
Abstract
Prisoners represent a group containing the highest problem gambling (PG) rate found in any population. PG is of particular concern among Indigenous Australians. Little data exist concerning PG rates among Indigenous Australian prisoners. The present study aimed to address this gap in the literature by examining the lifetime prevalence of PG among male prisoners, whilst identifying prisoners of Aboriginal background. The EIGHT Gambling Screen (Early Intervention Gambling Health Test) was administered to 296 prisoners across three male prisons in South Australia. Previous help-seeking behaviour and forms of gambling were also examined. Sixty percent of prisoners indicated a lifetime prevalence of PG with 18% reporting they were incarcerated due to offending relating to their gambling problem. Indigenous Australian prisoners indicated a significantly higher prevalence of PG (75%) than non-Indigenous prisoners (57%) and reported less than half the rate of help-seeking. Given the high levels of PG and overall low rates of help-seeking among prisoners, prisons may provide an important opportunity to engage this high-risk population with effective treatment programs, in particular culturally appropriate targeted interventions for Australian Indigenous prisoners.
Introduction
Problem gambling (PG) is associated with significantly harmful personal and social impacts such as occupational loss, family breakdown, and suicide (Productivity Commission, 2010). The Australia’s Gambling Industry’s Report (Productivity Commission, 2010) estimates that the number of problem gamblers in Australia over a 12-month period lies around 115,000, with a further 280,000 at moderate risk, comprising around 2% of the population. In addition, for every problem gambler, five to 10 others such as partners and children are also adversely affected (Productivity Commission, 2010). It is further reported that problem gamblers contribute 40% of all electronic gaming machine losses (Productivity Commission, 2010). The report states that the number of people who have ever experienced problems with gambling, that is lifetime prevalence, is considerably higher (around double) than annual prevalence estimates.
To clearly define PG, Shaffer, Hall, and Vanderbilt (1999) devised a three-level system to differentiate PG severity. Level 1 represents individuals who do not have a gambling problem. This includes both non–problem gamblers and nongamblers. Level 2 represents subclinical levels of pathological gambling which include “problem” gamblers, “potential pathological” gamblers, and “at-risk” gamblers. Level 3 represents the most severe level of problem, or “pathological,” gambling. Researchers have highlighted the need for further research to focus on “at-risk” populations who may experience a higher prevalence of gambling problems than the general population (Lahn & Grabosky, 2003). Criminal offenders who are incarcerated for their crimes represent a group containing the highest PG rate found in any population (Williams, Royston, & Hagen, 2005).
Gambling and Crime
Blaszczynski and Nower’s (2002) Pathways Model of Problem and Pathological Gambling suggests three subtypes of problem gamblers: (a) behaviourally conditioned problem gamblers, (b) emotionally vulnerable problem gamblers, and (c) antisocial impulsivist problem gamblers. The model suggests problem gamblers with a history of impulsivity engage in a broad range of behavioural problems independent of their gambling, including criminal offending. Thus, there is a substantial crossover among variables associated with both PG and criminal behaviour, resulting in a complex relationship between gambling and crime (Abbott, McKenna, & Giles, 2005). Given such versatility among antisocial impulsivist problem gamblers and criminal offenders in general, prisoners with histories of PG may or may not be incarcerated due to offending relating to excessive gambling. There is a lack of research examining the rate of prisoners with histories of PG who possess a nexus between their offending and PG. This study aims to address this gap in the literature, whilst identifying prisoners of Indigenous Australian backgrounds.
Choice of a Lifetime Instrument
Pathological gambling is considered a chronic rather than an acute disorder and therefore poses a lifetime vulnerability (Volberg, 2002). As such, measuring lifetime prevalence of PG, rather than PG within a specific time period, such as the previous 1 or 3 months, is important. Understanding lifetime prevalence can inform us about an individual’s or population’s vulnerability. This is particularly useful for prison populations, given the high rate of comorbidity of mental health disorders among pathological gamblers (Petry, Stinson, & Grant, 2005) and prison populations in general (Sirdifield, Gojkovic, Brooker, & Ferriter, 2009).
A survey conducted by Queensland Corrective Services (Queensland Government, 2002) reported almost half (46.1%) of prisoners surveyed admitted to gambling whilst in custody. Furthermore, another Australian study in Queensland reported that the majority of prisoners (81%) had engaged in gambling behaviour post release, with one in five reporting either moderate risk or PG (Kinner, 2006). Given these high rates of gambling behaviour among prisoners during incarceration and post release, along with reported high relapse rates among problem gamblers who have quit (Tepperman, Korn, & Reynolds, 2006), understanding the lifetime prevalence among this population can help to determine the need for health promotion, early intervention, treatment interventions, and relapse prevention strategies.
PG Prevalence Among Male Australian Prisoners
During the last two decades, six PG prevalence studies have been reported focusing on male offender populations in Australia: one in Western Australia, two in Queensland, two in South Australia, and one in the Australia Capital Territory (Australian Institute of Gambling Research, 1996; Jones, 1989; Lahn & Grabosky, 2003; Marshall, Balfour, & Kenner, 1997; Queensland Government, 2002; Riley & Oakes, 2014). Reported prevalence rates range between 12% and 52% depending on whether Level 2 or 3 gambling was reported and the type of measure used, for example, the previous 6 months prior to imprisonment or lifetime prevalence.
Of the six PG prevalence studies focusing on offender populations in Australia, four have examined lifetime prevalence. Jones (1989) surveyed 60 male adult offenders in a remand centre in Western Australia using the South Oaks Gambling Scale (SOGS) (Lesieur & Blume, 1987) lifetime tool (SOGS-LT). Twenty-two percent indicated a lifetime prevalence of Level 3 gambling. Level 2 gambling was not reported. The Australian Institute for Gambling Research (1996) distributed a gambling questionnaire (developed specifically for their study) to 550 adult male offenders in a South East Queensland prison. Seventy-four prisoners completed the survey with a response rate of 13.5%. Thirty-one percent reported they had experienced personal or financial problems because of their gambling with 7% reporting that their current offence was related to obtaining money to gamble on gaming machines. However, the low response rate needs to be taken into consideration, and levels of gambling were not reported. The Australian National University Centre for Gambling Research (Lahn & Grabosky, 2003) surveyed 102 adult offenders serving weekend sentences whilst in remand in the Australian Capital Territory, using the SOGS-LT. The sample was predominantly male (95.1%) consistent with the gender of admissions during the study period. Seventeen percent reported Level 2 gambling with a further 34% reporting Level 3 gambling, indicating 51% of the prison population had a lifetime prevalence of either problem or pathological gambling. Gender breakdown of PG was not reported. Riley and Oakes (2014) found a similar lifetime prevalence (52%) of PG (Levels 2 and 3) when surveying 105 male prisoners in South Australia using the EIGHT Gambling Screen (Early Intervention Gambling Health Test; Sullivan, 2007).
The limited available data concerning PG among First Nations people in Australia suggests prevalence rates are substantially higher than for the general Australian population (Breen & Gainsbury, 2013). A recent Australian study found that almost two thirds (63.4%) of Indigenous Australians who completed the Problem Gambling Screening Index (PGSI; n = 964) indicated they were at some risk from their gambling behaviour during the previous 12 months, with around one quarter having a serious problem (Hing, Breen, Gordon, & Russell, 2014b). Furthermore, help-seeking rates among Indigenous Australian problem gamblers are very low, as they are with the general Australian population (Hing, Breen, Gordon, & Russell, 2014a). Hing et al. (2014a) reported that 5.4% of Indigenous Australians who had participated in any type of gambling during the previous 12 months had sought help for their problems, including from informal sources such as family and friends. There is a further dearth of data concerning the prevalence rates of PG among Indigenous Australian prisoners. This is surprising given that despite Indigenous Australians comprising just 2.8% of the Australian population (Australian Bureau of Statistics [ABS]; 2016a), they make up more than a quarter (27%) of our Australian prison population (ABS, 2016c), and high rates of PG have been reported among Indigenous Australian populations in general (Hing et al., 2014b). In Australia, First Nations people are grossly overrepresented at all stages of the criminal justice system (Nettheim & McRae, 2009), and alarmingly, the Indigenous adult imprisonment rate has increased 77% between 2000 and 2015 (Steering Committee for the Review of Government Service Provision [SCRGSP], 2016). A 2002 report by the Queensland Government indicated a higher percentage of Indigenous Australian prisoners were moderate risk or problem gamblers (30.7%) during the previous 12 months compared with non-Indigenous prisoners (19.7%) (Queensland Government, 2002). A more recent report in 2013 by the Victorian Foundation for Responsible Gambling (Perrone, Jansons, & Morrison, 2013) revealed 57.1% of Indigenous prisoners were moderate risk or problem gamblers during the previous 12 months compared with 11.7% of their non-Indigenous counterparts. At the time of this writing, the present authors could not locate any published data concerning lifetime prevalence of PG among Indigenous Australian prisoners.
Aims of the Current Study
This study had three main aims. The first aim was to investigate the lifetime prevalence of PG among a group of male prisoners across three prisons in South Australia. The second aim was to examine forms of gambling causing problems and previous help-seeking behaviours among respondents. The third aim was to examine these variables among Australian Indigenous prisoners.
Method
The PG prevalence survey took place across three (two low and one medium security) correctional facilities in South Australia.
Ethics approval was received by the Southern Adelaide Clinical Human Research Ethics Committee to undertake the study, and prison management was supportive across all sites. Prisoners were invited to participate in the study via the prison newsletter and fliers placed in common areas of each prison. On the day of the survey, a table was set up in a common area within each prison, containing pencils and a sealed ballot box for completed surveys. A 2-hr period was available for prisoners to attend once they had been notified by prison staff. On arrival, participants were given the EIGHT Gambling Screen (Sullivan, 2007), a valid simple and brief lifetime PG screening tool originally designed for use by GPs, but has since been used in more generalized populations including prisons (Sullivan, 2007; Sullivan, Brown, & Skinner, 2008). The EIGHT Gambling Screen correlates with other accepted PG screening tools such as the SOGS (Lesieur & Blume, 1987) and assessment by clinicians using Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) pathological gambling criteria, and has high internal consistency (Cronbach’s alpha of .97; Sullivan, 2006). In addition, it has the advantage of being short, with only eight questions compared with 16 on the SOGS, and easy to score with only two responses compared with four on some SOGS items (Sullivan, 2006). Furthermore, it has been validated among a range of cultures and settings including prisons (Sullivan, 2007). A score of 6 or more has been recommended to identify Level 3, or pathological gambling, a score of 4 or 5 to identify Level 2 gambling, and a score of 2 or 3 is suggested as identifying potential participants for health promotional purposes or brief interventions (Sullivan, 2006).
The survey contained three questions in addition to the EIGHT Gambling Screen items, relating to participants’ gambling. The questions were “Is your current conviction related to gambling in any way?” “Have you ever sought help for any of these issues” “If you have experienced any of these issues what type of gambling was involved?” The first two additional questions invited a yes/no response. The final question presented five selections: pokies, TAB (horses, dogs, sports), keno 1 , casino games, and other, and invited respondents to mark the form of gambling that had caused them problems. More than one form of gambling could be selected. The survey was presented to participants by two investigators and then placed by participants in the sealed ballot box once completed. The sealed box was not opened in the prison to ensure that the investigators would be seen as independent from the prison authorities. The only demographic information collected was age and Aboriginal and/or Torres Strait Islander status. Limited sociodemographic data were collected so as to collect as little personal information as possible. Preserving anonymity has been found to increase honest responding to sensitive questions (Ong & Weiss, 2000); therefore, it was believed that preserving anonymity would increase both the validity of data and response rate. All participants were invited to speak confidentially with the prison institutional social workers if they wished to discuss any gambling-related issues.
Results
Analyses were performed using PASW Statistics 22. Prior to analyses, data screening was performed. Inspections of histograms, residuals scatter plots, and diagnostic tests indicated the data were normally distributed and met assumptions for parametric testing.
Response Rate
On the day of administration, there were a total of 450 prisoners available to take part in the survey across the three prison sites (219 prisoners in the low and 231 in the medium security facilities). The total number of surveys completed was 296 leaving us with an overall response rate of 66%. The response rate was comparable between the low- and medium-security facilities (68% and 63%, respectively). The mean age of respondents was 37.70 (SD = 11.08, Mdn = 37). Fifty-seven respondents (19%) identified as being of Aboriginal and/or Torres Strait Islander descent. The mean age for Indigenous respondents was 36.98 (SD = 9.82, Mdn = 36) and non-Indigenous respondents 37.86 (SD = 11.43, Mdn = 37).
PG Prevalence
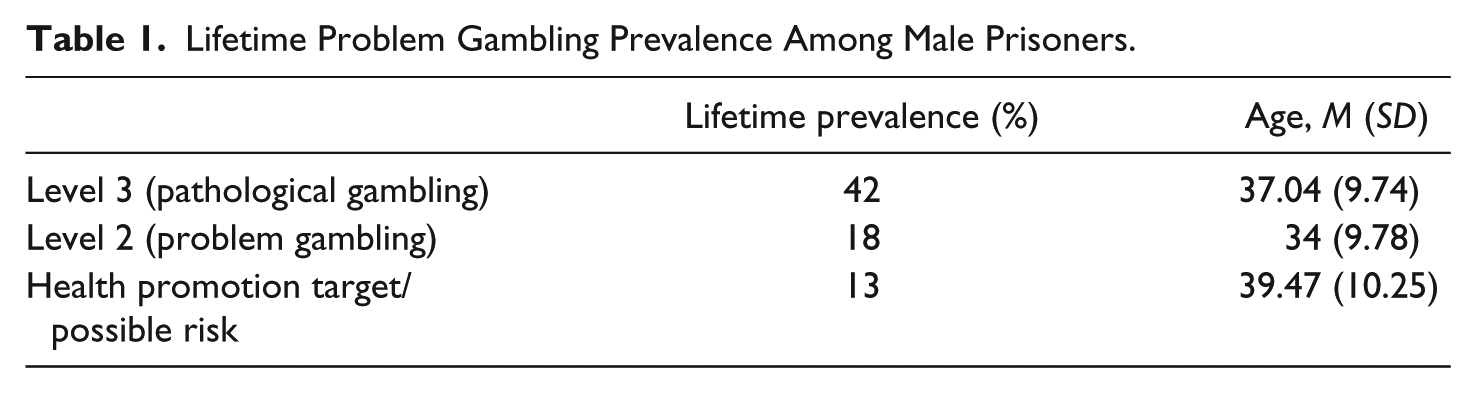
As presented in Table 1, 60% of respondents indicated a lifetime prevalence of PG with the majority of those pathological, and a further 13% of respondents scoring a 2 or 3 indicating they would benefit from a health promotion intervention concerning PG.
Lifetime Problem Gambling Prevalence Among Male Prisoners.
Forms of Gambling Causing Problems
The most frequently reported form of gambling among male respondents who scored in the PG range was electronic gambling machines (pokies) followed by casino games, TAB betting, keno, and then “other” which comprised private poker, Internet blackjack, and bingo. Table 2 presents the forms of gambling causing problems as reported by respondents with lifetime PG (respondents could choose more than one type of gambling as causing them problems). Forms of gambling were then examined with respect to gamblers who indicated one form of gambling as causing them problems, and those who indicated 2 or more forms as causing problems. These data were collapsed to form a new variable with 2 levels: multigamblers and non-multigamblers. Ninety-seven (54%) of Level 2 and 3 problem gamblers were multigamblers. A chi-square test revealed no significant difference in the proportion of multigamblers across Level 2 and 3 problem gamblers.
Forms of Gambling Causing Issues for Respondents.
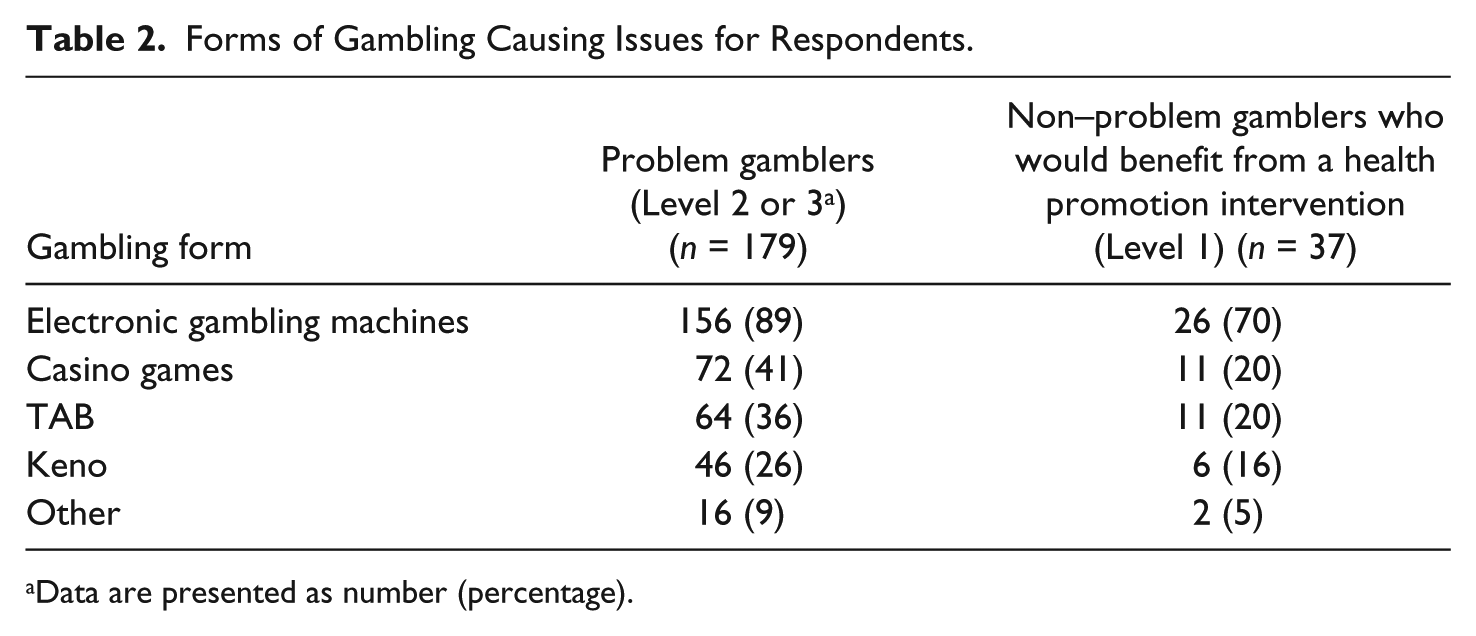
Data are presented as number (percentage).
Current Imprisonment and PG
Of the total respondents (N = 296), 53 (18%) reported their current term of imprisonment was related to gambling issues. Of the self-reported pathological gamblers (Level 3), 40% reported their current imprisonment was related to their gambling problem. A chi-square test was performed to determine whether gambling-related convictions were distributed evenly across levels of PG. Level 3 gamblers were significantly more likely than Level 1 or 2 gamblers to report their current conviction was related to gambling, χ2(3, N = 296) = 73.57, p < .001. An independent-samples t test was then performed to compare EIGHT Gambling Screen scores between Level 3 gamblers who were incarcerated for offending related to their gambling problem, and Level 3 gamblers who were incarcerated for offending unrelated to their gambling problem. EIGHT Gambling Screen Scores were significantly higher among gambling-related offending pathological gamblers (M = 7.69, SD = 0.69) than non–gambling-related offending pathological gamblers (M = 7.07, SD = .10); t(125) = −4.07, p < .001.
Previous PG Help-Seeking
Help-seeking was examined for prisoners who scored in the PG range (n = 179). Forty-five (25%) respondents reported having previously sought help for their gambling problem. Of these help-seekers, the vast majority (86%) were Level 3 gamblers.
Sociodemographics
Age and Indigenous status were examined with respect to PG behaviour.
Age
Age was negatively correlated with the EIGHT Gambling Screen, r(294) = –.14, p = .015, implying younger males had higher lifetime PG. Age was then examined with respect to forms of gambling. Respondents who reported TAB gambling as a problem were older (M = 39.46, SD =10.29) than non-TAB gamblers (M = 34.93, SD = 9.20), t(221) = −3.31 p = .001, and respondents who reported casino gambling as a problem were younger (M = 34.08, SD = 10.56) than noncasino gamblers (M = 38.38, SD = 8.11), t(220) = 3.35 p = .001. Respondents who reported having previously sought help for their gambling problem were younger (M = 34.60, SD = 9.08) than non–help-seekers (M = 38.34, SD = 11.33), t(282) = 2.09, p = .037.
Aboriginal and/or Torres Strait Islander Status
Respondents who identified as being of Australian Indigenous origin had significantly higher mean lifetime PG scores (M = 5.16, SD = 2.79) than non-Indigenous respondents (M = 4.06, SD = 3.06), t(291) = −2.40, p = .017. There was no significant difference in age between the Indigenous and non-Indigenous groups. A series of chi-square tests were then performed to determine whether the proportion of lifetime PG, help-seeking behaviour, gambling-related convictions, and forms of gambling were distributed evenly between Indigenous and non-Indigenous prisoners. The proportion of lifetime problem gamblers (Level 2 or 3) was significantly greater in the Indigenous group (75%) than in the non-Indigenous group (57%), χ2(1, N = 293) = 6.40, p = .015. Among respondents who reported Level 1 or 2 PG, there was more than twice the proportion of previous help-seeking behaviour among the non-Indigenous group (29%) than the Indigenous group (14%), χ2(1, N = 179) = 3.85, p = .035. There was no significant difference between the groups concerning the proportion of problem gamblers who reported their current imprisonment was related to a gambling problem.
Forms of gambling were then examined to investigate any differences between the Indigenous and non-Indigenous groups. Statistically significant differences were found for TAB gambling and electronic gambling machines. There was a larger proportion of respondents who reported TAB gambling as causing problems (38%) among the Indigenous group than in the non-Indigenous group (27%), χ2(3, N = 286) = 9.15, p = .027, and a slightly lower proportion of respondents who reported electronic gambling machines as causing problems in the Indigenous group (66%) than in the non-Indigenous group (69%), χ2(2, N = 286) = 9.50, p = .009.
Security Setting
A chi-square test was performed to determine whether PG prevalence was distributed evenly between low- and medium-security prisons. The proportion of lifetime problem gamblers was significantly greater in the medium-security setting (72%) than in the low-security setting (49%), χ2 (1, N = 296) = 15.79, p < .001.
Discussion
These data are consistent with existing literature and confirm an extraordinarily high rate of PG among this prison population. Almost two thirds of all prisoners surveyed (N = 296) reported that they had experienced a significant gambling problem at some time in their life, 16 times higher than would be expected in the general Australian population (Productivity commission, 2010). Furthermore, one in five male prisoners reported that their current term of imprisonment was related to a gambling problem. This result is similar to a previous study in South Australia (Riley & Oakes, 2014). With a rate of one in five incarcerated men indicating their current custodial sentence was related to a gambling issue, further research is necessary to examine more closely the nexus between PG and offending. As previously suggested, the relationship between PG and crime is complex. To gain a richer understanding of these phenomena, qualitative research using in-depth interviews may be a useful means to explore this relationship more closely. It is hoped that this current study and future research in this area may help to inform policy development in the judicial system. There may, for example, be opportunities to screen for gambling-related offending and direct suitable offenders to treatment as a part of the sentencing process.
Given the rate of PG among the Australian Indigenous population has been reported to be as high as 63% (Hing et al., 2014b), our finding that Indigenous prisoners experienced higher levels of PG than non-Indigenous prisoners is unfortunately not surprising. Nonetheless, the prevalence rate obtained for Indigenous prisoners in the current study of 75% is concerning. There is a need for culturally appropriate evidence-based interventions for our First Nations people. We were unable to identify any peer-reviewed literature concerning the adaptation of PG treatment for Indigenous Australians. In addition to the adaptation of a PG measurement tool for Indigenous Australians (Bertossa, Harvey, Smith, & Chong, 2014), Bertossa and colleagues have adapted a PG cognitive behavioural therapy program for use with Australia Aboriginal problem gamblers. The program provides a transport service to help clients attend appointments, allows contact with an Aboriginal specific project worker, uses more in-session therapy tasks as opposed to assigning large amounts of homework, and provides access to traditional healers (Bertossa, 2014). A pilot study examining the effectiveness of the program is currently underway.
Around 25% of prisoners who indicated that they had a gambling problem reported having previously sought help. This rate is higher than the estimated help-seeking rate of 8% to 17% among the general population of Australian problem gamblers (Productivity Commission, 2010). It should be noted, however, in our current survey that we did not enquire about and discriminate the type of help sought. Some respondents may have interpreted this question to include assistance sought from family or friends, as well as formal professional help. Previous research suggests problem gamblers often turn to family members or friends for informal help (Hing, Tiyce, Holdsworth, & Nuske, 2012). The rate of formal help-seeking may in fact be lower than was reported in the current data. Another reason for the higher than expected rate of help-seeking among this population may be the severity of gambling problems experienced by this group of problem gamblers. Research indicates help-seeking among problem gamblers is often a last resort, after experiencing significant negative consequences such as legal proceedings, family breakup, job loss, or physical or psychological breakdown (Productivity Commission, 2010). Problem gamblers facing prison terms for crimes related to gambling are also often encouraged by legal representatives to seek help prior to appearing in court, or may be ordered by the court to attend counselling services, and this may also contribute to higher rates of help-seeking behaviour. Although the rate of help-seeking was slightly higher than has been reported for the general Australian population (Productivity Commission, 2010), overall the rate was low, and suggests the prison environment may provide a useful opportunity to target prisoners afflicted by PG, to raise awareness of, and provide interventions for PG.
Limitations
One potential limitation is that we were relying on honest responses. This was addressed by asking prisoners to complete the questionnaires anonymously and place them in a sealed box. This method has been recommended to increase honest responding and thereby increasing the validity of the data (de Leeuw, Hox, & Dillman, 2008). Concerning previous help-seeking behaviour, we did not differentiate formal versus informal help. Future research could explore this and examine types of help sought: informal support from family or friends, or formal support from gambling help services or health care providers. A further limitation is that although we surveyed around two thirds of the available participants at each prison location, we did not collect any information about the third of prisoners who did not participate. This should be taken into consideration when interpreting these data. However, with respect to age and Indigenous Australian characteristics, our sample was comparable with the total male South Australian prison population at the time, which comprised a mean age of 37.6 (Mdn = 35.5) years and an Indigenous proportion of 23% (ABS, 2016b). Nevertheless, the relatively small sample of Indigenous Australians (n = 57) should be taken into consideration.
Conclusion
This study confirms an extremely high lifetime prevalence rate of PG among the male prison population and suggests the majority of prisoners would benefit from PG awareness and treatment programs. The data also provide the first examination of lifetime prevalence of PG among Indigenous Australian prisoners, with the results suggesting PG rates among Indigenous inmates are significantly higher and help-seeking rates significantly lower than in their non-Indigenous counterparts. These findings suggest prisons may provide an excellent setting for the identification and engagement of offenders with gambling problems, and an opportunity to arrange pre- and postrelease PG treatment interventions. The findings also highlight the need for culturally appropriate PG programs in the correctional services setting.
Footnotes
Acknowledgements
The authors thank all prisoners and prison staff for their support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors acknowledge the Department for Correctional Services (DCS) South Australia whose funding made this work possible.