
Abstract
Violence risk assessment and management are key tasks in mental health services and should be guided by validated instruments covering both risk and protective factors. This article is part of an international effort to validate the Structured Assessment of Protective Factors (SAPROF) for violence. The SAPROF, Historical, Clinical, Risk Management–20 (HCR-20) and the Psychopathy Checklist–Screening Version (PCL-SV) were administered in a sample of 261 patients in U.K. forensic, general inpatient, and community mental health settings. There was significant variation between these groups on SAPROF scores with fewer protective factors in the forensic group. The prospective validity of the SAPROF for nonviolence in the general inpatient and community samples was moderate (area under the curve [AUC] = .60). Adoption of the SAPROF or similar instruments as a supplement to risk-focused assessments has the potential to improve awareness of protective factors and enhance therapeutic engagement in a range of mental health services.
Keywords
Introduction
In the past decade, the structured professional judgment (SPJ) approach to violence risk assessment and management has developed with an emphasis on systematic evidence-based guidance for evaluating the presence of specific types of individual risk factors and developing responses to the overall profile which is identified. SPJrisk assessment tools are protocols containing empirically based static and dynamic risk factors for an individual, which are carefully interpreted by trained mental health professionals to arrive at a well-informed final judgment of violence risk (Douglas, Blanchard, & Hendry, 2013). Risk assessment has traditionally tended to focus on the presence or absence of negative features such as instability and traumatic experiences. However, this may skew the assessment negatively with implications for its validity and clinical utility (Miller, 2006). Thus, there has been growing interest in adding a focus on the presence of protective factors that could moderate and counterbalance the influence of risk factors. The Structured Assessment of Protective Factors (SAPROF; de Vogel, de Vries Robbé, de Ruiter, & Bouman, 2011) is an instrument designed in the Netherlands with these issues in mind to guide evaluations in conjunction with other tools, and this study was an attempt to examine the validity and utility of the tool in U.K. mental health services.
At present, protective factors are not routinely assessed in forensic mental health services to the same extent as risk factors. A risk-averse culture in many countries has previously obscured the desirability of focusing as well on strengths and protective factors and the integration of such information into routine health care decisions. This has the potential to compromise the clinical utility of protective factors in risk formulation if the rater is encouraged to think entirely in terms of a risk alone judgment. There is a need for a conceptual change if this is to be improved. Clinicians usually want to bring about positive change when working with patients rather than just reducing negative factors, and adding the SAPROF or some other measure of protective factors to the assessment package enables this to happen. The patients would be more motivated to engage in treatment if they are involved as much as possible in the risk assessment, including being party to the findings wherever possible. Risk assessment results are often kept away from patients, despite all of their other documentation being made available to them, but the SAPROF has the potential to produce profile results that can be more easily shared and thus to encourage collaborative working in constructing the risk management plan. The consideration of protective factors should thus bring a more balanced appreciation of the individual presenting risks than can be captured within current risk formulations.
The concept of a protective factor is evolving and still debated at a fundamental level in terms of whether it is simply the absence or converse of a risk factor or whether it is an independent entity, which may mediate or moderate the relationship between risk and violence. It has been defined by one set of researchers as any characteristic of an individual or their environment or situation that may moderate risk factors (de Vogel et al., 2011). Thus, protective factors are seen as conceptually distinct from risk factors and can act as a buffer in the relationship between risk factors and violent behaviour. De Vogel et al. (2011) give the example of religiosity which is negatively related (i.e., protects against) with criminality, but its absence, nonreligiosity, has no relationship, positive or negative, with criminality. Another way of viewing the distinction emphasises the orthogonality of risk and protectiveness: A person may score high on risk and high on protective factors, which moderates the high-risk level. Those who are truly “risky” combine high levels of risk factor with low levels of protective factors.
Based on the available evidence, it seems likely that including protective factors in violence risk assessment is likely to lead to a more comprehensive assessment of violence propensity (Quinsey, Jones, Book, & Barr, 2006; Salekin & Lochman, 2008). Indeed, some researchers have concluded that strengthening protective factors may be more effective in decreasing risk behaviours and increasing prosocial behaviour than reducing the presence of risk factors (Blum & Ireland, 2004; Resnick, Ireland, & Borowsky, 2004). An interest in systematically assessing this aspect has led to the development of a number of protective factor instruments in the last decade (Desmarais, Nicholls, Wilson, & Brink, 2012; Lodewijks, Doreleijers, de Ruiter, & Borum, 2008), including the SAPROF.
This instrument was developed as a supplement to the Historical, Clinical, Risk Management–20 (HCR-20; Douglas et al., 2014) to assess protective factors and their relationship to future violent behaviour in adult offenders and forensic psychiatric patients (de Vries Robbé, de Vogel, & de Spa, 2011). It is a structured assessment guideline intended for use in combination with a reliable and valid risk assessment instrument such as the HCR-20 in accordance with the overall SPJ approach. The instrument consists of two static and 15 dynamic protective items each located in one of three domains: internal factors, external factors, and motivational factors. It aims not only to assess protective factors but also to inform treatment planning by identifying potential areas for intervention, and it can offer valuable guidance in narrowing the gap between assessment and violence prevention. For research purposes, a global score combining the risk and protective profiles of an individual can be calculated by subtracting the SAPROF score from the HCR-20 score as well as considering the two domains separately (de Vries Robbé, de Vogel, Douglas, & Nijman, 2015).
De Vries Robbé et al. (2011) report good predictive validity for the SAPROF in relation to criminal recidivism at 1- and 2-year follow-ups in a sample of 126 Dutch patients released from a secure forensic mental health setting. It has since been subjected to further testing with sex offenders and other forensic groups in the Netherlands (de Vries Robbé et al., 2015) and more widely in Canada, Singapore, Ireland, and Germany (Abidin et al., 2013; Davoren et al., 2013; Doyle, 2014; Turner et al., 2014; Viljoen et al., 2016; Yoon, Spehr, & Briken, 2011; Zeng, Chu, & Lee, 2015). Results so far in these forensic setting studies are mixed but promising. Doyle’s (2014) prospective study comparing a cohort of forensic patients discharged from U.K. medium secure units (MSUs) with prison or the community found greater protective factors and lower risk scores in the latter group. In terms of predictive validity, results from the same cohort (Coid, Kllis, Doyle, Shaw, & Ullrich, 2015) indicated that a number of SAPROF items (e.g., intelligence, intimate relationship) were poor predictors of violence in the 6 months following assessment in both a standard predictive and a causal model. A meta-analysis has also indicated that the SAPROF dynamic items and total score had the strongest predictive validity across a range of protective factor instruments (O’Shea & Dickens, 2015).
Despite this growing literature in forensic services, there is currently very little research on the potential for the SAPROF’s application in other mental health populations where violence can also occur and where the concept of protective factors is equally applicable. This study therefore applied the SAPROF and HCR-20 to a nonforensic U.K. sample in general inpatient and community settings to (a) compare the protective factor profile with that of a U.K. forensic sample and (b) examine concurrent and predictive validity in the new settings.
Method
To establish concurrent validity, we adopted a cross-sectional design, in which we compared the relationship between scores on the SAPROF, the HCR-20, and a third instrument with established validity in terms of violence, the Psychopathy Checklist–Screening Version (PCL-SV; Hart, Cox, & Hare, 1995), in 261 patients. For predictive validity, we used a prospective design linking SAPROF scores and violence in the subsequent 6 months in a subgroup of the overall sample (n = 151).
Settings and Sample
The study was conducted in three settings in the North West of England (2010-2013), as follows.
Secure inpatient services (n = 55)
This consisted of a MSU (55 male and 11 female beds) and four low secure units (approximately 12 male beds each) on four separate sites. These units were locked and provide secure care to forensic and other high-risk populations drawn from a mixed urban and rural population. Most patients on the wards were detained under the Mental Health Act (MHA), and the average admission duration in the MSU was 12 months.
General inpatient services (n = 100)
This consisted of nine general acute wards, each with approximately 20 beds, on six separate sites. These units provided acute care (including one psychiatric intensive care unit) for adult male and female patients from a predominantly urban population. Most patients on the wards were not detained under the MHA, and the average admission duration was about 6 weeks.
Community services (n = 106)
This consisted of six Community Mental Health Teams (CMHTs) in various configurations on separate sites. These teams provided domiciliary and outpatient services to a predominantly urban population. General inpatients were clients of these CMHTs but were admitted at the time of assessment and thus are categorised as part of the general inpatient sample above.
Measures
The SAPROF (de Vogel et al., 2011) has three subscales: Internal Factors (e.g., intelligence; five items), Motivational Factors (e.g., leisure activities; seven items), and External Factors (e.g., social network; five items). A Final Protective Judgment (low, moderate, high) is made based on consideration of the overall pattern of scores but was not used here. The 17 items of the SAPROF are coded on a 3-point scale (0, 1, 2) according to the presence and strength of the relevant feature. Total scores therefore range from 0 to 34, with higher scores reflecting a higher level of protective features. It should be noted that items on the External subscale are almost always rated 2 for inpatients because of the high levels of control and treatment they receive as a result of their placement.
The HCR-20 (Webster, Douglas Eaves, & Hart, 1997) is a 20-item SPJ guideline for violence risk assessment that contains 10 Historical, five Clinical, and five Risk Management items that are commonly associated with risk for future violence. Each item is coded on the same 3-point scale as above. The HCR-20 has satisfactory psychometric properties and has been shown to be a robust predictor of institutional and community violence (Gray, Taylor, & Snowden, 2008). Version 2 of the instrument was used.
The PCL-SV (Hart et al., 1995) is a screening version of the Hare Psychopathy Checklist–Revised (PCL-R) and contains 12 items. Factor 1 of the PCL-SV reflects affective and interpersonal traits, and Factor 2 reflects behavioural or social deviance components of psychopathy. Each item is rated on a 3-point scale: 0 (not present), 1 (somewhat present), and 2 (present). This gives the instrument a range of 0 to 24 points, where the cutoff for psychopathy is set to 18. Total scores equal to or above 18 on the PCL-SV are considered indicative of psychopathy (Hart et al., 1995).
Violence in the 6 months following the baseline assessment was examined by case note review and, where necessary, discussion with their key worker. Incidents of physical aggression (to other people or property) and verbal aggression were recorded on a structured checklist based on the Liverpool Violence Assessment (LIVA; Nathan, Rollinson, Harvey, & Hill, 2003).
Procedure
Ratings on patients consenting to take part in the study were made by a team of raters consisting of eight mental health professionals and researchers. Each rater held a postgraduate qualification in psychology or psychiatry and had formal training in the use of the three instruments prior to the commencement of the research. Interrater reliability was only partially assessed. For a subsample of participants (mainly from forensic and acute settings), the raters met monthly during the data collection period and blind rated the SAPROF from a randomly selected set of case notes each time to maximise consistency between them. For the rest of the sample (i.e., general inpatient and community settings), interrater agreement was formally examined. We calculated a weighted kappa for categorical data for each instrument and each pair of raters (six raters; three pairs; 72 ratings in total). The mean kappa for pairs of raters across all three instruments was 0.96 (95% confidence interval [CI] = [.94, .98]). There was perfect agreement in 68% of ratings, and agreement was below a threshold of 0.75 (Fleiss, Levin, & Cho Paik, 2004) in only two ratings (<3%).
Data were collected on two occasions: at baseline and 6 months later. Baseline data included participants’ sociodemographics, diagnosis, history of inpatient admissions, and contacts with mental health services; history of violence; type of intervention offered; SAPROF scores; HCR-20 scores; PCL-SV scores; and violence frequency and severity. When rating, researchers were asked to consider any historic items over the lifetime of the participant, whereas the dynamic factors were scored with regard to the likely outcomes in the 6 months following the assessment.
Ethical approval was received from the Health Research Authority, the National Research Ethics Service (Liverpool East Health Research Ethics Committee), and governance approvals from all the participating National Health Service (NHS) trusts were in place before recruitment and data collection.
Data Analysis
We calculated descriptive statistics for demographic and clinical features of the sample and compared across the three groups using chi-square and ANOVA with post hoc Scheffe tests applied to pairs of groups, where the ANOVA was significant. We calculated a combined risk/protection index score by subtracting the SAPROF Total score from that of the HCR-20 total. We then examined means across the three groups for each SAPROF item, each SAPROF subscale, the SAPROF Total, and the combined index score. Concurrent validity was tested using bivariate correlations of the SAPROF (subscales and total), HCR-20, and PCL-SV total scores overall and for each setting. We measured predictive validity by calculating the area under the curve (AUC) statistic derived from receiver operating characteristics (ROC) analysis. ROC analysis has frequently been used to estimate predictive validity, with the AUC of the ROC providing an index for interpreting the overall accuracy of the predictor. An AUC of .50 represents chance prediction and an AUC of 1.0 perfect prediction. Rice and Harris (2005) suggest the following interpretations of AUC values: .500 to .556, small; .557 to .639, moderate; and .640 to 1.00, large. As protective factors are supposed to be associated with nonviolence, the AUC values for the SAPROF represent the accuracy of assessments for nonviolence.
We also used logistic regression to identify individual factors associated with violence in a subsample of the cohort of patients (n = 151). We examined the relationship between a number of potentially explanatory variables relating to demographics (i.e., age, gender, marital/relationship status, primary diagnosis, admission history and length of admission, history of violence), setting (general inpatient or community), SAPROF scores, and violence as the outcome variable (defined as physical aggression in the 6 months following assessment and coded as yes/no). We examined the relationship of each explanatory variable to violence using univariate analysis, and we retained those variables identified as being statistically related to the outcome at the 10% (p = .1) level for possible inclusion in the multivariate model. We adopted a p value <.05 to determine the significance of the variables included in the multivariate model.
Results
Characteristics of the Patient Sample
The sample consisted of 261 patients who gave consent to participate. In terms of setting at the point of assessment, 21% (n = 55) were detained in forensic settings under the MHA, and in this article, we refer to these patients as the “secure inpatients” group, whereas 38% (n = 100) entered their psychiatric unit voluntarily or were subject to a civil MHA section and these are referred to as the “general inpatients” group, and 41% (n = 106) of patients were accessing a community mental health service, which will be referred to as the “community patients” group. The main demographic and clinical characteristics of the three groups are shown in Table 1.
Characteristics of the Patient Sample.
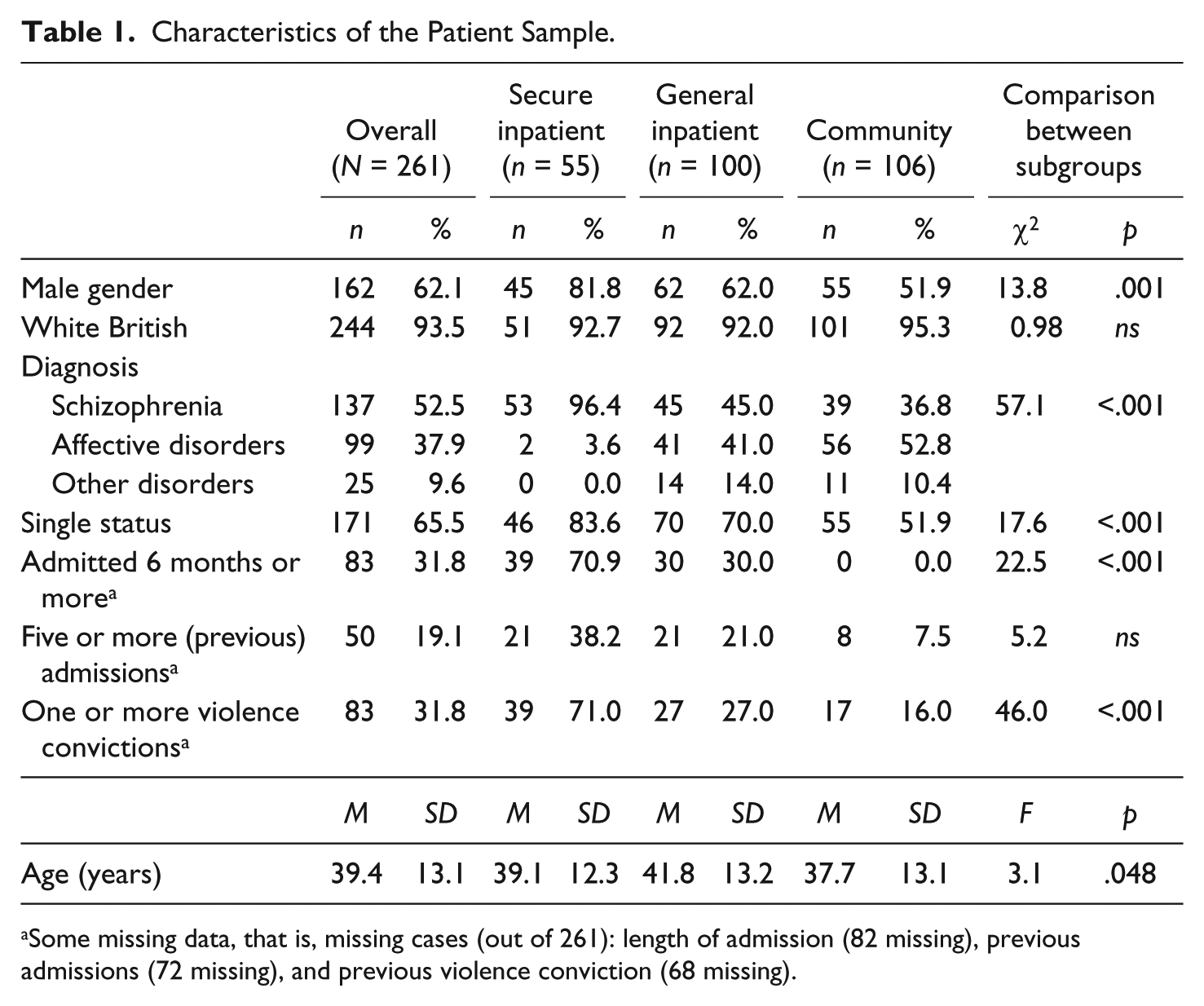
Some missing data, that is, missing cases (out of 261): length of admission (82 missing), previous admissions (72 missing), and previous violence conviction (68 missing).
The majority of patients were male (62%), White British, and not in a relationship at the time of assessment. The average age of patients was 39.4 years (range = 18-87). They mainly had a primary diagnosis of schizophrenia or affective disorders. In the secure setting group, index offences (i.e., the most recent offence which brought the offender into contact with the criminal justice system) were most frequently violent (n = 23, 41.8%) or sexual (n = 7, 12.7%) in nature. When characteristics were compared across the three groups, there were similarities in terms of ethnicity and the number of previous admissions to mental health services. On the contrary, there were highly significant variations (p < .001) in terms of diagnosis, marital status, duration of admission, and violence convictions. The secure setting group were much more likely to have a diagnosis of schizophrenia, single status, long admissions, and previous violent convictions, compared with the other groups.
SAPROF Scores in Forensic, General Mental Health, and Community Samples
SAPROF item, factor, and total scores for the overall sample and the three subgroups are shown in Table 2. The SAPROF Total and subscale scores were normally distributed in the combined sample.
SAPROF Item and Factor Scores.

Note. SAPROF = Structured Assessment of Protective Factors; HCR-20 = Historical, Clinical, Risk Management–20.
The community sample had significantly more and stronger protective factors overall (SAPROF Total) than the other two groups, but the general and secure inpatient groups did not differ significantly in overall protective factors. This pattern was apparent for the Internal and Motivational subscales as well. With the External subscale, the pattern of scores was reversed with the secure inpatient group scoring higher than the general inpatient group and the latter scoring higher than the community group. After a Bonferroni correction for multiple testing, variation in SAPROF item scores across groups was significant for every item apart from secure attachment in childhood (Item 2), leisure activities (Item 7), and social network (Item 13).
Concurrent Validity of SAPROF
Correlations between SAPROF factors and total scores of the HCR-20 and PCL-SV in the three groups are given in Table 3.
Correlations Between SAPROF (Factors and Total), HCR-20, and PCL-SV Scores.
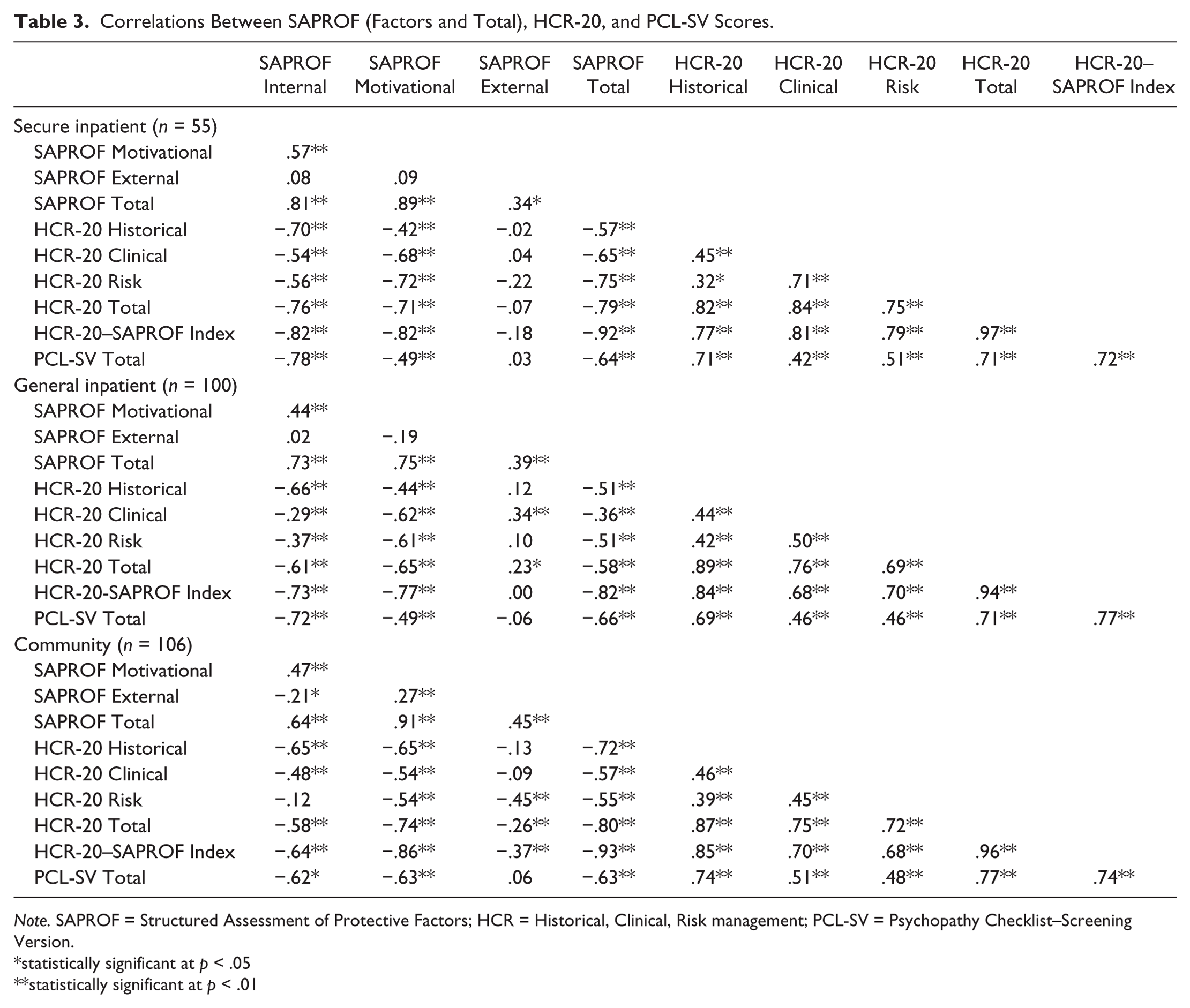
Note. SAPROF = Structured Assessment of Protective Factors; HCR = Historical, Clinical, Risk management; PCL-SV = Psychopathy Checklist–Screening Version.
statistically significant at p < .05
statistically significant at p < .01
The SAPROF Total score correlated significantly and negatively with the HCR-20 and PCL-SV in each of the subgroups. The association with the HCR-20 was weakest in the general inpatient group but remained significant. The SAPROF subscales all correlated positively and significantly with the SAPROF Total score in all three groups. The association with the SAPROF Total score was stronger (and statistically significant) in all three groups for the Internal and Motivational factors than it was for the External factor. The strength, direction, and significance of the relationship between the External factor and the two other instruments were also very variable.
Predictive Validity of SAPROF
Prospective data on violence were available for 148 of the nonforensic patients. Violence data comprised incidents of physical aggression that were recorded in the 6 months following the initial assessment, with a mean time between the assessment and outcome measurement of 188 days (SD = 3.8, 183-195 days). In this period, 12 (28.0%) of the general inpatient group and 21 (20.0%) of the community group were logged as engaging in an act of physical aggression. AUC values (with 95% CIs) are shown in Table 4.
Predictive Validity of SAPROF, HCR-20, and PCL-SV in Nonforensic Samples.
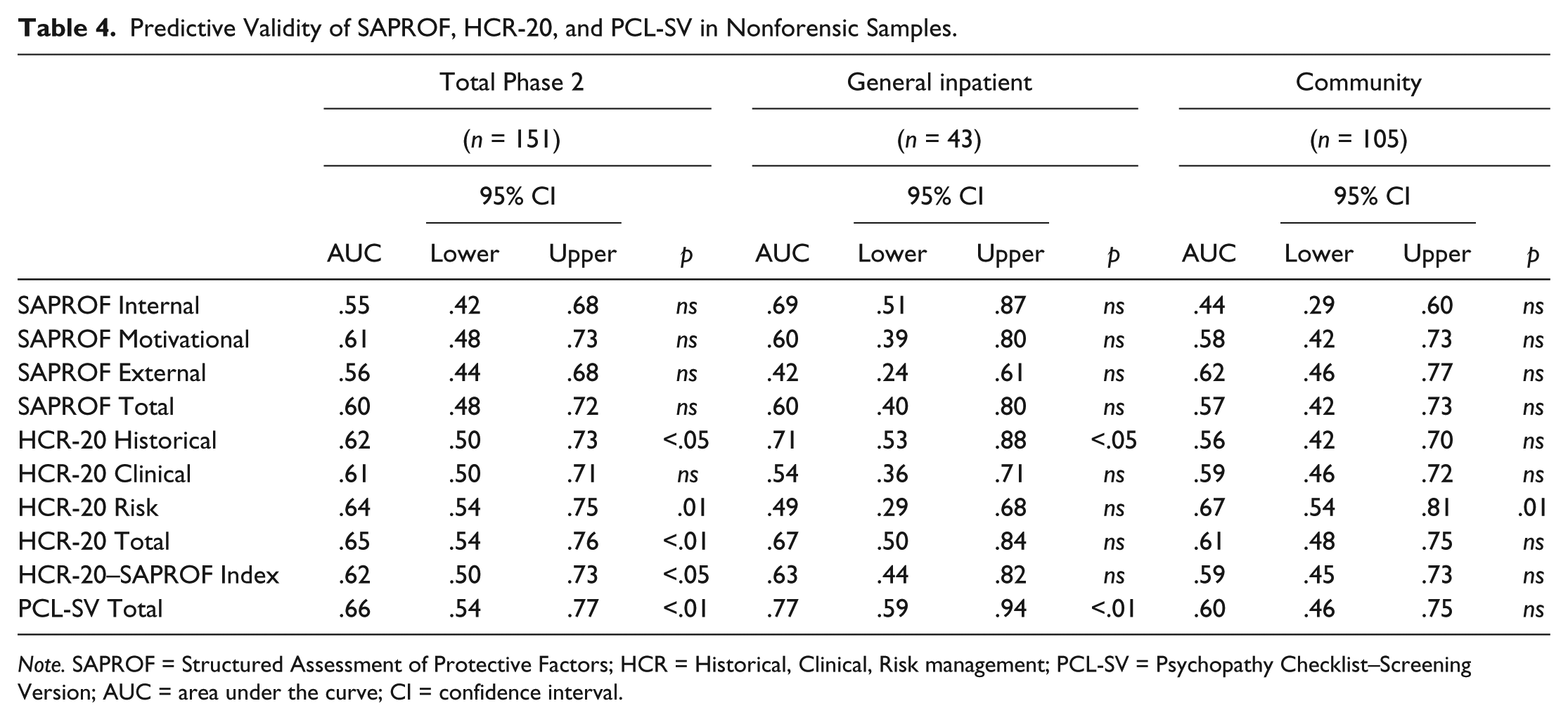
Note. SAPROF = Structured Assessment of Protective Factors; HCR = Historical, Clinical, Risk management; PCL-SV = Psychopathy Checklist–Screening Version; AUC = area under the curve; CI = confidence interval.
The AUC for the SAPROF overall and in the two subgroups was moderate in size but not statistically significant. The established tools (HCR-20 and PCL-SV) performed somewhat better in these nonforensic groups with higher and significant AUCs overall, but again there was relatively weaker predictive validity in the community group. The combined HCR-20–SAPROF Index did not outperform HCR-20 conducted on its own in either of the groups or the combined nonforensic group.
Individual Predictors of Violence for the Community and General Inpatient Samples
A logistic regression analysis was also conducted to examine the relative contribution of SAPROF scores to variations in violence propensity in the context of other possible predictors. The univariate analyses for this prospective sample (n = 151) showed that marital status, admission length, history of violence, and scores on two of the SAPROF subscales (Internal and Motivation) were all associated with violence at 6 months following assessment (p < .001). These two SAPROF subscales were entered into a multivariate analysis, but the Motivation subscale was not significant in this combination. Marital status and admission length were also not significant when included with the SAPROF Internal subscale. In the final multivariate model, only two variables remained significant: the SAPROF Internal score, β = –.525, SE = 0.122, Exp(β) = 0.591, p < .001, and history of violence, β = .031, SE = 0.012, Exp(β) = 1.032, p = .008. Patients who scored higher on the SAPROF Internal subscale were thus less likely to be violent in the future.
Discussion
The development of the SAPROF was influenced by a growing demand for a more strengths-based approach in clinical practice and the need for a complementary use of both risk and protective factors in violence risk assessment. This article addresses the important yet understudied issue of protective factors for violence risk and in particular extends the study of protective factors, which minimise violence risk beyond forensic services to a wider mental health setting. This comparison is novel, especially with regard to applying the SAPROF to community mental health samples, beyond the forensic setting in which it was developed, and provides valuable insights into the differences between patients in the various treatment contexts. Protective factors are likely to be relevant in some way to all types of aggression in all settings, so it is important to establish violence risk and protection profiles in a range of mental health populations.
Another central feature to considering risk with a strengths-based lens is the chance to involve those being assessed in the process. We would argue that any contact that promotes service user involvement during the risk assessment process brings with it a level of transparency that goes on to maximise the quality of the decision making. This raises the likelihood of keeping those being assessed engaged in interventions and risk management arrangements (Logan, 2003). We think the use of the SAPROF enables discussion with the patient around specific protective factors through ongoing clinical discussion.
A good relationship within which service users’ qualities and strengths are valued has been suggested to be important in discussing risk (Langan & Lindow, 2004). The format of the SAPROF offers a more holistic spread of factors, adding to the limited, narrow focus on risk. Whether the protective factors are conceptualised as either a mediation or buffer between risk factors and violence is for the clinical teams and individuals to agree. However, the therapeutic dialogue that will be evident will surely strengthen the working relationship as they move the generalised factors of the SAPROF into the specific features linked to that person’s recovery.
Patient involvement in the SAPROF Motivational and External items in particular encourages positive ownership and change in further developing these protective factors, and may form the basis of and be easily incorporated into specific therapy and care planning linked to their stage of recovery. In the action-orientated world of care planning, this model optimises the options for choice and shared decision making. Recognising that the service user is expert by virtue of their lived experiences should allow for more balanced decisions with a closer alliance to a common goal in terms of problem and outcome of treatment. It allows some ownership, for example, of developing more feasible plans around work or leisure as part of a relapse prevention care plan, in particular, in the transition from hospital to community, as well as highlighting and increasing the understanding of the importance of social network and professional care.
When interpreting the results of this study, it is important to note that the SAPROF itself was designed for a specific forensic population and not with a view to wider application as performed here. Evidence here for or against its suitability in these wider populations is not relevant to the specific forensic populations for which it was originally developed.
The results here indicate that, in terms of profiles, there is significant variation between the secure, general inpatient and community groups on SAPROF Total score and subscales. This variation is in the direction that would be anticipated, if the concept of a protective factor is valid and the instrument is robust, that is, fewer protective factors (lower SAPROF scores) for patients in secure settings. Patients in the community had significantly higher levels of protective factors overall compared with forensic and general inpatients even though they had significantly lower levels of external protection, especially with regard to professional care, living circumstances, and external control. It was expected for patients in the forensic group to score highly on these external items because of their management plans and detention under the MHA.
Protective factor profiles as measured by the SAPROF Total score tend to vary across different populations, even within the forensic setting. The relatively strong level of protective factors in the community sample here is actually lower than that reported for some inpatient forensic samples (Abidin et al., 2013; Davoren et al., 2013) but is comparable with another community sample surveyed by Yoon et al. (2016), although the latter was an offender group. Both the forensic and general inpatient groups here are comparable with other forensic samples examined by Viljoen et al. (2016) and Abbiati, Azzola, Palix, Gasser, and Moulin (2016), but somewhat stronger in terms of protective factors than others (de Vries Robbé et al., 2011; de Vries Robbé et al., 2015).
Internal and motivational protective factors in the community sample here were generally higher than those in the secure and general inpatient samples, apart from secure attachment in childhood, which was comparable with the levels identified for secure inpatients. This item is one of only two historical items in the SAPROF. Higher Internal and Motivational factors among community patients especially for those who have been previously hospitalised or recently discharged may reflect the fact that these factors are key goals of available inpatient interventions (i.e., insight and coping strategies) and should be improved to achieve a successful discharge. This is also in line with Doyle’s (2014) prospective U.K. study, which indicated that forensic patients discharged to prison were significantly less likely to have protective motivational factors.
We found evidence of good concurrent validity overall for the SAPROF, when compared with established tools such as the HCR-20 and the PCL-SV. We found a negative and highly significant correlation between the SAPROF Total score and those for HCR-20 and PCL-SV. These significant correlations were present in each setting, although a relatively poor correlation with HCR-20 in the general inpatient group stands out. These strong associations support the conceptual model underpinning the development of the SAPROF and fit with those reported elsewhere (Abbiati et al., 2016; Abidin et al., 2013; de Vries Robbé et al., 2011; de Vries Robbé et al., 2015; Persson, Belfrage, Fredriksson, & Kristiansson, 2017).
The predictive validity of SAPROF Total for nonviolence over 6 months in both general inpatient and community outpatients here was moderate in size (Rice & Harris, 2005). As such it was comparable with that achieved by the SAPROF in some forensic samples reported by Viljoen and colleagues (2016), Yoon and colleagues (2011), Yoon and colleagues (2016), and Zeng et al. (2015), but lower than that observed in other forensic settings (Abbiati et al., 2016; Abidin et al., 2013; Davoren et al., 2013; Persson et al., 2017) including the original high-security setting in which it was developed (de Vries Robbé et al., 2011; de Vries Robbé et al., 2015). The PCL-SV and HCR-20 were better predictors of violence with larger and significant AUC values (AUC > 0.6) in the general inpatient sample. The relatively low predictive validity here could simply be an indication that the SAPROF works best in the area for that which it was developed, that is, in forensic settings and for adults with a history of violent or sexually violent offending. It could also be linked to the degree of freedom and supervision that patients have in these settings—the more the freedom and less supervision, the more often aggressive behaviour may go unrecorded. It is generally expected that the number of incidents reported in these samples will be lower than that of patients who have less freedom or are unable to leave the hospital grounds.
When exploring individual factors linked to violence in the regression analysis, we found only the SAPROF Internal score and history of violence to be significant. This indicates that patients who scored higher on the SAPROF Internal subscale were less likely to be violent in the future, whereas those with a recorded history of violence were more likely to be violent in the future. The latter results are consistent with the literature on predictors of violence and recidivism (Klassen & O’Connor, 1988; Walters & Crawford, 2014). As the analysis did not differentiate between the different items making up the SAPROF Internal subscale, it was not possible to deduce the strength and direction of the relationship between these individual factors and violence. More research is warranted to further explore the correlation between total and individual SAPROF scores and incidents of violence following assessment.
Limitations
A number of issues are worth noting to ensure cautious interpretation of these results. In particular, assessing violence risk and protection in general inpatient and community samples is limited by the low rates of violence by people in these groups, especially, compared with those in the forensic samples on which the SAPROF has been developed. Nearly 80% of the nonforensic groups here had no previous violence convictions compared with about 30% of the forensic group. While other forms of violence may have occurred without prosecution, on the face of it, many in the nonforensic groups may be at very low risk of ever engaging in the behaviour that the SAPROF was designed to focus upon. Similarly, both the SAPROF and the HCR-20 target violent recidivism rather than first offences. Again, given the low rate of violent convictions in the nonforensic groups here, any violence in the follow-up period may well have been first rather than recidivist offences.
In terms of measurement, the individual raters scored all the instruments for each patient so the ratings are vulnerable to the problem of criterion contamination, especially when measuring the concurrent validity of SAPROF against the HCR-20 and PCL-SV. Although the researchers who made ratings were blind to the work of the others, this may have inflated the associations between the three instruments somewhat due to a lack of blinding. On the contrary, as the SAPROF was designed as a supplement to the HCR-20, scoring on both instruments by the same rater is an advantage. A further limitation in this area may be the risk of outcome data collection bias, as violence raters were not blind to SAPROF scores, though the data collection was done 6 months later and raters were specifically instructed to avoid consulting the data retrospectively.
It is furthermore unfortunate that the predictive validity analysis was limited to a subsample of the whole study cohort. This was due to the scope of the study being expanded for the general and community patient groups following the provision of greater resources that enabled more ambitious data collection objectives. Limitations should also be noted regarding the interrater reliability assessment between raters, as well as with regard to the lack of information about the proportion of patients who were approached but not consented to participate in the study.
The value of estimating predictive validity in the SPJ paradigm is contested as well, as the purpose of such instruments is to improve practice and, if successful, should lead to reduced violence and thus poorer predictive validity (Pedersen, Ramussen, & Elsass, 2012).
Conclusion
This novel examination of violent-protective factors in nonforensic populations using the SAPROF instrument has indicated that people with mental health problems living in the community have stronger internal and motivational protections against perpetrating violence than those who reside in secure or general mental hospitals. They also have greater protection overall even when the external supports provided by the institution are taken into account.
Footnotes
Acknowledgements
The authors thank Dr. Wally Barr, Mitra Ben-L’Amri, Rhiannah McCabe, and Dr. Rajan Nathan.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.