
Abstract
Adverse childhood experiences are associated with a multitude of health and social problems. In addition to an increased risk of poor health, mental disorders, and substance abuse, childhood maltreatment is also significantly related to adult violent offending. Although gender-specific analyses suggest that early childhood maltreatment precedes later violence for males across offense categories, it is unknown whether this association also applies to different types of female offenders. This study explores the types and quantity of adverse childhood experiences for two groups of violent female offenders: perpetrators of intentional homicide (N = 28) and perpetrators of sexual offenses (N = 47). A nonparametric analysis using odds ratios (OR) indicated that female homicide perpetrators experienced significantly more adverse childhood experiences (as measured by the Adverse Childhood Experiences Questionnaire) than female sex offenders. Implications for future research are discussed.
In addition to the numerous studies that found an association between adverse childhood experiences (i.e., early childhood trauma and dysfunctional households) and poor health outcomes (Anda et al., 2006; Centers for Disease Control and Prevention [CDC], 2013a; Felitti et al., 1998), there is also research identifying relationships between childhood maltreatment and later adult violent behavior (Reavis, Looman, Franco, & Rojas, 2013; Rossegger et al., 2009; Topitzes, Mersky, & Reynolds, 2012; Whitfield, Anda, Dube, & Felitti, 2003). Although the specific etiologies of this association are unknown at this time, various theoretical perspectives (e.g., neurobiological, social control, general strain, social learning, and integrated models) suggest a dose–response relationship between the number of adverse childhood experiences and later violent behavior mediated by various psychological and social characteristics (Anda et al., 2006; Topitzes et al., 2012; Mersky, Topitzes, & Reynolds, 2013).
In addition, this association appears to persist across gender (Levenson, Willis, & Prescott, 2015; Topitzes et al., 2012) and differing types or categories of violent behaviors (Levenson, Willis, & Prescott, 2016; Reavis, Looman, Franco, & Rojas, 2013; Whitfield, Anda, Dube, & Felitti, 2003). Despite a growing body of literature, however, there have been no empirically based studies that have examined whether the association between child maltreatment and later adult violent behavior is similar for women who have committed sexual offenses and women who have perpetrated homicide. Although the existing research on female perpetrated homicidal violence is limited, it is well established that women exhibit many unique psychological and behavioral characteristics, relative to males, for both general criminal and sexual offenses (Cortoni, 2010; Cortoni & Gannon, 2011, 2013; Cortoni, Hanson, & Coache, 2010; Pflugradt & Allen, 2011, 2013, 2015; Pizarro, DeJong, & McGarrel, 2010; Schwartz & Steffensmeier, 2007; Steffensmeier & Allan, 1995, 1996; Steffensmeier & Schwartz, 2004).
For example, Rossegger et al. (2009) found that compared with males, females who engage in violent behavior tend to be older, be married, have children, have higher rates of substance abuse, experience more physical and mental illness, have fewer prior convictions, have lower recidivism rates, and have lower rates of psychopathy. In addition, female violent offenders exhibit a different offense pattern relative to male offenders: (a) female violent offenses often involve someone close to them, within the context of interpersonal violence; (b) women are more likely to commit a violent crime at home; and (c) females most often offend violently during the perpetration of another crime. Moreover, female violent perpetrators are more likely to be current victims of physical, psychological, and sexual abuse, and 10 times more likely to have experienced childhood sexual abuse as compared with males (Rossegger et al., 2009).
In regard to homicidal behavior, women were four times more likely to commit murder during interpersonal conflict, that is, the victim is typically someone close to them rather than an acquaintance or stranger. Consequently, Rossegger and colleagues (2009) conclude that violent behavior perpetrated by females that results in death is not the result of antisocial personality traits but due to interpersonal conflicts. In similar research, Belknap (2015) expounded upon the factors that increase the likelihood that women will kill current or former intimate partners. Interestingly, the research indicates that the circumstances that trigger a woman to kill are related to the actions of her intimate partner. Belknap (2015) reported that women are more likely to kill their abuser when (a) the abuser physically and/or sexually abuses her children, (b) she perceives an increase and/or immediate sense of danger, and (c) she receives death threats and is terrorized by weapons. These empirical findings are consistent with early studies that proffered theoretical constructs to explain the female pathways to homicidal behavior (Belknap, 2015; Chesney-Lind & Pasko, 2013; Ogle & Jacobs, 2002; Ogle, Maier-Katkin, & Bernard, 1995).
For example, Ogle et al. (1995) proposed that female homicidal behavior is related to the strain of modern societies that results in negative “affect” or emotions. In general, women tend to internalize negative emotions as guilt and hurt instead of expressing it as anger toward a specific cause or person. Ogle and colleagues (1995) described this phenomenon as an “overcontrolled personality” that results in low rates of deviant behavior with occasional instances of extreme violence. They conclude that the conditions or strain associated with long-term abusive relationships and pre- or postpartum experiences are likely to produce these effects, that is, occasional episodes of severe violence. Although strain theories are helpful in explaining female homicidal behaviors within the context of sociocultural processes, they do not provide insights into how they occur within a battering relationship. Conversely, theories based upon pre- or postpartum experiences only apply to women who kill their children, that is, they only apply to specific cases and focus on psychological factors (Ogle & Jacobs, 2002).
In addition to strain and postpartum/psychosis perspectives, Ogle and Jacobs (2002) described another theoretical approach, the “battered woman syndrome” developed by Lenore Walker (1984). This theory posits that a battering relationship involves repeated cycling through three phases: (a) tension building, (b) acute battering incidents, and (c) contrition. Over time, the victim succumbs to learned helplessness, that is, she (or he) learns that the situation will not change despite her or his efforts; she essentially gives up and becomes a passive recipient of the abuse (Ogle & Jacobs, 2002). Although the cycle occurs repeatedly, Walker (1984) noted that it tended to change over time: The contrition phase lessens or disappears, the tension phase becomes longer, and the battering becomes more frequent and intense. Even though Walker did not elaborate upon why the cycle changed, Ogle and Jacobs (2002) indicated that according to studies, most battered women who kill reported feeling in constant survival mode while awaiting the next episode of potentially fatal violence.
Although this theoretical perspective has been widely accepted, it has several limitations. As suggested by Ogle and Jacobs (2002), it assumes psychological pathology of the victim, it does not explain how a woman who succumbed to learned helplessness suddenly defends herself in a lethal manner, it creates stereotypes of battery victims, and it does not address the influence of sociocultural factors and processes. As Ogle and Jacobs (2002) suggest, the cycle of battering may be best understood by combining Walker’s macrolevel approach with a microlevel interactional perspective that analyzes the ongoing exchanges and responses between the individuals involved in the battering relationship.
The application of a pathways perspective to female offending is a relatively recent research approach that examines whether women have distinct or unique pathways to crime as compared with men (Salisbury & Van Voorhis, 2009). In general, this pathways perspective recognizes that various realities or factors (e.g., biological, psychological, social) are unique to the female experience and form theoretical constructs that describe the course of female offending populations. Topitzes et al. (2012) tested the moderating effects of gender and examined “theory-informed” gender-specific mediators. In contrast to earlier research (Markarios, 2007), their results did not indicate that adverse childhood experiences significantly increased the risk for violence by females more than males. Rather, they found no significant “moderating effect” of gender on the association between childhood maltreatment and later adult violence. Despite the lack of a moderating effect, however, Topitzes and colleagues (2012) further reported that their results revealed that the pathways from early childhood victimization to later violent offending do differ across gender.
Although there is a well-established body of research examining the gendered offense pathways for female offenders (Salisbury, Van Voorhis, & Spiropoulos, 2009; Van Voorhis, Wright, Salisbury, & Bauman, 2010; Wright, Van Voorhis, Salisbury, & Bauman, 2012), there is a paucity of studies examining how they are behaviorally manifested. Such information could provide important information to establish treatment goals for trauma-informed care (Levenson et al., 2015). That is, if empirical investigation identifies an association between specific adverse childhood experiences and later adult behavioral pathways or patterns, then it may be possible to not only identify at risk persons but also provide more individualized interventions (Afifi & MacMillan, 2011). This is particularly important in regard to the differential effects of childhood abuse based upon gender, especially if such experiences increase the risk of female sexual and homicidal violence. For example, research has shown that by increasing the positive aspects of a child’s environment, risk may be mediated by promoting resilience (Benard, 1995; DuMonte, Spatz Widom, & Czaja, 2007).
This study compared two distinct groups of violent female perpetrators using a sample of female homicide perpetrators obtained by the authors and the sample of sexual offenders obtained and reported by Levenson and associates (2015) to explore the quantity and types of adverse childhood experiences. 1 The primary hypothesis is that women who commit intentional homicide experienced a greater number of adverse childhood experiences (ACE) than the general population. Moreover, a second hypothesis is that there is an association between the types of adverse childhood experiences of the study participants and their violent behavioral manifestations (i.e., homicide and sexual offenses).
In contrast to previous research in this area, which focused on identifying behavioral patterns from a single sample, this study compared two groups of violent offenders with distinct behavioral pathways (i.e., homicide and sexual assault). Consequently, a major assumption of this approach is that the effects of early child maltreatment result in distinctive adult behavioral manifestations that can be clearly differentiated between groups of violent offenders. This hypothesis further assumes that homicidal and sexual violence exhibited by female perpetrators originate from different psychological and/or neurobiological etiologies; that is, the divergent behavioral manifestations of violence are related to different adverse childhood experiences (Wilson et al., 2015).
Method
Measures
Adverse Childhood Experiences (ACE) Questionnaire
The adverse childhood experiences utilized by this study were operationalized using the Adverse Childhood Experiences Questionnaire constructed by Felitti and colleagues (1998) for the Adverse Childhood Experiences (ACE) Study (see appendix). The ACE Study is described as ongoing collaborative research between the CDC in Atlanta, Georgia, and Kaiser Permanente’s Health Appraisal Clinic in San Diego. 2 More than 17,000 Kaiser patients participating in routine health screening volunteered to complete the questionnaire designed to identify adverse childhood experiences. Felitti and colleagues (1998) developed and validated the ACE categories by using items adapted from earlier studies, including the Conflict Tactics Scale (Straus, Gelles, & Smith, 1990), the Child Trauma Questionnaire (Bernstein et al., 1994), and a survey by Wyatt (1985). If the respondents were ever exposed to adverse experiences as a child, that is, prior to the age of 18 years, they were instructed to indicate “yes” for each specific item. The number of “yes” responses was totaled, and an “ACE score” was obtained.
Although the ACE data continue to be analyzed, the results reveal a strong association between health, social, and economic risks and number of adverse childhood experiences, 3 that is, the higher the ACE score, the higher the risk for health and social problems. Moreover, the ACE study data were analyzed by gender, with 50.3% of women reporting one to three adverse childhood experiences, while 15.2% indicated that they experienced four or more. In comparison, 9.2% of the male respondents reported four or more adverse childhood experiences. 4
Participants
Although a matched control research design would have been preferable, there was not sufficient demographic information to determine confounding variables (Rose & van der Laan, 2009). Consequently, the participants of this study were obtained from three different samples comprised of female homicide offenders, female sex offenders, and a nonoffender community sample. The first group of participants for this study was a sample of 28 female offenders incarcerated in a medium/maximum security prison, whose index offense was first-degree intentional homicide. This was a convenience sample that included all of the offenders who volunteered to participate in the study. They were identified during record reviews by a psychology intern with a master’s degree under the supervision of the principal investigator. The inclusion criteria specified were that the females’ index offense was intentional homicide or that they were initially charged with intentional homicide. Of the 30 female offenders who qualified to participate, 28 agreed to participate in the research project. All but two of the participants were convicted of first-degree intentional homicide; two participants were initially charged with first-degree homicide that was later reduced to a second-degree intentional homicide conviction during the legal process. None of these participants were ever charged or convicted of a sexual offense.
The second sample was obtained from a study published by Levenson and colleagues (2015), which compared the ACE of 47 adult female sex offenders with the CDC female sample and a sample of male sexual offenders. As reported, they obtained a convenience sample of participants surveyed in outpatient and secure sex offender treatment programs across the United States, recruited from a professional listserv. The responding therapists from these programs agreed to become data collection sites and invited their clients to participate in the study. In regard to the specific characteristics of the sample, Levenson and associates (2015) reported that the majority of their sample was Caucasian (76%) and most were between the ages of 30 and 60 years (66%).
Most earned a high school diploma or graduate equivalency diploma (53%), with 30% of the participants reporting a college degree. In the last years of earned income, 58% reported earning less than $30,000 per year. In regard to marital status, 53% were divorced or separated, 15% were currently married, and 30% had never been married. Levenson and colleagues (2015) further reported other offender characteristics (e.g., total sex crime arrests, total victims, total nonsex arrests, months in treatment, lifetime months in prison, lifetime months on probation) and offense characteristics (e.g., use of force, use of weapon, caused injury) and victim characteristics (e.g., age, gender, relationship to female offender). None of these participants were ever charged or convicted of homicide, with 80% reporting a history of nonsex arrest.
The third sample was obtained from The CDC-Kaiser Permanente ACE Study, which is one of the largest studies of the association between childhood abuse/neglect and health and well-being in later life. 5 The initial ACE Study was conducted from 1995 to 1997 at Kaiser Permanente, involving two periods of data collection. More than 17,000 Health Maintenance Organization members in Southern California completed confidential surveys regarding their childhood experiences 6 and current health status and behaviors. 7 The completed medical evaluation for every eligible person included his or her medical history, laboratory results, and physical findings. For the entire ACE Study sample (N = 17,337), 54% were women, and 74.8% reported their race/ethnicity as White. In addition, most of the participants (46.4%) were 60 years or more, and 39.3% had a college degree or higher.
Procedure
Upon receiving approval from the Department of Corrections Institutional Review Board, the offenders who fulfilled the inclusion criteria were sent an invitation to participate in the research study. Informed consent was obtained for each of the 28 volunteers who were then provided with an ACE Study Questionnaire and instructed on how to complete it by a predoctoral psychology intern. The participants were asked to complete it in her presence; the entire data collection process occurred over a 12 month period. As previously stated, all the participants volunteered to participate and were not compensated for their participation. The completed questionnaires were then given to the principal investigator who transposed codes to replace all identifying information to ensure confidentiality.
Analysis
The data were analyzed using OR, which is a measure of association between an exposure or event(s) and an outcome. The OR represents the odds that an outcome will occur given a particular exposure compared with the odds of the outcome occurring in the absence of that exposure (Daniel, 2009). An OR analysis was used to compare the relative odds of individual adverse childhood experiences between the group of homicide perpetrators and two other groups, that is, the female sexual offenders reported by Levenson and associates (2015) and the normative CDC sample.
Results
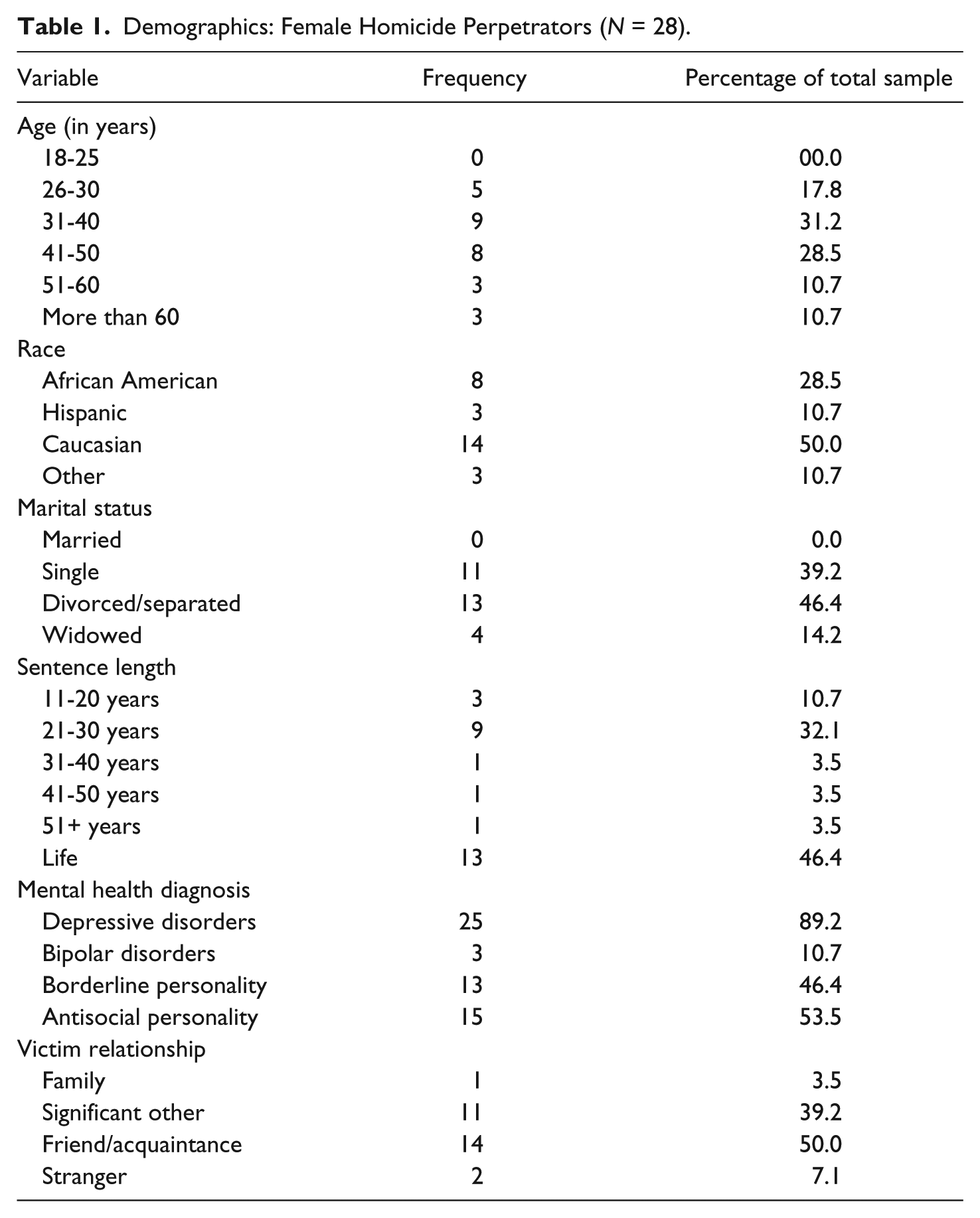
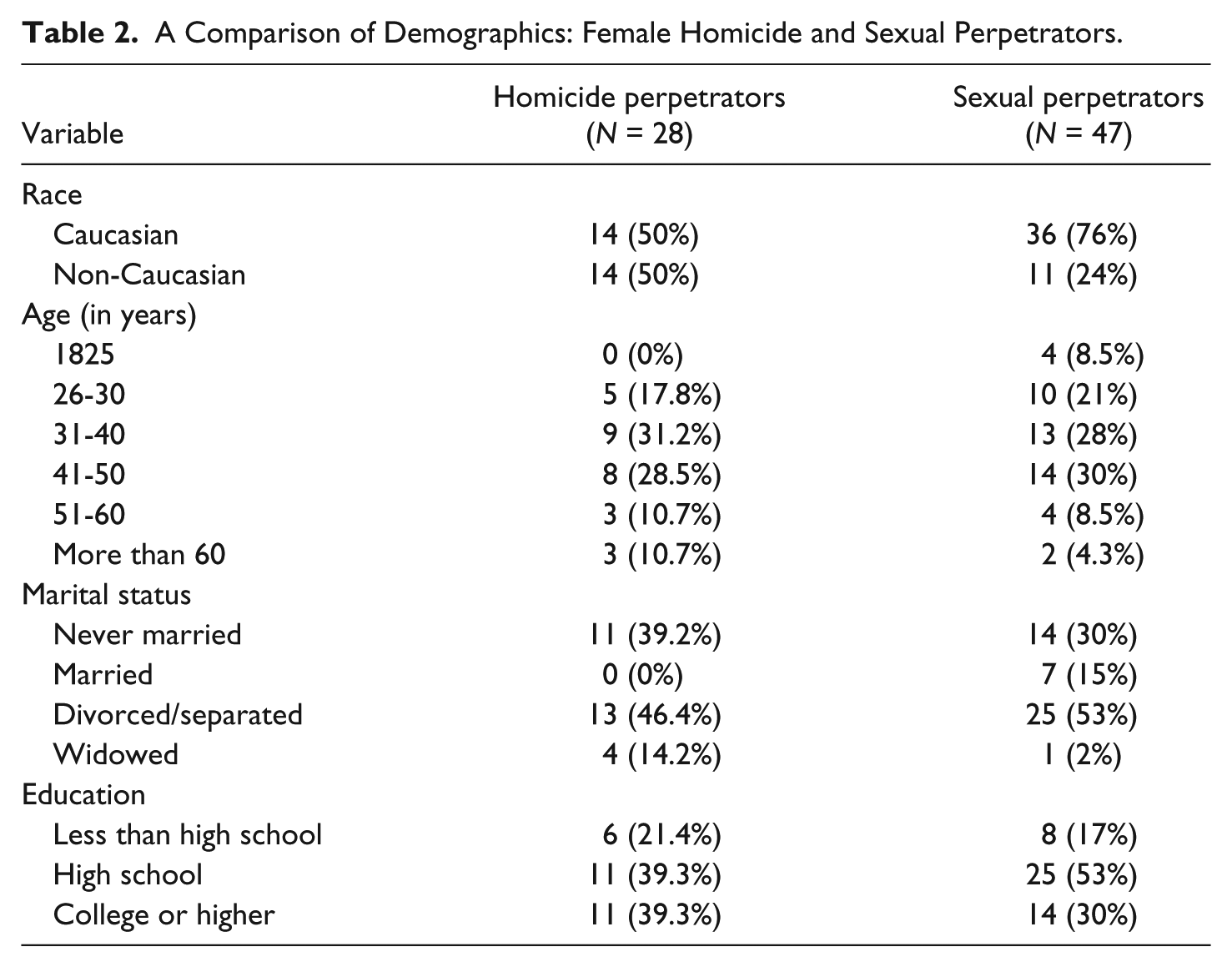
The mean age of the study participants was 42.5 years (SD = 11.8 years) and ranged from 26 to 66 years. As illustrated in Table 1, the majority of the participants were either Caucasian (n = 14) or African American (n = 8) and were single (n = 11) or divorced/separated (n = 13). In addition, relatively fewer participants had mothers (n = 5) or fathers (n = 6) with a history of felony offenses. The participants’ sentences were varied, although most had either a sentence of 21 to 30 years (n = 9) or a life sentence (n = 13). Moreover, most participants had a history of felony criminal offenses (n = 19) and substance abuse (n = 18), with 16 reporting that they were using substances at the time of their index offense. The victims included significant others (n = 11), friends/acquaintances (n = 14), strangers (n = 2), and family members (n = 1). Victim ages ranged from 2 to 92 years, with a mean of 43.9 years (SD = 21.6 years). Interestingly, a significant number, slightly more than half of the participants, committed the offense with a co-offender (n = 16), which is consistent with some of the research on female sexual offenders (Budd, Bierie, & Williams, 2017; Vandiver, 2006). In general, as seen in Table 2, the demographic characteristics of the homicide offenders were similar to those of the sex offenders reported by Levenson and colleagues (2015).
Demographics: Female Homicide Perpetrators (N = 28).
A Comparison of Demographics: Female Homicide and Sexual Perpetrators.
Although 20% of the sexual offenders and 35% of the CDC sample reported zero ACE, the entire sample of homicide perpetrators reported at least one adverse childhood experience. The majority of participants who were convicted of homicide (82%) reported four or more ACE, with 71% reporting five or more; the mean of the ACE total scores is 5.9 (SD = 2.6). This result is compared with 41% of the sexual offenders and 15% of the general female population reporting four or more ACE. As presented in Table 3, the mean scores for each of the individual ACE domains for the female homicide perpetrators are Abuse = 1.92 (SD = 1.08), Neglect = 1.28 (SD = .76), and Dysfunctional = 2.71 (SD = 1.32).
ACE Scores (N = 28).
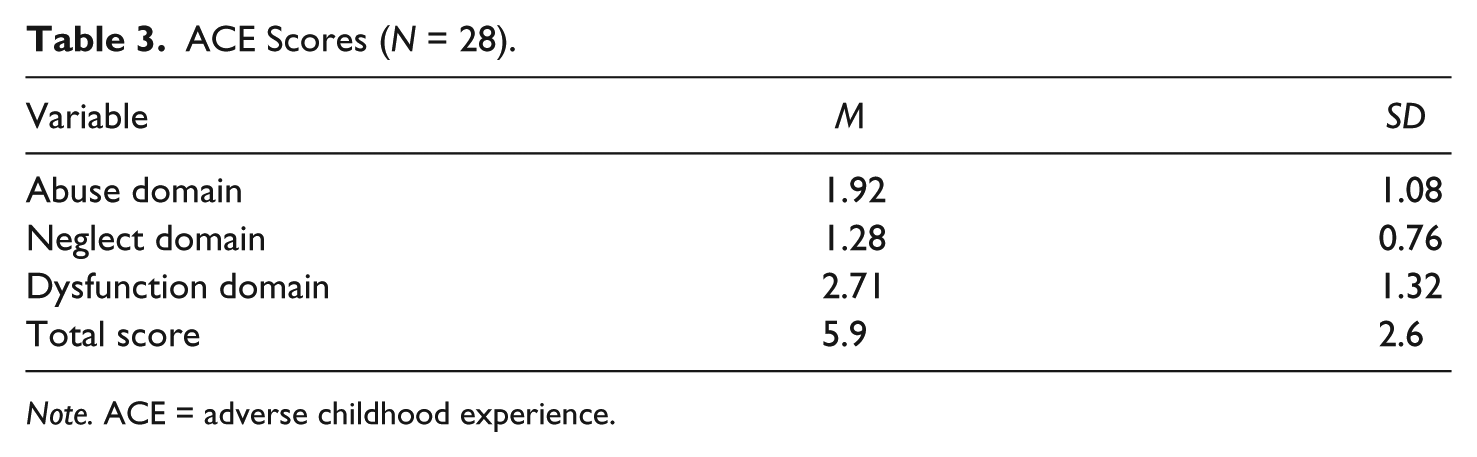
Note. ACE = adverse childhood experience.
When compared with the general female population or CDC sample using an OR analysis, the homicide participants reported significantly more (p < .01) ACE across all of the individual items. In comparison with the sexual offenders, significantly more homicide offenders endorsed verbal/emotional abuse, physical abuse, emotional neglect, physical neglect, substance abuse, and mental illness in the home. When examining the domains, the female homicide perpetrators reported a significantly greater number of ACE for all types of abuse and neglect (except for sexual abuse) and a higher incidence of the dysfunctional domain items substance abuse and mental illness in the home.
Discussion
The results of this exploratory study support the hypothesis that women who were convicted of homicide experienced a greater proportion of adverse childhood experiences than women in the general population. While 35% (n = 3,231) of the CDC sample reported zero adverse childhood experiences, 100% (n = 28) of the homicide perpetrators endorsed at least one adverse childhood experience. In addition, 82% (n = 23) of the participants who committed homicides reported four or more adverse childhood experiences (with 20, or 71%, reporting five or more), as compared with 15% (n = 1,423) of the general female population. In regard to individual ACE items, OR analyses resulted in a significantly greater proportion of homicide perpetrators (p < .001), endorsing each of the questionnaire items. Although the significant differences in self-reported ACE between female homicide offenders and women in the general population are expected, the magnitude of the childhood maltreatment was not. The majority of homicide offenders reported five or more total ACE, and at least half endorsed all but two of the 10 items. Another notable result was the large standard deviations for the total scores in each of the domains (especially the abuse and dysfunction domains), suggesting wide variability in regard to the types of ACE among the individual participants.
Comparable with other research, these results suggest a similar dose–response relationship; that is, the more the ACE, the greater the likelihood of female perpetrated violent behavior. From this perspective, the question then becomes as follows: “How an increased number of ACE relates to an individual’s propensity to engage in acts of future homicidal and sexual violence?” Perhaps one of the most discernable explanations is that early childhood maltreatment is associated with significant mental health issues and substance abuse (Anda et al., 2007; Anda et al., 2002; Chapman et al., 2004; Edwards, Holden, Anda, & Felitti, 2003). The findings presented here are consistent with this hypothesis insofar as the majority of participants were diagnosed with mental disorders (e.g., depressive and personality disorders) and reported issues with substance abuse.
When asserting this possible association, however, it is important to consider whether the ACE caused a mental disorder that led to violence or the propensity to develop a mental illness was preexisting and activated or exacerbated by ACE. Despite the issue of causality, however, this comparison between the ACE experienced by the homicide perpetrators and general female population suggests a relationship between the magnitude of early childhood maltreatment and the development of adult mental illness and/or substance abuse. Whether the increased prevalence of these disorders leads to some individuals engaging in behavioral manifestations of violence is unclear; most women with mental disorders and/or substance abuse issues do not engage in homicidal behavior.
These results also support the second hypothesis; there appears to be an association between the adverse childhood experiences of the participants and their differing behavioral manifestations or pathways. Although both samples reported more ACE than the general population, the homicide perpetrators endorsed significantly more early adverse childhood experiences than the sex offenders. As illustrated in Table 4, homicide offenders endorsed a greater frequency of all but four of these items (i.e., sexual abuse, parents separated/divorced, domestic violence in the home, and incarcerated family member). In addition, at least half of the participants who committed homicide reported all but two ACE (i.e., domestic violence in the home and incarcerated family member). In comparison, below 50% of the female sexual perpetrators reported nine of the ACE items; half reported experiencing sexual abuse as children. It should be further noted, however, that there were some similarities as both the homicide and sexual perpetrators reported a comparable proportion of ACE for four items—sexual abuse, parents separated/divorced, and domestic violence—suggesting that all the participants grew up in unstable households with sexual abuse and domestic violence.
ACE Item Comparisons and OR Between Homicide and Sexual Offenders.

Note. ACE = adverse childhood experience; OR = odds ratio.
Data were taken from Levenson, Willis, and Prescott (2015). The frequency of participants for each ACE item was converted from percentages and rounded to nearest whole number.
In addition to supporting the research hypotheses, these findings also suggest that the homicide perpetrators and sexual offenders shared some common early childhood experiences. That is, a similar proportion of participants from each group reported the ACE of sexual abuse, parents separated/divorced, domestic violence in the home, and an incarcerated family member. Thus, despite differing behavioral manifestations, these results suggest that later adult violence, of any type, may be more likely when a female is raised within an abusive (i.e., especially sexually abusive), dysfunctional household (Cubellis, Peterson, Henninger, & Lee, 2016). Of the results obtained from this study, this particular finding offers an important consideration for future research. That is, it raises questions about whether the influences of abusive, dysfunctional households are a common criminal pathway for all children, especially those who engage in violent behavior as adults.
The association between ACE and later behavioral manifestations is an important factor to consider when discussing the prevention of adult violence. That is, changing aspects of a child’s environment in a positive manner to promote resilience provides him or her with the support he or she requires to recover from the effects of ACE (Benard, 1995; DuMonte, Spatz Widom, & Czaja, 2007). As proposed by Benard (1995), these positive environmental aspects or protective factors include caring and supportive relationships, high positive expectations, and opportunities for meaningful participation. That is, the presence of at least one supportive person in a child’s life facilitates healthy development and promotes learning while motivating her or him to achieve. In addition, schools that adopt high positive expectations and provide the resources to achieve them have higher rates of academic success and fewer behavior problems. And finally, meaningful participation promotes responsibility and a sense of autonomy, which is an important component of resilience.
Due to the small samples explored in this study, there are numerous limitations that must be considered. Perhaps the most obvious is the issue of generalizability or the ability to draw conclusions from a limited number of participants. The base rates for female perpetrated crimes, especially homicide and sexual offenses, are smaller relative to male offenders (Cortoni et al., 2010; Federal Bureau of Investigation Uniform Crime Reporting, 2014). As a result, empirically based studies are limited to qualitative and quasi-experimental designs that are often exploratory in nature, which are intended to generate hypotheses or operationalize theoretical constructs. Second, a possible confounding variable is that about 75% of women who commit homicide are also victims of domestic violence (Campbell, 2007). Although the participants of this study also reported some history of domestic maltreatment, the magnitude of adult violence perpetrated against them was unknown. Consequently, there may be an interactive effect between childhood and adult experiences that was not examined by this study.
As the research on the effects of early childhood trauma continues to develop, it will be important to maintain a focus on female offenders who are all too often overlooked as resources are allocated to the vastly greater number of male offenders. Although such decisions are typically based upon misperceptions that males are more dangerous or threatening (Pflugradt & Allen, 2011), appropriately treating and supporting female trauma survivors will have a significant positive societal impact. To adequately address the effects of ACE on female adult violence, however, the association between early traumatic experiences and the later development of mental illness, substance abuse, and relationship problems for women is a critical consideration when designing services that are comprehensive, integrated, and efficacious (Covington, 2007; Covington & Bloom, 2007; Levenson et al., 2015). That is, services should be responsive to gender differences, and specifically designed to address the psychological, behavioral, social, and etiological differences in criminal pathways for women (Covington & Bloom, 2007; Levenson et al., 2015; Topitzes et al., 2012).
In addition, it is important to understand how these factors are interrelated and direct the services within both institutional and community-based settings (Levenson et al., 2015). That is, effective services must provide for fundamental needs such as housing, medical and mental health care, child care and parenting services, financial self-sufficiency, and support systems that target the needs of each individual. Thus, in spite of the devastating effects of ACE, there are several empirically identified protective factors that may be used to promote individual resilience. The future challenge, however, will be to effectively apply these factors within an individual treatment context. Consequently, it appears that if the effects of dysfunctional family environments can be mediated with resiliency facilitated through effective programs and treatment, the detrimental effects of ACE could be avoided and, for some individuals, resolved.
Footnotes
Appendix
Acknowledgements
The authors would like to thank theWardenand the staff at Taycheedah Correctional Institution for their assistance with this project. The authors would also like to thank Jill Levenson for allowing us to use her results for comparison in this study.
Authors’ Note
The views expressed in this article are those of the authors and do not necessarily represent the views of the Department of Corrections, Department of Health Services or St. Joseph Hospital.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.