
Abstract
Outcomes research in forensic mental health (FMH) has concentrated on reoffending as the principal indicator of success. Defining success in one-dimensional, negative terms can create a distorted view of the diverse objectives of the FMH system. This qualitative study examined the complexity of success from the perspectives of people in the FMH system. Interviews were conducted with 18 forensic service users and 10 forensic service providers. Data were analyzed inductively using thematic analysis to identify predominant themes. The participants conceptualized success as a dynamic process materializing across six different domains in the context of the FMH system: (a) normal life, (b) independent life, (c) compliant life, (d) healthy life, (e) meaningful life, and (f) progressing life. The results indicate that people who provide or use FMH services emphasize a broad range of processes and outcomes, apart from public safety, when they think about success.
Keywords
Sociologists have long recognized that it is misguided and unproductive to frame our social institutions as just being the means to a single end (Garland, 1993). Penal systems pursue a range of objectives other than crime control (Garland, 1991; Raynor & Robinson, 2009). Despite a few notable exceptions (e.g., Farrington, Gallagher, Morley, Ledger, & West, 1988), pathways to and from crime continue to be the central focus of criminology. The concentration of orthodox criminological inquiry on issues that are defined and deemed important by the state (e.g., interpersonal crime, criminal recidivism) has been challenged by critical scholarship (e.g., Hannah-Moffat, 2005; Michalowski, 2016), new theoretical perspectives, and innovative studies.
For instance, the subfield of positive criminology calls for greater recognition of how positive experiences and forces in a person’s life encourage lawful behaviour (Ronel & Elisha, 2011; Ronel & Segev, 2014). Similarly, desistance theories shift attention toward the relational processes and social contexts that support the development of positive identity and the discontinuation of offending over time (Farrington, 2007; Maruna & LeBel, 2010; McNeill, 2006). Several studies have forged new paths by studying positive outcomes among criminal justice and forensic mental health (FMH) populations (e.g., Munn & Bruckert, 2013; Viljoen, Nicholls, Greaves, de Ruiter, & Brink, 2011). Despite these welcomed advancements, there remains a tendency to privilege state-centric, public safety objectives over others. Although the new variables contributed by the aforementioned perspectives (e.g., positive experiences, protective factors, human agency, and prosocial identity) offer alternative ways of explaining changes in criminal behaviour, the field of criminology and FMH scholarship continues to be oriented toward crime control objectives. In other words, people are defined as a “success” primarily on the basis of whether or not they manage to stay away from crime for a specific duration. Several problems are associated with overly narrow and legalistic conceptualizations of success.
The first problem is methodological in nature. Even though it is the most important indicator of the impact of the criminal justice system, there is no commonly accepted measure of recidivism (Bonta, Dauvergne, & Rugge, 2003). Recidivism can be crudely defined as a return to crime following the conclusion of a sentence; however, there is substantial variability in the methods used to identify whether or not someone has returned to crime (Chambers et al., 2009). Many recidivism studies tell us nothing about changes that may have occurred in the nature and pattern of offending behaviour. No social indicator is perfect; recidivism certainly is no different. Given the known limitations associated with measuring recidivism, a predictable consequence of using it as the sole indicator of success is that people will be erroneously labelled as “successful” or “unsuccessful.” In turn, social institutions and interventions will be misdiagnosed as being effective or ineffective. It would make sense to study the FMH system, including the mechanisms underlying successes, using multiple indices of processes and outcomes.
The second problem is conceptual in nature. A systematic review of 308 published FMH intervention studies found that the most common outcome measure was criminal recidivism—comprising almost 40% of all outcome variables (Chambers et al., 2009). The next most common FMH outcomes were substance abuse, comprising 14% of all variables, followed by patterns of service use (10%), mental state (7.5%), and psychological functioning (7.5%). Quality of life comprised 0.6% of FMH outcome measures. Such findings lend support to criticisms that research in this area has excessively focused on public safety at the expense of other clinical, humanitarian, and rehabilitative objectives (Cohen & Eastman, 2000). Knowing whether a person has returned to crime reveals little about his or her quality of life, and the achievements or setbacks he or she may have experienced in other life domains. Surely, the validity of using recidivism as a sole indicator of success is doubtful in such cases when an individual terminates his or her offending behaviour but continues to live a life filled with deprivation or misery.
Over the past 30 years in the mental health and substance use fields, researchers and service providers have been moving away from defining success in one-dimensional, negative terms. First person accounts from people with mental illnesses provoked the idea that “the course of severe mental illness was not an inevitable deterioration” (Jacobson & Greenley, 2001, p. 482). Moreover, personal stories from people with mental illnesses suggested that their recovery was a lifelong process—not an event—of learning to manage and live well with mental illness (Davidson, O’Connell, Tondora, Styron, & Kangas, 2006). This paradigm shift led to complementing traditional mental health outcome indicators, such as symptom reduction, with other indices focused on the individualized needs, personal strengths, and subjective experiences of mental health recovery (Andresen, Caputi, & Oades, 2010; Davidson, Davidson, O’Connell, Tondora, & Lawless, 2005). In Canada, the push toward a mental health recovery paradigm, and away from the biomedical model, has been promoted by grassroots advocates and propelled by the ideals articulated in the nation’s first mental health strategy (Mental Health Commission of Canada, 2012).
Recently, there have been efforts to apply recovery principles to the FMH system (Livingston, Nijdam-Jones, Lapsley, Calderwood, & Brink, 2013; Simpson & Penney, 2011), but much of the FMH outcomes research remains fixed on crime control. Given the changing landscape of the FMH system, researchers ought to ask different kinds of questions that tap into the multiple objectives of the FMH system. Some attention has been paid to important issues outside the domain of public safety—for instance, the Good Lives Model (Barnao, Robertson, & Ward, 2010); however, little is known about the institutional objectives and outcomes that are valued by people in the FMH system. The current study attends to this knowledge gap by examining how people who use or provide FMH services understand the concept of “success.”
Method
The study used a qualitative descriptive design, which is an established qualitative methodological approach (Neergaard, Olesen, Andersen, & Sondergaard, 2009; Sandelowski, 2010). Although qualitative description can have overtones or elements of other research approaches, such as ethnography, grounded theory, or phenomenology, the core of this approach is to provide “straight descriptive summary of the informational contents of data organized in a way that best fits the data” (Sandelowski, 2000, pp. 338-339) by presenting an insider’s perspective (Milne & Oberle, 2005). Qualitative description highlights participants’ voices by describing their experiences using their own language (Neergaard et al., 2009). The aim is descriptive and interpretive validity, whereby theoretical and latent interpretations are minimized to accurately present events or experiences as those with lived experiences would perceive and make meaning of them (Sandelowski, 2000). Although not as interpretative or theoretical as other qualitative research methods, it is not atheoritcal as it is influenced by, and can contribute to, existing theory. Moreover, it is not purely descriptive because all qualitative research involves systematic analysis and thoughtful interpretation (Sandelowski, 2010).
Participants
Using a purposive sampling strategy, participants were recruited from forensic and general mental health services in Halifax, Nova Scotia, Canada. All participants had the ability to speak and understand English. To access a diversity of perspectives and experiences, both FMH service users and service providers were invited to participate in the study. The final sample consisted of 28 participants.
The FMH service user group was comprised of 18 adults who had received FMH services after being found “not criminally responsible on account of mental disorder” (NCRMD). The average age was 35 years, ranging from 27 to 52 years of age. Around three quarters were men (78%, n = 14) and were living in an FMH hospital (72%, n = 13), either on a conditional discharge or custody order, at the time of the interview; however, 13 (72%) had lived in the community at some point after receiving an NCRMD adjudication. The service users had been involved with the FMH system for an average of 4 years, ranging from 5 months to 11 years. Information about the participants’ psychiatric diagnoses and criminality was not gathered; however, other research in Canada indicates that one half of NCRMD findings are for minor assaults, property offences, and other nonviolent criminal acts; one half of not criminally responsible (NCR) persons have no prior contact with the criminal justice system; three quarters of NCR people are diagnosed with a psychotic spectrum disorder; and one third have co-morbid substance use disorders (Crocker et al., 2015).
The FMH service provider group was comprised of 10 adults who were providing hospital- or community-based services to NCR people. The average age was 46 years, ranging from 32 to 62 years of age. Half (n = 5) were women. On average, they had been providing services to FMH populations for 12 years, ranging from 4 to 20 years. They worked in hospital and community settings, and reflected a diverse range of professions including case coordinators, psychiatrists, psychologists, and various types of counsellors and therapists (e.g., recreation, spiritual, employment).
Materials and Procedure
The author administered individual, semi-structured interviews, consisting of open-ended questions that probed various dimensions of what success meant in the FMH context. A small set of interview questions was prepared. For instance, participants were asked to share their views regarding the main objectives of the FMH system (e.g., “what is the forensic system designed to do?”). They were also asked to describe FMH service users who they believed to be successful or unsuccessful (e.g., “think of someone who you consider to be the most successful person to have gone through the FMH system. Can you please describe them to me?”). Moreover, several vignettes depicting fictional stories of FMH service users were incorporated into selected interviews to stimulate discussion (see the appendix). Near the end of the interview, the vignettes were read aloud and the participants were invited to give their impressions about the fictional characters’ level of success. In addition to predetermined questions, the interviewer employed a flexible, conversational approach by following the interviewees’ narration and asking spontaneous questions in response. Interviews lasted for approximately 1 hr, and were audio recorded and transcribed by a research assistant. Throughout the interview process, the interviewer and transcriber wrote analytic memos to reflect on the data, identify emerging patterns, and develop preliminary codes. Participants received $20 in cash or donated to a local charity. Research ethics approvals were obtained from the Research Ethics Boards of Saint Mary’s University and the Capital District Health Authority. All participants provided written research consent.
Analysis
The data were analyzed using an inductive thematic analytic framework to identify predominant themes and recurring patterns (Saldaña, 2009). All analysis was performed by the author who uses an interpretivist/constructivist approach and has extensive experience with qualitative research in FMH settings. Throughout the analysis, the author maintained a reflective journal to document how decisions were being made in relation to coding. Qualitative software (NVivo 9) was used to efficiently store, organize, visualize, and reconfigure the data.
The coding process generally followed the six stages outlined by Braun and Clarke’s (2006) guide to performing thematic analysis. First, the list of preliminary codes produced during the interview process was entered into NVivo. Next, the author carefully read and reread the transcripts, and assigned passages of text (e.g., phrases, sentences, paragraphs) to existing, relevant codes. New codes were also created in NVivo to reflect and contain passages of text conveying new, meaningful ideas about the participants’ understandings of success that did not fit into existing codes. All codes were given operational definitions describing how they were to be applied during the coding process. Complete coding of all transcripts produced 60 codes. The next cycle of coding began with extracting and rereading the text associated with each code, and then reorganizing and reconfiguring the codes to develop a smaller set of themes. Codes were grouped based on conceptual similarities. Prevalence data, such as the numbers of participants and passages of text contributing to each code, also informed the process of transforming codes into themes. Through this process, the 60 codes were transformed into six overarching themes.
Below is a description of each theme, including a selection of narrative excerpts that have been edited (e.g., speech errors removed) to improve clarity. Each quote is identified with a pseudonym and the group (service user or provider) to which the participant belonged.
Results
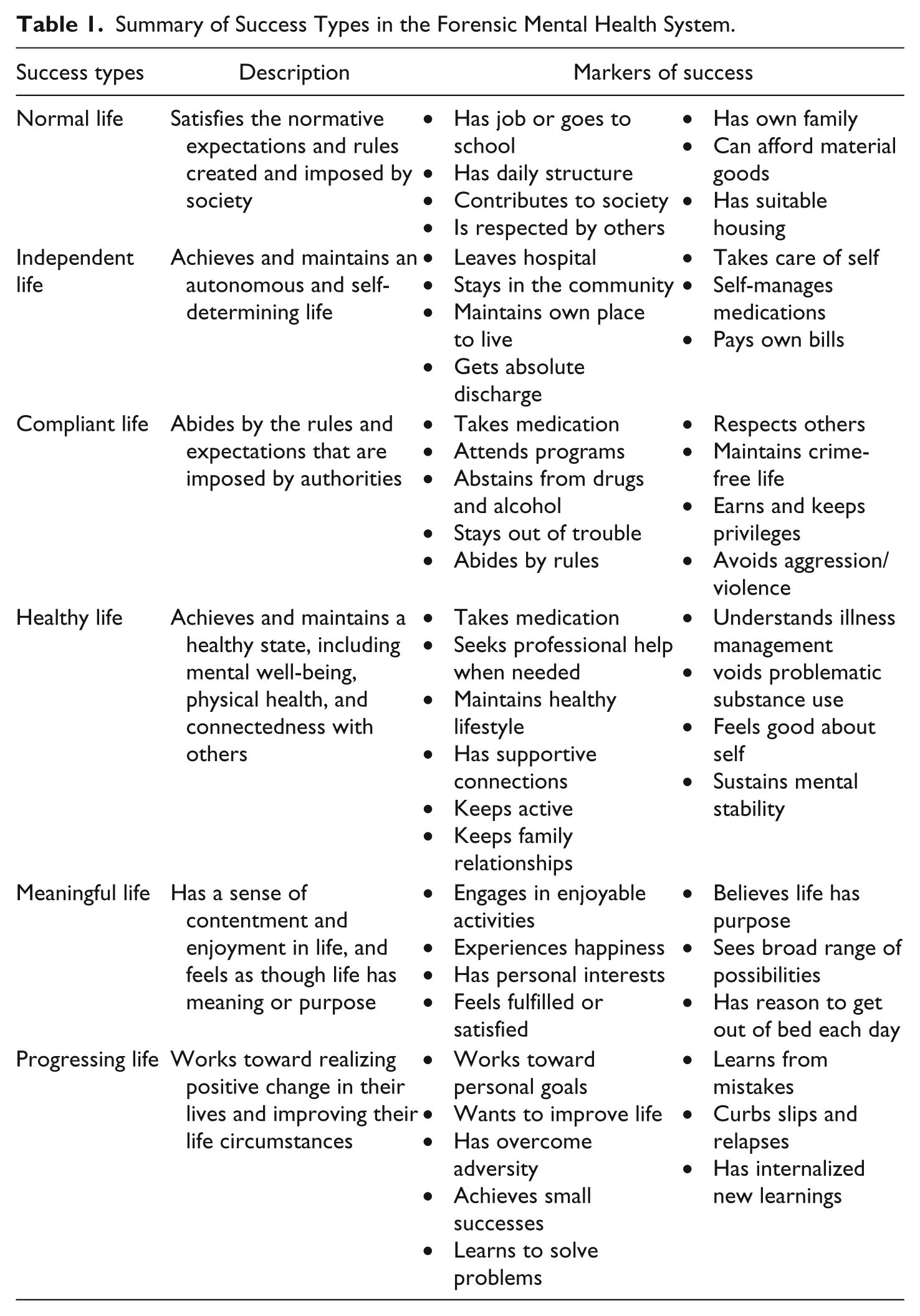
The participants spoke about the qualities that characterize success in the FMH system. Generally, success was seen as a dynamic process rather than an end state; that is, it describes something that a person works toward rather than an event or a characteristic. They also discussed the historical, social, and political factors, such as media coverage of sensational events and recent “tough on crime” reforms that shape the meaning of success in the FMH system. During the interviews, it became clear that multiple forms of success were operating in the FMH system. The participants rejected the idea that people were either successful or unsuccessful; rather, they indicated that most, if not all, FMH service users would achieve success, although it may manifest in unique ways: “What makes one person successful might not make the other person successful” (Julia, service user). The participants’ responses suggested that success in the FMH system materialized across six different domains: (a) a normal life, (b) an independent life, (c) a compliant life, (d) a healthy life, (e) a meaningful life, and (f) a progressing life (Table 1).
Summary of Success Types in the Forensic Mental Health System.
Normal Life
Having a “normal life” referred to a FMH service user’s ability to satisfy the normative expectations and rules placed on them by society: They [review board] want you to have a job, money, a car, a wife, a family, a house, a white picket fence, groceries in the fridge, RSPs [retirement savings] in the bank . . . that’s their version of success. (Oliver, service user)
The FMH system facilitated this by undertaking the societal role of “fixing and creating normal proper lives” (Beth, service provider). When describing what a “normal life” looks like, the participants used phrases such as average citizen, decent person, respectable person, structured life, and productive life. Being normal meant adhering to basic conduct rules: “like brushing your teeth, combing your hair, shaving, getting dressed, holding a conversation” (Evan, service user). Beyond this, it meant contributing to society, being productive, and having structure in one’s daily life: “being able to function normally and productively and efficiently in society” (Oliver, service user).
Participating in conventional activities, especially paid employment, was a key marker of achieving a “normal life”: “We have vocation and work as a staple in our overall definition of success” (Dan, service provider). When describing people who were perceived as being successful, the participants often referred to someone who was working: “I see him as a success because, first of all, he had a job” (Evan, service user). For the participants, getting a job indicated that the person was trying to be a productive, contributing member of society—an important criterion for having a “normal life.” It also provided structure to daily life and promoted feelings of self-worth. Moreover, work allowed people to purchase highly valued material goods, such as stylish clothing, nutritious food, suitable housing, and personal transportation: Success for a lot of people with mental illness . . . is . . . being able to work, buy your own groceries, pay [for] your medication, drive a car if you have enough money. Like, to fulfil a normal person’s work kind of schedule. (Logan, service user)
Beyond working, participants talked about school and other ways to create structure in daily life. They spoke about the value of education, with many service users expressing the desire to further their own schooling: “Successful thing to me would be getting back to school and try to get a degree” (Noah, service user). Education was tied to an instrumental aim of getting a good job and income. Moreover, going back to school helped them acquire greater knowledge and enhanced their social status. Other structured activities, such as volunteer work, were also mentioned as important ways for FMH service users to establish a “normal life.”
FMH service users felt burdened by having normative expectations placed on them as they were recovering with mental illness and coping with other problems: “There was a lot of sort of unspoken pressure to have some positive behaviours like exercising and looking for a job and that kind of thing” (Julia, service user). They spoke about the stress of being measured against previous times in their lives when they were capable of meeting normative standards: “Here I am trying to struggle to be this person that I was and I just can’t even get up” (Julia, service user). Others spoke about their lack of achievement relative to their peer group: “Why can’t I do what my peers are doing? They’re working forty hour weeks or they are at a school for a PhD program, and I’m just coming out of sleeping practically every day for eighteen hours” (Evan, service user).
Service providers discussed the fact that prevailing standards of a “normal life” in society were unachievable for some service users: “Many clients [would] love to have a wife and kids, or . . . to buy a home—things that may never be available to them . . . Society does use that as a benchmark for success” (Anna, service provider). They also talked about investing huge amounts of time, energy, and resources on imposing society’s norms onto FMH service users, with one participant referring to such a project as “pounding square pegs into rounds holes.” Another service provider spoke about this issue in detail: We have an idea of what a good life looks like and wanna fit our patients into it. So, everybody should be productive and structured, and some of that is risk management . . . But, aside from that, philosophically . . . I don’t know how much we should force people to be the way we envision things should be. (Beth, service provider)
Independent Life
A central function of the FMH system is to regulate and control people’s liberty and freedom. As such, an important type of success focused on reclaiming and maintaining an autonomous and self-determining life: “I think independence is a very high factor in being successful . . . You need to learn how to do your own things by your own self” (Olivia, service user). It was common for the participants’ stories about success to feature people who were living in the community with few constraints on their freedom. FMH service users often imagined their own success in terms of living independently: “I just see myself having my own apartment” (Ben, service user).
A key facet of an “independent life” was getting out of the forensic hospital. The aim of moving people out of hospital and, eventually, out of the FMH system was mentioned repeatedly as criterion for success: “We tend to take the attitude with everybody that they are going back out into the community . . . that’s what we want for them” (Beth, service provider). The dispositions of the Criminal Code Review Board (e.g., conditional or absolute discharges) were perceived as markers of success insofar as they supplied FMH service users with greater freedom. Although being released from hospital was an important and necessary first step toward an “independent life,” the participants recognized that more was required to be successful in this domain: “What happens after hospital is . . . where successes will begin to start again” (Evan, service user).
Staying out of hospital was described as an indicator of success in relation to achieving independence: “At the hospital, they’re successful if we never hear from them again” (Beth, service provider). The participants spoke about the revolving door and recycling rate of the FMH system as they reflected on people who were struggling to achieve an “independent life.” However, rehospitalisation was not, in-and-of-itself, framed as an absolute measure of a person’s level of success, because it could be the product of chronic, relapsing illnesses, and indicative of serious problems located within the service system: He’s unsuccessful not so much that he keeps winding back in the forensic system. That’s surely not the issue . . . He’s not successful because his illness has precluded him from having stability in the community and the quality of life that he otherwise could have if his illness had remained stable. (Zach, service provider)
At its core, staying out of hospital and, eventually, moving out of the FMH system were indicators that service users had established their autonomy and found a way to avoid “having their rights impinged upon [by] the psychiatric system” (Adam, service provider).
Getting their own place to live was another important element of achieving an “independent life” for the FMH service users: “I was talking to a friend of mine the other day . . . he was working and he had an apartment. That’s a success to me” (Dylan, service user). Connected with this was the freedom to choose where they would like to live: “In a way, he [NCR person] is successful: he’s living somewhere where he wants to be, is doing what he wants to do” (Jacob, service provider). Service providers recognized that an “independent life” may look differently for some service users: “The successful individual is as independent as he or she can be, given the circumstances of their illness and their environment. So for some that means full independence and for others it may not” (Jacob, service provider). Participants spoke about independence as the ability to do simple things that were not subjected to the surveillance or control of the FMH system: “Just being able to do whatever I want to do and if I wanted to sit up all night to watch TV, I could” (Emily, service user). An independent life also insisted that FMH service users become less dependent on the system by taking care of themselves, shopping for their own groceries, paying their own bills, getting to their appointments, and managing their own medications—even after restrictions on their freedoms are relaxed and support from the FMH system is reduced.
Compliant Life
This version of success concentrated on abiding by the rules and expectations imposed by authorities. Traditional outcomes, such as recidivism and rule compliance, are situated within this domain. Failure to achieve this type of success can result in severe consequences, such as the loss of liberty for FMH services users and the erosion of legitimacy for the FMH system. To achieve a “compliant life,” FMH service users must refrain from engaging in denounced behaviours. Desisting from crime and staying out of trouble with the law were key markers of success in this domain: “You have to be able to stay away from problems with the law” (Ben, service user). When asked to describe FMH service users who were successful, participants referred to people who were not involved in crime and violence: “They don’t come back for new offences or new changes or come back into our system as new NCR acquittees . . . they don’t wind back up in the forensic system” (Adam, service provider). Abstaining from drugs and alcohol was mentioned frequently by participants, because it is prohibited and connected with criminality: “I’m sure that the hospital would see a success story as not having reoffended or being off of drugs” (Ethan, service user).
The prospect of achieving a “compliant life” were diminished when service users engaged in unruly or unacceptable conduct, such as being disrespectful or inappropriate, incurring unauthorized absences, or acting aggressively. Many of these behaviours violated hospital rules as well as the requirement to “be of good behaviour” imposed by Criminal Code Review Boards. Adhering to conduct rules was particularly problematic for an “antisocial” subgroup of FMH service users: Some of the guys . . . apart from their illness, they have . . . largely antisocial traits. They’re unsuccessful in the sense that their illness isn’t the main driver that gets them into difficulties with the law . . . Once they’re in our system, they’re hard to get out . . . because their behaviour continues to be problematic. (Adam, service provider)
A “compliant life” was exhibited when service users obeyed the rules, earned and kept privileges, attended prescribed programs, adhered to a medication regime, and stayed out of trouble—a formula for success that was summarized by one participant: Stay clean . . . be where you’re supposed to be at the right times . . . just do your programs, and get along with other patients and . . . staff members . . . that’s pretty well success. (Gabe, service user)
At times, the FMH service users’ descriptions of a “compliant life” sounded as though they were retelling someone else’s formula of success. The narratives in this domain suggested that achieving a “compliant life” sometimes requires performing a role; that is, service users must learn what others expect and demonstrate that they can enact this role. This was described as “working the system”: “you have to learn to do what they say and learn to meet their expectations, even if none of them are your own” (Oliver, service user). For service providers, this presented a real challenge: “We do so much programming with the patients . . . it’s often hard to know whether claimed insight is true or not” (Adam, service provider). One participant compared this form of success with an illiterate student graduating from university: So, in the same way the school system does . . . people just get through our system . . . they’ll graduate from the forensic system . . . get an absolute discharge, but they don’t get it. (Zach, service provider)
Reflecting on this notion, the participants described how meaningful and enduring change was not required if service users are only expected to follow the rules and perform a particular role, as was implied by the following remark: “You can bake a cake; it can look good. Once you actually eat it, that’s when we know” (Liam, service user).
Healthy Life
Living a healthy life was an important way that FMH service users could be successful. Although this theme intersects with a “normal life,” it does not share the intense emphasis on material success goals. Instead, it focused on making an effort to achieve and maintain a healthy state, including mental well-being, physical health, and connectedness with others. Conversely, it involved avoiding behaviours and activities that were likely to jeopardize one’s wellness and safety. In this domain, individuals made choices and engaged in behaviours, not because they were told to do so, but rather, because they wanted to establish and preserve a healthy way of living: “As long as you have your good health, I guess, that’s successful right there” (Jacob, service user). The participants described a “healthy life” in a holistic sense, consisting of having awareness of one’s illness and how to manage it, taking medications to manage symptoms of mental illness, keeping physically healthy, avoiding problematic substance use, maintaining supportive connections, being engaged in activities, and seeking professional help when needed: “Try to keep a healthy state . . . . Stay on your meds, eat properly, sleep properly, try to go to the gym, try to keep good fitness. I think that measures . . . success” (Noah, service user).
The participants spoke about the importance for FMH service users to accept that they live with a mental illness that needs to be taken care of: “I think . . . success is admitting that I have an illness and basically treat it” (Oliver, service user). As such, an important function of the FMH system was to improve service users’ understanding of mental illness and how to manage it: Ideally you would try to help develop the person’s insight into their illness. You would help them understand what impact their illness has, not only on their health, but on their relationships. (Adam, service provider)
Without this awareness, FMH service users risked becoming unwell, which had a spiralling effect on other domains of success: “They [FMH service providers] just wanna see people sober and stable . . . Some people, when they get sick, they get aggressive” (Dylan, service user). Participants stories of success often referred to people who were managing their symptoms: “That’s the basic level of a success story is that their delusions are under control” (Ethan, service user). Taking medication was an important mechanism for controlling symptoms: “Medication doesn’t solve everything, but it solves a lot . . . it’s a piece of the puzzle” (Ethan, service user). And, it was a key ingredient of a healthy life: “To be successful you have to take your medication on a regular basis” (Olivia, service user).
Another aspect of a “healthy life” was establishing and maintaining supportive connections. Achieving success in this domain required the existence of a system of supports and services capable of meeting the needs of FMH service users. For participants, service users who sought professional support when needed demonstrated that they were taking an active role in managing their mental health problems. The importance of having social connections and feeling supported in their community was also underscored by the participants: “I think to be successful . . . you have to have friends and family, and not just people on the internet” (Emily, service user). Living a “healthy life” also meant staying away from unhealthy peer groups: “I think that if I hang around people that don’t do drugs, I’d be more successful” (Dylan, service user).
The topic most frequently spoken about in relation to success in the FMH system was substance use. Success can hinge on a person’s ability to manage his or her substance use problems, because it can compromise his or her mental stability: I can be successful if I . . . refrain from drugs and alcohol and just maintain on medications . . . My whole downfall is the drugs and alcohol cause it . . . affects my sleep patterns and I get delusional. (Lucas, service user)
The participants identified drugs and alcohol use as a contributing factor to offending behaviour: The successful individual is the person that, to the best of their abilities, manages their risk . . . For a person to be successful, they have to deal not only with their illness, they have to deal with those other characteristics that might put them at risk of getting back into difficulties. Substance use is probably . . . the biggest issue for us. (Adam, service provider)
Participants indicated that abstinence from using drugs and alcohol was required for FMH service users to be successful “If you’re with mental illness and you’re smoking marijuana or you’re drinking alcohol and you’re not taking your medication, then you’re putting yourself in jeopardy to lose everything you have and that can make you very unsuccessful” (Noah, service user). Others indicated that using drugs and alcohol was fine for some, as long as it did not place the person in unhealthy or risky situations: “I’m sure there’s lots of successful people who smoke a joint once in a while” (Jen, service provider).
Using drugs or alcohol did not exclude someone from success because “relapse is part of recovery” (Gabe, service user). The participants maintained that a relapse did not negate progress that service users had made in trying to achieve a healthier life: “I don’t think we can say . . . they’re [FMH service users] succeeded or not succeeded based on some relapse” (Alice, service provider). However, the severe consequences associated with drug and alcohol relapses can make people feel like failures: “Every time I feel like I’m succeeding, I use substances. And that brings me back here [FMH hospital]” (Tom, service user).
Meaningful Life
In this domain, success referred to gaining a sense of contentment and enjoyment in life and feeling as though life had meaning and purpose. Although these topics were sometimes discussed in the context of spirituality and religion, meaningfulness was more often spoken about in secular, goal-oriented terms. The importance for service users to see life as meaningful and purposeful was described: “A lot of times, not reoffending is really kinda linked with having a purpose in your life or being able to fill your life with goals” (Ethan, service user). Wrapped up in this was the need to feel loved and wanted by others: “I think everybody wants to feel loved and to be healthy” (Jen, service provider). Another participant framed this as, “A feeling of being wanted somewhere, a feeling that somebody being happy when they see you, all those types of things which are hard to quantify” (Dan, service provider).
Much the narrative in this domain centred on happiness: “Being a success story, it got to do a lot of happiness” (Lucas, service user). Happiness, or having happy moments, was mentioned as a marker of success: “Being well on medication, eating good food, getting your education, having a happy life—and happy moments, anyways. . . . They [FMH service users] have to have something that makes them happy” (Logan, service user). Another participant shared this sentiment: “I don’t think it’s rocket science . . . Folk who living with chronic mental illness—forensic patients—they just wanna be happy . . . It’s not that complex in a certain way” (Zach, service provider). Happiness was viewed as an elusive state associated with success: “I don’t think you need to be happy for success; I just think success comes with happiness” (Olivia, service user).
Participants noted that happiness could serve a protective function, such as preventing someone from relapsing into problematic substance use; however, FMH service providers contested the use of happiness and life satisfaction as a criteria for success if they were achieved through unacceptable means (e.g., drug use, mania), brought about through an inadequate lifestyle (e.g., staying in bed all day), or placed a person at risk for adverse outcomes: “Sometimes people will be satisfied with things that are unhealthy and unsafe” (Beth, service provider). Similarly, it was suggested that FMH service users may be content with their present life circumstances because they have a restricted view of what is possible or have settled into a low social position: Folks’ . . . understanding of what’s possible seems to be rather limited . . . You know, it’s actually not a given that you have to live in that neighbourhood, there’s actually other possibilities . . . you could live somewhere else that there wasn’t drug deals going on in the apartment elevator . . . So, it’s really [about] enlarging their view. (Vicki, service provider)
Another indicator for establishing a meaningful life was that FMH service users had personal interests (e.g., hobbies) and engaged in enjoyable activities. This was described in various ways, including “having a passion for something” (Jen, service provider), being “engaged in things that are important” (Vicki, service provider), finding “ways to enjoy myself without getting high” (Dan, service provider), and having a reason to “get me up in the morning” (Ethan, service user). One FMH service user who was in the early stages of community resettlement spoke about the pleasure of partaking in simple, yet gratifying, activities: I feel successful because I get up every morning and I can have a coffee, I can smoke a cigarette, and I can eat breakfast, and then I can see people, and I smile . . . That right now is a success because for the past year that wasn’t happening and I’m really happy about that. (Evan, service user)
Progressing Life
In addition to conceptualizing success in terms of outcomes (e.g., health, independence), the participants also framed it as the process of working toward positive change: “No matter where you are in life . . . change needs to be part of . . . success” (Anna, service provider). In this domain, success was operationalized as establishing personal goals and making an effort to achieve them. Conversely, lack of success involved stagnating or backsliding: “The big thing I would say about not succeeding is just consistently stepping backwards and not forward” (Jen, service provider). Moreover, someone who lacked the desire to improve his or her life circumstances may be considered unsuccessful in this domain: “I think some [FMH service users] just don’t care . . . they don’t care if they’re here [FMH hospital] or where they’re at . . . That’s why they’re not a success story, because they don’t care” (Lucas, service user). Progress can be evidenced by someone who engaged in harmful or prohibited behaviour, but then learned from his or her mistakes: “In order to be successful you have to learn how to be successful . . . Learn from my mistakes and learn from other people’s mistakes too” (Nathan, service user). Participants also spoke about learning knowledge and skills from programs and services designed to encourage personal growth and progress.
When speaking about making positive changes, FMH service users referred to moving forward in small, measured steps. For them, it was important to remain aware of small achievements as they work toward re-establishing their lives: “I celebrate the small stuff . . . ’Cause, if you just wait for one big moment, it’s just a moment and then it’s gone. So, it makes me happy to celebrate a little bit as things progress” (Olivia, service user). Given that most FMH service users faced numerous constraints related to severe mental illnesses as well as serious social marginalization, the early stages of recovery required deliberate attention to basic aspects of life: “Recovery itself . . . takes time to learn to do simple things . . . just like eating and getting dressed” (Evan, service user). Attending to and acknowledging small improvements were echoed by another participant who struggled with depression and medication side-effects: Some days, success is just not to think about some of the negative stuff . . . So, the little thing like being in a good mood wouldn’t even be on the radar for most people; that’s where I’m at. (Julia, service user)
Progress was perceived as being essential for maintaining hope and optimism about the future: “Seeing the progress and being able to move forward—keeps that hope going” (Olivia, service user).
The participants’ stories of success often referred to people who had experienced and overcame tremendous adversity in their lives: I am a success story because I’ve just come so far. Even the staff here . . . can’t believe the difference in me. I remember I first came here [FMH hospital] I was really sick. I was very aggressive . . . I’m not the same person I was ten years ago. (Emily, service user) I look back at all of that segregation, solitary confinement . . . One time I did try to take my own life . . . I overcame that and was successful. Enduring all that is a form of success I believe. (Oliver, service user)
From this perspective, success was gauged by a person’s ability to live through and learn from difficult life experiences—an interpretation of success that was endorsed by service providers: Is he [FMH service user] the person who’s going to be on the front page of the paper advertising forensics? Probably not. But, definitely someone I would say is a success when you look back at what a rough life he’s had. (Anna, service provider)
Behaviours, such as substance use or other rule violations, that might disqualify someone from being considered successful in other domains, would be interpreted differently in this domain if they improved in severity, frequency, or duration.
Discussion
Research indicates that as many as 80% to 90% of FMH service users in Canada do not reoffend within 2 to 3 years after being released from hospital to the community (Charette et al., 2015; Livingston, Wilson, Tien, & Bond, 2003). Research outside of Canada confirms the rarity of reoffending among this population (Hayes, Kemp, Large, & Nielssen, 2014). Although such findings are an important part of the story of success, they provide little insight into how people safely return to, and resettle in, the community after involuntary detention. Moreover, studies in this area continue to focus heavily on people’s deficits and failures, with success being operationalized as the absence of an adverse event or outcome (e.g., not reoffending, not returning to hospital), rather than the process of working toward a positive accomplishment.
The results of the current study offer a multidimensional and holistic way of viewing success that is grounded in the lived experiences of people who provide or use FMH services. It would be naïve to suggest that reducing recidivism is an insignificant aim of the FMH system; however, these findings point to the inadequacy of using a single outcome indicator to evaluate success, because people in the FMH system prioritize a broader range of objectives. Other scholars also point toward the need to incorporate a more balanced assortment of outcomes in evaluations of forensic and correctional systems (Cohen & Eastman, 2000; Lee & Stohr, 2012). The participants do draw linkages between risk management, recidivism reduction, and success, but they also frame the various forms of success in ways that are not dependent on public safety objectives. In other words, the participants recognize the potential for these types of success (e.g., health, meaningfulness, normality) to enhance public safety, but their value transcends their risk management function. Such views may, in part, be a product of the rehabilitative orientation and multi-disciplinary nature of FMH services in Canada, as well as the recent infiltration of recovery approaches into FMH systems (Drennan & Alred, 2012; Livingston et al., 2013).
In many ways, the participants’ conceptualization of success is similar to the manner in which other concepts have been defined in the literature. For instance, like the current study, research on the meaning of recovery among substance users highlights their desire to have a “normal life” or to become a “normal person” (Best, Gow, Taylor, Knox, & White, 2011). Participants in the present study also posit that success waxes and wanes throughout a person’s involvement in the FMH system and the remainder of their life—a finding that echoes how constructs such as “resilience” (Werner & Brendtro, 2012, p. 20), “recovery” (Davidson et al., 2005; White & Kurtz, 2005), and “desistance” (Maruna & LeBel, 2010) are viewed as dynamic, complex processes rather than static traits or end states. The chronic, relapsing nature of mental illnesses and substance use disorders combined with under-resourced, fragmented community services makes it probable that FMH service users will experience negative life events, such as rehospitalisation or relapse to substance use. Consistent with understandings of recovery in the substance use field (Best et al., 2011), the current study suggests that it would be a mistake to label someone as “unsuccessful” on the basis of such adverse experiences, which challenges conventional ways of evaluating outcomes in the FMH system.
As a group, the participants share a vision of success that is distributed across the six domains. If the views of FMH service users and providers are the main drivers of the FMH system, then this calls for bringing clinical practices, therapeutic programs, models of care, and outcome evaluations into line with the framework presented in this study. However, as with any social institution (Garland, 1993), there are much stronger social and political forces that influence the shape of the FMH system—some of which were discussed by the participants (e.g., “tough on crime” political agendas). Importantly, the FMH system maintains its legitimacy primarily by pacifying public fear concerning people with mental illnesses. As a result, an inordinate amount of attention and resources in the FMH system are directed toward the public safety domain, despite this being incongruent with the beliefs of people who provide and use its services. Criminologists can avoid reproducing and perpetuating the dominance of a state-centric, crime control paradigm in the FMH system by moving beyond recidivistic-oriented objects of inquiry and by asking questions that “expand the criminological horizon beyond the crime problem” (Michalowski, 2016). Accordingly, criminological attention should be paid to the multiple forms of success that are valued by people within the FMH system and that allow FMH service users to be defined by qualities other than their criminal acts. Such a paradigm shift aligns with the holistic, strengths-based, individualized, and relational approaches promoted by several emerging theoretical perspectives (e.g., desistance, recovery, positive criminology).
The study has methodological limitations to keep in mind when considering the results. The sample represents the views of FMH service providers and service users, from one Canadian province, who self-selected to participate in the study. It is possible that unique features of the sample or local context may affect the applicability of these findings to other contexts or settings. For instance, most of the FMH service providers interviewed for this study endorsed a recovery approach to mental health care, which promotes a particular way of viewing illness, health, and treatment. The results may not be transferable to contexts where the mental health recovery model is not widely accepted. Another limitation is that the data collection and qualitative analysis were conducted by a single person, which may affect the study’s credibility and dependability. Several methods were used to maximize the credibility and transparency of the analytic process, including maintaining a reflective journal with copious analytic memos about the coding process, and creating a qualitative codebook with code lists and definitions.
Despite these limitations, the current study offers a compelling way of conceptualizing success in the FMH system that exposes novel directions for research and theory. We know very little about the people who have achieved success following an involuntary hospitalisation in an FMH hospital. There would be benefits from systematically studying FMH service users who are living “successfully,” as defined by the current study. Another valuable line of future research would be to ascertain the level of public and political support for expanding the objectives of the FMH system beyond the public safety domain—especially because many FMH systems are positioning their services with recovery-oriented philosophies of care (McKenna, Furness, Dhital, Park, & Connally, 2014). A related and important extension of this study would be to examine how the current findings compare with conceptualizations of success by other groups, including those who have been victimized by persons found NCRMD. Theoretically, a multidimensional definition of success opens the door to extending and applying existing approaches, such as positive criminology or desistance theories, to enhance the understanding of non-recidivistic institutional objectives, and the mechanisms influencing their realization, in the FMH context.
Footnotes
Appendix
Acknowledgements
The author would like to express appreciation for the contributions of Dr. Andrew Starzomski, Mr. Igor Pekelny, and the study participants who shared their personal stories.
Author’s Note
A version of this article was presented on June 4, 2015, at the 3rd North American Correctional and Criminal Justice Psychology Conference in Ottawa, Ontario.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided by grant awarded by Saint Mary’s University.