
Abstract
Despite the growing incidence of child exploitation offences, there is little knowledge of the neuropsychological function of older child exploitation material offenders (CEMOs). Given that studies have reported that sex offenders demonstrate deficits attributed to frontal and temporal lobe function, the aim of this pilot study was to investigate the frontotemporal function of older first-time child exploitation material offenders (FTCEMOs). The neuropsychological performance of 11 older FTCEMOs was compared with 34 older historical sex offenders (HSOs) and 32 older nonsex offender (NSO) controls. Forty-five percent of FTCEMOs admitted to a pedophilic interest, which was significantly lower than those reported by HSOs. FTCEMOs provided significantly higher intellectual function scores than HSOs. Results revealed no evidence of mild or major neurocognitive disorder in FTCEMOs. Although the groups were not significantly different, compared with normative data, FTCEMOs reported a high incidence of impairment on a measure of decision making and on a measure of facial emotional recognition.
Keywords
Although the literature on the neuropsychological function of sex offenders has been mixed and inconclusive, a number of studies have reported deficits/weaknesses associated with the functions attributed to frontal and temporal areas (Cantor et al., 2004; Eastvold, Suchy, & Strassberg, 2011; Joyal, Beaulieu-Plante, & de Chanterac, 2014; Kelly, Richardson, Hunter, & Knapp, 2002; Langevin & Curnoe, 2008a; M. H. Stone & Thompson, 2001; Suchy, Whittaker, Strassberg, & Eastvold, 2009; Young, Justice, & Edberg, 2010). Some studies suggest an association between generalized and discrete cognitive dysfunction and child sexual offending, including lower intelligence (IQ; Cantor, Blanchard, Robichaud, & Christensen, 2005; Joyal, Black, & Dassylva, 2007; Langevin & Curnoe, 2008b), deficits in verbal fluency (Joyal et al., 2007), attention (Kafka & Hennen, 2002), executive function (Eastvold et al., 2011; Schiffer & Vonlaufen, 2011; Veneziano, Veneziano, LeGrand, & Richards, 2004), and processing speed (Suchy, Eastvold, Strassberg, & Franchow, 2014). In their meta-analysis, Joyal et al. (2014) concluded that sex offenders against children demonstrate lower scores than sex offenders against adults on executive function measures, namely, the Wisconsin Card Sorting Test (deduction and cognitive flexibility), the Controlled Oral Word Association Test (COWAT; verbal fluency), and the Stroop Test (control of internal interference).
The majority of neuropsychological studies have focused on adolescent and adult sex offenders below the age of 40, with little research conducted on older sex offenders. Although some studies have reported a high prevalence of psychiatric morbidity in sex offenders, including psychosis, substance abuse, and mood and personality disorders (Cohen et al., 2002; Dunsieth et al., 2004; Fazel, Hope, O’Donnell, & Jacoby, 2002; Fazel, Sjostedt, Langstrom, & Grann, 2007; Kafka & Hennen, 2002; Koch, Berner, Hill, & Briken, 2011; McElroy et al., 1999; Wallace et al., 1998), a surprisingly low prevalence of brain abnormality has been reported in older sex offenders (Clark & Mezey, 1997; Fazel et al., 2002; Fazel, O’Donnell, Hope, Gulati, & Jacoby, 2007; Hucker & Ben-Aron, 1985). Contrary to long-held beliefs that sexual offending by older men is associated with age-related brain changes (Roth, 1968), Fazel, O’Donnell, et al. (2007) found no evidence of frontal dysfunction in a sample of 50 older sex offenders. However, Fazel, O’Donnell, et al. (2007) used four screening tests (verbal fluency, alternating sequences, a measure of abstraction, and a measure of set-shifting), which may have limited their conclusions.
Although a number of studies have investigated psychological profiles (Elliott, Beech, Mandeville-Norden, & Hayes, 2009), personality characteristics (Aslan, 2011; Reijnen, Bulten, & Nijman, 2009), and pedophilic diagnosis (Eke, Seto, & Williams, 2011; Seto, Cantor, & Blanchard, 2006), as well as the imminent risk that child exploitation material offenders (CEMOs) can pose to children (Long, Alison, & McManus, 2013), there are no known neuropsychological studies in CEMOs.
This pilot study compared the neuropsychological function of older adult first-time child exploitation material offenders (FTCEMOs) with older adult contact sex offenders, historical sex offenders (HSOs), and older adult nonsex offenders (NSOs). In addition, this study investigated social cognition, by using a measure of facial emotional recognition, to clarify whether facial emotional recognition deficits were present in FTCEMOs. This study had two hypotheses:
Method
Participants
Seventy-seven male participants (median age = 59, range 50-85 years) participated in this study; 90% were incarcerated, including 82% of FTCEMOs, 85% of HSOs, and 100% of NSOs. The remaining 10% of participants were recruited from a community-based sex offender treatment program. Exclusion criteria for HSO and NSO groups were being non–English speaking, unable to complete questionnaires, being illiterate, or having medical conditions known to affect neuropsychological performance.
FTCEMO
Eleven FTCEMOs, with a mean age of 61 years (SD = 7.8, range 52-75 years) with a median age of 58 years, who were charged at or after the age of 50 of at least one child exploitation material offence were recruited. The number of child exploitation images in possession of the offender depicting young children of either gender, from the ages of 8 to 16, ranged from 6 to 24,000.
HSOs
Thirty-four sex offenders against children with convictions before the age of 50 (HSO) with a mean age of 62.3 years (SD = 6.6, range 51-85 years) and a median age of 57 years were consecutively recruited. Fifty-three percent of the victims were male. Eighty-two percent were extrafamilial sex offenders, and 21% were incest offenders, with five (15%) HSOs committing both types of sexual offences against children. The inclusion criteria for HSOs were being male over the age of 50 and having been convicted, before the age of 50, of a contact sexual offence against at least one child.
NSOs
Thirty-two offenders with no history of sex offences (NSO) with a mean age of 57.3 years (SD = 6.5, range 50-75 years) and a median age of 56 years were recruited. Furthermore, NSOs had no history of pervasive violence. The criminal history was corroborated for accuracy from official criminal records. The recruitment of NSOs was to control for neuropsychological findings potentially attributable to incarceration-related stress or general criminality.
Procedure
FTCEMOs were compared with HSOs and NSOs on various neuropsychological measures. In addition, the results were compared with normative data to assess impairment using age and education norms from individual measures.
The prison assessments were conducted at a Sex Offender Program and the general offender population of Long Bay Prison, Sydney. The community assessments were conducted at a Forensic Psychology Service, which offers group treatment to individuals who have committed sexual offences and are subject to probation or parole. The first author of this article conducted all the neuropsychological assessments over a 3-year period (from December 2008 to September 2011), which formed the basis of his doctorate studies.
Ethics approval from the New South Wales Department of Corrective Services and the Justice Health Human Research Ethics Committee, Sydney, Australia, and written informed consent from all participants were obtained. No incentives or inducements were offered.
Measures
Semistructured interview
Clinical data were obtained via a 60-min semistructured interview that included collecting demographic information. The medical, drug and alcohol, and psychiatric histories were collected to establish a possible association with impaired neuropsychological function. This information was corroborated from prison files.
Screening measures
Participants were screened for major neurocognitive disorders using the Addenbrooke’s Cognitive Examination–Revised (ACE-R; Mioshi, Dawson, Mitchell, Arnold, & Hodges, 2006), which measures performance on five cognitive domains, including attention/orientation, memory, language, verbal fluency, and visuospatial skills.
The Depression, Anxiety, and Stress Scales (DASS; Lovibond & Lovibond, 1995) was used to screen for depression, anxiety, and stress.
Neuropsychological measures
Intellectual function
As neuropsychological test performance is known to be associated with intellectual ability (Diaz-Asper, Schretlen, & Pearlson, 2004), the Wechsler Abbreviated Scale of Intelligence (WASI) was used to assess global intellectual function.
Executive function
The Hayling Test (Burgess & Shallice, 1997) was used to assess response initiation and suppression. The Hayling Test is associated with left prefrontal lobe function (Collette et al., 2001; Nathaniel-James, Fletcher, & Frith, 1997). The Hayling consists of two sets of 15 sentences, each having the last word missing. In the first part, Section 1, the examiner reads each sentence aloud and the participant has to complete the sentence as quickly as possible. For example, “The old house will be torn . . . (participant says) down.” This section yields a simple measure of response speed. In the second part, Section 2, the participant is faced with the novel task of completing the sentence with a word that is unconnected to the sentence in every way. For example, “The captain wanted to stay with the sinking . . . (Participant says) light bulb.” In this instance, the participant has to inhibit a strongly activated (automatic) response before generating a new response. This section yields two scores, an error score and response speed. Category A errors are responses that plausibly complete the sentence. Category B errors are responses connected to the sentence in some way, but not direct completions of the sentence. Sentence completions that are unconnected to the sentence are considered correct responses.
Letter fluency was assessed using the COWAT (Benton & Hamsher, 1989), which, in this study, required participants to generate words beginning with the letters “F,” “A,” and “S” in 1 min, excluding proper nouns, numbers, and the same word with a different suffix.
Decision making was assessed with the Iowa Gambling Task (IGT), which can, along with other measures of executive function, be predictive of deficits in decision making in patients with damage to the ventromedial prefrontal cortex (VMPFC), who exhibit real-world decision-making deficits (Bechara, 2007).
Attention, concentration, resistance to distraction, and cognitive flexibility (or set-shifting) was assessed using the Trail-Making Test (TMT). The TMT is a standardized visual search and sequencing task that is heavily influenced by attention, concentration, resistance to distraction, and cognitive flexibility (or set-shifting; Strauss, Sherman, & Spreen, 2006). More specific purposes include the detection of deficits in executive function, psychomotor speed, visual search and sequencing, attention, and set-shifting (Demakis, 2004; Reitan & Wolfson, 1994). Part A of the TMT requires visual scanning, numeric sequencing, and visuomotor speed. This portion of the test is not a valid indicator of brain impairment as there is not a significant amount of time difference between normal subjects and brain-damaged patients (Bradford, 1992). However, the time performance of Part B has been found to be sensitive to frontal lobe pathology and is an index of executive function (Arbuthnott & Frank, 2000; Davidson, Gao, Mason, Winocur, & Anderson, 2008; Gouveia, Brucki, Malheiros, & Bueno, 2007; Misdraji & Gass, 2010; Sanchez-Cubillo et al., 2009; Terada et al., 2013).
Memory function
The Rey Complex Figure Test (RCFT; Meyers & Meyers, 1995) was used to test for visuospatial memory. The RCFT has been found to load on executive function and memory (Smith & Zahka, 2006). In clinical studies, patients who use disorganized strategies to copy the RCF demonstrate difficulty recalling the figure after a delay and, subsequently, perform poorly (Newman & Krikorian, 2001).
The Rey Auditory Verbal Learning Test (RAVLT) was used to assess immediate memory span, new learning, susceptibility to interference, and recognition memory (Schmidt, 1996).
Facial Emotional Recognition measure
Recognition of facial expressions of basic emotions was assessed with the Facial Expression of Emotion: Stimuli and Tests (FEEST; Calder, Ekman, Perrett, Sprengelmeyer, & Young, 2002), which has been shown to be a reliable measure of emotion recognition in various populations (Edwards, Jackson, & Pattison, 2002; Spikman et al., 2013). The FEEST uses a range of photographs from the Ekman and Friesen series of Pictures of Facial Affect (Ekman & Friesen, 1976). Six basic emotions (happiness, sadness, disgust, fear, surprise, and anger) were presented on a computer screen for 1.5 s each. The participants were asked to respond as fast as they could by identifying the emotion from the list of six emotions.
Statistical Analysis
Descriptive analyses were performed to examine baseline characteristics of study participants. Maximum likelihood chi-square tests were used for categorical variables. Analyses of variance (ANOVAs) were used to evaluate group differences in continuous measures. Multivariate analysis of variance (MANOVA) was used to compare the individual neuropsychological tests among the three groups to reduce the family-wise error rate. The relationship between three or more discrete variables was analysed through the multiway frequency analysis and log-linear analysis. Logistic regression was used where the response variable was binary, for example, data with measured responses present/absent. The three variables of age, education, and intelligence were assessed for their suitability as covariates. The statistical program SPSS 21.0 was used and a test was deemed significant at p < .05.
There were missing data for some variables: leaving the following data set: DASS (n = 73); ACE-R (n = 76); Full-Scale Intelligence Quotient (FSIQ) (n = 73), Performance Intelligence Quotient PIQ (n = 69), Verbal Intelligence Quotient (VIQ) (n = 67); Hayling (n = 76); F,A, and S words (FAS) (n = 75); TMT-A & B (n = 70); RCF (n = 74); RAVLT (n = 74); and FEEST (n = 65). The available data were sufficient to conduct the analyses. No cases were deleted due to missing data.
Results
Demographic Data
As Table 1 demonstrates, NSOs were significantly younger than HSOs, F(2, 74) = 4.783, p = .011. In addition, FTCEMOs demonstrated significantly higher FSIQ, F(2, 69) = 3.352, p = .041, than HSOs. Age and FSIQ were therefore entered as covariates in the final analyses unless age-appropriate normative data were already provided by the individual measure, as is the case with the WASI. The groups did not differ in years of education. FTCEMOs were more likely to be married compared with HSOs (χ2 = 6.823, df = 1, p < .05) and were more likely to be employed in skilled or semiskilled occupations compared with HSOs (χ2 = 14.436, df = 2, p < .001). While the majority of offenders reported a heterosexual orientation, HSOs reported a significantly lower rate of heterosexuality (χ2 = 15.565, df = 2, p < .001). The groups did not significantly differ in the rate of alcohol abuse, although the rate of alcoholism was high (between 41% and 46%). NSOs reported higher rates of drug use than both sex offender groups (not interpretable by chi-square due to low frequencies in the sex offender groups).
Sample Demographics.

Note. FTCEMO = first-time child exploitation material offenders; HSO = historical sex offender; NSO = nonsex offender.
Although FTCEMOs did not differ from HSOs and NSOs, they self-reported a 55% rate of lifetime depression. The groups did not differ in the rate of head injury (defined as a self-reported period of loss of consciousness, requiring medical observation), which was 56% for the sample.
FTCEMOs self-reported a significantly lower rate of pedophilic interest than HSOs (χ2 = 5.786, df = 1, p = .016).
FTCEMOs had spent significantly less time in prison than HSOs and NSOs (p < .001). As expected, NSOs had a significantly higher nonsexual offending rate compared with the two sex offender groups (χ2 = 15.341, df = 2, p < .001). Approximately 46% of FTCEMOs had a nonsexual criminal history (i.e., one break and enter, two stealing, two common assault, one driving offence, one auto theft). FTCEMOs and HSOs did not differ in their rate of nonsexual offending (see Table 2).
Types of Nonsex Offences Committed by HSOs and NSOs.

Note. HSO = historical sex offender; NSO = nonsex offender.
The “Other offences” category included larceny, perverting the course of justice, and receiving/possession of stolen goods.
Screening Data
None of the FTCEMOs met ACE-R cutoff criteria for a neurocognitive disorder, whereas almost 30% of HSOs and 22% of NSOs met such criteria. HSOs provided significantly lower ACE-R scores than FTCEMOs (p = .004) and NSOs (p < .001). The groups provided similar DASS scores; therefore, any significant difference in neuropsychological scores results could not be attributed to symptoms of depression, anxiety, or stress.
Neuropsychological Data
Intellectual function
FTCEMOs provided significantly higher mean FSIQs, F(2, 71) = 3.659, p = .034, than HSOs, but they were not significantly different from NSOs. The HSOs and NSOs did not differ in FSIQ. The groups did not differ in VIQ or PIQ.
Executive function
HSOs provided significantly lower Hayling total scores than NSOs (p = .002). There were no other group differences. Log-linear modelling revealed that the two sex offender groups committed significantly more Category A errors than NSOs (p < .001), whereas the sex offender groups did not significantly differ from each other. The groups did not significantly differ on Category B errors. There were no significant differences in Hayling impairment, which was defined as a score of 3 or less. FSIQ accounted for the majority of the variance between the groups (p = .009).
Despite the FAS mean differences, log-linear modelling showed no significant group differences, when age and IQ were included in the analysis. FSIQ accounted for the majority of the variance (p = .006) on the FAS.
On the IGT, ANCOVAAGE, IQ revealed no main group differences. In addition, log-linear modelling showed no significant group differences. Although the groups did not significantly differ on IGT impairment, compared with norms, the groups demonstrated high impairment rates on the IGT; that is, 42% of offenders were impaired on the IGT, including 55% of FTCEMOs.
On the TMT, the covariates Age and IQ were significant; however, there were no group differences in TMT-A. Although NSOs provided faster mean TMT-B times compared with the sex offender groups, these differences were not significant.
Memory function
RCF copy and immediate recall ANCOVAAGE, IQ revealed that Age was not a significant covariate. There were no group differences in RCF copy even when the covariate Age was taken out of the analysis. On RCF Immediate Recall, the mean recall performance by NSOs was not significantly different to those provided by HSOs due to the effect of Age and IQ.
A MANOVA of RAVLT Total and Recognition showed that Age was not a significant covariate; however, FSIQ was marginally significant (p = .048). A MANCOVAIQ of RAVLT Total and Recognition revealed no group mean differences.
Facial Emotional Recognition
The groups did not significantly differ on total FEEST; however, the three groups, compared with FEEST norms, demonstrated high rates of impairment, that is, between 57% and 76%. Although compared with FEEST norms the three groups demonstrated difficulties identifying fear, they were not significantly different from each other (see Table 3).
Neuropsychological Performance.
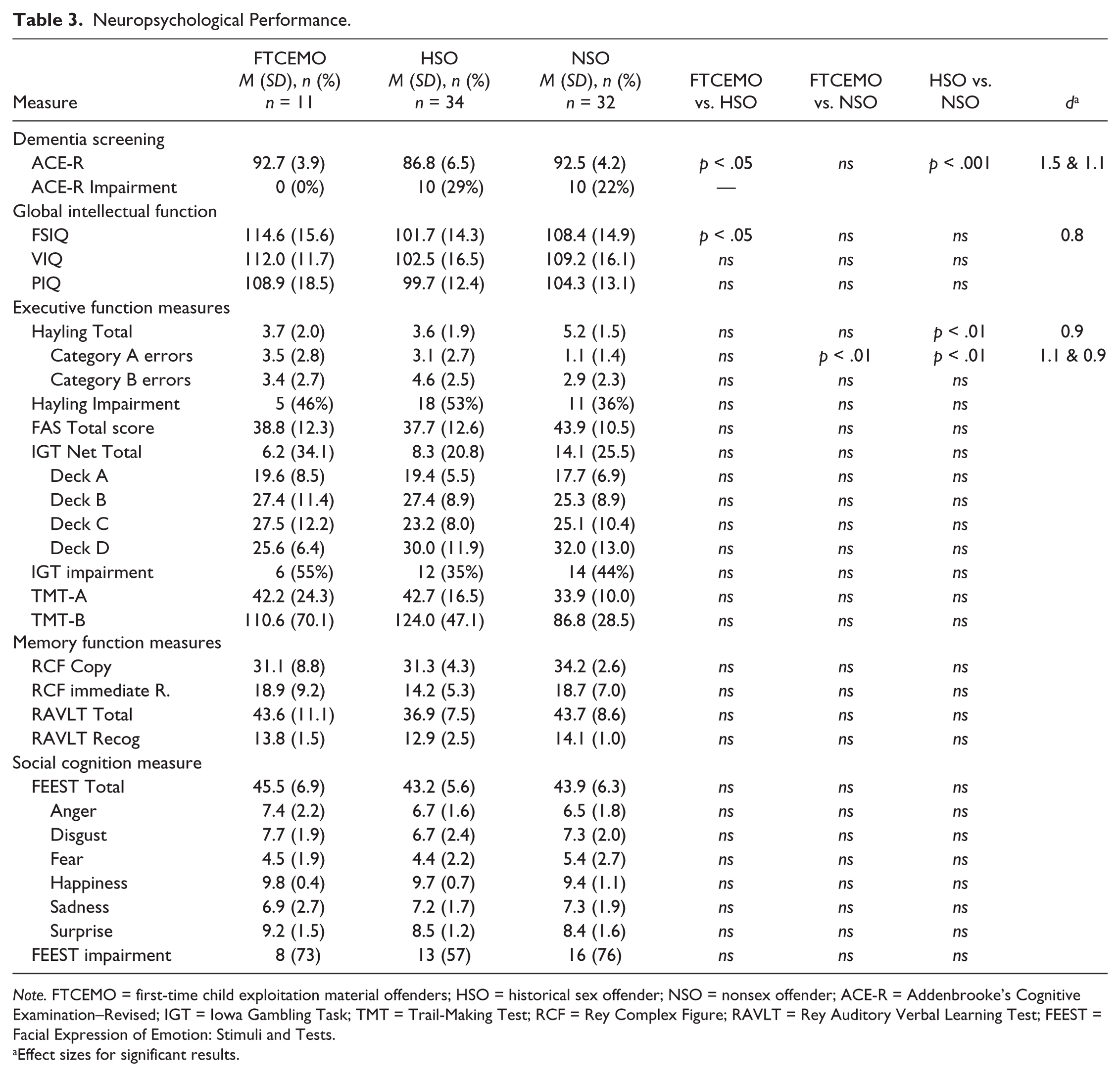
Note. FTCEMO = first-time child exploitation material offenders; HSO = historical sex offender; NSO = nonsex offender; ACE-R = Addenbrooke’s Cognitive Examination–Revised; IGT = Iowa Gambling Task; TMT = Trail-Making Test; RCF = Rey Complex Figure; RAVLT = Rey Auditory Verbal Learning Test; FEEST = Facial Expression of Emotion: Stimuli and Tests.
Effect sizes for significant results.
Discussion
This pilot study investigated whether older first-time CEMOs demonstrate neuropsychological deficits, namely, in executive function, memory, decision making, and social cognition. Overall, there was no significant difference in neuropsychological function between FTCEMOs and controls. Although there was a nonsignificant trend in inferior neuropsychological function in the sex offender groups, there was no support for the second hypothesis that sex offenders would demonstrate poorer neuropsychological function compared with NSOs.
Although the groups did not differ significantly on a measure of decision making, 55% of FTCEMOs demonstrated impairment on the IGT compared with normative data. However, conclusions made about IGT impairment, without evidence of executive function deficits, are premature in concluding that FTCEMOs present with decision-making deficits.
Although the groups did not differ on the FEEST, compared with norms, 73% of FTCEMOs displayed impairment in facial emotional recognition. Although the current findings are not definitive, the FEEST performance could suggest that FTCEMOs may lack empathy and demonstrate difficulty perceiving the mental states of others; that is, they lack “theory of mind” (V. E. Stone, Baron-Cohen, & Knight, 1998). Conversely, it is possible that FTCEMOs possess fewer victim empathy distortions than contact offenders (see Babchishin, Hanson, & VanZuylen, 2015; Elliott et al., 2009), which may explain why FTCEMOs demonstrate restraint to contact sexual offences, but demonstrate less victim empathy to child exploitation offences.
It is possible that the high lifetime depression rates among FTCEMOs, also previously found in CEMOs (Magaletta, Faust, Bickart, & McLearen, 2014), could have resulted in social avoidance, although the absence of significant differences in the rates of depression between the groups prevent any firm conclusions about this factor. Presumably, viewing child exploitation material provides a way to avoid negative emotional states, which has been identified previously in CEMOs (Quayle, Vaughan, & Taylor, 2006).
Limitations
This pilot study had a number of limitations. Given the small sample size, the conclusions are only preliminary. Conversely, the lack of statistical differences could be due to a lack of statistical power. For example, despite the non-significant results, group comparisons between FTCEMOs and NSOs revealed medium effect sizes, Cohen’s d (Cohen, 1988), for FAS Total Score (d = 0.5); TMT-B (d = 0.5); and RCF Copy (d = 0.5); and a large effect size, (d = 0.9) for Hayling Total. Conversely, when significant group differences were found, the effect sizes were large (i.e., above 0.8 in ACE-R, FSIQ, Hayling Total, and Hayling Category A errors).
The major limitation of this study was the recruitment of FTCEMOs and the lack of reliability of information in prison files. Those individuals not previously charged or convicted of a sexual offence, who self-report that their first CEMO occurred after the age of 50, limit the reliable interpretation of the data. Given the confidentiality concerns in custodial settings, many offenders may be fearful that the information they provide could have negative social and legal repercussions for them. They are therefore likely to provide “selective” information regarding any other sexual offences committed.
Future Directions
The focus of this study was to investigate whether neuropsychological deficits could explain the sudden sexual offending of older adult First-Time CEMOs. The effect of age could be explored in future studies by including a comparison group of CEMOs who offended before the age of 50. Future studies with larger sample sizes have the potential to explore the association between cognitive deficits and sexual offending in older CEMOs.
Given the poor results in the majority of offenders in facial emotional recognition, the assessment of social cognition may be further enhanced by instruments such as the Faux Pas Recognition Test (Baron-Cohen, Jolliffe, Mortimore, & Robertson, 1997; V. E. Stone et al., 1998), the Theory of Mind Task Battery, Reading the Mind in the Eyes Test (Baron-Cohen et al., 1997; Baron-Cohen, Wheelwright, Hill, Raste, & Plumb, 2001), and/or the Prosody Perception Task (Borod, Welkowitz, & Obler, 1992). These measures, which are reliant on prefrontal areas (Dolan, 2007; Viskontas, Possin, & Miller, 2007), would evaluate whether CEMOs demonstrate empathy deficits, and may assist in determining whether CEMOs pose a risk of contact sexual offences against children, a concern that has received much interest (see Aslan, 2011).
Due to their lower rates of impulsivity, nonsexual and nonviolent offenders are more appropriate controls than those used in other studies. This study, therefore, shares the view of Joyal et al. (2007) that nonviolent offenders are more closely matched than antisocial, impulsive, and violent offenders.
Conclusion
The present study found little evidence that older FTCEMOs demonstrate greater neuropsychological deficits than older contact sex offenders and older NSOs. FTCEMO demonstrated high intellectual function and high verbal fluency, and no evidence of a neurocognitive disorder. Although, there were no group differences, the three groups demonstrated high impairment rates on the IGT and the FEEST, compared with norms, which suggest that offenders, regardless of offence type, demonstrate deficits in decision making and facial emotion recognition. It is therefore possible that such deficits are inherent in offenders regardless of offence type.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.