
Abstract
The aim of this article is to examine the effects of a short-term one-to-one anger management program delivered to community-based offenders in Malta. The program delivered was the Individual Managing Anger Program (I-MAP), a Cognitive behavioural therapy (CBT) and mindfulness-based anger management intervention developed as an EU project. A randomized control trial (RCT)with waitlist controls was carried out to investigate the effects of I-MAP on the reduction in anger dysfunction among offenders serving a community-based sanction. Participants were 24 male offenders aged between 18 and 57. Eligibility for treatment was based on screening for anger dysfunction and success of interventions was determined through psychometric measures. All the statistical analyses carried out showed significant reduction in psychometric scores on anger symptoms. Results of the interventions show clinical significance. These results are discussed in light of recent research.
Background
The aim of the study was to establish the treatment outcome of a structured one-to-one anger intervention program: the Individual Managing Anger Program (I-MAP), developed in partnership by the Romanian Ministry of Justice, the Irish Probation Service, and the Italian Ministry of Justice. The I-MAP was developed under Framework 2008/947/JHA of the European Union and financed by the European Commission’s 2010 “ Criminal Justice” program. The scope of this program is to reduce the dysfunctional anger in community-based offenders. The I-MAP has not been validated to date. Furthermore, there have been no other studies exploring the effectiveness of psychological interventions on Maltese offenders or possible cultural differences in anger expression.
Anger Management and Offender Populations
Anger as an emotion can be classed as having a cognitive, affective, and physiological component. Cognitively anger may elicit many mental schemas that might involve harm to self or to others, thoughts aimed at diminishing one’s responsibility, attributing blame onto others, and other similar thoughts. Affectively anger may elicit a range of feelings ranging from mild frustration to more intense feelings of rage. Finally, it may trigger physiological arousal in the person’s body, a state of readiness for action (Deffenbacher & McKay, 2000). High levels of anger in the person might elicit more negative schemas and cognitions increasing the chance of resorting to dysfunctional forms of expression and behavior such as aggression (Berkowitz, 2011; Deffenbacher, 2011). Fernandez and Wasan (2010) define anger as a cognitive motivational process, specifying that the person experiencing anger may perceive themselves as being wronged or slighted. Inherent with this appraisal is the motivation to redress that perceived offence. Aggression, in this instance, might be viewed as one of the behavioral means to correcting the perceived wrong (Fernandez, 2010; Fernandez & Wasan, 2010).
A study carried out by Gilbert, Daffern, Talevski, and Ogloff (2013) concluded that offenders with high trait anger were prone to activate aggressive behavioral scripts which stay activated for longer periods. Furthermore, they suggest that intensity, frequency, and the duration of the anger problem were more salient than normative beliefs about violence and aggressive script rehearsal in determining future violence. Thus, by addressing anger dysfunction one could prevent future acts of violence. Furthermore, offenders convicted for non-violent crimes may also have dysfunctional levels of anger, as they could use other means to redress the perceived wrongdoing. Also, lack of emotional regulation, self-management, and negative appraisals can put them at risk of harming themselves or others whether incarcerated or in the community. This might make anger management a valid intervention among correctional populations as it might inhibit the use of aggression or facilitate offender management.
However, not all anger manifests itself in aggression. Some anger might be seen as invigorating the person to take action, seek expression, or positive coping by trying to address the problem or the source of the frustration. Generally, the frequency, intensity, duration, and mode of expression distinguish pathological from functional forms of anger expression (Novaco, 2011b). On the other hand, aggressive or violent acts are not always a result of or preceded by dysfunctional anger. Although aggressive or violent acts may be considered action schemas/scripts associated with anger, they may be motivated by various factors such as financial gain in robbery (Fernandez, 2010). In fact, some studies have reported that some violent offenders had no pathological or problematic levels of anger despite being incarcerated for violence and aggression (Heseltine, Howells, & Day, 2010; Howells, 2004; Watt & Howells, 1999). Therefore, proper assessment and formulation to determine the role of anger in the offending behavior and the person’s overall functioning is essential to ensure that appropriate interventions are delivered to respective clients (Howells, 2004; Novaco, 2011a, 2011b; Walker & Bright, 2009). It is recommended that anger management should only be considered if there are clear triggers for anger; a pattern of dysfunctional cognitive appraisal systems; an element of physiological arousal; an intense feeling of anger; impulsive actions and behavioral reactions related to the angry feeling (Howells, 2004).
Anger management typically consists of cognitive behavioral techniques. The cognitive component in anger management aims at replacing the dysfunctional cognitions, inferences, and evaluations with anger inhibiting ones such as seeking alternative reality-based explanations for the antecedent events (Trower, Casey, & Dryden, 2008). Novaco (2011a), argues that arousal reduction techniques are important in anger management as arousal is a central component of anger. Furthermore, it might limit the potential for aggression as it is argued that it is not possible to experience the state of anger and relaxation concurrently. Mindfulness techniques such as visualization and breathing exercises are useful arousal reduction strategies adopted in some anger management programs. Anger management also has a behavioral component where clients are usually taught behaviors that are functionally equivalent to their dysfunctional behavior. Rehearsal is needed to ensure the client feels confident enough with the new skill to use it in real life situations and increase self-efficacy (Deffenbacher, 2011). Examples of behavioral interventions can vary. However, assertiveness skills training is a typical example of skills exercises in anger management interventions. All of these components can be found in the I-MAP (Johnson & Gast, 2013).
Aims
The aim of this study was to explore the effects of a brief one-to-one anger management program on male community-based offenders. The research question is whether I-MAP, a Cognitive behavioural therapy (CBT)-based anger management with mindfulness techniques, can reduce anger. Due to the limited time available for the study, effectiveness of the intervention was only assessed through changes in self-reported anger scores. It was hypothesized that significant post-treatment differences would be noted following the delivery of treatment for both groups in the study.
Methods
The CONSORT statement was used as a checklist to ensure that the study information was reported adequately (Schulz, Altman, & Moher, 2010).
The Intervention
The I-MAP aims to target community-based offenders aged 16 years or above. It consists of nine sessions lasting approximately 90 min each. Although manualized and structured, the sessions allow flexibility to focus on the idiosyncratic variants and needs of the client’s problematic anger. This focus on individual needs is considered one of the hallmarks of good quality interventions (Walker & Bright, 2009). The one-to-one format might mitigate for the brevity of interventions.
The I-MAP aims to address anger through cognitive behavioral techniques and mindfulness strategies. The cognitive behavioral components included
understanding of anger;
identifying triggers, thoughts, emotions, and behaviors associated with anger;
developing positive communication strategies and positive relationships;
understanding thinking styles and thinking errors;
recognizing and disputing unhelpful thoughts; and
developing inhibitions to anger and strategies to increase anger control (Johnson & Gast, 2013).
During each session, skills were practiced and tasks were completed in situ or given to the participant as homework. A typical example of these exercises was a journal which would consist of an analysis of the angry experience and an opportunity to challenge unhelpful anger-inducing thoughts and inferences (Trower et al., 2008). The mindfulness-based techniques in the I-MAP consisted of relaxation and visualization exercises such as the Body Scan technique. These tasks were meant to facilitate an understanding of anger and how it might affect one’s cognitions, behavior, and emotions. It also sought to enable participants to increase tolerance of anger which might in turn alleviate the negative reactions to anger (Johnson & Gast, 2013).
To ensure program integrity, the I-MAP sessions were delivered by two qualified psychologists and 92% of the sessions were carried out by the first author (K.S.H.). These psychologists had received priori training in the use of the program from one of the program developers. All the sessions were delivered in a one-to-one format which allowed the facilitator to adapt the manual to cater for the idiosyncratic aspects of the participants’ problematic anger.
Measures
Treatment progress was indicated by changes in anger symptoms. This was measured through the Anger Disorder Scales (ADS) (Di Giuseppe & Tafrate, 2004). Due to the short study timeframe, self-reported psychometric measures were used.
The ADS is a multidimensional scale which distinguishes between varying levels of pathological anger (mild, moderate, or severe). It consists of 18 different subscales across five domains of anger: the Provocations domain (Scope of Anger Provocations and Hurt/Social Rejection); the Arousal domain (Physiological Arousal, Duration of Anger Problems, and Episode Length); the Motives domain (Revenge, Tension Reduction, and Coercion); the Cognitions domain (Suspiciousness, Resentment, Rumination, and Impulsivity); and the Behavioral domain (Brooding, Verbal Expression, Physical Aggression, Relational Aggression, Passive Aggression, and Indirect Aggression). These subscales are loaded on three higher order scales: Anger In, Vengeance, and Reactivity/Expression.
In the ADS, T-scores above 65 are indicative of a clinical problem with the anger symptom in terms of duration, frequency, and severity. T-scores were based on the overall normative sample in the ADS Manual (Di Giuseppe & Tafrate, 2004) rather than the age-specific norms (18-29, 30-49, 50+) to facilitate the comparison to the current sample which was comprised of different age groups together (age range of sample 18-57).
The higher order scale of Reactivity attempts to measure the outward expressions of anger. Individuals within the clinical range of the scale tend to exhibit periods of rumination which could further disinhibit the respondent to more acts of aggression and also affect relationships with others. Respondents scoring within the clinical range for the Anger In scale might be particularly sensitive to perceived threats to self-esteem or rejection. This might make them suspicious of others around them. They might also have high levels of resentment. Such individuals also tend to stay angry for prolonged periods of time. Respondents who score high on the Vengeance scale are typically characterized by a sense of revenge or retribution especially once they perceive an attack or slight. Di Giuseppe and Tafrate (2004) maintain that these respondents are primed by a sense of injustice and seek to get even with those they perceive to have transgressed against them. To achieve these aims, individuals with high Vengeance would attempt retribution through either direct use of aggression or less confrontational means such as damaging property, or resisting any instructions or obligations (Di Giuseppe & Tafrate, 2004). The reported stratified alpha as a measure of internal consistency for the ADS total was .97, for the Anger In .93, Reactivity .96, and Vengeance .94. The ADS correlates positively, r(450) = .78, p < .001, with other measures of anger such as Spielberger’s (1999) State-Trait Anger Expression Inventory - 2 (STAXI-II) and the test-retest reliability for the ADS total score was r = .89, p < .001 (Di Giuseppe & Tafrate, 2004).
Participant Recruitment and Allocation
This study was carried out at the Department of Probation and Parole (DPP) in Malta. The department primarily provides supervision of community-based offenders by probation and parole officers. As part of offender case management, probation officers might request the offender to address particular criminogenic needs to reduce the potential risk of recidivism and increase public safety.
Before launching the study, probation officers attended training related to anger dyscontrol and the use of the Screening Candidates Checklist (Van Dieten, Winogron, & Grisim, 2001), which they would be required to complete with the referral and would help them identify potential anger dysfunction in clients. Consent for participation in the randomized control trial (RCT) was included in the referral. The consent form specified the overall aims of the research and the intervention. Prospective participants were informed that all data collected would be handled anonymously and their participation was on a voluntary basis.
Participants for the program were recruited from among offenders on probation or parole in Malta. All offenders referred for treatment were screened for anger or attitudes supportive of violence. These participants were referred by their probation/parole officer following the administration of an adapted form based on the Screening Candidates Checklist (Van Dieten et al., 2001). Following the referral, candidates were assessed by the psychologists using the baseline measures to determine whether the candidate fulfilled the entry criteria for the program. Candidates who did not score pathological or clinical levels of anger were not entered into the study and were directed to more apposite interventions. Thus, participants were selected on the basis of anger dysfunction rather than their offence history.
All the participants received the intervention. However, one group (Group B) was waitlisted and received the intervention 3 months after the target group (Group A) completed their intervention. Participants were randomly assigned to their groups. Group allocation was carried out by generating a list of random numbers through a coin toss method. Referrals were then assigned to the group according to their respective number. Figure 1, based on the CONSORT statement (Schulz et al., 2010), outlines the phases of the study. Group A started the intervention first, after the baseline assessment (Testing Period 1 or TP 1), and were reassessed with the outcome measures upon completion of treatment (Testing Period 2 or TP 2) as well as after a 3 month period (Testing Period 3 or TP 3). Group B was also assessed at the baseline (TP 1) and then placed on a waitlist for 3 months during which they received standard probation supervision. Following this they were reassessed before starting the intervention (TP 2). This waitlist period was meant to control for the potential confounding effects of supervision. The outcome measures were readministered once the intervention period was completed (TP 3).
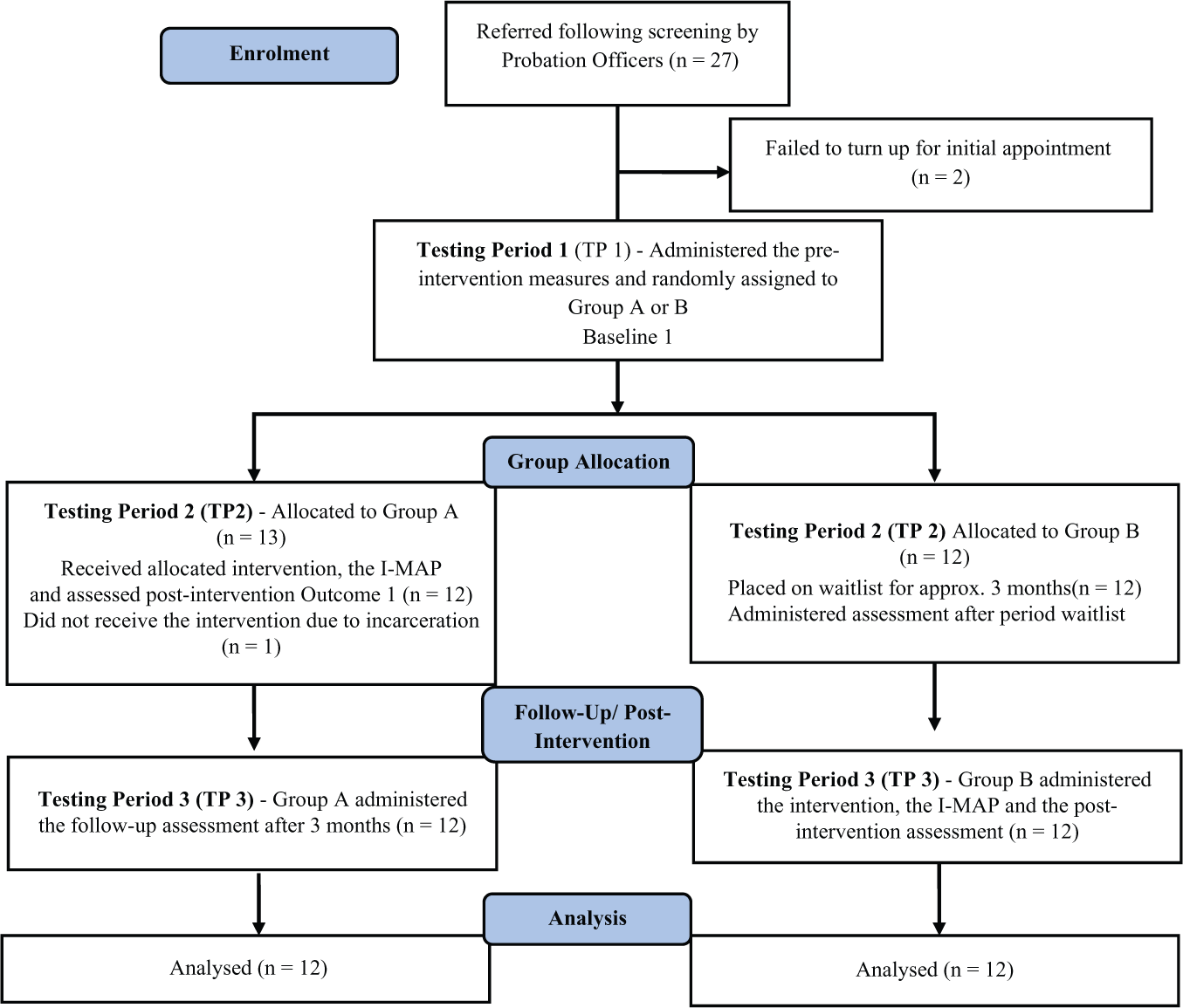
Study flow diagram for the randomized control trial (RCT) exploring the effectiveness of brief anger management.
A number of statistical analyses were carried out to assess differences on the anger measures at the different time periods between Group A and Group B. Differences before and after the intervention periods scores were also calculated for the total sample (N = 24) to assess for any reductions of symptoms of anger through the intervention.
Participants
Twenty-seven offenders were referred for the anger management program between March 2014 and December 2014. Two offenders did not attend the initial session or complete the baseline assessments. The other participant was administered the baseline assessments but was incarcerated following a breach of his conditions. Their data were not included in the analysis. Following the referral a number of variables pertaining to the participants’ criminal history and psycho-social factors were extracted and coded as either present or absent from the information in the participants’ case file. Demographic and psycho-social variables included age, employment status, literacy and educational level, history of substance abuse, previous contact with mental health professionals, and stability of relationships. Criminal history variables included the level of risk, incarceration history, pending cases, attitudes supportive of violence, and history of previous convictions. The level of risk was established using the Level of Service Inventory–Revised (LSI-R; Andrews & Bonta, 1995). This assessment is usually carried out by the probation officers under the supervision of psychologists. This assessment can also help identify criminogenic needs thus could have helped probation officers ascertain whether the client’s anger was in need for interventions (Andrews & Bonta, 1995). The participants were also administered the Anger Readiness to Change Questionnaire (ARC-Q) to assess whether they were either in the Pre-Contemplation, Contemplation, or Action Stage (Williamson, Day, Bubner, & Jauncey, 2003). Previous research identified readiness to change as a salient factor influencing treatment effect (Howells, 2004). Thus, to control for potential differences between the two groups on this variable, participants were also administered the ARC-Q (Williamson et al., 2003).
The ADS provides a Positive Impression Index (PII) which aims to identify those respondents who attempt to fake good the test and minimize their anger problems. Scores under 15 on this scale may indicate socially desirable responding (Di Giuseppe & Tafrate, 2001). This could confound any treatment effect identified.
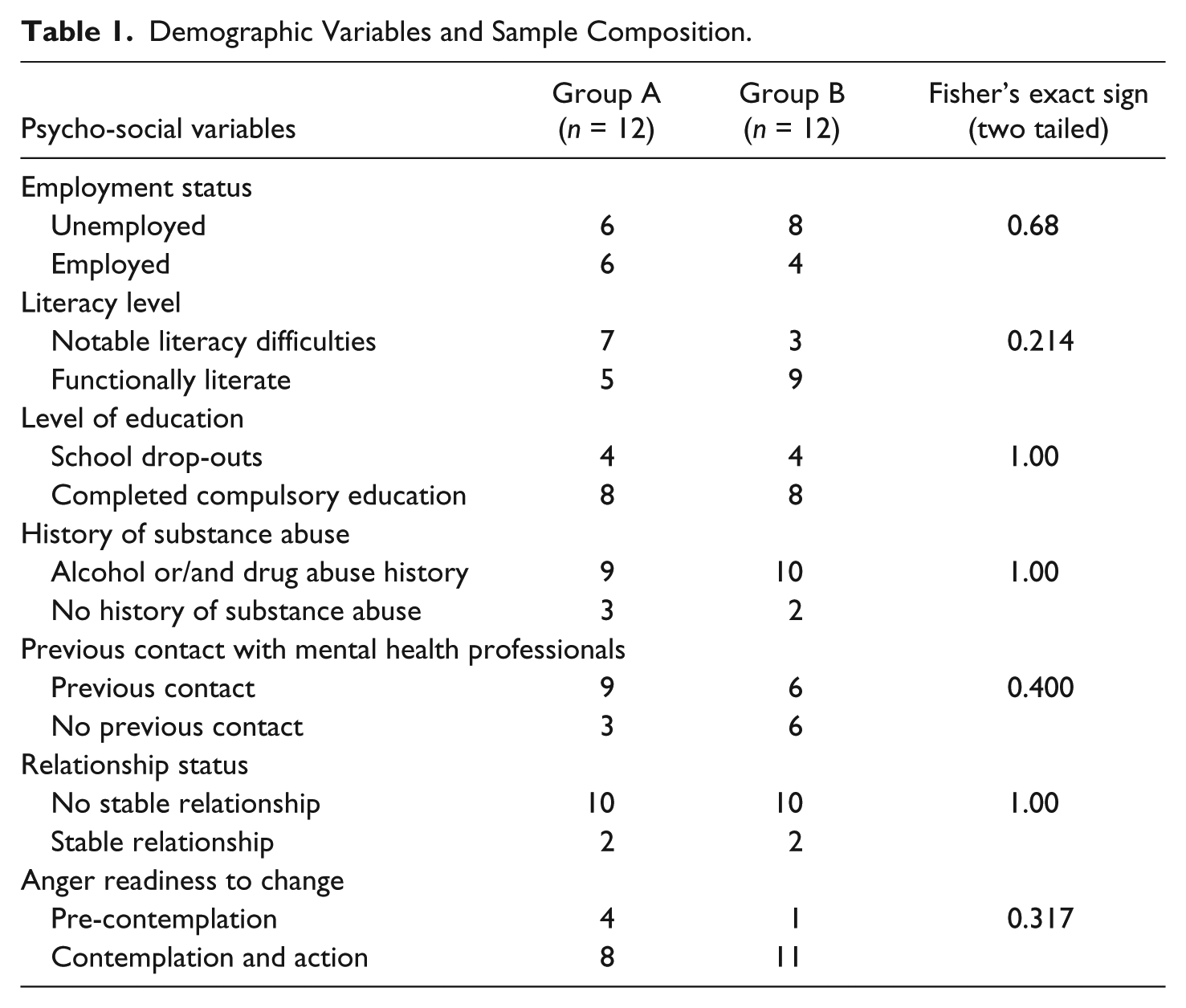
Cross tabulation analysis was carried out to assess for any differences in the group allocation (Group A and B). Since some of the cell values had small expected frequencies (less than 5) the Fisher’s Exact Test was used. All the results were not statistically significant which indicated that the variables of interest were similar in Group A and Group B (see Table 1 and 2).
Demographic Variables and Sample Composition.
Criminal History Variables and Sample Composition.
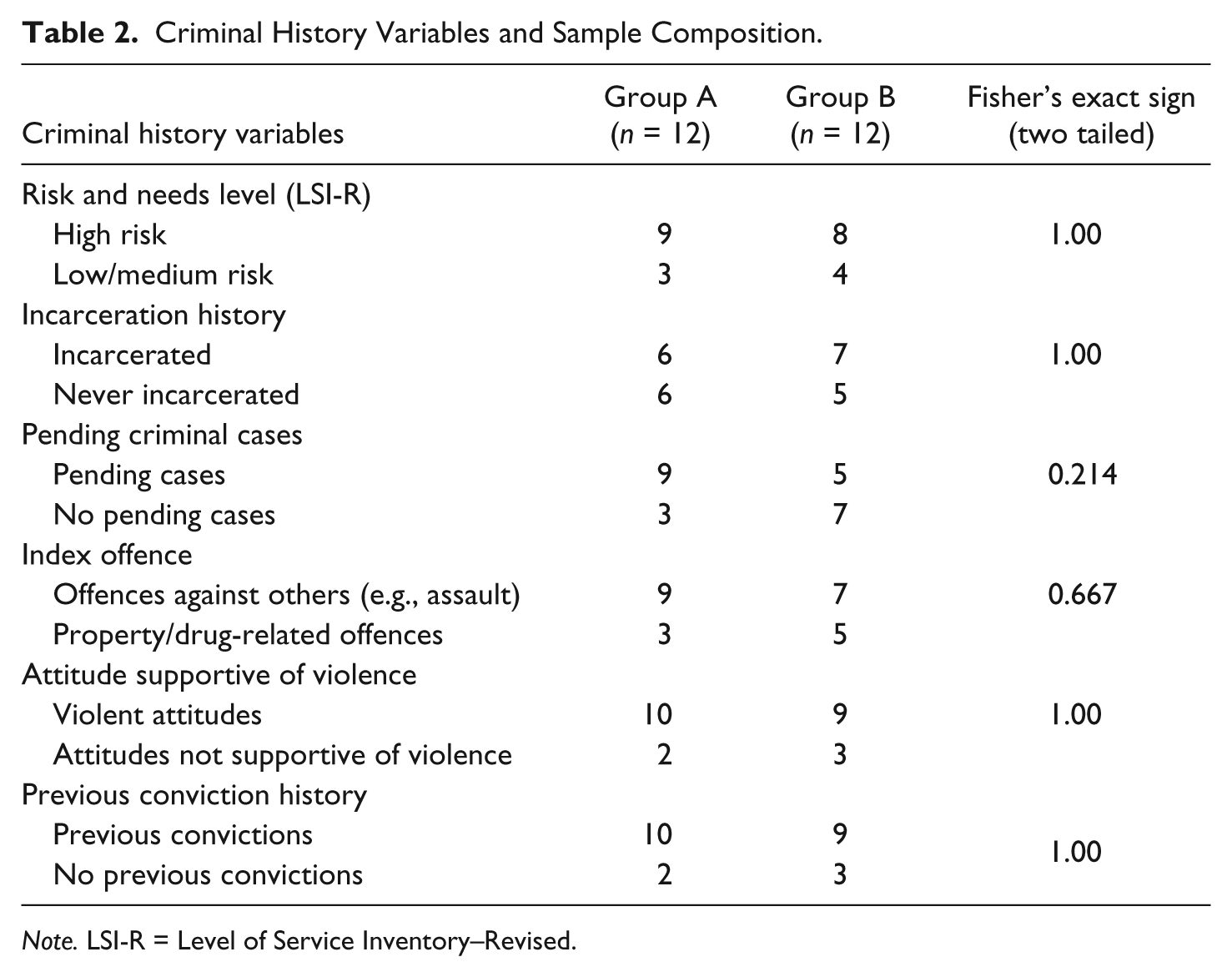
Note. LSI-R = Level of Service Inventory–Revised.
Demographic Variables
The mean age for Group A was 33.25 (SD = 12.32) and for Group B 33.08 (SD = 10.51). Statistical analysis revealed no significant difference between groups on age, t(0.36) = 21.465, p = .972.
More than half (58.3%) of the participants were unemployed at the time of the study. Although 66.7% reported to have completed their compulsory education, a substantial proportion (41.7%) of the participants reported to be illiterate in Maltese and English. This may indicate a socially disadvantaged background. Most participants (79.2%) were reported to have had a significant alcohol or drug abuse problem in the past and 62.5% had previous contact with mental health professionals mainly in relation to substance abuse or for assessments purposes. None of the participants had previously been in treatment for anger management or violence reduction. Another requirement for admission to the program was that clients were not currently abusing substances for at least the last 12 months prior to the program. Those referred with a comorbid problem of substance abuse were excluded and referred for other more appropriate interventions. The results of the Anger Readiness to Change Scale indicated that a substantial proportion (approx. 79%) of the participants were either in the contemplation or action phase.
Criminal History Variables
The participants were all assessed by their probation/parole officers as having significant issues with anger control or attitudes supportive of violence. The screening process might have led to high risk offenders being overrepresented in the sample. The results from the LSI-R (Andrews & Bonta, 1995) show 70.8% of offenders referred as high risk for recidivism and in high needs for supervision. Of those, 58.3% also had other pending criminal court proceedings, 79.2% had previous convictions, and a further 54.2% had been incarcerated in the past. In terms of index offence, most participants were serving a supervision order for crimes against persons such as assault or threats against others (66.7%). The other 33.3% had been sentenced for property or drug-related offences.
Analysis of Social Desirable Responding
At pre-intervention, TP 1, none of the participants exhibited social desirable responding. However at TP 2 and TP 3, a number of participants had scores on the PII of less than cut off (<15). Table 3 consists of a cross tab analysis of the observed frequencies on the levels of anger and social desirability. The level of anger was categorized into clinically significant anger (> 65 on the ADS total score) and non-dysfunctional anger (< 65 on the ADS total score). The social desirability responding was categorized into social desirable responding (< 15 of the PII) and no social desirable responding (> 15 of the PII) across TP 2 and TP 3. The Fisher’s Exact test (two sided) could only be calculated for Group A at TP 3 which was not significant (p = 1.00). The small sample size limited the further analysis of the relationship between scores on the PII and the level of anger dysfunction.
Cross Tab Analysis of the Positive Impression Index.
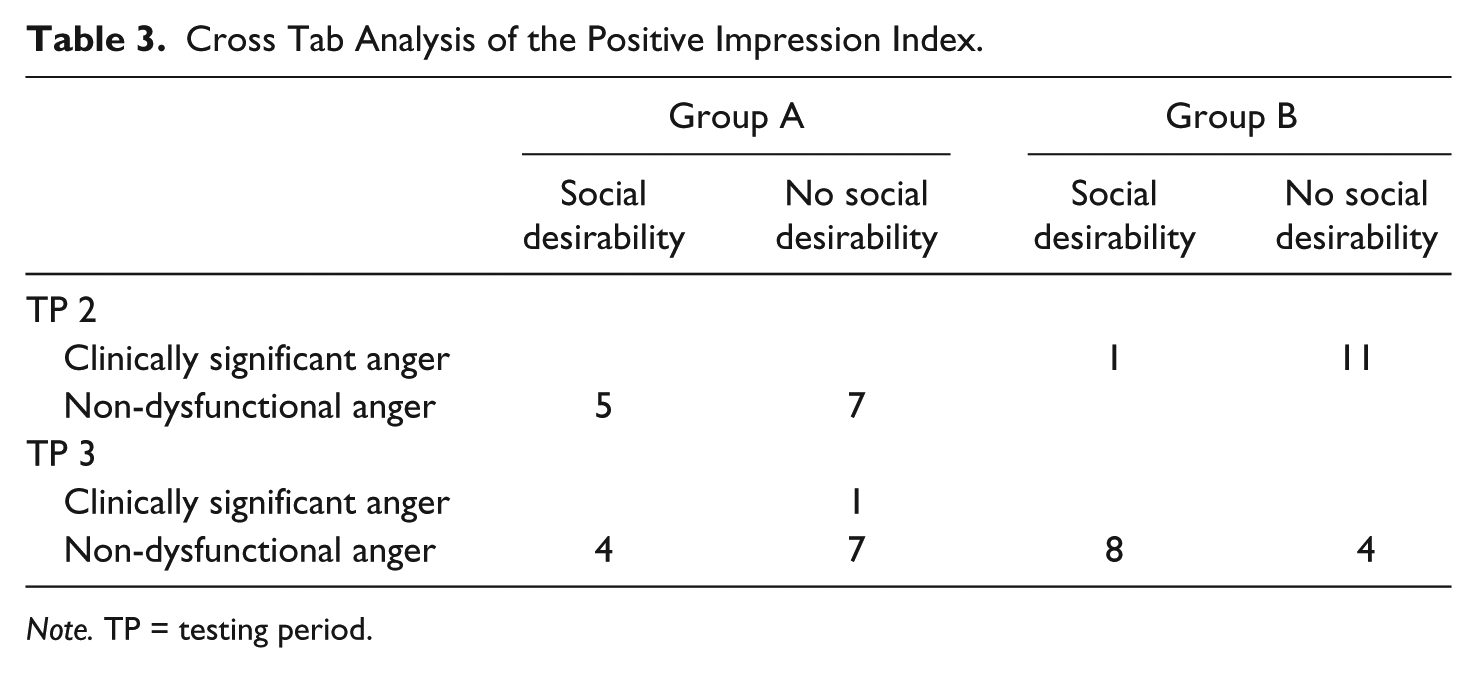
Note. TP = testing period.
As it appeared that positive impression responding emerged mostly after the delivery of interventions for both groups (TP 3), a separate analysis was carried out. For this analysis, participants were categorized according to levels of social desirability (15 as the cut-off point). It was considered that the group that did not demonstrate social desirable responding would not show statistically significant differences in the outcome scores if the result is only due to impression management. On the other hand, significant post-treatment differences in the outcome measures in this group would indicate an effect of treatment regardless of the desire to manage their impression.
Table 4 shows that both the social desirable responding group and those above the cut off of the PII experienced significantly lower post-intervention scores on the ADS total. This might indicate a treatment effect regardless of the desirability demonstrated by some of the participants.
Mean Scores on the Positive Impression Scale.
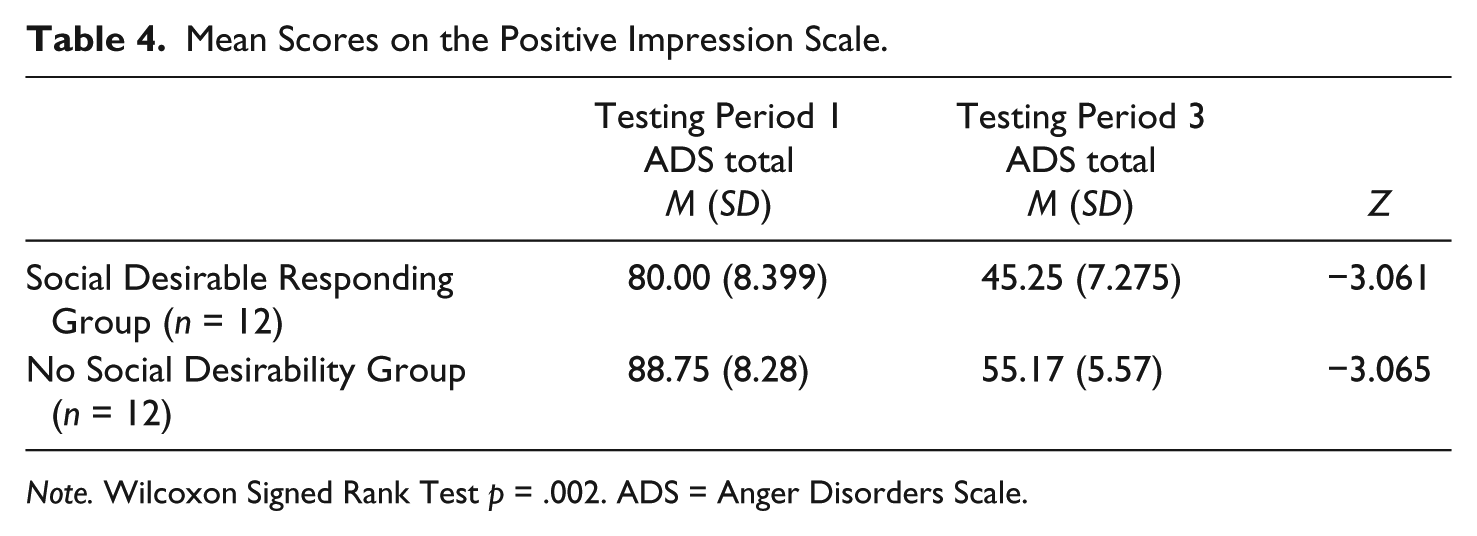
Note. Wilcoxon Signed Rank Test p = .002. ADS = Anger Disorders Scale.
Results
Within-Group Analysis
A necessary inclusion criterion was pathological anger so the anger level of participants was possibly higher than the anger level of the general population. An analysis of skewness and kurtosis of the ADS baseline measures indicated that the data were fairly normally distributed at pre-intervention: Reactivity scale skewness was −.588 (SE = .472) and kurtosis .801 (SE = .918); Anger In scale skewness was −.152 (SE = .472) and kurtosis −.492 (SE = .918); Vengeance scale skewness was −.156 (SE = .472) and kurtosis −.734 (SE = .918); and the ADS total scale skewness −.242 (SE = .472) and kurtosis .356 (SE = .918). Despite the normal distribution of the sample on this measure, non-parametric analyses were carried out due to the small sample size. Furthermore, the items and subscales of the ADS are purposefully positively skewed and the ADS also uses linear T-scores that are positively skewed. In fact, most of the analysis reported in the ADS Technical Manual used non-parametric statistics (Di Giuseppe & Tafrate, 2004). Consequentially, the Freidman test was used to assess for pre- and post-intervention differences in Groups A and B. Post hoc analysis was then carried out using the Wilcoxon Signed test with the Bonferroni adjustment to adjust for multiple comparisons. Thus, the within group analysis sought to explore significant differences in the baseline scores (TP 1 for Group A and TP 1 and TP 2 for Group B) and the outcome scores (TP 2 and TP 3 for Group A and TP 3 for Group B).
Table 5 displays the mean and standard deviations of the outcome measures at the different testing periods and the results of the within group analysis using the Freidman test for Group A.
Group A Within-Study Results Across the Testing Periods.
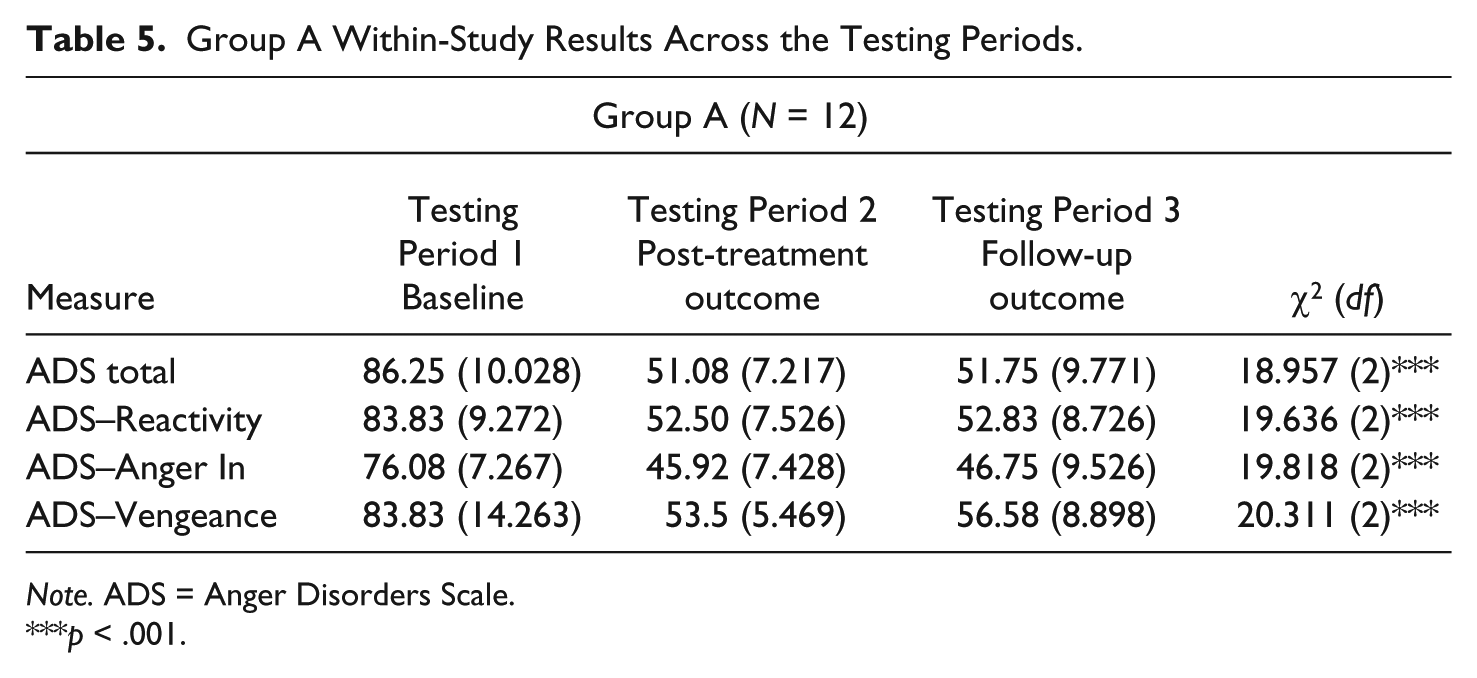
Note. ADS = Anger Disorders Scale.
p < .001.
The differences between the baseline and outcome scores on the ADS total score were statistically significant. Post hoc analysis using the Wilcoxon Signed Rank Test applying the Bonferroni Adjustment (p value set at < .017) indicated a significantly different score on the ADS total scores between pre-intervention and post-intervention (z = −3.061, p = .002) and between the pre-intervention and follow-up scores (z = −3.064, p = .002). Post-intervention and follow-up scores were significantly lower than the pre-intervention scores on the ADS total score measure. There was no significant difference between post-intervention scores and follow-up scores (z = −0.563, p = .574).
The results of Group A on the higher order scales of Reactivity, Anger In, and Vengeance were all statistically significant which implied that the distributions on these scales were different at the different measurement periods.
The related samples Freidman test indicated significant differences between the baseline (TP 1) and outcomes scores (TP 2 and 3) for Group A. Post hoc analysis showed significant lower scores between pre- (TP 1) and post-treatment (TP 2) on Reactivity (z = −3.065, p = .002), Anger In (z = −3.068, p = .002), and Vengeance (z = −3.061, p = .002). Significantly lower scores were also observed between the pre-intervention scores (TP 1) and the follow-up scores (TP 3) on the Reactivity scale (z = −3.062, p = .002), the Anger In scale (z = − 3.068, p = .002), and the Vengeance scale (z = −3.063, p = .002). No significant differences were observed between post-treatment scores (TP 2) and follow-up scores (TP 3) on the Reactivity scale (z = .000, p = 1.00), Anger In scale (z = −.722, p = .470), and the Vengeance scale (z = −1.931, p = .053).
Group B was first tested at baseline (TP 1) and then placed on a 3 month waitlist. Prior to delivering the interventions, another baseline measure was collected (TP 2). This was supposed to control for the effects of time, standard error in measurement due to retesting using the same tools, and the effects of supervision. The outcome measures were then recorded following the delivery of the intervention (TP 3). Statistical analysis using the Freidman test showed significant differences in the median scores of the four scales analyzed across the three testing periods (Table 6).
Group B Within-Study Results Across the Testing Periods.
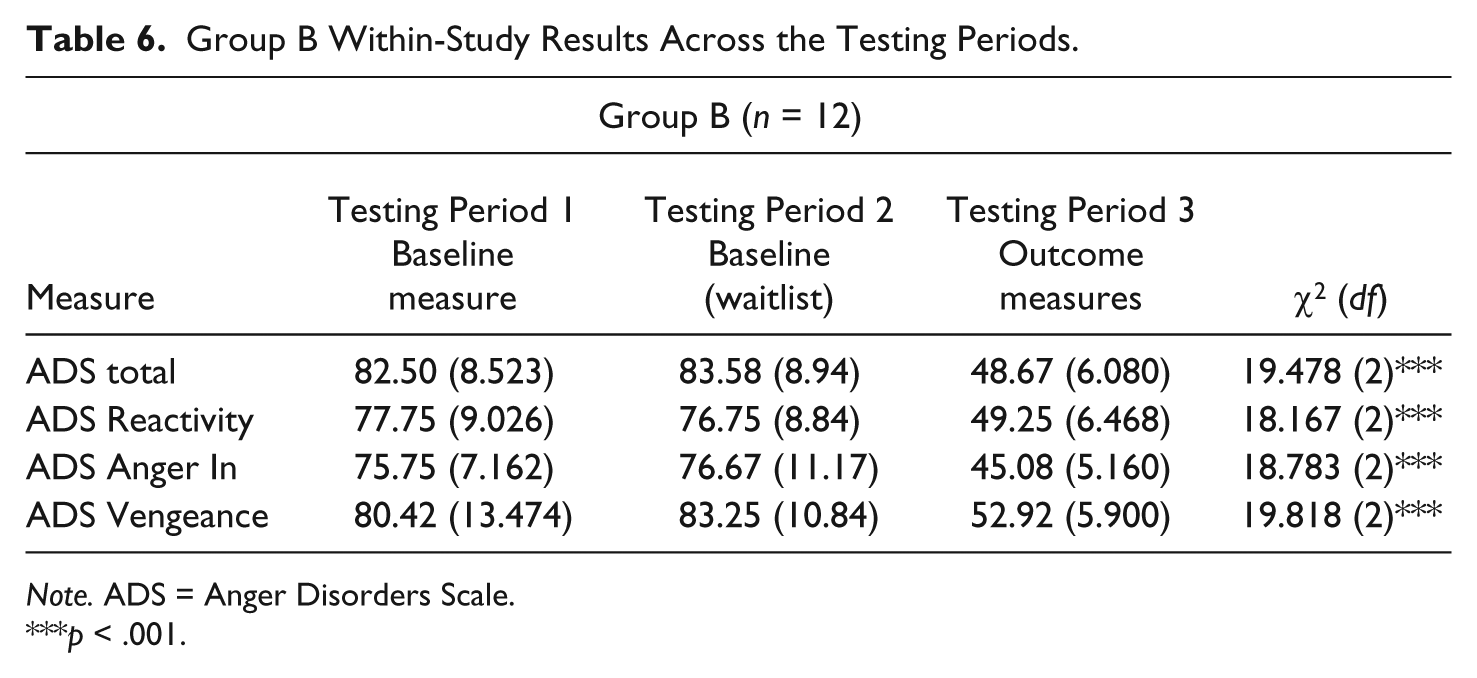
Note. ADS = Anger Disorders Scale.
p < .001.
Post hoc pairwise comparisons using the Wilcoxon test with a Bonferroni adjustment explored the statistical significance between each time period. The median scores on the baseline measures, that is, TPs 1 and 2 of Group B for the ADS total score (z = −.767, p = .443), the Reactivity scale (z = −.670, p = .503), Anger In scale (z = −.102, p = .919), and Vengeance scale (z = −1.268, p = .205), were all not significant. The pairwise comparisons between TP 1 (baseline) and TP 3 (outcome) showed significantly lower scores at the outcome stage for the ADS total (z = −3.061, p = .002), the Reactivity scale (z = −3.063, p = .002), the Anger In scale (z = −3.063, p = .002), and the Vengeance scale (z = −3.063, p = .002). Similar results were also obtained in the comparisons between TP 2 (baselines after the waitlist period) and TP 3 (the outcome measures post-intervention) showing significant reduction in scores after interventions on the ADS Total score (z = −3.062, p = .002), the Reactivity scale (z = −3.062, p = .002), the Anger In Scale (z = −3.063, p = .002), and the Vengeance Scale (z = −3.063, p = .002).
Between-Group Analysis
A Mann Whitney test (Table 7) on the ADS total scores indicated that only the scores at TP 2 were significantly different between Group A (equivalent to post-treatment) and Group B (the waitlist before intervention group) U = .000, p < .001 with scores in Group A (Mdn = 52.5) being significantly lower than Group B (Mdn = 85). There was no significant statistical difference between Group A and Group B on the baseline measure at TP 1 (U = 60.0, p = .487) and the final outcome measures at TP 3 (U = 53.0, p = 271).
Between-Group Comparisons on the Three Testing Periods Using the ADS Total Score.
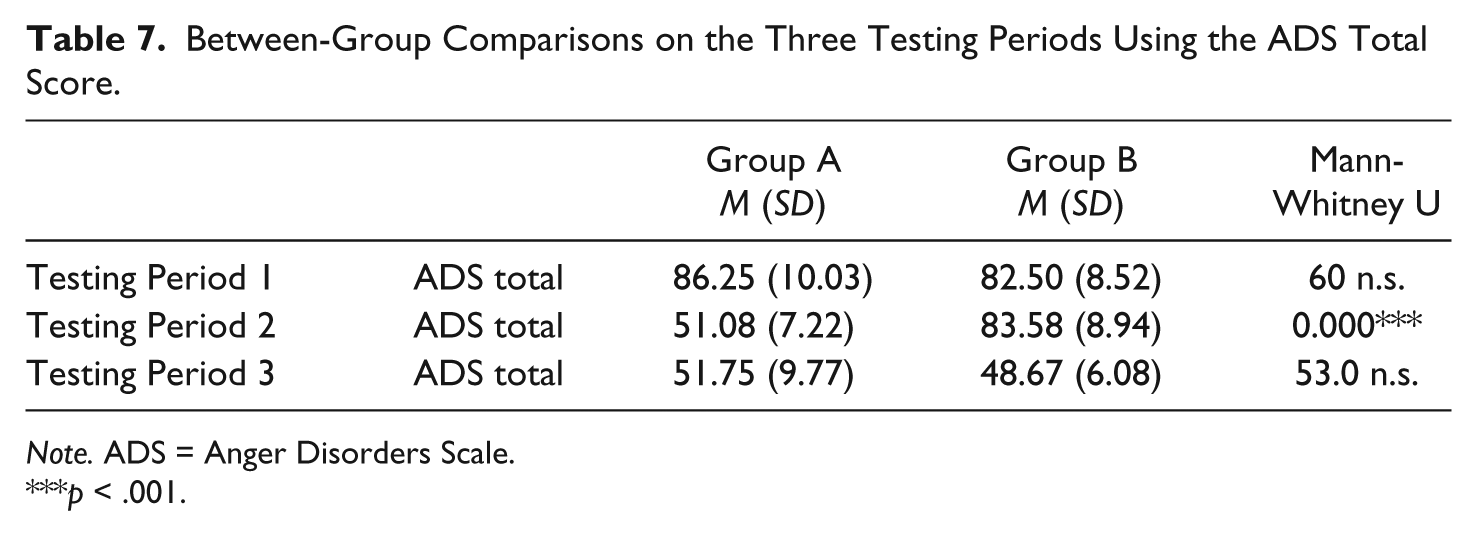
Note. ADS = Anger Disorders Scale.
p < .001.
Clinical Significance
Using the raw scores on the ADS total at TP 1 and TP 3, which is equivalent to a period pre-intervention and post-intervention for both groups, an analysis of clinically significant change (CSC) was carried out through the Leeds Reliable Change Indicator (Morley & Dowzer, 2014). The pre-treatment raw score mean was 59.71 (SD = 7.66) and at TP 3 the raw score mean was calculated at 32.08 (SD = 6.68). The Reliable Change Index was estimated at 7.05 with a standard error of measurement of 2.54. This analysis demonstrated that all participants experienced improvement following the intervention. Furthermore, 14 also met the CSC criterion c with their mean placing closer to the mean of the normative comparison group than the mean for the clinical samples reported in the ADS Technical Manual (Di Giuseppe & Tafrate, 2004). All raw scores on the ADS total of the 24 participants post-treatment fell within 1.96 standard deviations of the mean raw score of the normative comparison group reported in the manual.
Summary of Results
Significant post-treatment effects in both Group A and Group B were observed, indicating substantial improvements in self-reported anger symptoms. Significantly lower dysfunctional anger was reported even after the follow-up period (TP 3 for Group A), indicating possibly that the treatment gains were maintained over stipulated time period. Within group analysis on Group B, the waitlist group showed that there were no significant differences between the baseline scores at TP 1 and TP 2, which might indicate that without the intervention, the reported anger symptoms remained constant over the 3 month waitlist period. In other words, time and supervision did not have significant effects on self-reported anger. It also indicated the reliability in the measures of anger used although this was not analyzed statistically. Significant differences where noted between the scores obtained in TP 1 and TP 2 when compared with the scores in TP 3, indicating that post-intervention the participant scores showed lower levels of anger. This supported the analysis of Group A in finding statistical differences post-administration of the I-MAP.
Between-group comparisons were carried out on the ADS for the three time periods. No differences were found in the scores on anger at TP 1 (the baseline) and at TP 3 (the outcome), indicating that at pre-intervention (TP 1) the scores on the anger measures of Group A and Group B were similar. No significant differences between the scores of Group A (follow-up) and Group B (post-intervention) at TP 3 might mean that the effect of the I-MAP was similar for both groups with a significant reduction in the negative symptoms of anger in both groups following treatment.
Discussion
Findings from studies exploring the effects of short-term anger management on offender samples are often contradictory. For example, Heseltine et al. (2010) found no reductions in measures of anger following a 20-hr anger management program except for increased anger knowledge post-intervention. However, Chen et al. (2014) found significant post-treatment reduction in self-reported hostility, impulsivity, and observed aggression in their RCT on anger management for young offenders. Thus, it indicated that anger management was successful in reducing symptoms associated with anger dysregulation. Similarly, Black et al. (2011) found that those inmates completing a 10-week anger management program experienced significantly lower reported anger on the STAXI-II post-intervention when compared with the unmatched controls. The results of this study seem to support the main conclusions of these latter studies, showing that anger management can effectively reduce symptoms of dysfunctional anger among offender populations. Due to the association between anger and some forms of violence, it was expected that the significant reductions in anger symptoms as measured by psychometric measures would not only lead to a better quality of life for the offender but also lower the risk of engaging in violent behavior (Novaco, Ramm, & Black, 2001). Indeed some studies concluded that offenders who were exposed to or completed an anger management program (Dowden, Blanchette, & Serin, 1999; Dowden & Serin, 2001) had significantly lower general and violent reoffending rates than their controls. By addressing emotional regulation and developing self-management skills, which were integral parts of the intervention, the supervision and case management of the community-based offender might have been facilitated.
The treatment effect might have been a factor of the treatment components of the program, the I-MAP. Towl (1994) maintains that effective anger management should focus on increasing the regulation of physiological arousal, increasing behavioral strategies, and challenging thinking errors. These three components are intrinsic features of the treatment program used in the research study.
Individualized Treatment
Despite the small size of the sample in the study and the relatively short duration of the interventions approximately of 14 hr per participant, a substantial treatment effect was noted. This treatment effect could in part be explained by the format of interventions. One-to-one sessions could have mitigated for the relative brevity of the intervention. The program itself is designed to offer the client a myriad of skills and techniques from which the participant would then chose those that most suit their idiosyncratic needs. This together with careful fostering of a therapeutic bond might have facilitated change in the participants.
Most interventions reported in the aforementioned studies were carried out in a group basis (e.g., Chen et al., 2014; Heseltine et al., 2010). This in part might be due to financial reasons as group therapy could potentially address larger number of offenders. However, a more individualized approach to treatment might also have significant cost-effective implications in addressing anger disturbances.
Importance of Screening
As an intervention, the I-MAP contains a blend of CBT techniques and mindfulness strategies, which are recommended for individuals with anger and information processing problems, deficiencies in emotional regulation, and impulsivity (Walker & Bright, 2009). Ireland (2004) concluded that anger management interventions should be administered only with angry offenders and anger measures should be used to assess anger. Therefore, the screening process in this study could have contributed to selecting candidates that might benefit the most from the intervention, which in turn could have enhanced the treatment effect.
The large number of offenders referred for anger dyscontrol who did not have violent crime as their index offence further supports the need for screening and assessment to determine eligibility for anger management rather than assessing eligibility on the basis of index offence. The similarity between the two groups despite randomization might be due to the relative homogeneity of the population from which the sample was extracted. Also the screening process could have contributed in the selection of clients with very similar characteristics.
Readiness to Change and Mindfulness Components
Davey, Day, and Howells (2005) argue that readiness to change might facilitate the development of therapeutic engagement. Indeed, a large proportion (n = 19) of the participants were deemed to be either in the contemplation or action stage in terms of readiness to change prior to administering treatment. This readiness to change was facilitated throughout the program by focusing on the individual needs of the participants and adopting developmental perspectives in conceptualizing and contextualizing their anger symptoms in the initial phases of the program (Howells, 2004; Honos-Webb, Stiles, & Greenberg, 2003). This might have contributed to the treatment effect noted in this study.
The mindfulness training in the I-MAP could have also contributed positively to the magnitude of the treatment effect. Wright, Day, and Howells (2009) maintain that mindfulness might increase the process of cognitive change and increase self-regulatory behavior when experiencing anger states by preventing the maladaptive anger responses.
Limitations and Future Research
This study shows that an RCT can be carried out within the criminal justice system. Nevertheless, a number of biases and limitations could have affected the analysis of treatment effectiveness.
Firstly, the rigorous participant screening process could have limited an already small pool of potential participants from community-based offenders in a small island. Future research could extend the recruitment period to increase the sample size while maintaining the pre-intervention screening. A larger study could also incorporate a cost-effectiveness analysis comparing one-to-one and group-based interventions.
A major issue of any community-based program for offenders is high attrition rates as it might not only affect the study but also might pose a greater risk for recidivism (McMurran & Theodosi, 2007). Effective monitoring and supervision by probation officers was encouraged to increase the retention of participants in the study during the 3 month follow-up for Group A and 3 month latency period for Group B. The reported attrition of about 8% in this study is low for a community-based study with offenders. The individualized format of the interventions and the continued supervision could have contributed to the retention of participants. Participants received treatment on a voluntary basis although one must acknowledge that they were directed toward interventions by their probation/parole officer. One-to-one interventions had the distinct advantage of moving with the pace of the client receiving the intervention and might have fostered a greater therapeutic bond. It also allowed sufficient logistical flexibility to reschedule and reorganize sessions when the client could not attend. Most group-based interventions would not have this flexibility and consequentially either clients miss out on important therapeutic aspects or skills or are removed from the program altogether.
The number of offenders offered the intervention and yet refused to attend or did not consent for the sessions were not recorded. Such information would be useful in gauging the level of attrition bias and the type of offenders that are resistant to treatment. Furthermore, the analysis in this study only focused on those participants who received the treatment and complied with the research protocol. Such an analysis might be useful to estimate the effectiveness of the interventions delivered at the intended intensity and dose and would help validate the I-MAP as an effective program. It might be argued that those participants who did not turn up for the appointments and/or breached conditions might have a poorer prognosis than those completing treatment. An intention-to-treat analysis could have been used with the few participants who did not complete the treatment.
Other Sources of Bias and Socially Desirable Responding
The participants were aware that they were participating in a study exploring anger symptoms and the response to treatment. Therefore, the post-intervention reduction in the anger symptoms might have been a result of a Hawthorne effect, where their responses might have been modified as a consequence of being studied.
Furthermore, group allocation was not concealed to the main researcher. However, the fact that the researcher carried out the assessments as well as delivered the interventions might have helped in fostering a sense of therapeutic alliance with the participants and increase their commitment. Conversely, the substantial treatment effect observed might have also been a by-product of the therapeutic alliance itself as clients might have felt compelled to exaggerate the effects of the program out of a desire to please the researcher/therapist. This occurred primarily after considering the resources available for research at the DPP. Future research might consider external measures to avoid potential sources of bias such as recruiting independent professionals to carry out the assessment.
Polaschek, Bell, Calvert, and Takarangi (2010) suggest that self-reported measures with offenders might be prone to social desirability in the response pattern. In fact half the sample demonstrated social desirable responding when the tests were administered at the outcome phase and this could have confounded the true treatment effect size. The psycho-educational component of the intervention might have taught clients how to respond appropriately to particular items in the outcome measures due to a better recognition of “angry responses.”
The instructions given to the participants could have also affected this type of responding. To make the tools more sensitive to treatment effects or to changes in anger levels at different points in time, the participants were instructed to rate particular items according to frequency or duration of the particular behavior since the previous administration of the test. This instruction could have invalidated the scale as some of the items require respondents to rate whether a statement describing their anger holds true for the participant for the past year, months, weeks, or days. The response is in a likert-scale format with the longer duration incurring higher scores (e.g., Item 5 of the ADS).
Nevertheless, an analysis comparing the pre- and post-treatment scores of those participants who did not exhibit socially desirable responding, still demonstrated significantly lower scores after treatment. Thus, despite the susceptibility of psychometric measures to social desirable responding in offender populations, there might be some significant treatment change. Furthermore, Di Giuseppe and Tafrate (2001) maintain that the PII was only validated on clinical populations and a low score on this scale might also be indicative of normalized anger reactions. This could imply that the scores of post-intervention had decreased significantly to the extent that their anger was no longer dysfunctional and within normal experience. The use of further assessment tools such as the Paulhus Deception Scales (Paulhus, 1999) may gain more insight in any tendency of impression management by the participants.
The Use of Psychometric Measures
A substantial proportion of participants had literacy difficulties especially in the English language. Great care was taken during the interventions to cater for the educational differences of the offenders. However, certain aspects might have reduced the effectiveness of the interventions. For example, many participants reported that they could not complete tasks that require some academic skills such as the diary. Although alternatives to writing were explored in some cases, the diary was completed during the intervention session. This could have introduced bias of exploring “angry” events after the passage of time and led to reporting only the issues the client expected the therapist wanted to hear. It also increased the time spent competing and analyzing the journal which could have limited the amount of time spent exploring other components of the I-MAP. Language difficulties could have introduced bias and error in the measures of anger.
The psychometric measures used in this study have not been validated on Maltese samples, and unfortunately there are no standardized norms of Maltese populations. Also the psychology profession in Malta has not yet sought to officially translate many of the psychometric tools to Maltese. Even though Malta is officially a bilingual country, many offenders express difficulty in communicating in English. Thus, the use and interpretation of tools has to be done with great care. Nevertheless, the tools in this study used very simple English. In fact, the ADS’s readability analysis based on word and syntax difficulty was determined to be of the reading level of a 10 to 11 year old (Di Giuseppe & Tafrate, 2001).
Furthermore, self-reported measures may only measure attitudinal changes which may not translate into behavioral change. During the sessions, the therapists monitored the behavioral reactions of clients through their analysis of journal to assure of their progress. However, such data were not analyzed in this study. Further research could focus on the possible long-term behavioral effects of the program through following up on the recidivism rates of those offenders who underwent the program or monitoring the frequency of anger expressions. Furthermore, it might inform practitioners on how well the reduced self-reported anger scores translate into positive behavioral change.
Footnotes
Acknowledgements
We thank Dr. Chantal Avellino, psychologist at the Department of Probation and Parole Malta, for her help with some of the interventions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially funded through the Malta Government Scholarship Scheme.