
Abstract
High levels of depression have been found among incarcerated youth, which suggests that mental health problems are associated with delinquent behavior and are part of a constellation of risk factors that contribute to youth entering the juvenile justice system. In this project, we investigated trauma and mental health issues among male youth in residential treatment, and addressed the following questions: (a) Does childhood trauma predict current depression for male juvenile sexual offenders? (b) If so, do different types of traumas predict depressive affect better than others? and, (c) Does extent of trauma exposure predict depression? Data on incarcerated male juvenile sexual offenders were analyzed (n = 379). Multiple regressions of various types of traumas and cumulative trauma and depression were conducted. Emotional abuse was the strongest predictor of depressive affect for this sample, and multiple exposures to trauma were the second strongest predictor.
Introduction
Male juvenile delinquency is a social problem that affects adolescents, their families, and their communities psychologically, socially, and economically. The Office of Juvenile Justice and Delinquency Prevention (OJJDP) researchers report that between 20% and 30% of all violent victimizations involve a juvenile offender, a number that has remained stable over the past 40 years (OJJDP, 2011). In 2006, almost 20% of people arrested for violent crimes toward others were below the age of 18, and adolescent boys represented 83% of the juvenile arrests for these crimes (Snyder & Sickmund, 2006). In 2008, nearly 1.7 million delinquency cases were processed in juvenile courts across the country (Sickmund, Sladky, Kang, & Puzzanchera, 2011), and many of these cases resulted in incarceration in correctional facilities or residential programs. These programs are often expensive to run, and can be overly restrictive and punitive while failing to achieve the goal of decreased criminal behavior (Mendel, 2011).
Researchers have found that children who experience abuse and neglect are significantly more likely to commit crime and become incarcerated than those who are not (Child Welfare Information Gateway, 2006; Wilson, Stover, & Berkowitz, 2009). These same researchers report that children who have experienced abuse or neglect are 59% more likely to be arrested as a juvenile, 28% more likely to be arrested as an adult, and 30% more likely to commit a violent crime (Child Welfare Information Gateway, 2006).
Common risk and resiliency factors have been associated with delinquency across race, gender, and socio-economic status. Specifically, early victimization experiences and subsequent traumatic sequelae, including affective states (the focus of this study), have been identified as significant risk factors warranting further and more complex investigation (Becker, Kaplan, Tenke, & Tartaglini, 1991; Finkelhor, Ormrod, Turner, & Hamby, 2005; Mrug & Windle, 2010). Research on risk factors, considered individually or in combination, contributes to an understanding of effective prevention and intervention efforts.
Childhood Trauma
Relevant to the current study, the literature on cumulative trauma categorizes childhood traumatic experiences as broad categories: sexual abuse, physical abuse, emotional abuse, physical neglect, emotional neglect, and general exposure to violence. These types of traumatic experiences individually and cumulatively have been found to contribute to a variety of negative psychological and behavioral outcomes, including depression (Finkelhor et al., 2005; Harrell, 2007; Mrug & Windle, 2010). Furthermore, depression has been identified as one of the leading causes of suicide, unexpected death, and disability in the United States among adolescents and adults (Kessler et al., 2003; McKenna, Michaud, Murray, & Marks, 2005; Thapar, Collishaw, Pine, & Thapar, 2012), which underscores the importance of investigating depression as an outcome of post-traumatic stress (Collishaw et al., 2007; Wingo et al., 2010). However, despite this body of literature, there is limited research on the link between early childhood traumatic experiences and depression in adolescent males. Given that adolescent males represent the majority of juvenile delinquency cases, understanding the role depression may play in a male adolescent’s reaction to developmental trauma may also contribute to a greater understanding of the possible contribution of depression to the trauma-to-delinquency trajectory (Jencks & Burton, 2013).
As high as 80% of adolescent male sexual offenders report experiencing childhood sexual abuse (CSA; Burton, 2003; Weeks & Widom, 1998). CSA has been correlated with increased anxiety, depression, and post-traumatic stress disorder (PTSD) symptoms in adolescents (Briere & Elliott, 2003; Danielson et al., 2010; Kendall-Tackett, Williams, & Finkelhor, 1993), as well as with many other impairing psychological issues. More recent research conducted by Danielson and colleagues (2010) found that 26% of their sample of sexually abused adolescents (n = 269) experienced a lifetime course of PTSD, 36% reported a lifetime course of major depression, and 80% reported symptoms of both disorders. CSA has also been correlated with subsequent sexual offending (Jesperson, Lalumière, & Seto, 2009), although one researcher suggested that it may be more of a “marker” than a validated risk factor (Mallie, Viljoen, Mordell, Spice, & Roesch, 2011).
Since the late 1980s, researchers have reported that child physical abuse may predict aggressive behavior during adolescence (Widom, 1989). This finding has been corroborated in similar research over the past few decades (e.g., Benda & Corwyn, 2002; Briere & Elliott, 2003). However, understanding and comparing the findings of this body of research are difficult because of the diversity of the methodology, research settings, and the characteristics of the participants, as well as a lack of differentiation among different forms of trauma. For example, Widom’s work has been critiqued for only using data regarding children involved with social service agencies, as that population is more likely to have exposed to greater interpersonal victimization and violence and they receive state services (Lahey & Waldman, 2003). Widom reported that an abused or neglected male child has a 1.76 times greater likelihood of being arrested as an adult male. However, all forms of abuse and neglect were assessed collectively, which may diminish the applicability and sensitivity of her findings.
Emotional abuse is challenging to assess, measure, and substantiate by child protective services, but occurs and is underreported (Iwaniec, 2006). It is also “almost always present” when other forms of abuse are identified (Child Welfare Information Gateway, 2008), and may be considered one of the most pervasive and destructive forms of abuse (Barnett, Miller-Perrin, & Perrin, 2005; Bingelli, Hart, & Brassard, 2001). In regard to sexually abusive behavior, it has also been linked to deviant sexual behaviors among adolescent males (Fleming, Jory, & Burton, 2002).
Physical and emotional neglect rates among juvenile delinquents involved with the Juvenile Justice Department have been reported at approximately 75% (OJJDP, 2011), making it among the most common forms of child maltreatment within this population. However, they are less researched forms of child maltreatment (Powers, Ressler, & Bradley, 2009). The negative impact of neglect on children and adolescents is well documented, but here again, due to differences in definitions of neglect, as well as differences in sample sizes and characteristics, findings do not generalize broadly to victimized youth (McSherry, 2007). Measurement of neglect is also challenging because it represents an absence of care, as opposed to a presence of a negative behavior as is the case with physical or sexual abuse (English, Thompson, Graham, & Briggs, 2005). Researchers have proposed that neglect and poverty have a reciprocal, circular, and interdependent relationship, and that while neglect should be responded to quickly and adequately as a childhood trauma, it should not be associated with only a single causal factor (McSherry, Iwaniec, & Larkin, 2004).
Childhood exposure to violence has been researched within individual exposure types, such as domestic violence and community violence, yet few researchers have analyzed its impact when there are multiple types of trauma exposures. These researchers have also not often taken into account the number of exposures and other individual factors that could influence the psychological impact of exposure, such as proximity to and severity of the event, child’s gender and age, the chronicity of the exposure, the relationship the child had with the victim and perpetrator, and whether other stressors were also occurring at the time of the abuse (Kracke & Hahn, 2008).
Information about children’s exposure to violence within their home, school, and community environments from birth to age 17 was provided by the authors of the National Survey of Children’s Exposure to Violence (Finkelhor et al., 2005). The survey (n = 2,030) was unique in that it gathered information from a general population versus referral-based children, and the researchers found that a significant number of children were exposed to violence in their everyday lives, with more than 60% of the sample being victimized in the year prior to completing the survey (Finkelhor, 2008).
Impact of Poly-Victimization and Cumulative Trauma
Complex trauma experiences among juvenile justice involved youth are linked to sexual and non-sexual behavior problems and delinquency (Ford, Chapman, Connor, & Cruise, 2012; Marini, Leibowitz, Burton, & Stickle, 2013). More than 90% of youth in the juvenile justice system reported having experienced at least one traumatic event (Arroyo, 2001), and youthful offenders in the prison system in the United States have experienced cumulative life course trauma, a potential pathway to delinquency. Evidence for the trauma–delinquency link was also found among youth adjudicated for sexual offenses (Burton, Leibowitz, Eldredge, Ryan, & Compton, 2011). Complex trauma includes sexual and physical abuse and neglect, and is associated with sequelae that include a range of emotional and behavioral impairments in core competencies related to attachment, self-regulation, executive functioning, conduct, and psychiatric concerns (Cook et al., 2005).
Prior research has tested the multiple pathways linking trauma and delinquency in a nationally representative sample of youth with the finding in one study that internalizing symptoms such as negative affect resulting from trauma mediate this link (e.g., Maschi, Bradley, & Morgen, 2008). Delisi et al. (2010) tested the associations between childhood maltreatment, early exposure to violence, and subsequent delinquency, and found evidence that trauma resulting from maltreatment was related to misconduct and other outcomes such as suicidality among incarcerated youth.
Researchers have found that cumulative trauma or multiple (re)victimizations and poly-victimization are common among general population–based adolescents, with 38.7% having experienced two or more victimizations in the previous year, and 10.9% having experienced five or more direct victimizations in the past year (Finkelhor et al., 2005). In a major national research project assessing exposure to violence and victimization rates for children aged 0 to 18, Finkelhor, Turner, Ormrod, and Hamby (2009) found that 60.6% of their population-based sample (n = 4,549) had experienced or witnessed violence in the prior year. Exposure in multiple contexts (e.g., home, neighborhood, and school) was also common for this sample, and exposure to one type of trauma/victimization doubled or tripled the youth’s likelihood of being exposed to another type (Finkelhor et al., 2009). Witnessing violence and victimization have both been found to predict delinquency and aggressive behavior in adolescent males (Weaver, Barkowski, & Whitman, 2008), and their rates of exposure to violence and exposure to victimization of others have been found to be between 50% and 68% (Macmillan & Hagan, 2004; Menard, 2002).
Analyses of data on early trauma exposure collected from a large, non-referred sample of children aged 9 to 13 (n = 1,420) indicate that over two thirds of the youth reported experiencing at least one traumatic event by the age of 16 (Copeland, Keeler, Angold, & Costello, 2007). Of these youth, approximately 15% experienced three or more traumatic events, which puts them at higher risk of psychiatric disorder (mainly anxiety and depression) and poor outcomes in adulthood (Copeland, Miller-Johnson, Keeler, Angold, & Costello, 2007), such as persistent mental illness and criminal justice involvement.
Other investigations with child and adolescent samples found that lifetime and childhood cumulative trauma contributed to the increased severity of mental health symptomology in youth (Cloitre et al., 2009). Cloitre and colleagues found that childhood cumulative trauma was associated with symptom complexity in a “rule-governed way,” and it significantly influenced whether the symptoms persisted into adulthood.
While a relationship between early traumatic experience and depression for male adolescents has been explored by prior researchers to a certain extent (Beyers & Loeber, 2003; Capaldi & Stoolmiller, 1999; Chen & Simons-Morton, 2009; Drabick, Gadow, & Sprafkin, 2006), there is a knowledge gap regarding the effects of different types of traumas and the impact of cumulative traumatic experiences on emotional and behavioral functioning among sexually abusive youth.
A meta-analysis of 31 studies investigating sexual abuse history in juvenile sex offenders (JSOs), the vast majority of studies found that adolescent sex offenders had experienced greater sexual victimization compared with non-sexual offenders (more than 5 times greater), and sexually abusive youth had a higher prevalence of physical abuse compared with their counterparts (59% vs. 49%; Seto & Lalumière, 2010). Relevant to testing the trauma–delinquency association, Leibowitz, Burton, and Howard (2012) compared sexually victimized and non-sexually victimized adolescent sexual abusers with a group of non-sexually victimized delinquent youth (N = 478). Findings included that the sexually victimized sexual abusers had the highest mean scores on trauma and personality measures, followed by non-sexually victimized sexual offenders and general delinquent youth. Understanding the role of adverse environments and traumatic sequelae in subsequent offending and juvenile justice involvement, as well as the relative effects of different types of abuse on mental health outcomes, is critical to effective management, assessment, and treatment strategies.
Adolescent Depression and Mental Health Outcomes
Research with community samples of adolescents indicates that between 1.8% and 8.0% met the criteria for depression (Angold & Costello, 1993; Substance Abuse and Mental Health Services Administration, 2008), and higher levels of depression have been found among incarcerated youth. Researchers in one study reported that of approximately 1,000 incarcerated adolescents, 25% were moderately depressed and 22% were severely depressed (Domalanta, Risser, Roberts, & Risser, 2003). These researchers also reported that 60% of their sample had one or more psychiatric disorders. Becker and colleagues (1991) investigated depressive symptomatology with male juvenile sexual offenders with trauma histories, and found that 41.9% (n = 246) met criteria for major depression and that childhood physical or sexual abuse was linked to higher scores on the depressive measure. High levels of anxiety and depression among incarcerated youth suggest a correlation between their mental health and delinquent behavior that resulted in juvenile justice involvement.
The current research project investigated whether childhood trauma predicted current depression for male juvenile sexual offenders, and whether different types of traumas predicted depressive affect better than others. In addition, the current study investigated whether the extent of traumatic exposure predicted depression in youth with sexually harmful behavior.
Method
The impact of different rates of depression among JSOs has been minimally investigated. Methodological considerations for the current study included a review of this research, for example, Becker’s (1991) investigation of the rates of depression among JSOs, especially those that reported being physically or sexually abused in childhood. The overall sample of JSOs’ (n = 246) mean score on the Beck Depression Inventory indicated mild depression (14.3), with abused participants scoring 4.1 points over non-abused participants (16.4 vs. 12.3). Research is needed on the relationship between types of childhood traumas, cumulative trauma, and depression, especially as they relate to sexually abusive behavior. The current study is a further investigation of the relationship between trauma, poly-victimization, and depression. As noted previously, the JSO population has higher rates of childhood traumatic exposure (e.g., Becker, 1991; Burton, 2003; Burton, Duty, & Leibowitz, 2011), and the current study builds on this research using a large sample of juvenile justice involved youth.
Participants
The data combine three datasets of incarcerated residentially based sexually abusive youth from two states (n = 574 youth). Group 1 data were collected from a Midwest state in 2004, Group 2 data from the same Midwestern state in 2009, and Group 3 data from an eastern state in 2009. The data collected from Groups 1 and 2 were confidential, and Group 3 data were anonymous. In total, youth from 18 facilities and two states were queried.
Fifty-four percent of this sample endorsed living with two adults; either mother and father, mother and a partner, or father and a partner. Twenty-five percent endorsed living alone with their mother, 3% endorsed living alone with their father, and 14.5% reported living out of their home. Twenty-two percent of this sample endorsed being “very poor,” while 73% reported being “not very poor” when asked if they were very poor growing up. All participants were incarcerated for sexual crimes at the time of data collection, although specific information about types of crimes was unavailable.
Total sample size was decreased due to invalid responding. Using the social desirability and valid response rules of the Millon Adolescent Clinical Inventory (MACI), 94 youth were excluded from the original sample due to invalid responding. This resulted in a total of 420 youth: 275 in Group 1, 111 in Group 2, and 34 in Group 3. On average, the youth were 16.7 years of age (SD = 1.8 years) and in the ninth grade (M = ninth grade, SD = 1.6 grades). Typical of juvenile sexual offender samples, most of the youth were Caucasian (52.5%) followed by African American (28.7%) and Hispanic (6.3%), and 5.8% were Native American. An additional 6.8% were from other racial groups.
Materials
Community Exposure to Violence (CEV) is an unpublished self-report assessment tool used in previous research (e.g., Burton, 2003) and was used to measure level of exposure to violence within the study participant’s community. The instrument contains 13 questions, as shown in Table 2, with a 4-point frequency scale ranging from 1 (never) to 4 (many times). Total scale scores could therefore range from 13 to 52, with higher numbers indicating greater exposure to violence within the community. Reliability for this measure in this study was calculated to be α = .92. When only data from sexual offenders were used, Cronbach’s alpha was even stronger (α = .95). Validity of this measure could not be established as the measure was created for this research project.
The Childhood Trauma Questionnaire (CTQ) is a 37-item self-report scale that screens for five types of traumatic experiences in childhood (Bernstein, Fink, Handelsman, & Foote, 1994). Each question has a 5-point frequency scale ranging from 1 (never true) to 5 (very often true). The scale is summative, with some items being reversed so that higher scores reflect more abuse. In previous studies, the full measure reliability (test–retest) is α = .88, and internal consistency ranges between .80 and .97 (Bernstein et al., 1994). Criterion validity for the measure was assessed and found to be acceptable (Bernstein et al., 1994). Reliability of each CTQ subscale in the current study ranged from α = .79 to α = .92.
The MACI is a self-report personality inventory that was originally designed for use with adolescents in clinical, residential, or correctional settings (Millon, 1993). The MACI was originally normed on 579 adolescents residing in such facilities, as well as two smaller cross-validation samples. The inventory consists of 160 True–False items which were derived from Millon’s personality theory, and each of the items was intended to elicit aspects of adolescent personality characteristics and clinical disorders. Multiple subscales exist within the MACI, and those specifically relating to depressive affect were used for this research project. Higher scores on each subscale indicate higher degree of impairment with that particular clinical syndrome. The Depressive Affect subscale is based on 33 questions. The subscales do not have a summative score but instead are base rate scores (Millon, 1993). This method of scoring includes adjustments for age and over- and under-disclosure tendencies of adolescents, as well as the influence of depressed affect at time of measure completion. A score below 60 is considered not indicative of the presence of an affective disorder. Scores between 61 and 74 indicate the presence of clinical syndrome although scores are not clinically significant until a score of 75 or higher, and scores of 85 and above indicate a strong presence of the clinical syndrome.
The authors of the instrument manual reported high test–retest validity for the MACI subscales used for this project, and Depressive Affect had 81% agreement (Millon, 1993), in which test re-administrations were spaced 3 to 7 days apart. In the current study, overall reliability for the MACI is α = .86, and the subscales met the standards for reliability with the following Cronbach’s: Depressive Affect Scale (33 items, α = .97). Good criterion and concurrent validity have also been established for this measure (Millon & Davis, 1993; Pinto & Grilo, 2003).
Results
Childhood Trauma
Frequencies of each of the childhood trauma types experienced by the sample were calculated using the CTQ (see Table 1). The percentage rates reflect the number of male youth endorsing one or more questions regarding each form of trauma, divided by the number of youth who responded to the questions on each subscale. Percentages for each type of childhood trauma were very high, which may have been due to the sample used (incarcerated male adolescent sexual offenders) or due to an overlap of different forms of childhood trauma that may not have been differentiated adequately by the scale. Also, participants were included in the percentage for each subscale even if they only answered one question positively. This being said, the sample used for this project endorsed CEV and physical neglect as the most frequent forms of childhood trauma experienced, with emotional neglect and physical abuse following close behind. Sexual abuse was endorsed the least by this population, although it was nevertheless endorsed by almost 77% of the sample.
Frequency of Trauma Exposure by Type.
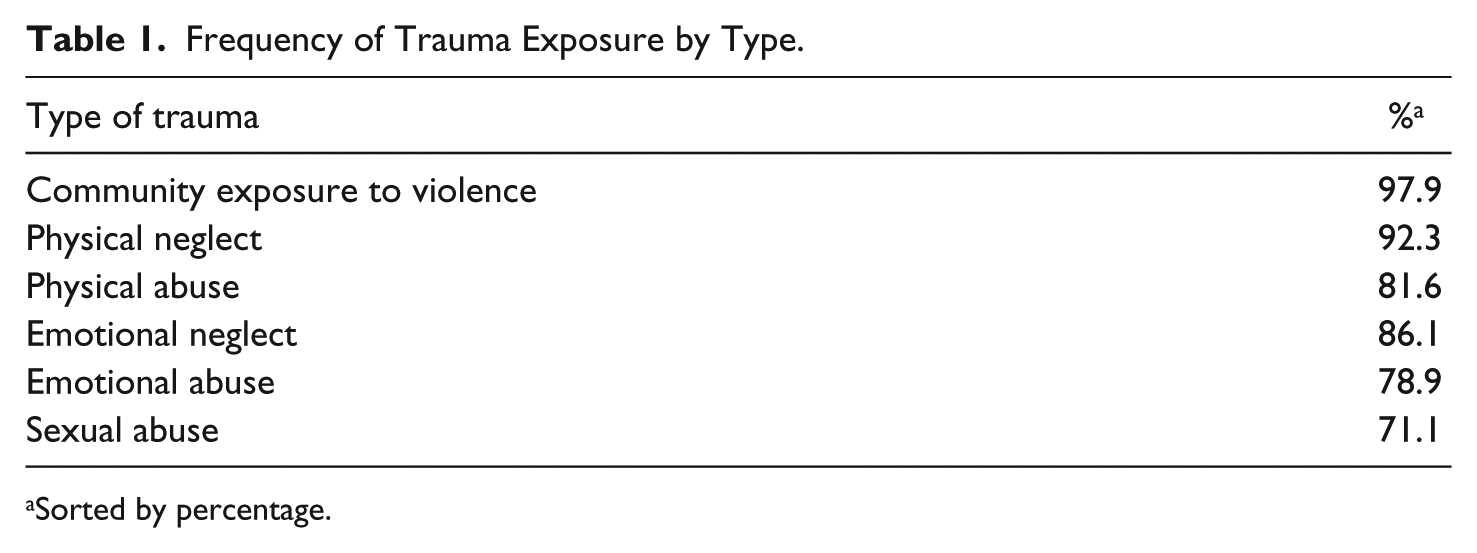
Sorted by percentage.
Each question on the CEV scale had a minimum of 1 and a maximum of 4 points, with final scores being a sum of each question. Frequency results for each question of the CEV scale, ordered by total positive endorsement of exposure, are located in Table 2.
Percentage of Sample Endorsing Each Item of the CEV Scale.
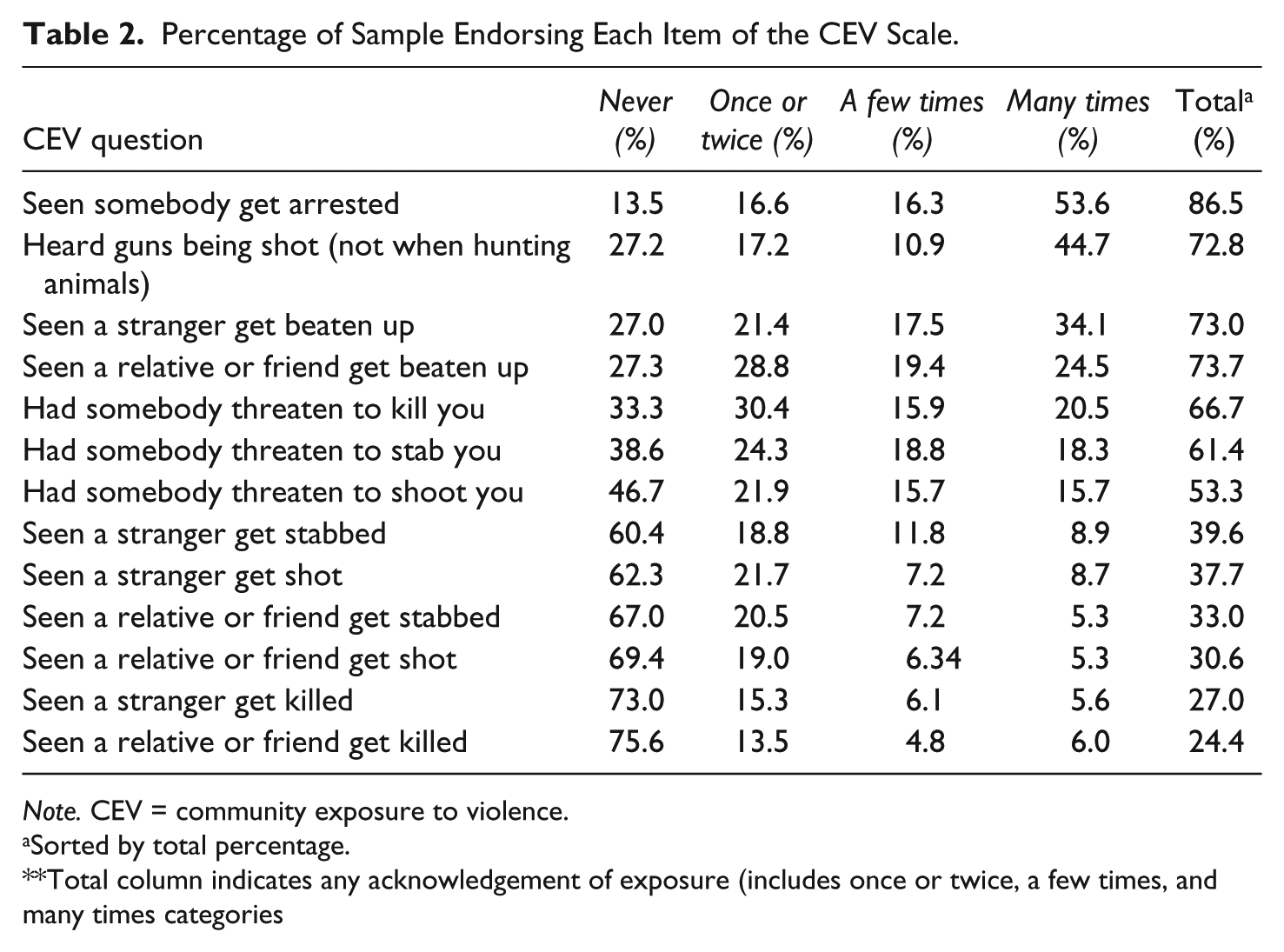
Note. CEV = community exposure to violence.
Sorted by total percentage.
Total column indicates any acknowledgement of exposure (includes once or twice, a few times, and many times categories
The most endorsed forms of exposure to violence for the sample were witnessing an arrest, hearing gunshots, and seeing a stranger or relative get beaten up. These are more passive forms of violence exposure, not involving the individual, which are important to acknowledge because exposure and direct victimization are often researched separately, and can have varying impacts on youth. Being threatened in any form was also highly endorsed by this sample.
Impact of Poly-Victimization/Cumulative Trauma
Given that multiple exposures to trauma are common for juvenile sexual offenders (Macmillan & Hagan, 2004; Menard, 2002; Finkelhor et al., 2009), measurement of the frequency of exposures to each childhood trauma type was conducted using the CTQ (see Table 3). Less than 10% of the sample used for this project experienced three or fewer traumas during their childhood. None of the participants reported zero childhood traumas, and more than half of the youth endorsed six or more traumatic experiences. Given that approximately 90% of the sample endorsed four or more traumas, further exploration of the impact of multiple traumas on level of depression was conducted.
Frequency Data for Multiple Exposures to Trauma.

Participants were included in the percentage rates even if they only endorsed one question on the subscale positively.
Depression
In this sample, 27% of the youth were at or above the base rate of 75 indicating a clinical level of concern for depression. Correlations were used to assess the relationship between scores on each scale, including the six subscales reflecting each type of trauma, and the MACI Depressive Affect scale. The highest correlation (r = .84) was between emotional abuse and physical abuse, perhaps because these forms of abuse often co-occur (Barnett et al., 2005; Bingelli et al., 2001; Trickett, Kihyun, & Prindle, 2011). Physical neglect is also significantly and highly correlated with physical abuse (r = .57), emotional abuse (r = .51), and emotional neglect (r = .49). This may support recent research efforts, suggesting that emotional and physical neglect, as well as emotional abuse, are perhaps a component of all other forms of abuse (Barnett et al., 2005; Bingelli et al., 2001). Emotional abuse was most highly correlated with depressed affect (r = .28), followed by physical abuse (r = .21). Sexual abuse, emotional neglect, and physical neglect were very close to the same level of correlation with depression as physical abuse. All p values for the reported correlation coefficients are <.01.
Table 4 contains a summary of regression model in which all six forms of trauma were regressed onto depressive affect. Multi-collinearity was assessed to ensure that the predictor variables were not too highly correlated: All the variance inflation factors were below 4. Only emotional abuse had a significant relationship with depressive affect, making it the best predictor of variance in depressive affect score when all forms of trauma were entered into the model. To create a more parsimonious model, the other five types of abuse were removed, and a regression of emotional abuse onto depressive affect was calculated. The results of that model indicate that for every 1-point increase in the emotional abuse score, the depression score increases by 1.53 points. Emotional abuse accounted for 6% of the variance in the respondents’ Depressive Affect scale scores. While the percentage of variance accounted for is not large, emotional abuse is significantly related to depressive affect (p < .001).
Trauma × Depressive Affect.
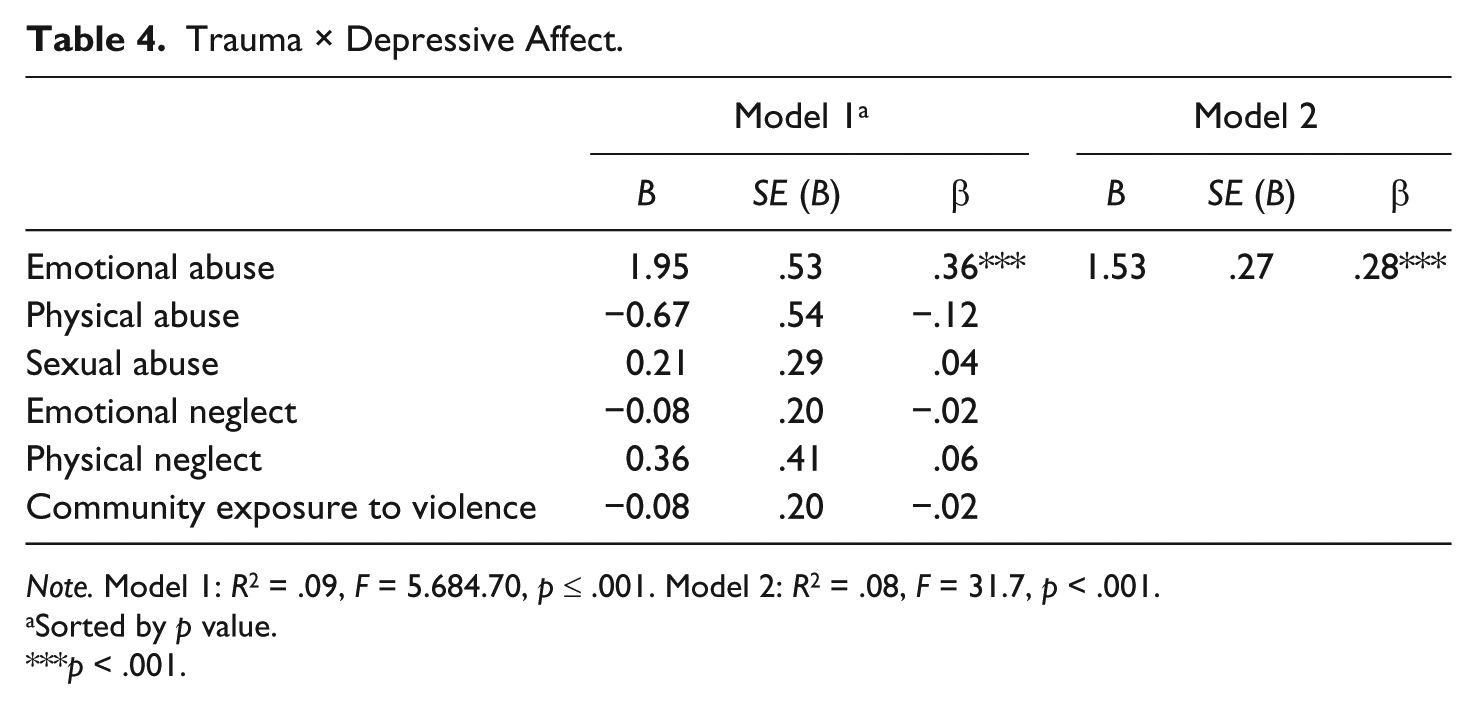
Note. Model 1: R2 = .09, F = 5.684.70, p ≤ .001. Model 2: R2 = .08, F = 31.7, p < .001.
Sorted by p value.
p < .001.
Next, a regression analysis was conducted to explore the impact multiple abuses had on depressive affect (see Table 5). This analysis revealed that for every additional type of trauma experienced, the depression score increased by 5.85 points. This implies that it is useful to assess the number of trauma types experienced by a youth as a predictor of variance in depressive affect score because it would allow for easier interpretation of the change using the Beta. For example, using Model 2 of the first regression, if one youth has a 5-point difference than another on the Emotional Abuse scale of the CTQ, he may then have a depression score which is elevated by 7.7 points. With the second regression, if one youth has two more trauma types than another, his depression score may be elevated by 11.7 points. Number of types of abuse accounted for 5% of the variance in the respondents’ Depressive Affect scale scores. While this percentage is low, the results are still statistically significant. Given the large percentage of the sample endorsing six or more exposures to childhood trauma, this second model has greater ability to identify which youth are experiencing or at risk of developing higher levels of depressive affect.
Number of Types of Abuse × Depression.

Note. R2 = .05, F = 23.313.67.
p ≤ .001.
Discussion
Rates of each type of trauma in this sample of incarcerated sexually abusive youth were significantly higher than those found in prior research projects (Burton, 2003; Copeland, Keeler, Angold, & Costello, 2007; Johnson-Reid & Way, 2001; OJJDP, 2011; Weeks & Widom, 1998). Finkelhor and colleagues’ (2005) findings from similar research with typical adolescents found that rates of each type of trauma were also much lower than those reported in this project. While adequate comparison of the results of the current project with the results of Finkelhor and colleagues is challenging due to different sample characteristics and differences in the measures used, it is worth noting the significantly higher trauma rates for the sample of JSOs included in the current study (recalling inclusion criteria).
Rates of exposure to multiple traumas obtained from this project were also much higher than those reported for both typical adolescents (Finkelhor et al., 2009) and JSOs (Johnson-Reid & Way, 2001). A comparison of results, acknowledging different sample sizes and characteristics, can be seen in Table 6. Also, Johnson-Reid and Way (2001) reported that 45% of their sample of sexual offenders (N = 51) had at least three prior confirmed reports of childhood trauma, which is less than half of the current study’s rate. Given the large difference between scores, recognition of the need to identify multiple exposures to trauma for juvenile sexual offenders is warranted, and further exploration of the impact of multiple exposures and adequate intervention strategies is needed.
Comparison of Number of Trauma Exposures with Finkelhor, Turner, Ormrod, and Hamby’s (2009) Results.

Emotional abuse emerging as the strongest predictor of depressive affect for adolescent juvenile sexual offenders was an interesting finding from this study. While several trauma researchers have shown that constant criticism, threats or rejection by caregivers, and the withholding of love, support or guidance can have a negative impact on a child’s attachment and overall development (Cloitre et al., 2009; Cook et al., 2005), it is useful to have statistical support for the negative effects of emotional abuse, and highlights the need to address this under-assessed, under-studied, and often under-treated form of abuse. This result is consistent with prior research findings that verbal abuse by a parent is more predictive of depressive symptomatology than physical or sexual abuse (Rich, Gidycz, Warkentin, Loh, & Weiland, 2005). This may be explained by the development of negative or worthlessness schemas that are internalized by the youth after experiencing emotional abuse by a parent or primary caregiver, which can subsequently lead to the development of depression (Lumley & Harkness, 2007).
While parents are often held accountable in the child welfare systems for obvious and extreme neglectful behavior, it can be challenging to recognize and assess milder forms of emotional abuse and neglect. Often, it is only ongoing and excessive forms that receive state intervention, which may mean that more pervasive but less severe forms of emotional abuse and neglect are unnoticed and untreated for some youth. This may contribute to clinicians, researchers, and child welfare workers “making a mole-hill out of a mountain” (McSherry, 2007), in which significant issues of emotional abuse and neglect remain under-recognized and addressed.
Prior researchers have suggested that physical and sexual abuse are most highly correlated with higher rates of depression among juvenile sexual offenders (Becker et al., 1991), although the results of this project did not support these findings. While sexual abuse was the next strongest predictor of depression for our sample, it offered roughly one quarter of the predictive strength of emotional abuse.
Unlike Finkelhor et al.’s (2009) prior findings, the number of traumas did not turn out to be as strong a predictor of depressive affect as emotional abuse history. However, multiple exposures to trauma were significant predictors of depressive affect on its own, and collecting data on number of types of trauma exposures is probably easier and less intrusive than gathering details of actual traumatic incidents. Also, the experience of multiple traumas in childhood has been linked to depression in adulthood (Powers et al., 2009; Vranceanu, Hobfall, & Johnson, 2007), which suggests persistence of the negative impacts.
Researchers who have explored complex trauma reactions in children now offer a more comprehensive model for understanding the developmental effects of traumatic exposure on youth (Cloitre et al., 2009; Cook et al., 2005). The full biological and neurobiological impact of trauma affects critical regions of the brain that help children develop and maintain relationships, learn and recall information, and regulate their emotional states (Krystal & Neumeister, 2009). Trauma may also affect the part of the brain that helps control behavior and modulate impulses, especially those that occur secondarily to intense negative affect (Cloitre et al., 2009; Cook et al., 2005; Krystal & Neumeister, 2009). The current research study highlights the connection between violence exposure/victimization and depression, and the complex trauma reaction research suggests how the biological impact of trauma could lead some of these victimized youth on a pathway toward delinquency (Ford et al., 2012).
Rates of depressive affect in this sample were 9 to 39 times higher than those observed in the general adolescent population (Angold & Costello, 1993; Substance Abuse and Mental Health Services Administration, 2008). The number of participants from this study meeting criteria for concerning level of depressive affect was 27%, higher than research findings on both typical adolescent juvenile delinquents (Domalanta et al., 2003) and incarcerated male adults (Stinson, Becker, & Tromp, 2005). Given the connections between depression and suicide (Rohde, Mace, & Seeley 1997) and depression and delinquency (Domalanta et al., 2003; Stinson et al., 2005), as well as the finding that negative mood states consistently occur prior to sexually inappropriate acts within sex offending populations (Nelson, Miner, Marques, Russell, & Achterkirchen, 1989; Stinson et al., 2005; Ward & Hudson, 1998), adequate assessment of and treatment for JSOs with depression are warranted.
In addressing the research questions formulated for this study, emotional abuse strongly predicts current depression for male juvenile sexual offenders. Number of traumas was not as strong a predictor of depression in JSOs as emotional abuse; yet, multiple exposures to trauma were significant predictors of depressive affect on its own.
Research Implications
Future researchers could further explore the role multiple exposures to trauma play in the development of delinquent adolescents. Research on and development of the diagnosis of complex trauma reactions (Cook et al., 2005) show promise for reflecting the multi-domain impact that traumatic childhood experiences can have for youth. Integration of neurobiological research findings on the effects of trauma on the developing mind and body with adequate information regarding the influence of affective states could lead to more powerful interventions that may foster resiliency and diminish the negative impact trauma can have (Caspi et al., 2002; Cook et al., 2005).
In addition, more research on emotional abuse would be helpful to define this form of abuse in a manner that can be used across disciplines, and to clarify which forms and how much exposure to it correlate with a traumatic effect on youth. In line with recent efforts to promote interprofessional collaboration when working with juvenile justice involved youth, child welfare professionals, social workers, as well as lawyers and judges, need common language and diagnostic criteria to make effective and consistent decisions for children exposed to emotional abuse (and other types of traumas). Researchers of non-physical, emotional abuse in adult couples and families have developed a stage model that may be useful for future research efforts with children (James & MacKinnon, 2010). Their framework incorporates length of time over which the abuse takes place and the intentions of the abuser, in addition to the overall impact on the victim. Their model defines and distinguishes among verbal, emotional, and psychological abuse, and proposes that these forms of non-physical abuse exist on a continuum of intensity ranging from mild to severe (James & MacKinnon, 2010). The use of this, or a similar, framework in future research on children exposed to emotional abuse may provide information that could be useful for improved policy and intervention development.
Treatment Implications
Several salient treatment implications may be drawn from the findings of this study. First, identifying children who have experienced emotional abuse and providing treatment for reactions to this form of trauma may decrease the likelihood that they will suffer with depression presently or in the future. Clinicians and professionals conducting assessments with juvenile sexual offenders should consider the degree of depressive affect impacting the adolescent, particularly if there is an indication that emotional abuse or exposure to multiple traumas has occurred. Depressive symptoms have a strong causal link with adolescent suicide (Hetrick, Parker, Robinson, Hall, & Vance, 2012; Rohde et al., 1997) and psychiatric problems in adulthood (Pine, Cohen, Gurley, Brook, & Ma, 1998), and can be very disruptive and damaging to an adolescent’s daily functioning and overall development. Overall, effective and clinically indicated treatment approaches when working with juveniles with sexually harmful behavior address the sequelae of traumatic stress and incorporate strategies to address co-occurring disorders and behavioral health issues into usual sex-offense treatment programs (Righthand, Baird, Way, & Seto, 2014). Examples of approaches include trauma-focused cognitive-behavioral therapy (TF-CBT; Cohen, Mannarino, & Iyengar, 2011) which is designed to help youth develop effective coping strategies and engages the family system to address trauma narratives.
Second, assessment and treatment for childhood trauma among juvenile sexual offenders are important to address the associations among trauma exposure, depression, and subsequent delinquent behavior. Researchers developing complex trauma assessment and treatment protocols offer insight into how to understand the multi-faceted impact of trauma and provide guidance for practitioners in terms of treatment targets (Cook et al., 2005). A comprehensive assessment of the domains of impairment related to complex trauma that include attachment, biological concerns, affect regulation, dissociation, degree of behavioral control, cognitive strengths and weaknesses, and overall self-concept is needed to address the specialized mental health needs of youth with sexually harmful behavior (Burton, Duty, & Leibowitz 2011; Ford et al., 2012). Individualized assessments and treatment plans are necessary for JSOs, as well as comprehensive service delivery with coordination between providers that include the caregivers (Bengis, 2010). Promising interventions that reduce the likelihood of recidivism address the multiple needs of youth and engage the caregiver network, such as multi-systemic therapy for problematic sexual behavior (MST-PSB; Letourneau et al., 2009). As JSOs receive services in a variety of settings, coordination of care and consistent implementation of assessment and intervention strategies are needed.
Limitations
It is important to consider the limitations of this research. The first limitation is that data were collected at one point in time, and therefore provide cross-sectional versus longitudinal information about how exposure to traumatic experiences or depressive affect changes over time. Second, while the sample size was large, a bigger and more diverse sample may have provided more extensive findings. Third, self-report measures were used which rely on adolescent participant’s ability to recall events accurately and their overall motivation to offer accurate information. In addition, comparison studies had different sample characteristics (correctional vs. non-adjudicated youth) and used different measures for data collection (the Juvenile Victimization Questionnaire [JVQ] compared with the CTQ). Differences in sample characteristics and methodology across studies made it difficult to generalize the results.
Finally, no information was available in the dataset regarding genetic predisposition to depression, or whether incarceration had an impact on each adolescent’s mood state at the time of assessment. Other risk and resiliency factors were also unavailable for this sample, such as cognitive strengths and limitations, which may have provided additional insights into different reactions to traumatic experience by study participants. Future researchers could explore these important areas, and therefore contribute to the overall effort to improve services for juvenile sexual offenders.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.