
Abstract
The aim of this study was to compare results of and develop guidelines for mandatory allocation of sexually transgressive juveniles to Multisystemic Therapy - Problem Sexual Behavior (MST-PSB), Secure Youth Care (SYC), or Forensic Youth Care (FYC), based on the risk-need-responsivity model. Results of current allocation showed a population with relatively less treatment needs to receive community-based MST-PSB, compared with populations receiving residential SYC and FYC. Furthermore, estimated recidivism risk levels did not always support the need for risk reduction by the imposition of limitation of freedom of movement and maximum supervision, provided by all three treatment modalities. Based on the assessed sexual recidivism risk, 38% of the juveniles in FYC, 7% in SYC, and 24% in MST-PSB received treatment that was too intensive, which is considered detrimental to motivation and development. Future allocation practices could benefit from assessing treatment needs and recidivism risk, by use of an actuarial tool.
Introduction
Background: Literature Review
A significant proportion of sexual offenses are considered to be committed by juveniles. Studies estimate that between 20% of rapes and 30% to 50% of child molestations are committed by adolescent males (Barbaree & Marshall, 2006), for whom consequently allocation to treatment is an option. Research into allocation practices, however, is scarce. Such research may prove useful, especially among juveniles who have shown sexually harmful behavior, a notoriously heterogeneous group. Several studies into typologies, specific mental illnesses, traits, executive functioning, and personality profiles of adolescents who have sexually offended have been conducted (e.g., Adjorlolo & Egbenya, 2016; Butler & Seto, 2002; Drew, 2013; Glowacz & Born, 2012; Hart-Kerhoffs, Doreleijers, Jansen, van Wijk, & Bullens, 2009; Hendriks, 2006; Hissel, Bijleveld, Hendriks, Jansen, & Collot d’Escury-Koenigs, 2006; Kjellgren, Wassberg, Carlberg, Långström, & Svedin, 2006; Lawing, Frick, & Cruise, 2010; Margari et al., 2015; Purcel, 2010). Caldwell (2010), after conducting a meta-analytic review, stated that developmental issues (i.e., incomplete maturation, impulsiveness or exploratory behavior) might be important factors in the etiology of juvenile sex offending. Seto and Lalumiere (2010), also through a meta-analytic study, found sexually transgressive juveniles to have risk factors in common with juvenile non-sex offenders (i.e., age of onset, antisocial thoughts, and behavior patterns), but also found them to differ (i.e., more sexual victimization and deviancy, more social and emotional dysfunctions, and more learning problems), suggesting other risk factors may (also) play a role in the development of sexual transgressive behavior. Lussier, Van den Berg, Bijleveld, and Hendriks (2012) defined a small subgroup (10% of their total sample, N = 498) of sexually transgressive adolescents who sexually offended at a relatively high rate, and of whom 60% persisted in sexual reoffending even beyond adolescence: the high rate, slow desisters. None of the aforementioned traits or typologies, however, was found exclusively in this group, making it hard to identify them prospectively, that is, at allocation.
For allocation practices, the etiology of transgressive behavior is very important. For, when deemed primarily antisocial or adolescence limited in nature, non-specialist treatment may prove a good fit. When origins are deemed more sexually deviant or pervasive in nature, a specialized type of treatment, aiming prominently at, for example, specific cognitive distortions, may prove the best fit. We aim to contribute to the literature on juvenile sex offender typology by offering a description and comparison of recidivism risk levels and treatment needs of juveniles who have sexually offended in the Netherlands.
Treating Juveniles Who Have Sexually Offended in the Netherlands
In Europe, important differences exist between juvenile justice systems. Countries have developed their own approach in offering juveniles the help they need and/or punishing undesirable behavior (Walgrave & Mehlbye, 1998). For example, in the Netherlands, the lower limit for adjudication is 12 years of age, whereas in the neighboring countries of Great Britain and Belgium this limit, respectively, is 10 versus 18 years (Brouwers, 2007). In most European countries, a continuum between youth protection services and a juvenile justice system is available. Both systems usually are equipped to respond to transgressive behavior and are able to mandate supervision or treatment. In comparison with other European countries, in the Netherlands, a relatively large number of juveniles are detained (and receive treatment there). Only in Germany, and in England and Wales, juveniles are imprisoned more often (Kalidien & De Heer-De Lange, 2015). In contrast, in Sweden and Denmark, detaining juveniles is very rare. Core of the Dutch policy on justice involved interventions is to intervene only when the development of a juvenile is threatened. Compared with other European countries, justice involvement is less prevention focused (Bol, 2002).
In Figure 1, a representation of the Dutch process of (mandatory) allocation into intensive treatment for sex offending is presented. Non-specialized treatment options (i.e., treatment aimed at transgressive behavior in general) or non-intensive treatments available (i.e., psychoeducation on sexual transgressions; Jonker, de Haas, Reijmers, Rekers, & Van Berlo, 2011, and specialized outpatient treatment; Hendriks, 2011) are not included in this diagram. In both allocation pathways (civil law on the left and criminal justice on the right), an evaluation is performed to establish the etiology of the problem behavior, and determine risks and treatment needs. Different professionals and methods, however, are used. In the “civil law pathway”, first, a youth protection board caseworker assesses the reported situation. When the decision is made to resort to mandated residential care, an independent psychologist has to agree. Specialized contextual treatment can be administered without an independent assessment of treatment needs. In the “criminal justice pathway”, the prosecutor’s office first establishes whether or not prosecution is feasible. If a decision to prosecute is reached, an independent forensic psychological and psychiatric evaluation, making use of structured risk assessments, is performed to advise the juvenile judge.
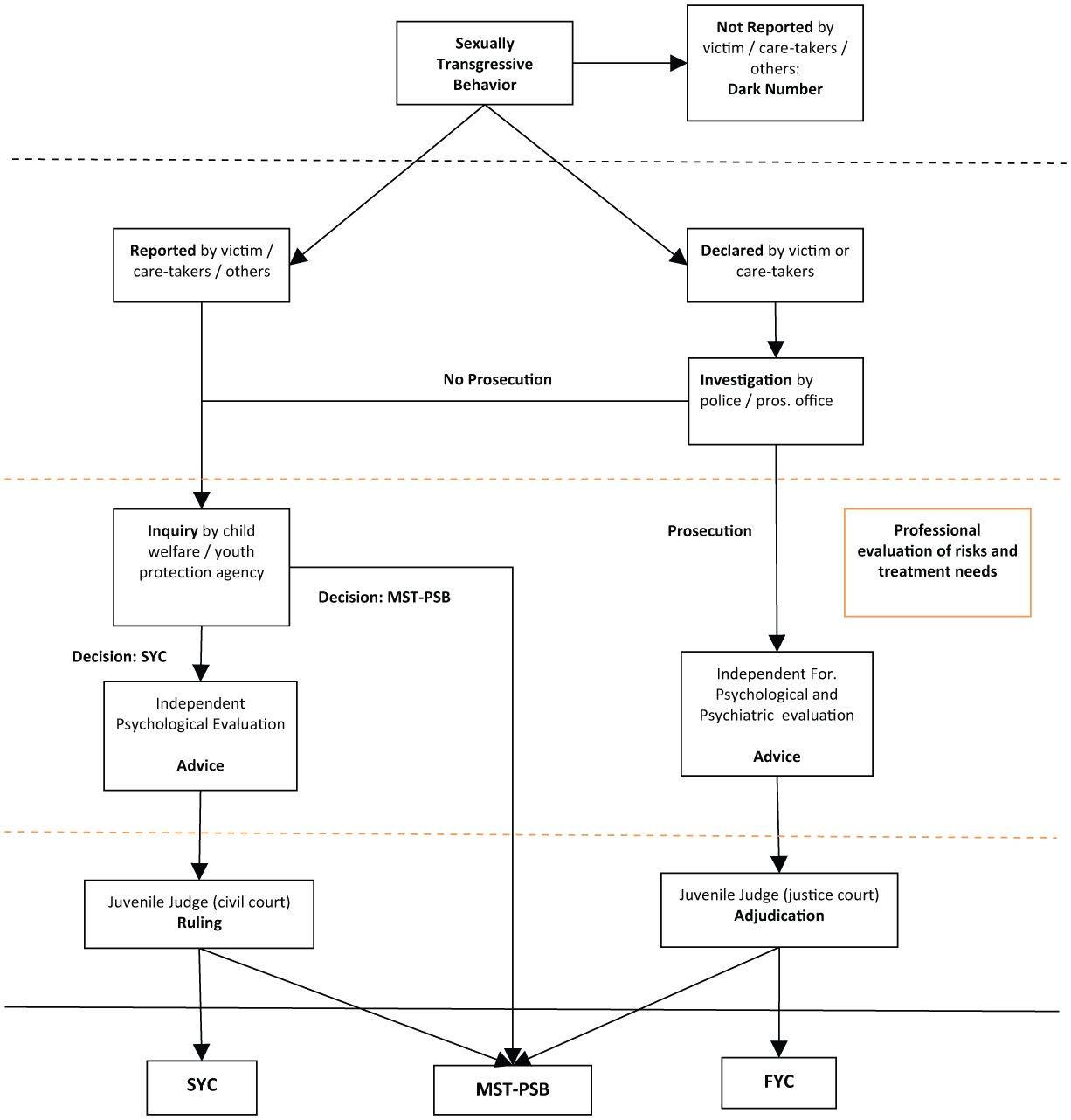
Schematic process of allocation to intensive specialized treatment.
If specialized intensive treatment is necessary, a 5- to 7-month community-based treatment, multisystemic therapy for youth with problem sexual behavior (MST-PSB; Borduin, Henggeler, Blaske, & Stein, 1990), is available via both pathways. MST-PSB is aimed at adjudicated and non-adjudicated juveniles aged 10 to 18 years, who exhibit sexually deviant behavior, have complex (family) issues, and pose a risk to society (Borduin et al., 1990). Because MST-PSB is a community-based type of treatment, the family system involved needs to actively take responsibility for safety issues during the at-home treatment. The exact nature of interventions applied varies for each family, depending on their strengths and weaknesses, although the interventions mainly involve cognitive behavioral and family therapeutic techniques (Henggeler, Schoenwald, Borduin, Rowland, & Cunningham, 2009). Contraindications for the MST-PSB program are an IQ < 70, acute psychiatric problems, and severe forms of autism (Boonstra & Van der Rijken, 2010).
Another intensive specialized treatment available for non-adjudicated juveniles (aged 12-18 years) is mandated specialized treatment in a Secure Youth Care (SYC) facility. Dutch law on youth care (Hirsch Ballin, 2007) states that the invasion of fundamental children’s rights, such as restricting freedom of movement, must be kept to a minimum, and therefore is applicable only (by civil court order) if so advised by an authorized psychologist. SYC should adhere to minimalizing imposed restrictions of freedom and the shortest possible stay, with youngsters receiving further treatment in less restrictive settings (Veldhuijzen van Zanten-Hyllner, 2011). Contraindication for placement is an IQ < 70; these youngsters receive treatment in institutions for the mentally disabled. One specialized SYC treatment group (10 beds) is available in the Netherlands.
A second possibility for adjudicated juveniles who have sexually offended (12-18 years of age at the time of the offense) is treatment in Forensic Youth Care (FYC), of which there are 16 beds available in the Netherlands. In accordance with the European Rights of Children (Council of Europe, 1996), only juveniles who pose the highest possible risk to society are to receive treatment in a maximum security residential facility. Their treatment measure (a “PIJ-maatregel”; placement in a forensic institution for juveniles) is usually imposed for a minimum of 2 years, and may remain imposed for a maximum period of 6 years. One year of aftercare (care and supervision outside the institution) is also mandatory. A contraindication for placement is an IQ < 70; these youngsters receive treatment in a forensic treatment group for the mentally disabled. For an overview see Table 1.
Main Characteristics of Intensive Specialized Treatments Offered.
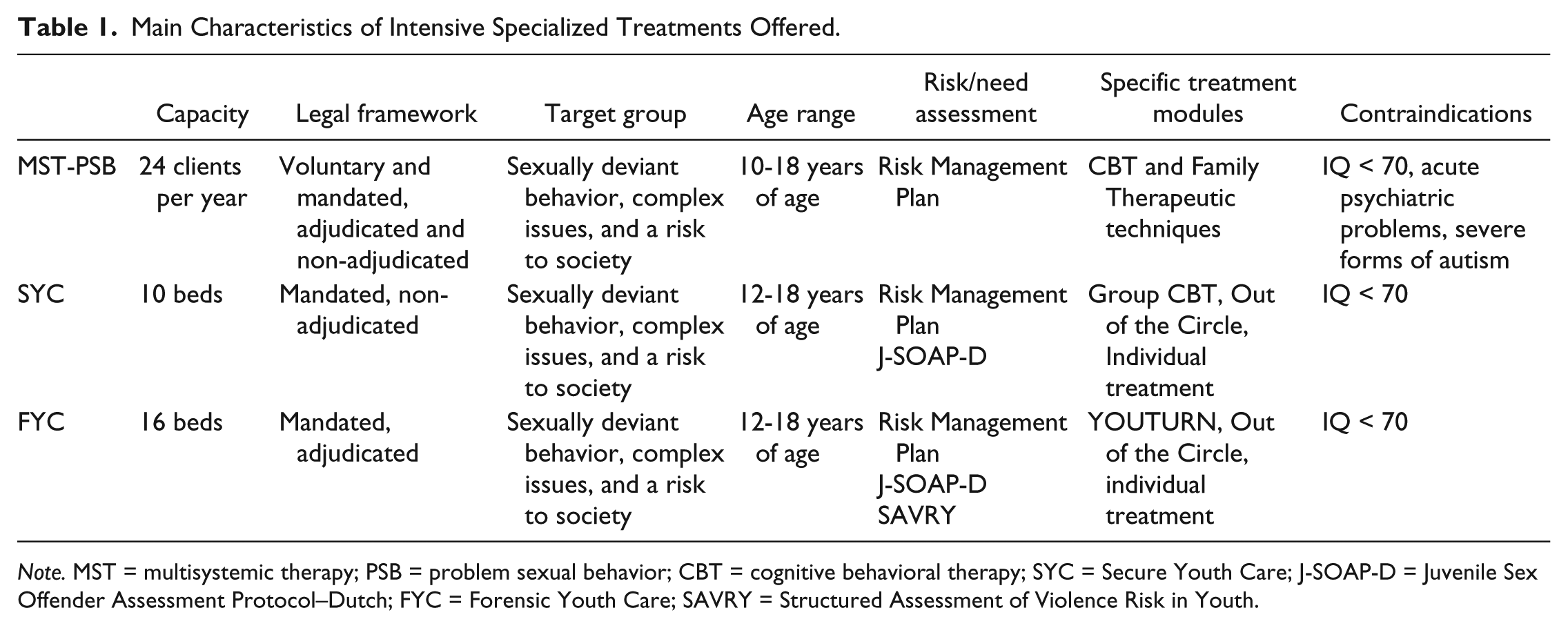
Note. MST = multisystemic therapy; PSB = problem sexual behavior; CBT = cognitive behavioral therapy; SYC = Secure Youth Care; J-SOAP-D = Juvenile Sex Offender Assessment Protocol–Dutch; FYC = Forensic Youth Care; SAVRY = Structured Assessment of Violence Risk in Youth.
Notably, the three intensive treatment options available are all theoretically aimed at a relatively small group of very problematic and “at risk” sexually transgressive juveniles. Clear differentiating indication criteria between the treatment types are lacking.
Evidence-Based Allocation: Literature Review
A well-known and empirically based model for guiding allocation to mandatory treatment is the risk-need-responsivity (RNR) model (Andrews & Bonta, 2010; Andrews, Bonta, & Hoge, 1990; Andrews, Bonta, & Wormith, 2006, 2011; Bonta & Andrews, 2007). The RNR model is built on general personality and cognitive social learning theory. Importantly, it states that treatment allocation should be based on three principles. The first is the risk principle, which matches the level of service to the client’s risk to reoffend (who should be treated). The second is the need principle, which assesses criminogenic needs as to target these in treatment (what should be treated). The third is the responsivity principle, which maximizes a client’s ability to learn from an intervention by providing cognitive behavioral treatment and by tailoring the intervention to the learning style, motivation, abilities, and strengths of the client (how the client should be treated).
The inaccurate matching of treatment intensity with treatment need and risk level has been shown to lead to a waste of resources (Bonta & Andrews, 2007; Cecile & Born, 2009; Hendriks & Bijleveld, 2008). Low risk offenders receiving intensive treatment, especially in residential settings, have even shown an increase in criminal behavior (Bonta, Wallace-Capretta, & Rooney, 2000; Lowenkamp, Latessa, & Holsinger, 2006). Adhering to the RNR model is associated with a reduction of recidivism, whereas non-adherence is associated with increased recidivism or null effects on reoffending (Andrews & Dowden, 2007). As a consequence, the characteristics of treatment should generally match treatment needs and risk levels. As treatment needs and risk levels increase, the intensity of the treatment should increase accordingly. Hanson, Bourgon, Helmus, and Hodgson (2009) have, via meta-analysis, shown the RNR principles to apply to adults and juveniles who have sexually offended. Skeem, Steadman, and Manchak (2015), based on their review of RNR literature, stated that in general, there is a large body of empirical support for the RNR model to be applied to mentally disordered clients in need of treatment.
Evidence-Based Allocation in the Netherlands: Hypotheses
When adhering to the first RNR principle (risk), in the allocation of sexually transgressive juveniles to intensive treatment in the Netherlands, only high at-risk juveniles are expected to receive FYC, for this constitutes mandatory, long-term, intensive, and comprehensive treatment at a maximum security level. At the commencement of FYC treatment, a behavioral specialist and the juvenile perform a comprehensive offense analysis to determine (criminogenic) treatment needs. For risk assessment, tools such as the Juvenile Sex Offender Assessment Protocol–Dutch (J-SOAP-D; Bullens, Van Horn, & Van Eck, 2012) and the Structured Assessment of Violence Risk in Youth (SAVRY; Lodewijks, Doreleijers, de Ruiter, & de Wit-Grouls, 2006) are regularly administered. Promoting the safety of society is a primary directive of FYC; fostering a juvenile’s well-being and health are important secondary goals. Youngsters are notably restricted to a reduced degree and for a shorter period of time in community-based MST-PSB and residential SYC. That said, the freedom restrictions in MST-PSB and SYC are still considerable; both offer 24-hr monitoring, a focus on risk management, and comprehensive protocolled treatment by skilled professionals targeting all areas of development. In MST-PSB, at admission, a risk management plan is made based on the referrer’s, the parents’, and the youngster’s description of the problem behavior and, if present, using the judicial files. Clinical, non-structured, assessment demonstrates which factors constitute a risk. Parents monitor the risk management plan and are addressed as responsible for the safety of their own and other children. They are stimulated to ask and receive support from their informed and activated social network (e.g., extended family, neighborhood), community (e.g., school, local police), and the professional MST-PSB counsellors. In SYC, the J-SOAP-D (Bullens et al., 2012) is scored at admission for risk assessment and treatment planning purposes. In the first period of residential SYC treatment, no leave outside the institution is granted (until a safety plan is in place). Therefore, when adhering to the risk principle, only medium to high risk cases are expected to be allocated to MST-PSB and SYC.
Notably, for the assessment of recidivism risk in juveniles who have sexually offended, two instruments are regarded “state of the art” (Christiansen & Vincent, 2013; Lodewijks & Domburg, 2012). These are the Estimate of Risk of Adolescent Sexual Recidivism (ERASOR; Worling & Curwen, 2001) and the Juvenile Sex Offender Assessment Protocol–II (J-SOAP-II) by Prentky and Righthand (2003). The ERASOR is not used in the Netherlands. The J-SOAP–Dutch version (J-SOAP-D) is a translated and adapted Dutch version of the J-SOAP-II (Bullens et al., 2012). Sexually transgressive adolescents, however, are a relatively small group, and sexual recidivism is rare among them (Caldwell, 2010; Lobanov-Rostovsky, 2015; Mulder, Vermunt, Brand, Bullens, & Van Marle, 2012). Therefore, it is difficult to determine risk factors through research, as larger numbers of reoffenders are needed for robust statistical analysis of predictors. Hempel, Buck, Cima, and Van Marle (2011), in a review of risk assessment instruments for juveniles who have sexually offended, concluded that no one instrument to date has shown unequivocal positive results in predicting future offending. Specialized tools, such as J-SOAP-II, best predict sexual recidivism. Thus, long-term judgments are never to be based solely upon any single risk instrument and the term high risk must be used with caution, for it is a potentially unwarranted and therefore damaging label.
Regarding the need principle, Hanson et al. (2009) defined a criminogenic need as a dynamic risk factor that is theoretically and empirically associated with criminal behavior and can be influenced by means of treatment. In an overview by Worling and Långström (2003), the following empirically supported criminogenic factors for sexual reoffending in adolescents were defined: sexual deviation (e.g., interest in prepubescent children or sexual violence), prior criminal sanctions for sexual assault(s), two or more victims, stranger victimization, lack of intimate peer relationships/social isolation, and incomplete offense-specific treatment. Two further factors were deemed promising: poor relationship with parents and attitudes supportive of sexual offending. Christiansen and Vincent (2013), using a large sample of 39,249 juvenile offenders, of which 695 were juveniles who had offended sexually, recently added prior non-sexual offending, prior sexual offending, hands-off offending, offending against a child, and younger age at time of initial offense as risk factors for sexual reoffending. Some of these factors are static (not to be influenced by therapy).
MST-PSB targets deficits in the adolescent’s cognitive processes (denial, empathy, distortions), family relationships (cohesion, empowering parents, monitoring skills, supervision), peer relationships, and school performance. In SYC, cognitive behavioral–based treatment is offered by youth care professionals, and monitored by a behavioral specialist. Criminogenic treatment needs are assessed and central to therapy. Social learning strategies are explicitly used to stimulate change. Group therapy “Out of the Circle” (Koster & Tel, 2010) is additionally administered, which focuses on the sexual misconduct and on creating an individualized risk management plan with the youngster. The plan is presented by the youngster to his parents/social network, providing insight into the transgressive behavior and its origins. Individual therapy may supplement the group treatment offered. A stay in FYC implies treatment through YOUTURN, a comprehensive, phased, cognitive behavioral–based method (Stuurgroep YOUTURN, 2009) that focuses on all developmental tasks for adolescents (Erikson, 1968). YOUTURN is supplemented with group therapy “Out of the Circle” (Koster & Tel, 2010) and individual therapy. In sum, the dynamic factors, sexual deviation, social isolation, relationship with parents, and attitudes supportive of sexual offending, are described as central elements in FYC, SYC, and MST-PSB treatment, with MST-PSB taking a more holistic approach to all factors mentioned, and focusing primarily on treatment of the family (parental) system. Due to the out-of-home placement of the juvenile, FYC and SYC focus less on parental training; yet, sexual deviation, social isolation, and attitudes of the juvenile are specifically central to the therapy offered.
The responsivity principle comprises two elements: (a) general and (b) specific responsivity. General responsivity calls for the use of cognitive social learning methods to influence behavior. Cognitive social learning strategies are found to be the most effective regardless of the type of offender. Core correctional practices, such as prosocial modeling, the appropriate use of reinforcement and disapproval, and problem solving (Dowden & Andrews, 2004), comprise the specific skills represented in a cognitive social learning approach. Specific responsivity is a fine tuning of the cognitive behavioral intervention. It takes into account the strengths, learning style, personality, motivation, and biosocial (e.g., gender, race) characteristics of the individual. MST-PSB, SYC, and FYC use cognitive social learning–based methods to influence behavior. They also instruct their professionals on how to take into account the individual strengths, learning style, and personality of the youngster being treated (i.e., specific responsivity). In the current study, however, differences in the responsivity of the three treatment forms were not assessed, so no statements on differences in responsivity can be made.
In summary, the three most intensive treatment modalities available in the Netherlands for young sexually transgressive juveniles appear to show an overlap in RNR criteria. First, all three should only be administered to youngsters with a high and specific treatment need. Based on legislation and therapy characteristics, however, some differences in target group are expected. For medium to high risk sexually transgressive youngsters, MST-PSB or SYC treatment seems an adequate choice. Within this group, only those in unsafe living situations may need to be placed in SYC. Finally, only high risk (re)offenders may need to be treated in a maximum security setting (an FYC), as to also protect society.
Study Aim
The current study aims to strengthen the process of allocation to specialized treatment, by a retrospective investigation of the recidivism risk and treatment needs of the current target groups of (intensive) contextual and residential treatments. Currently, the differences and similarities between the various intensive treatment populations are unknown, as is the degree to which mandatory treatment allocation follows RNR principles. This study aims to further illuminate these areas and provide guidelines for future allocation practices.
Method
Participants
Case file information was coded for 86 adolescent boys (MST-PSB: N = 25; SYC: N = 29; FYC: N = 32). This group constituted all juveniles (no girls, IQ = 70) admitted to intensive specialized treatment in the Netherlands between January 2010 and April 2012. This study, thus, investigated the total Dutch population of sexually transgressive juveniles allocated to intensive specialized treatment. The majority of the boys were of Dutch origin (77%) and their mean age was 14.8 years (SD = 2.1 years) at the start of treatment. Table 2 provides an overview of background characteristics.
Overview of Background Characteristics.
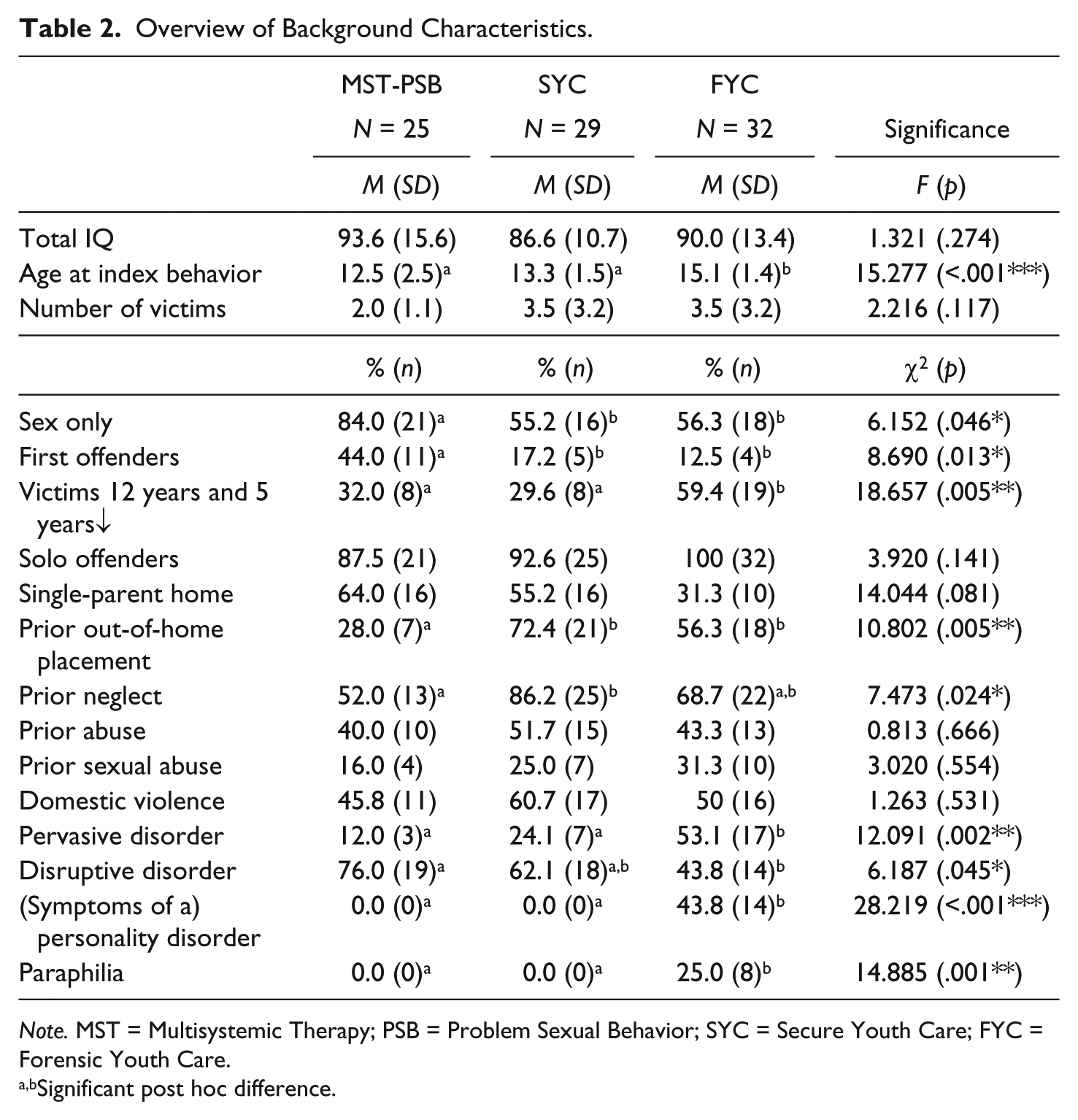
Note. MST = Multisystemic Therapy; PSB = Problem Sexual Behavior; SYC = Secure Youth Care; FYC = Forensic Youth Care.
Significant post hoc difference.
Treatment Forms
MST-PSB is provided by de Viersprong treatment center in the southern region of the Netherlands. Mean treatment duration of the MST-PSB group examined in this study was 7 months (SD =1.1 months, range = 3-8 months).
SYC treatment for sexually transgressive youth is provided by Horizon, center for youth care and education. Mean stay in the SYC group examined in this study, including aftercare, was 22 months (SD = 10.3 months, range = 1-53 months).
There are two specialized FYC treatment groups for sexually transgressive behavior in the Netherlands, both at the Den Hey-Acker state institution for juveniles. Mean stay of the FYC group examined in this study, including aftercare, was 47 months (SD = 14.8 months, range = 7-69 months).
Instruments
Due to the availability of a validated Dutch version, the J-SOAP–Dutch version (J-SOAP-D) (Bullens et al., 2012) was selected as the instrument to be used in the assessment of treatment need and risk levels in this study. The J-SOAP-D was designed to be used with boys aged 12 to 18 years who had been adjudicated for sexual offenses, as well as non-adjudicated youths with a history of sexually coercive behavior. Prentky and colleagues (2010) also established the use of the J-SOAP-II as valid for pre-adolescents with a high risk of reoffending. Its items were generated from an extensive review of risk factor literature (Prentky & Righthand, 2003). The J-SOAP-D consists of two static criminogenic need scales and two dynamic criminogenic need scales, which are used to estimate the level of recidivism risk. The scale items are scored on a 3-point scale according to the instruction manual, after which an average score per scale is calculated (ranging from 0 to 1). Scale 1 measures sexual drive and preoccupation (i.e., previous sex offenses, number of victims, duration of sex offense history, and sexual victimization history). Scale 2 measures impulsive and antisocial behavior (i.e., caregiver consistency, school behavior problems, previous arrests, and history of physical assault/exposure to domestic violence). Scale 3 measures intervention items (i.e., accepting responsibility, internal motivation for change, empathy, shame and guilt, and cognitive distortions). Finally, Scale 4 measures community stability and adjustment (i.e., management of sexual urges and desires, stability of living situation, stability in school, and a positive support system). A complete overview of the scales, items, and scoring criteria is available in the J-SOAP-D manual (Bullens et al., 2012). Recidivism risk is classified in two ways, namely, sexual recidivism risk and general recidivism risk, which are coded as low, medium, or high.
Research on the reliability of the J-SOAP-II shows a good to excellent interrater reliability, ranging from .75 to .91, with an average of .83 (Prentky & Righthand, 2003). Validity outcomes (Elkovitch, Viljoen, Scalora, & Ullman, 2008; Hecker, Scoular, Righthand, & Nangle, 2002; Martinez, Flores, & Rosenfeld, 2007; Powers-Sawyer & Miner, 2009; Prentky et al., 2010; Rajlic & Gretton, 2010; Viljoen et al., 2008) however, vary. An area under the curve (AUC) value of .50 indicates that an estimate is considered equal to chance (i.e., flipping a coin is considered as accurate as using the instrument). A value between .70 and .75 is considered moderate; a value greater than .75 to .80 is considered good (Fawcett, 2006). The J-SOAP AUC values measured for general recidivism (all types of reoffending) range from .53 (Elkovitch et al., 2008) to .76 (Martinez et al., 2007). J-SOAP AUC values measured for sexual recidivism range from .44 (Elkovitch et al., 2008) to .83 (Prentky et al., 2010). Therefore, the validity of the J-SOAP-D is considered to be restricted.
Procedure
The study complied with the American Psychological Association (APA) ethical principles regarding research with human participants. Permission for the retrospective case file research performed was granted by the Dutch Ministry of Justice and the participating organizations. All boys receiving treatment via one of the included treatment forms from January 2010 (when all three types of treatment were operational) until April 2012 (when case files were scored) were included. Case files contained referral information (including psychodiagnostic evaluations), treatment reports, and judicial documents on criminal history. A broad range of items was coded by a single assessor. Special attention was given to diagnostic history, treatment history, and offense history, as well as to protective and risk factors. All items were operationalized in a codebook and the majority concerned factual information; therefore, little interpretation of data was required. Nevertheless, seven files were scored by a second assessor to establish inter-coder reliability through the use of intra-class correlation (ICC). Following the guidelines by Shrout (1989), single ICCs were calculated for the two-way random effects model, with absolute agreement as a criterion. The single ICC provides information about the reliability of the risk assessment performed by a single evaluator. Critical ICC values are defined as follows: ICC ≥ .81 = substantial, .60 ≤ ICC ≤ .80 = moderate, .41 ≤ ICC ≤ .60 = fair, ICC ≤ .40 = slight (Shrout, 1989). In the scoring of case files, single measures showed an ICC of .99 (i.e., substantial reliability).
As a J-SOAP-D was not available for all youths, J-SOAP-D questionnaires were completed retrospectively by a trained assessor, based on the case file information available at admission. 1 Twenty cases (23% of the total sample) were scored by a second trained assessor as to establish interrater reliability. Calculation of single measures for the J-SOAP set yielded an ICC of .71 (i.e., moderate reliability). One case file was excluded from the study due to insufficient information. This case did not substantially differ from the other cases.
Statistical Analyses
All statistical analyses were performed using IBM SPSS version 22.
To analyze group differences on the four treatment need scales, a one-way ANOVA procedure and Bonferroni post hoc analyses with a two-tailed probability level of <.05 was used. We tested the differences in mean score (the higher this score, the more problematic youngsters on average are perceived to be). No standardization of J-SOAP-D treatment need scores is available, so no statements about a low, medium, or high treatment need measured is possible. Dunnet’s one-tailed post hoc analysis was used for the community stability scale, because MST-PSB clients were expected to show relatively lower (less problematic) scores than SYC or FYC clients on this scale.
To compare the estimated sexual and general recidivism risk of the three treatment groups, chi-square tests with a two-tailed probability level of <.05 were performed. Percentages of low, medium, and high at recidivism risk cases in each of the treatment programs were calculated and compared, expecting an even distribution between MST-PSB and SYC and relatively more high at-risk youngsters in FYC.
As to assess the clinical relevance of differences found, Cohen’s d was calculated, using the calculator of Wilson (2013) and formulas of Lipsey and Wilson (2001). Effect sizes in terms of Cohen’s d are considered small (.10-.30), medium (.31-.50), or large (≥.51; Cohen, 1992). The power of the analysis was also assessed, and showed the sample size to be too small to detect medium size effects, at p = .05 and power = .80, requiring a total of 133 participants, more or less equally distributed across categories. Thus, using the current population, even when they represent the total population in a period of 2 years, small, but possibly clinically relevant, effect sizes could not be detected. Therefore, effect sizes that just failed to reach significance (trends, p < .1) were reported.
Results
Although Table 3 (pre-treatment comparison of treatment needs) shows that comparison of sexual drive scores failed to reach significance, it did show a trend toward a difference between the groups. Post hoc analyses revealed a trend toward MST-PSB clients scoring as less problematic than FYC clients (p = .056, Cohen’s d = .66). On the impulsive/antisocial scale, SYC clients scored highest (most problematic). MST-PSB clients scored least problematic on these items. Post hoc analyses confirmed that MST-PSB youngsters scored significantly less antisocial than did SYC youngsters (p = .015, Cohen’s d = .78).
Comparison of Criminogenic Treatment Needs/J-SOAP-D Scale Scores.
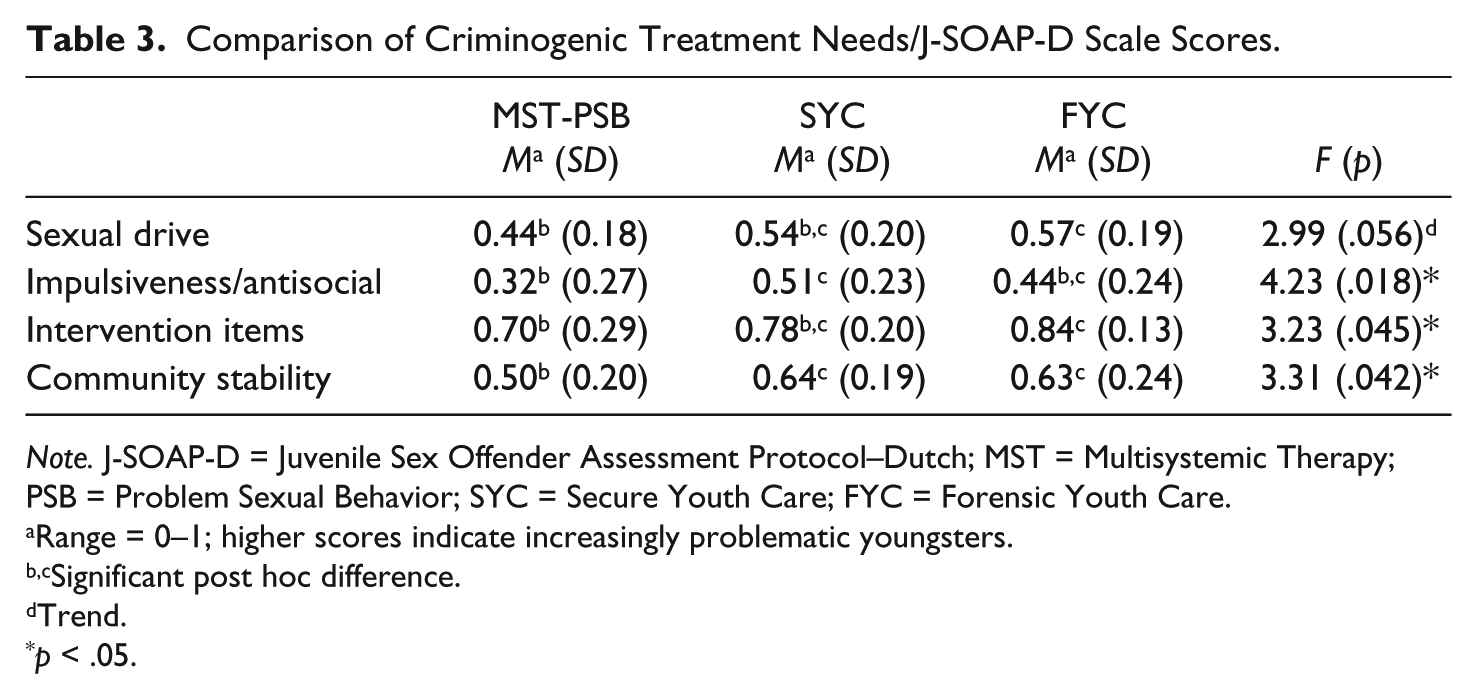
Note. J-SOAP-D = Juvenile Sex Offender Assessment Protocol–Dutch; MST = Multisystemic Therapy; PSB = Problem Sexual Behavior; SYC = Secure Youth Care; FYC = Forensic Youth Care.
Range = 0–1; higher scores indicate increasingly problematic youngsters.
Significant post hoc difference.
Trend.
p < .05.
On intervention items, FYC clients scored most problematic, whereas MST-PSB clients scored least problematic. Post hoc analyses confirmed that MST-PSB youngsters scored significantly higher on problem insight and motivation than did FYC youngsters (p = .039, Cohen’s d = .67). Regarding community stability, MST-PSB clients scored the lowest, which indicates a higher stability. Post hoc analyses showed that MST-PSB clients scored significantly lower than SYC and FYC clients (p = .021 and p = .028; Cohen’s d = .69 and .56, respectively).
As Table 4 (pre-treatment comparison of estimated recidivism risk) shows, the assessed sexual recidivism risk did not differentiate between the three treatment groups. There was a trend indicating that youngsters with low sexual recidivism risk received MST-PSB more often than FYC (p = .087, Cohen’s d = .32).
Comparison of Estimated Recidivism Risk/J-SOAP-D Scores.
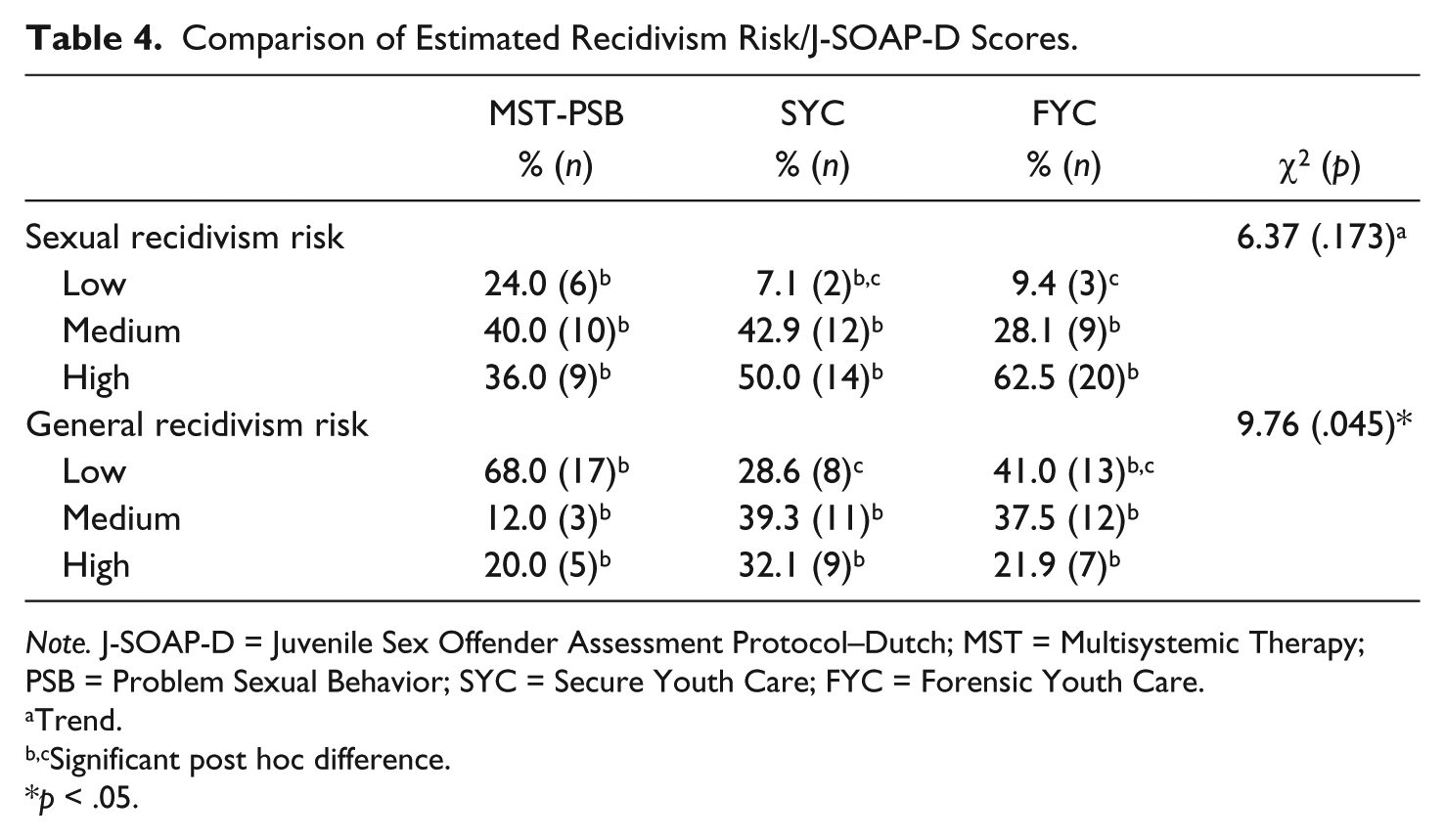
Note. J-SOAP-D = Juvenile Sex Offender Assessment Protocol–Dutch; MST = Multisystemic Therapy; PSB = Problem Sexual Behavior; SYC = Secure Youth Care; FYC = Forensic Youth Care.
Trend.
Significant post hoc difference.
p < .05.
General recidivism risk showed a significant differentiation (p = .045). Low at general recidivism risk youngsters were treated more often by MST-PSB than by SYC (Cohen’s d = .68).
Taking into account the substantial medium to large Cohen’s ds that were found, all results, including trends, were deemed clinically relevant (Dunst, Hamby, & Trivette, 2004).
Discussion
The aim of this study was to assess the recidivism risk and criminogenic treatment needs of sexually transgressive juveniles treated by MST-PSB, SYC, or FYC in the Netherlands, to ascertain whether treatment allocation was performed in accordance with RNR principles. All three treatment modalities are aimed at juveniles with complex issues and show similar allocation criteria. However, two distinctive allocation processes are in use to allocate sexually transgressive juveniles to treatment. In both pathways (civil law or criminal justice) an evaluation of treatment needs and risks is performed, but different professionals use different assessment techniques (non-structured clinical to actuarial). Notably, the (severity of) problem behavior does not differentiate between pathways. The response of people surrounding the youth or the decision whether or not to prosecute a case does (see Figure 1). Only youngsters in need of specialized treatment (i.e., a moderate to high criminogenic treatment needs score on the J-SOAP-D) were expected to receive MST-PSB, SYC, or FYC. Juveniles deemed unsuitable for outpatient treatment (high score on community (in)stability) and assessed at medium to high recidivism risk were expected to receive SYC. Only youngsters assessed at “high risk” for recidivism were expected to receive treatment in an FYC. To test the hypotheses, the J-SOAP-D scale scores (criminogenic treatment need) and the assessed recidivism risk were compared.
The comparison of treatment needs, as based on the J-SOAP-D scale scores, revealed a number of differences. MST-PSB clients showed a reduced treatment need in comparison with FYC or SYC clients. MST-PSB clients particularly scored less problematic than FYC and SYC clients on impulsive and antisocial behavior (i.e., caregiver consistency, school behavior problems, previous arrests, and history of physical assault/exposure to domestic violence), intervention items (i.e., accepting responsibility, internal motivation for change, empathy, shame and guilt, and cognitive distortions), and community stability and adjustment items (i.e., management of sexual urges and desires, stability of living situation, stability in school, and positive support system). On sexual drive and preoccupation (i.e., previous sex offenses, number of victims, duration of sex offense history, and sexual victimization history), a trend was found for MST-PSB clients to score less problematic than FYC clients. Because there are no cutoff scores available for the criminogenic needs scale, it was not possible to determine whether scores of MST-PSB clients should be considered “low” and the clients, therefore, were not in need of specialized treatment. Regarding the etiology of the sexual problem behavior, the clients of intensive specialized treatment in the Netherlands seem more “generalist/antisocial” in SYC, and more “sexually deviant” in FYC, underscoring the viability of both typologies for sexually transgressive juveniles.
On their assessed recidivism risk, groups also differed at the time of allocation. More youngsters with an estimated low recidivism risk were referred to MST-PSB. Transgressive youth with a more “generalist” pattern of offending (multiple type of rule breaking) generally tend to reoffend sooner and at an increased rate, sexually as well as violently (Chu & Thomas, 2010; Drew, 2013; Hissel et al., 2006; Parks & Bard, 2006), so a target group at greater recidivism risk appears to be treated in SYC and FYC. In FYC, however, only youngsters assessed as “high at sexual recidivism risk” were expected to be treated. Based on this premise, 38% (low and medium at sexual recidivism risk) of FYC youngsters still seem to have received a too restrictive type of treatment. Seven percent of the juveniles in SYC, and 24% in MST-PSB, were assessed to be at low sexual recidivism risk, whereas only medium to high at sexual recidivism risk youth were expected to be treated here. Therefore, if estimated sexual recidivism risk is perceived a valid indicator for receiving intensive specialized treatment, 38% of the juveniles in FYC, 7% in SYC, and 24% in MST-PSB appear to have been misallocated.
In sum, youth referred to MST-PSB seem less problematic (i.e., on treatment needs and estimated recidivism risk levels) than youth referred to SYC and FYC. Low at recidivism risk youth are not in need of specialized intensive treatment and may even suffer adverse effects if allocated as such. Therefore, both referrers and MST-PSB providers should more stringently adhere to admission criteria and only refer youngsters with more (specific) treatment needs, and consequently, a higher (sexual) recidivism risk.
The populations of SYC and FYC seem to better “fit” the treatment objectives of an intensive treatment form (they show a relatively high treatment need). However, their risk levels did also not always support the need for risk reduction by (long-term) limitation in freedom of movement and maximum supervision offered.
Thus, the current allocation process used, despite the use of professional judgment of risks and needs, may lead to poor allocation decisions. As a result, youth may have received treatment that is too restrictive or intensive, which may in turn have adverse effects on development, behavior, and motivation (Bonta & Andrews, 2007; Bonta et al., 2000; Cecile & Born, 2009; de Valk, Kuiper, van der Helm, Maas, & Stams, 2016; Hendriks & Bijleveld, 2008). Taking into account the low prevalence of actual sexual recidivism (7%-13% after 59 months at risk), and very low rates of persistence of sexual offending into adulthood by adolescents (Lobanov-Rostovsky, 2015; Lussier et al., 2012), these are consequences to be taken very seriously.
Allocation to treatment of sexually transgressive juveniles is to be based on specific knowledge, so the authors deem it important that a structured assessment of treatment needs and recidivism risk is administered and given more weight in the allocation to mandatory forms of treatment. The validity of the J-SOAP-D is restricted, but, in the Netherlands, currently “as good as it gets” for treatment allocation purposes based on RNR principles; actuarial assessment certainly outperforms clinical judgments (Dawes, Faust, & Meehl, 1989; Hanson & Morton-Bourgon, 2009). Because of the restricted validity in predicting (sexual) recidivism, a focus on the assessed treatment needs (i.e., etiology or typology), might provide the most valid base for treatment allocation purposes.
For example, the practical implications of the assessed background characteristics (e.g., highest age, more prepubescent victims, more paraphilia, pervasive and personality disorders) and treatment needs (relatively high scores on sexual drive, intervention items, and community instability) in FYC appear to be that stimulating moral development and learning to cope with a deviant sexual interest should be specific targets. Lord (2016) recently reviewed literature regarding the treatment of mentally disordered sexual offenders (a target group similar to the one here identified in FYC) and strongly advocated the combined use of the RNR and the Good Lives model (GLM; Collie, Ward, Ayland, & West, 2007) principles, as mentally disordered sexual offenders are especially in need of an emphasis on approach goals, enhanced responsivity, and skills acquisition. GLM is a therapy model that focuses beyond risks and needs on creating meaning and life fulfillment. It has recently been suggested that the GLM, therefore, may more effectively motivate people to make a difficult change, as the change advocated is (also) meaningful to themselves, in contrast to making a change for which society’s reward is non-persecution (Andrews et al., 2011; Ward, Yates, & Willis, 2012).
In contrast, the practical implications of background characteristics (e.g., more neglect, prior out of home placements, and disruptive disorders) and treatment needs assessed in SYC (relatively high scores on impulsive/antisocial behavior and community instability) may be that their program should focus less specifically on deviant sexual behavior and attitudes, and more on a broader set of (generalist) criminogenic needs. Improving personal adjustment (taking classes/qualifying for employment, anger management, and social skills training) and building (new) social networks could be key elements for effective treatment. The latter especially may currently receive too little attention in the specialist treatment offered by SYC.
Limitations
Some aspects of this study merit further reflection. First, this study was limited by restrictions in the validity of the instrument used (J-SOAP-D). Insufficient research is available into the prediction of sexual recidivism by adolescents. Further research into the field of relapse into sexual transgressions by youth is needed to obtain a fuller understanding of which youngsters persist and which desist. Second, the J-SOAP was retrospectively coded based on case file information, which could have restricted our knowledge of the cases. Allocation, however, usually takes place based on case file information, and case files were extensive. Both assessors of the J-SOAP-D were affiliated with one of the treatment modalities (SYC). Therefore, files were coded blind, and it was ensured that the coders had never had any therapeutic contact with the subjects coded, restricting the knowledge of the coders regarding the clients to the case files presented. Third, the sample on which the research was performed was small (although it contained all participants from a period of 2 years). This meant that some analyses were underpowered. Fourth, at the time of the study, MST-PSB had only recently been implemented as a new treatment in the Netherlands. This may have influenced allocation due to an unfamiliarity with the treatment and its referral criteria. In addition, it may have influenced the acceptance of less problematic cases for MST-PSB treatment due to an insufficient number of referrals. Finally, allocation results have been studied in the Netherlands, where a broad spectrum of possible responses to sexually transgressive behavior by adolescents (from criminal prosecution to voluntary enrolment in treatment) is available. In other countries (e.g., Belgium), the criminal prosecution of youths does not exist, and, in contrast, in some states of the United States, a firm judicial response (lifetime registration) of all types of sexual misbehavior, including that by adolescents, is common practice. In light of this, the results of this study should be interpreted with caution, as transferability may be limited by contextual differences. The administration of mandated specialized residential or community-based therapy, however, is general practice. Therefore, the results of this study may very well prove useful in any situation in which allocation to community-based versus residential treatment, based on RNR principles, occurs.
Conclusion
Allocation of sexually transgressive juveniles to treatment is a complex task. Juveniles assessed as low at (sexual) recidivism risk are not in need of intensive treatment, and may even suffer adverse effects if allocated as such. For juveniles assessed as medium to high at recidivism risk, with a high community stability, an out-of-home placement can be avoided by allocation to intensive specialized community-based treatment. Only juveniles in unsafe living situations may need to be placed out of home, and only assessed as high at-risk sexually (re)offensive juveniles may need to be treated in a maximum security setting, as to protect society. At the same time, while allocating youth, it is important to keep in mind that assessment of sexual recidivism risk in juveniles might sooner overestimate, than underestimate real risks, because sexual recidivism is rare and most juvenile sexual transgressions remain adolescence limited.
Therefore, to improve the current allocation process, a structured (actuarial) assessment of treatment needs (i.e., etiology) of sexually transgressive juveniles should, in the opinion of the authors, be administered prior to allocation to specialized mandatory forms of treatment. Broad usage of one instrument might contribute to a more matched care for all sexually transgressive juveniles, whichever allocation pathway they follow.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.