
Abstract
This study examined whether the disposition of juvenile justice encounters among youth with severe emotional disturbance was associated with the likelihood of recidivism. Court dispositions, such as probation and diversion, as well as Medicaid-funded out-of-home mental health treatment, were compared. Data sources included the Florida Department of Juvenile Justice and Medicaid claims data. Youth receiving probation had the highest recidivism rates. Among youth in out-of-home treatment, those receiving treatment in foster care services had the lowest recidivism rates. Youth placed into a diversion program were less likely to be re-arrested for a felony, whereas youth receiving inpatient psychiatric services were less likely to be re-arrested for a misdemeanor. Mental health treatment may reduce the likelihood of youth continuing on increasing criminal trajectories.
Introduction
The relationship between judicial responses to juvenile criminal behavior and future offending behavior has been the subject of considerable research. Although there are many variations, typical judicial interventions include juvenile detention, probation, or diversion. Gatti, Tremblay, and Vitaro (2009) compared future adult criminal justice involvement for youth that received specific types of juvenile justice interventions (non-supervisory, supervisory, or institutional). Youth placed in institutional settings had greater justice involvement as adults, which may indicate negative consequences from punitive institutional placements. In addition, Bayer and colleagues found evidence of negative peer effects among youth in juvenile corrections who have committed similar crimes (Bayer, Hjalmarsson, & Pozen, 2009). In their review of the literature, Lipsey and Cullen (2007) found that longer prison terms did not lead to a reduction in recidivism.
One alternative to detention is to place youth on supervised probation. Lower re-arrest rates have been found for youth placed on probation compared with secure confinement (Loughran et al., 2009; Ryan, Abrams, & Huang, 2014). Probation was most effective when combined with rehabilitation treatment (Lipsey & Cullen, 2007; Wooldredge, 1988). Numerous community-based programs are available that have been associated with reductions in juvenile justice recidivism including family-functional therapy (Alexander & Parsons, 1982), multisystemic therapy (Henggeler, Schoenwald, Borduin, Rowland, & Cunningham, 2009), multidimensional treatment foster care (Chamberlain & Reid, 1998), Wraparound (Kamradt, 2000), and cognitive behavioral therapy (Jewell, Malone, Rose, Sturgeon, & Owens, 2015). Such services are best delivered within a system of care where the mental health and criminal justice systems coordinate and integrate services (Foster, Qaseem, & Connor, 2004).
Although community-based treatment interventions can occur while youth are on probation, diversion programs minimize formal court intervention and justice costs while providing some supervision of offending youth (Cuellar, McReynolds, & Wasserman, 2006). The premise of diversion programs is to treat the underlying problem of juveniles and reduce future criminal activity. When diversion services occur soon after arrest, they can involve youth and their families in beneficial interventions at a point when they are more receptive to outside assistance, thus potentially reducing treatment entry and engagement problems (Dembo, Wareham, & Schmeidler, 2005).
One reason why community-based treatment programs are effective is their emphasis on youth mental health. Mental health problems are extremely common among delinquent youth. Among youth who have been arrested, one study found that 31% of youth had received services from the mental health system (Rosenblatt, Rosenblatt, & Biggs, 2000). Youth with emotional disturbances who enter juvenile detention may become further traumatized leading to worsening mental health problems (Kupers, 1999). Two studies of youth in juvenile detention found between 60% and 68% met the diagnostic criteria for a mental health disorder (Teplin, Abram, McClelland, Dulcan, & Mericle, 2002; Wasserman, Ko, & McReynolds, 2004). Common psychiatric disorders include disruptive behavior disorders, anxiety disorders, affective disorders (major depression, mania), and attention-deficit disorders (Teplin et al., 2006). Comorbid substance abuse problems are also common among youth in the justice system (Teplin et al., 2006).
A number of theories could be used to explain why youth with mental health disorders are at increased risk of justice involvement. Moffitt (1993) developed a theory to explain the life course persistent (including high frequency persistent and low-level chronic offending) and adolescent limited offending behavior. Life course persistent criminal behavior results from neurological deficits and failed parent–child relationships early in childhood. Behavior problems during childhood lead to increasingly limited opportunities as the youth grows up, leading to an increased risk of persistent offending. In particular, youth suffering from depression, phobias, or anxiety tend to experience social withdrawal as a child and are at risk of low-level chronic offending. Adolescent limited offending occurs when youth are not exposed to the risk factors consistent with low-level chronics and life course persisters. Instead, adolescent offending is a function of environmental and peer pressures during adolescence. However, Moffitt (2007) suggested that some youth who would otherwise be adolescent limited offenders become ensnared in the system and thus develop into chronic offenders. Youth can become ensnared due to incarceration, drug addiction, and a lack of education, which are all common among youth with serious emotional disturbance. Youth with emotional disturbances have characteristics associated with low-level chronic offending and the potential for becoming ensnared in the system. Consequently, offending behaviors occur through the remainder of childhood and into adulthood (Baillargeon, Binswanger, Penn, Williams, & Murray, 2009; Constantine, Andel, Robst, & Givens, 2013; Constantine et al., 2010).
In many cases, community-based services can be provided to youth while they reside in the home with their parent(s). However, in some cases, the severity of illness or problems in the child’s environment requires that the child be removed from the home for mental health treatment. There are three typical forms of out-of-home (OOH) mental health treatment: inpatient psychiatric residential programs, therapeutic group home (TGH) care, and treatment foster care (TFC) (see Armstrong et al., 2008, for a detailed description of each OOH treatment setting). Inpatient psychiatric residential programs typically provide short-term (6 months or less) mental health treatment services that include crisis intervention; biopsychological and/or psychiatric evaluation; close monitoring by staff; medication; individual, family, and group therapy; and connections to community services after discharge. In these locked residential facilities, youth live, attend school, and receive treatment. Access to the community is limited. TGH services are community-based psychiatric residential treatment services for young people with emotional and behavioral problems. TGH services occur in a structured group environment with up to 12 youth that is similar to but less restrictive than inpatient facilities. Residents attend regular schools and have greater access to the community. TFC provides intensive treatment in a licensed treatment foster home. TFC provides both long-term and crisis support in a structured home-like setting, with the goal of working toward reunification with the family of origin or a foster family. Although youth mental health is the focus of services in each setting, improvements in mental health are expected to have beneficial effects on delinquent behavior as well.
Youth may enter OOH treatment as a component of diversion or probation, or be completely independent of court action. Research evaluating OOH treatment has found mixed results. Emotional and behavioral problems tend to improve during treatment (e.g., Hair, 2005); however, these gains are not maintained after discharge (e.g., Barth et al., 2007; Hooper, Murphy, Devaney, & Hultman, 2000). There was also no change in justice involvement after residential mental health treatment (Pullmann, 2011). Differences in justice involvement have been found across OOH treatment settings. A series of studies by Chamberlain and colleagues found that youth served in multidimensional TFC, a highly structured TFC program, had better outcomes than youth in group homes (e.g., Chamberlain, 1990; Chamberlain & Reid, 1998). Barth et al. (2007) and Robst, Armstrong, and Dollard (2011) found better outcomes for youth in TFC compared with residential (inpatient and group home) treatment, whereas Lee and Thompson (2008) found no significant difference in justice outcomes for youth treated in group homes and TFC.
Although comparisons of outcomes across different OOH settings are informative, it does not determine whether OOH treatment leads to better outcomes than judicial interventions such as probation or diversion for in-home services. For example, the lack of a significant change in justice outcomes does not necessarily indicate a lack of effect as even a relatively small or no reduction in arrest rates may represent an important effect among youth at risk of increasing severity and frequency of offending. One challenge to evaluating the effectiveness of OOH treatment in reducing justice involvement is the lack of a clear comparison group of youth receiving in-home services. Youth who receive community-based services while living at home may not be comparable with youth who receive OOH treatment services due to differing severity of illness or differing home environments. Thus, it is important to compare youth receiving OOH treatment services with comparable youth receiving other judicial interventions.
This article examined whether the disposition of a juvenile justice encounter was associated with the likelihood of juvenile justice recidivism among youth with severe emotional disturbance. The study compared the risk of recidivism among youth with a severe emotional disturbance who received probation, diversion, or OOH mental health treatment. However, instead of selecting a random sample of justice involved youth with severe emotional disturbance, the sample contains youth who received OOH mental health treatment during the study time period. The limitation to youth who received OOH treatment at some point reduced heterogeneity within the sample as all youth were Medicaid-enrolled, had a severe emotional disturbance that merited OOH treatment, were at risk of continued justice involvement, and had a high likelihood of a low socioeconomic background. In addition, we determined whether treatment in different settings (inpatient, group home, or TFC) had differential effects on recidivism compared with judicial interventions (probation, detention). Given the long-term negative consequences of repeated juvenile justice involvement, it is important to identify interventions that may improve future outcomes for youth at high risk of continued involvement in the justice system.
Method
Data
There were two primary data sources used to examine children involved in both the OOH treatment system and the juvenile justice system. Florida Medicaid claims data were used to identify all children and adolescents who received any of the three types of Medicaid-funded OOH mental health treatment, including Inpatient (provided through the Statewide Inpatient Psychiatric Program, SIPP), TGH, and TFC, in fiscal years 2002-2003 through 2007-2008 (July 2002-June 2008). The sample period began in the 2002-2003 fiscal year because it was the first year that therapeutic group care was a covered Medicaid service, whereas the sample period for the data available for this study ended with 2007-2008 fiscal year. Identifiers for the 5,521 youth with OOH treatment were matched with Department of Juvenile Justice data using a combination of matching methods including individual identifiers and deterministic matching using name, date of birth, and gender. Deterministic matching was necessary due to a high rate of missing Social Security numbers in Florida Juvenile Justice (JJ) data. Thus, the matched data provided a sample of youth who had a diagnosed mental illness that was sufficiently severe to require OOH mental health treatment and also had contact with the juvenile justice system. Youth without a diagnosed mental health diagnosis or without juvenile justice contact were excluded from the analysis.
To be consistent with available Medicaid data, only arrests after July 1, 2002, for felony or misdemeanor charges were included in the analysis. The intervention was defined based on a combination of the judicial disposition and whether the youth received OOH treatment. Only arrests that resulted in referral to a diversion program or probation were included. Arrests that resulted in juvenile commitment were excluded because the data lacked release dates. As such, we could not determine when the youth returned to the community. Arrests where charges were not filed (and the youth did not receive diversion services) were also excluded because guilt is unclear. Data on OOH mental health treatment were from the Medicaid claims files and included the type of OOH treatment and the start and end dates of treatment. Thus, the intervention was defined as the type of OOH treatment, and in the absence of OOH treatment, the court disposition of the case.
Only arrests where the intervention occurred within 90 days of the arrest were included. We focused on a short time frame after the initial arrest for two reasons. First, Dembo et al. (2005) emphasized the importance of having diversion programs intervene shortly after the arrest. Second, court dispositions are potentially endogenous. The disposition of the initial arrest may be influenced by the youth remaining out of trouble or conversely being re-arrested. A shorter time frame reduces potential problems with the disposition of the original arrest being dependent on follow-up behavior.
The outcome of interest, JJ recidivism, was examined over a 6-month period while the youth was residing in the community. For youth without OOH treatment, the time period was 6 months after the disposition date. The timing of the 6 months varied across youth in OOH treatment depending on placement. For youth with TFC or TGH placements, a 6-month period was examined after the start of the treatment episode. The time in OOH treatment was included because prior research has shown that arrest rates remain high for youth in TFC and TGH treatment in part because both treatment modes are community-based (Robst et al., 2011). For youth receiving SIPP treatment, the time period did not start until treatment ended. SIPPs are restrictive facilities and youth have limited access to the community. Consequently, arrest rates are quite low while the youth is in treatment but tend to increase after release. Index arrests were excluded from the analysis when the youth was re-arrested prior to the disposition date or beginning of OOH treatment.
Analysis
Generalized estimating equations (GEE) were used to estimate associations between individual characteristics and the likelihood of re-arrest. The dichotomous dependent variable (re-arrest) calls for a logistic distribution. The regressions took the following form:

where i denotes respondents and e denotes episodes. The independent variables (X) included demographic variables (age and gender), whether the base arrest charge was a felony (ref: misdemeanor), charge (aggravated assault, weapons offense, burglary, grand larceny, assault/battery, petit larceny, obstruction of justice, violent drug laws, vandalism, trespass; ref: disorderly conduct), number of prior offenses, mental health diagnosis (schizophrenia/psychosis, mood disorder, acute reaction to stress, adjustment reaction, conduct disorder, attention-deficit hyperactivity disorder [ADHD]; ref: other), and the intervention after the base arrest (diversion program, SIPP treatment, TGH treatment, TFC treatment; ref: probation). Probation was the reference group to compare options that involved mental health treatment to an arrest intervention that did not explicitly involve treatment and involved deeper penetration into the justice system than diversion. In addition, we examined whether the interventions had different effects on the probability of being re-arrested for a felony and the probability of being re-arrested for a misdemeanor. The analyses were conducted using SAS procedure GENMOD. GEE is an appropriate method because it can accommodate a variety of distributions, and samples with repeated measures/observations on individuals (Hardin & Hilbe, 2002). Empirical (robust) standard errors were calculated to account for repeated observations on the same participant.
Results
Table 1 contains descriptive statistics. The 943 youth averaged 14.0 (SD = 1.9) years of age, and were 58% male, 31% Black, and 46% White. The most common mental health diagnoses were mood disorders (32.2%), ADHD, and conduct disorders (18.2%).
Demographic Characteristics.
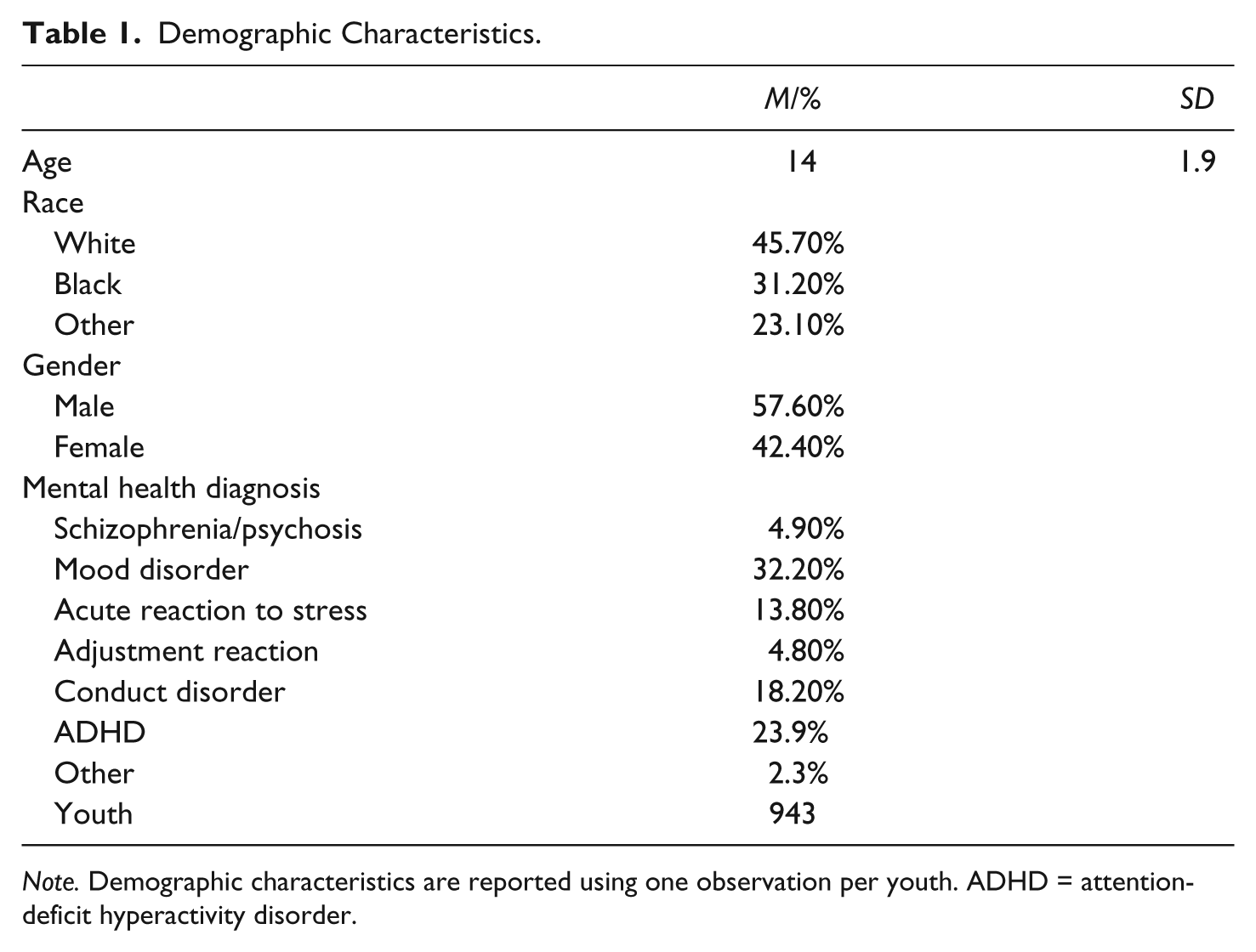
Note. Demographic characteristics are reported using one observation per youth. ADHD = attention-deficit hyperactivity disorder.
Table 2 contains descriptive statistics for the initial arrests and OOH treatment after the base arrest.After the inclusion and exclusion criteria, there were 1,388 arrests among 943 youth or 1.5 per youth. Despite all youth in the sample being involved in the OOH care system at some point in the study time frame, only 26.3% of the arrests had OOH treatment begin within 90 days. The most common OOH treatment was SIPP treatment (15.6%) followed by TGH treatment (5.3%) and TFC treatment (5.3%). Thirty-nine percent of the episodes resulted in placement into a diversion program, whereas 35% resulted in probation. Twenty-eight percent of the arrests involved a felony charge, with assault/battery (36.2%), aggravated assault/battery (13.1%), and petit larceny (12.8%) among the most common charges. Youth had averaged 1.45 prior arrests, and 41% had a re-arrest within the 6-month follow-up period.
Arrest Characteristics.

Note. SIPP = Statewide Inpatient Psychiatric Program; TGH = Therapeutic group home; TFC = Treatment foster care.
Table 3 contains rates of recidivism for youth by type of intervention. Youth placed on probation or who received TGH treatment had the highest rates of recidivism as well as the high rates of felony and misdemeanor arrests. Youth in diversion programs also had rates of misdemeanor arrests similar to youth placed on probation. Youth receiving TFC services had the lowest rates of overall recidivism, felony, and misdemeanor arrests.
Rates of Recidivism.

Note. SIPP = Statewide Inpatient Psychiatric Program; TGH = Therapeutic group home; TFC = treatment foster care.
Table 4 contains the GEE regression results examining the probability of a re-arrest. The odds ratios (OR) indicate that youth treated in TFC had the lowest likelihood of being re-arrested (OR = 0.39, confidence interval [CI] = [0.23, 0.68]). Youth who received SIPP services (OR = 0.71, CI = [0.50, 0.99]) also had a lower likelihood of being re-arrested than youth placed on probation. Youth receiving diversion services (OR = 0.68, CI = [0.48, 0.95]) or TFC services (OR = 0.25, CI = [0.14, 0.47]) had a lower likelihood of being re-arrested for a felony charge. Significant differences in the probability of being re-arrested for a misdemeanor were also evident. Re-arrests for misdemeanor charges were less likely for youth receiving SIPP services (OR = 0.58, CI: 0.38-0.87) or TFC (OR = 0.23, CI: 0.12-0.46).
GEE Regression Results. Dependent Variable: Re-Arrest Within Six Months.
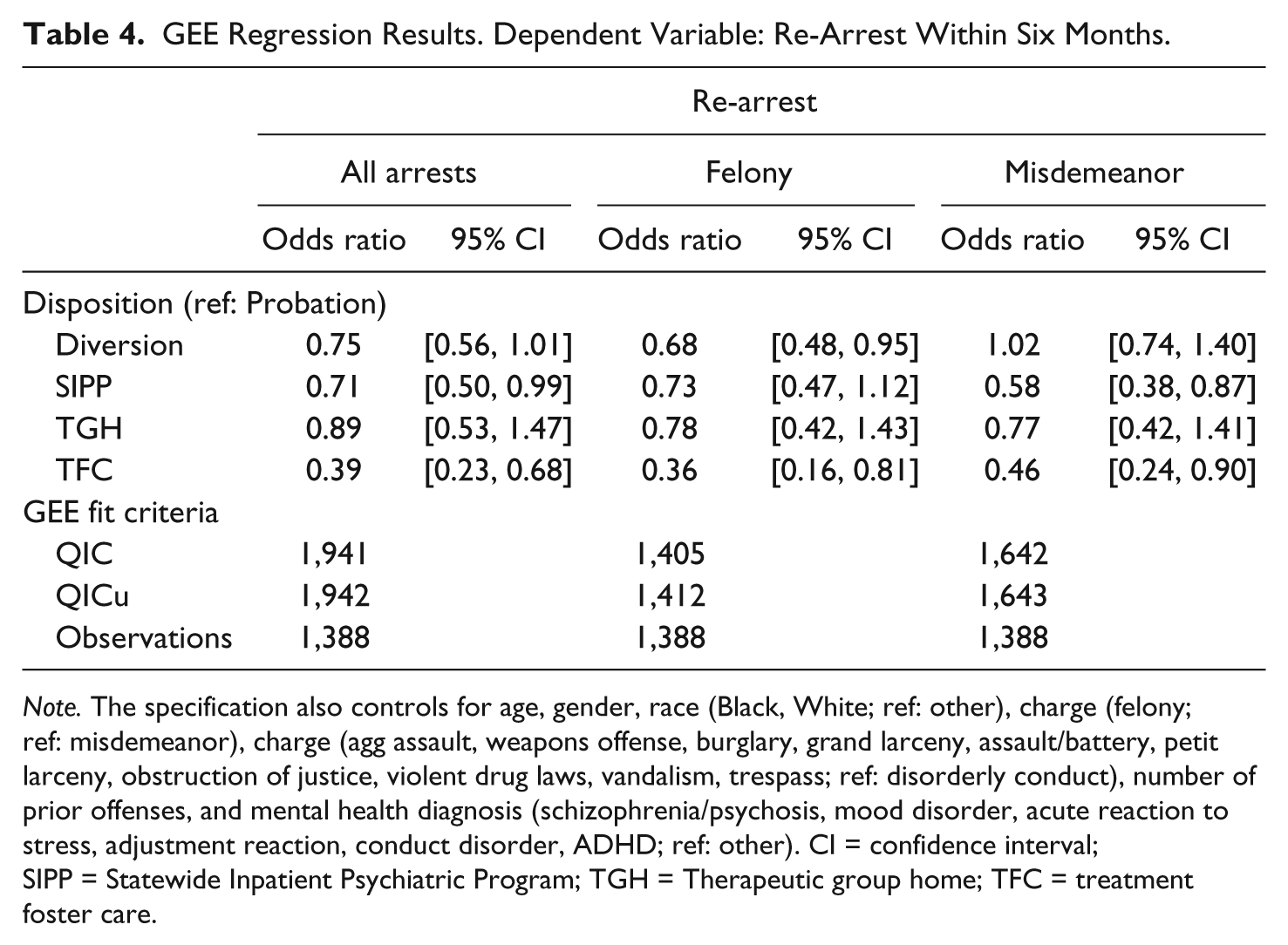
Note. The specification also controls for age, gender, race (Black, White; ref: other), charge (felony; ref: misdemeanor), charge (agg assault, weapons offense, burglary, grand larceny, assault/battery, petit larceny, obstruction of justice, violent drug laws, vandalism, trespass; ref: disorderly conduct), number of prior offenses, and mental health diagnosis (schizophrenia/psychosis, mood disorder, acute reaction to stress, adjustment reaction, conduct disorder, ADHD; ref: other). CI = confidence interval; SIPP = Statewide Inpatient Psychiatric Program; TGH = Therapeutic group home; TFC = treatment foster care.
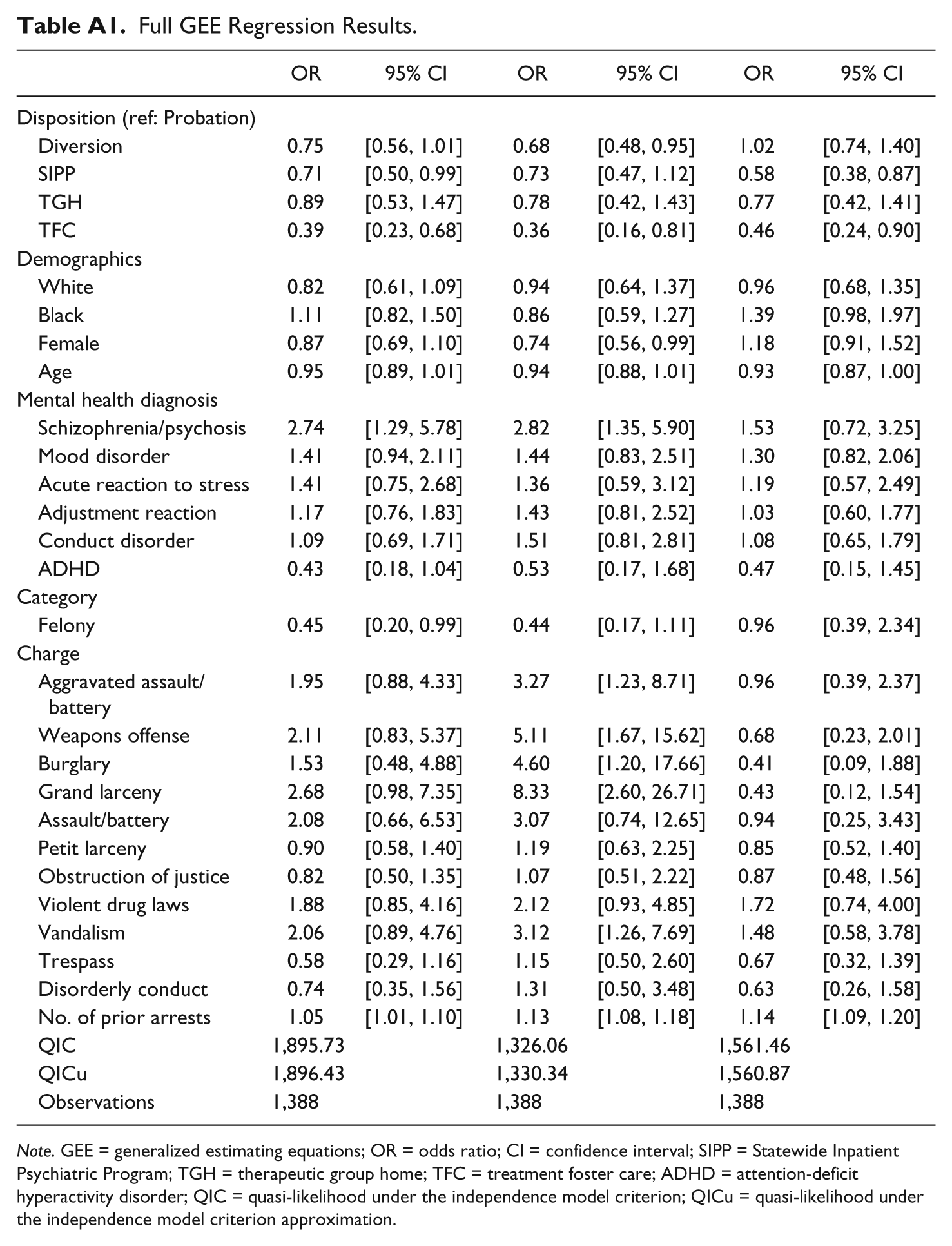
Among the other variables (see Appendix for full regression results), youth with a diagnosis of schizophrenia/psychosis were the most likely to be re-arrested (OR = 2.74, CI = [1.29, 5.78]), whereas youth with ADHD had the lowest odds (OR = 0.43, CI = [0.18, 1.04]). Youth with a felony charge were less likely to be re-arrested, particularly for another felony charge. However, re-arrest with a felony charge was more common when the initial arrest involved aggravated assault, weapons, burglary, grand larceny, or assault charges. The number of prior arrests was associated with an increased likelihood of re-arrest (OR = 1.05, CI = [1.01, 1.10]), re-arrest with a felony (OR = 1.13, CI = [1.08, 1.18]), and re-arrest with a misdemeanor (OR = 1.14, CI = [1.09, 1.20]).
Discussion
This study examined whether interventions after an arrest were associated with the likelihood of re-arrest for youth with severe emotional disturbance. Consistent with prior studies (Armstrong et al., 2008), the likelihood of re-arrest was quite high with more than 41% of youth being re-arrested within the 6-month follow-up period. Interventions after the initial arrest were associated with the likelihood of re-arrest. Youth receiving mental health treatment, either through a diversion program, residential inpatient, or TFC had a lower likelihood of re-arrest than people placed on probation. However, the results were not consistent across types of arrests. For example, diversion services were more strongly associated with a reduction in felony arrests. Thus, diversion services that take place soon after arrest can improve youth outcomes (Dembo et al., 2005). SIPP services were more strongly associated with a reduction in misdemeanor arrests. Only TFC services were consistently associated with a reduction in the risk of re-arrest. In addition, TGH services were not associated a reduction in arrests.
Among youth treated in OOH settings, those treated in residential settings (SIPP and TGH) had a higher probability of re-arrest in the 6 months after starting treatment than youth treated in TFC. This result is consistent with prior research that found high arrest rates while youth were in residential settings. The high arrest rates may result from several factors. The presence of negative peer effects in group facilities was one possible explanation for the high arrest rates during group home treatment (e.g., Barth, 2005; Dishion, McCord, & Poulin, 1999). Association with delinquent peers was found to account for much of the variance in antisocial behavior after treatment as well (Eddy & Chamberlain, 2000; Leve & Chamberlain, 2005). A second explanation is that group homes typically have specific procedures and thresholds in place that lead to more arrests. Ryan, Marshall, Herz, and Hernandez (2008), for example, found that youths in group homes were more likely to be arrested for threat offenses than their peers in foster care placements. Threatening behavior may automatically lead to police involvement in a group home, but foster parents may not involve police (Ryan et al., 2008). A third explanation is that, perhaps due to peer effects in group settings, youth are more likely to become part of a snared adolescence group (Moffitt, 2007). Such youth, due to repeated interactions with the system, teen pregnancy, limited education, and drug addiction, develop chronic offending patterns as a result of perceived negative life events.
Recidivism for youth receiving diversion services was similar to youth in residential mental health settings. Youth in diversion programs are less likely to be residing in group environments, but face numerous challenges. Mental health treatment for youth residing at home (or in regular foster homes) may not be as consistent or intensive as with OOH treatment settings. Youth are also likely to associate with the same peers as they did prior to the initial arrest because they continue to live at home. Youth in TFC settings may be able to receive needed treatment while developing new relationships with non-delinquent peers. Nevertheless, for youth who do not require (or are not eligible for) OOH mental health treatment, diversion services appear to provide significant improvement in outcomes over probation.
Given that the best predictor of future offending is past offending (Farrington, 2003; Piquero, 2008), it is important to limit juvenile justice involvement during adolescence and prevent behavior from developing into life-long criminal involvement. Although Moffitt (1993) suggests that the behavior of these children is the product of interactions that occur early in life and develop into cumulative disadvantage that is difficult to overcome, some interventions may reduce behavior causing arrest among adolescents and young adults. The results of this article are consistent with prior research that emphasizes the importance of treatment. However, it is important to emphasize that the results of this article should not be interpreted as encouraging removal of children from their homes. Most youth benefit from receiving needed services while remaining in the home. However, all youth in the study had severe emotional disturbance, had contact with the justice system, and received OOH treatment at some point in time during the study period. The results should be interpreted as indicating that youth who receive OOH treatment benefit most when receiving such services promptly after an arrest.
More than one third of the sample that received probation were arrested again during the study period. This supports the idea that youth receiving probation were less likely to receive community-based treatment and as a result had high recidivism rates. Future research needs to focus on youth on probation to determine whether youth are receiving evidence-based community mental health services, whether those services are provided with fidelity, and whether provision of those services reduces recidivism risk.
One implication of including the time during treatment is that the treatment is assumed to have a potential effect on JJ recidivism at the start of the TGH or TFC services. This was clearly a strong assumption, but results in a conservative estimate of the effect of OOH treatment. For example, if JJ recidivism was not affected until several months into treatment, then JJ recidivism might remain quite high in the initial months making OOH treatment appear less effective. Thus, the results for TGH, although consistent with prior studies, may also indicate that the effects of treatment take longer to appear.
There were several limitations to this study. First, it was limited by the fact that the sample was only from Florida Medicaid data so it may not generalize to the United States. Second, the data did not contain information on the type of diversion program or degree of adherence to the program. Third, we analyzed arrests as reported in state crime statistics. However, this most likely underestimates the numbers of crimes actually committed. In fact, our previous experience with arrest data from the Florida Department of Juvenile Justice was that more arrests were reported than contained in Florida’s official arrest records at the Florida Department of Law Enforcement. Fourth, we do not have data on time spent in juvenile commitment. Fifth, we lacked complete mental health service data for youth who received diversion services or were placed on probation. Thus, we were unable to determine the amount of mental health treatment, if any, they received after the arrest.
Conclusion
The receipt of mental health treatment promptly after an arrest may reduce juvenile recidivism. Efforts to reduce recidivism can include diversion programs that enable youth to remain at home, receive treatment, and limit their penetration into the justice system. For other youth, specific types of OOH mental health treatment may be the appropriate intervention. Appropriate assessment and referral are crucial to identify youth who may benefit from placing a priority on mental health treatment instead of punitive commitment programs.
Footnotes
Appendix
Full GEE Regression Results.
| OR | 95% CI | OR | 95% CI | OR | 95% CI | |
|---|---|---|---|---|---|---|
| Disposition (ref: Probation) | ||||||
| Diversion | 0.75 | [0.56, 1.01] | 0.68 | [0.48, 0.95] | 1.02 | [0.74, 1.40] |
| SIPP | 0.71 | [0.50, 0.99] | 0.73 | [0.47, 1.12] | 0.58 | [0.38, 0.87] |
| TGH | 0.89 | [0.53, 1.47] | 0.78 | [0.42, 1.43] | 0.77 | [0.42, 1.41] |
| TFC | 0.39 | [0.23, 0.68] | 0.36 | [0.16, 0.81] | 0.46 | [0.24, 0.90] |
| Demographics | ||||||
| White | 0.82 | [0.61, 1.09] | 0.94 | [0.64, 1.37] | 0.96 | [0.68, 1.35] |
| Black | 1.11 | [0.82, 1.50] | 0.86 | [0.59, 1.27] | 1.39 | [0.98, 1.97] |
| Female | 0.87 | [0.69, 1.10] | 0.74 | [0.56, 0.99] | 1.18 | [0.91, 1.52] |
| Age | 0.95 | [0.89, 1.01] | 0.94 | [0.88, 1.01] | 0.93 | [0.87, 1.00] |
| Mental health diagnosis | ||||||
| Schizophrenia/psychosis | 2.74 | [1.29, 5.78] | 2.82 | [1.35, 5.90] | 1.53 | [0.72, 3.25] |
| Mood disorder | 1.41 | [0.94, 2.11] | 1.44 | [0.83, 2.51] | 1.30 | [0.82, 2.06] |
| Acute reaction to stress | 1.41 | [0.75, 2.68] | 1.36 | [0.59, 3.12] | 1.19 | [0.57, 2.49] |
| Adjustment reaction | 1.17 | [0.76, 1.83] | 1.43 | [0.81, 2.52] | 1.03 | [0.60, 1.77] |
| Conduct disorder | 1.09 | [0.69, 1.71] | 1.51 | [0.81, 2.81] | 1.08 | [0.65, 1.79] |
| ADHD | 0.43 | [0.18, 1.04] | 0.53 | [0.17, 1.68] | 0.47 | [0.15, 1.45] |
| Category | ||||||
| Felony | 0.45 | [0.20, 0.99] | 0.44 | [0.17, 1.11] | 0.96 | [0.39, 2.34] |
| Charge | ||||||
| Aggravated assault/battery | 1.95 | [0.88, 4.33] | 3.27 | [1.23, 8.71] | 0.96 | [0.39, 2.37] |
| Weapons offense | 2.11 | [0.83, 5.37] | 5.11 | [1.67, 15.62] | 0.68 | [0.23, 2.01] |
| Burglary | 1.53 | [0.48, 4.88] | 4.60 | [1.20, 17.66] | 0.41 | [0.09, 1.88] |
| Grand larceny | 2.68 | [0.98, 7.35] | 8.33 | [2.60, 26.71] | 0.43 | [0.12, 1.54] |
| Assault/battery | 2.08 | [0.66, 6.53] | 3.07 | [0.74, 12.65] | 0.94 | [0.25, 3.43] |
| Petit larceny | 0.90 | [0.58, 1.40] | 1.19 | [0.63, 2.25] | 0.85 | [0.52, 1.40] |
| Obstruction of justice | 0.82 | [0.50, 1.35] | 1.07 | [0.51, 2.22] | 0.87 | [0.48, 1.56] |
| Violent drug laws | 1.88 | [0.85, 4.16] | 2.12 | [0.93, 4.85] | 1.72 | [0.74, 4.00] |
| Vandalism | 2.06 | [0.89, 4.76] | 3.12 | [1.26, 7.69] | 1.48 | [0.58, 3.78] |
| Trespass | 0.58 | [0.29, 1.16] | 1.15 | [0.50, 2.60] | 0.67 | [0.32, 1.39] |
| Disorderly conduct | 0.74 | [0.35, 1.56] | 1.31 | [0.50, 3.48] | 0.63 | [0.26, 1.58] |
| No. of prior arrests | 1.05 | [1.01, 1.10] | 1.13 | [1.08, 1.18] | 1.14 | [1.09, 1.20] |
| QIC | 1,895.73 | 1,326.06 | 1,561.46 | |||
| QICu | 1,896.43 | 1,330.34 | 1,560.87 | |||
| Observations | 1,388 | 1,388 | 1,388 | |||
Note. GEE = generalized estimating equations; OR = odds ratio; CI = confidence interval; SIPP = Statewide Inpatient Psychiatric Program; TGH = therapeutic group home; TFC = treatment foster care; ADHD = attention-deficit hyperactivity disorder; QIC = quasi-likelihood under the independence model criterion; QICu = quasi-likelihood under the independence model criterion approximation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.