri, & Cicchetti, 2011). In actual fact, these individuals tend to believe that the best way to pursue and achieve one’s goals is to resort to aggressive and coercive strategies and to the cognitive mechanisms that can legitimate them (Walters, 2007). The value that children and adolescents place on potential outcomes of attacking others has also been implicated in persistent aggression (Pardini & Byrd, 2011). Moreover, in line with previous findings (Paciello et al., 2013), we hypothesize that self-enhancement affects MD, which, in turn, affects the behaviour, especially rule-breaking behaviours. Oppositely, self-transcendence inhibits MD, and thus might indirectly prevent these harmful behaviours. The presence of a normal level of self-transcendence might suggest that MD has not yet fully settled. Effectively, the profile analyses attested that, even if these risk factors related to moral area (MD) are present in adolescents with DBDs, they can access other-oriented PVs, generally associated with relational-affective motivation and sense of community. For example, self-transcendence could refrain MD by promoting prosocial behaviour and by reducing the emotional distance between perpetrator and victim. Furthermore, increasing investment in other-oriented PVs can affect the frequency of positive peer interactions and the formation of quality relationship with peers. This, in turn, may lead to opportunities to develop more competent social skills. This dimension might be very important when planning interventions on cognitive processes in adolescence, a phase of life in which moral-cognitive processes such as MD could become stable (Paciello et al., 2008). Future studies might verify if interventions in small groups might decrease the recourse to MD also through an increased interest toward the other. In our opinion, in group therapy, adolescents have more opportunity for social/peer interactions and, therefore, they are less likely to be self-focused and morally disengaged (e.g., group therapy promotes emotion sharing with peers, and thus it could improve children’s interest toward the other).
Implications for Assessment and Treatment
During adolescence, it is still possible to prevent the typical escalation leading from conduct problems to more severe antisocial behaviours. Our findings on the role of PVs and MD in understanding disruptive behaviour in a clinical and community sample could provide some indications for assessment and therapeutic intervention. In the first phase of an intervention, it could be clinically helpful to assess PVs as emerging guiding principles in adolescence, and MD as a self-serving cognitive mechanism aimed at avoiding moral sanction, and moral feelings related to adolescents’ disruptive behaviours. Including these moral dimensions in the clinical assessment of DBD allows a deeper understanding of the overall psychological functioning of these adolescents.
In line with these findings, by identifying PVs and MD in adolescents, clinicians may be better able to target the motivational (PVs) and self-serving mechanisms (MD) behind aggressive behaviours. A specific intervention addressing MD and PVs, during a cognitive behavioural therapy, may affect DBD and increases the treatment gains. Based on our results, possible goals of this specific intervention could be as follows: (a) enhancing the patient’s choice of investing in self-transcendence PVs, (b) decreasing the overinvestment in self-enhancement PVs, and (c) reducing the stable recourse to MD, which allows adolescents to systematically avoid moral-emotional reactions such as guilt and remorse. Devaluing aggressive solution when engaging the adolescent in problem solving could be an important step in decreasing their overinvestment in self-enhancement PVs. Particularly, a comprehensive treatment program should, according to McGlynn, Hahn, and Hagan (2013), Lochman, Powell, Whidby, and FitzGerald (2012), and Dodge and Godwin (2013), amply resort to cognitive restructuring to modify the numerous cognitive biases (e.g., other blame for their aggressive behaviours) noticeable in antisocial individuals. In fact, these biases could sustain the MD mechanisms and the investment in self-oriented PVs; this, in turn, could be considered risk factors for increasing aggressive behaviours.
To reach these objectives, within the therapeutic protocol, a series of group activities could be integrated, promoting the investment in self-transcendence PVs and fostering the employment of cooperative behaviours. The positive social experience with peers can enhance other-oriented PVs, which could subsequently be incorporated into one’s moral self-system. Regarding the role of parents, in the same vein it might be particularly useful to focus on rewarding adolescents for engaging in prosocial behaviours or activities rather than only punishing them for their aggressive and disruptive behaviours (Moretti & Obsuth, 2009).
Although there are several efficacious treatments for DBDs (Eyberg, Nelson, & Boggs, 2008), few studies have examined the extent to which decreasing the levels of MD (but not those of self-oriented PVs) may beneficially affect adolescent’s treatment outcome (Shulman et al., 2011). Especially for the development of more and more efficacious clinical interventions in adolescence, during which antisocial conduct can produce irretrievable losses of life options, interventions should include not only strategies to improve self-control and problem-solving skills (Garland, Hawley, Brookman-Frazee, & Hurlburt, 2008) but also strategies to improve the individual’s moral engagement. Indeed, an effective treatment for externalizing problems should help the individual countercheck the cognitive processes and mechanisms of MD, designing specific and evidence-based interventions capable of modulating these variables.
Moreover, the PVs and the existential ideals related to the desired conditions of the Self and of the world (Schwartz, 2010) seem to be motivational determinants, particularly relevant to the understanding of antisocial phenomena, as discussed above. With regard to the latter, the question why some individuals give particular or exclusive weight to PVs such as power and achievement is particularly relevant. These PVs, indeed, are highly related to aggressive, rule-breaking attitudes and behaviours. High self-enhancement, for example, can make the individual give little importance to cooperation and sense of collectivity and community (Teisl et al., 2011). In actual fact, these individuals tend to believe that the best way to pursue and achieve one’s goals is to resort to aggressive and coercive strategies and to the cognitive mechanisms that can legitimate them (Walters, 2007). The value that children and adolescents place on potential outcomes of attacking others has also been implicated in persistent aggression and in perception of victim suffering (Pardini & Byrd, 2011). In line with this, in our opinion an in-depth study of this matter is very important from both a preventive and a clinical perspective.
Limitations and Future Studies
Our findings have underlined the importance of an early detection of the moral structures and processes, such as PVs and MD, in clinical settings, because they can provide the cognitive framework within which aggression and rule-breaking behaviours appear appropriate and acquire legitimacy. Overall, the results suggest that (a) the clinical group is more likely to show self-oriented values and MD; (b) in general, the higher the priority adolescents give to other-oriented values, the less they resort to MD; and (c) the higher the priority adolescents give to self-oriented values and the higher the recourse to MD mechanisms, the more they show externalizing problems. The detection of predisposing and maintenance factors, such as PVs and MD, seems to be a particularly relevant area of clinical research to set a prompt intervention of those behaviours (Perren & Hornung, 2005; Posada & Wainryb, 2008).
However, in this article we have presented only a pilot study which needs to be replicated in larger clinical samples. Due to the sample size, in fact, we were only able to consider group and gender as covariates. The small sample size and cross-sectional nature of our data represent methodological limitations and make impossible for us to infer causal relationships between variables and to test whether model relationships are gender invariant. These limitations should be addressed through the replication of the study in other clinical contexts with larger and longitudinal samples of adolescents to test for the generalizability of the findings. In particular, from an intervention development perspective, it would be more informative to look at relationships among values, MD and externalizing problems in a larger clinical sample.
Moreover, self-report measures have been administered for the variables considered in the theoretical model. It is well established that shared variance due to common method could represent a limitation of this type of studies. The findings of this study need to be indeed corroborated by means of other sources of information, such as objective reports or other ratings regarding externalizing problems. For example, it could be important that parents of community sample can also be involved in a similar research to better compare adolescents’ behavioural profiles.
Finally, further studies might investigate how a psychotherapy intervention addressing PVs and MD could prevent antisocial outcomes adopting a longitudinal perspective and considering other factors related to moral development such as moral-emotional aspects (e.g., emotional callousness, guilt), previous experiences (e.g., victimization), and environmental factors (e.g., deviant culture) that could affect the development of antisocial outcomes.
Footnotes
Acknowledgements
Special thanks to Federica Ciaponi and Graziella Auricchio for their assistance on this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.