
Abstract
The study examined family and teacher support as factors that can protect adolescents from internalized and externalized problems after exposure to community violence (ECV). Self-administered questionnaires were filled out by a sample of 1,832 Arab and Jewish Israeli high school students. The Arab adolescents reported significantly higher levels of community violence victimization, internalized problems, externalized problems, family support, and teacher support than the Jewish adolescents. The girls reported higher levels of internalized problems, and the boys reported higher levels of externalized problems. ECV predicted high levels of internalized and externalized problems, family support predicted low levels of internalized and externalized problems, and teacher support had no predictive role. Path analysis confirmed the significance of the relationships between ECV effects, support variables, and gender. The limitations of the study and implications of the findings for future research and for the development of family care and family intervention programs are discussed.
Keywords
Introduction
The number of publications dealing with the effects of exposure to different types of violence on mental health among varied populations has risen over the past two decades from less than 10 to more than 2,000 publications per year (Lindert, 2015). Exposure to community violence (ECV) includes personal experience, direct witnessing, and indirect witnessing (hearing about) various types of violent events occurring within the community context (in the neighborhood, school, clubs, streets, etc.). According to recent studies across a variety of national and cultural contexts, 20% to 40% of all adolescents have been victims of community violence (CV; Haj-Yahia, Leshem, & Guterman, 2013; Lambert, Boyd, Cammack, & Ialongo, 2012), and 75% to 98% have witnessed CV (Haj-Yahia, Leshem, & Guterman, 2011; Salzinger, Feldman, Rosario, & Ng-Mak, 2011). Hence, ECV is perceived as a major public health problem (Krug, Mercy, Dahlberg, & Zwi, 2002). Although numerous studies have linked ECV with various adverse effects (Clark, Benkert, & Flack, 2006; Scarpa, Haden, & Hurley, 2006), there is a lack of research on the factors that mitigate the negative effects of ECV on behavior problems among adolescents. Hence, the current study focused on family and teacher support as potential moderators of externalized and internalized problems resulting from ECV among Jewish and Arab youth in Israel.
Effects of ECV
ECV has short- and long-term negative effects (Merikangas et al., 2010; Ozer & McDonald, 2006; Patchin, Huebner, McCluskey, Varano, & Bynum, 2006). The intensity of the effects depends on the type of exposure (personal experience or witnessing), the nature of violence (from threats to killing), and the frequency of exposure (Osofsky, 1995). The most severe effects are linked to multiple events of personal victimization (Finkelhor, Ormrod, & Turner, 2007). Although the prevalence of ECV among youth from at-risk communities is similar to the prevalence among the general population, the severity of ECV events is higher in at-risk communities (Scarpa et al., 2002), and these youth display negative effects similar to those displayed by the general population of at-risk youth (Ozer, 2005; Scarpa, 2003; Scarpa et al., 2006).
Mental health problems in children and adolescents are typically grouped into two categories: internalized and externalized problems. Internalized problems are related to difficulty controlling negative emotions such as depression, anxiety, and loneliness. These problems are more commonly observed among girls, whereas externalized problems are more commonly observed among boys, who show difficulty controlling negative behaviors (Rescorla et al., 2011). Internalized behavior problems related to ECV among youth include emotional distress (Jenkins & Bell, 1994; Raviv, Raviv, Shimoni, Fox, & Leavitt, 1999), anxiety (McMahon, Coker, & Parnes, 2013; Siegel, La Greca, & Harrison, 2009), depression (Mrug, Loosier, & Windle, 2008; Self-Brown et al., 2006), intrusive thoughts (Martinez & Richters, 1993), sleep disorders (Saltzman, Pynoos, Layne, Steinberg, & Aisenberg, 2001), and somatic problems (Cooley-Quille, Boyd, Frantz, & Walsh, 2001). Externalized behavior problems resulting from ECV include behavioral disorders, aggression, involvement with gangs, crime, and the use of weapons (Guterman, Cameron, & Hahm, 2003; Halliday-Boykins & Graham, 2001; Scarpa et al., 2002).
Fowler, Tompsett, Braciszewski, Jacques-Tiura, and Baltes (2009) performed a meta-analysis of 114 studies, which were conducted between 1992 and 2007. The studies documented the effects of ECV on the mental health of children and adolescents, and explored the relationships of risk factors and resilience to internalized and externalized problems. In light of these studies, Fowler et al. (2009) concluded that the relationship between ECV and externalized behavior problems was stronger than the relationship with internalized behavior problems. They also concluded that although the effect of ECV on internalized behavior problems was greater for girls than for boys, there were no gender differences in the effect of ECV on externalized behavior problems. Nevertheless, the researchers were not able to draw definitive conclusions regarding the contribution of risk and protective factors due to the methodological differences among the reviewed studies (Fowler et al., 2009). A more recent longitudinal study revealed higher levels of internalized problems after ECV among 14-year-old youth, and higher levels of externalized problems among 16-year-old youth (Hardaway, Sterrett-Hong, Larkby, & Cornelius, 2016). The differences in the prevalence and severity of post-ECV mental health problems could be explained by differences in the coping skills and levels of resilience of the exposed youth (Garbarino, Dubrow, Kostelny, & Pardo, 1992; Ozer, 2005; Scarpa et al., 2006).
Among at-risk youth, internalized behavior problems were linked with direct and indirect exposure to violence, low perceived family support (PFS), and poor relations with teachers (Solberg, Carlstrom, Howard, & Jones, 2007). Researchers have tested the contribution of social and family support, family conflict, emotional control, social recognition, and coping style as mediators or moderators of the effects of ECV (Buka, Stichick, Birdthistle, & Earls, 2001; Kliewer, Murrelle, et al., 2006; Lynch, 2003; Miller & MacIntosh, 1999; Schwartz & Proctor, 2000). However, there is still no conclusive evidence regarding the differences in types, rates, and severities of post-ECV mental health problems among youth (Margolin & Gordis, 2004). Against this background, the current study aimed to examine the role of family support and teacher support as protective factors that might moderate the relationships between ECV and internalized and externalized behavior problems among teenagers.
Family Support
Parental and family support could protect children and adolescents from externalized and internalized problems after exposure to violence (Howard, Budge, & McKay, 2010; Kaynak, Lepore, & Kliewer, 2011; Punamäki, Qouta, Miller, & El-Sarraj, 2011). Previous studies have recognized several factors linked to support from family members, including the following: parental support (Brookmeyer, Henrich, & Schwab-Stone, 2005; Davis, Ammons, Dahl, & Kliewer, 2015), family cohesion and parental supervision (Kliewer et al., 2006), family support (Jain & Cohen, 2013; Leshem, Haj-Yahia, & Guterman, 2016), family functioning (Sheidow, Henry, Tolan, & Strachan, 2014), parent–child relations and guidance (Hammack, Richards, Luo, Edlynn, & Roy, 2004; Kliewer et al., 2004), and mother and sibling support (Eisman, Stoddard, Heinze, Caldwell, & Zimmerman, 2015). Researchers have found that family support may moderate depression and anxiety among adolescents exposed to CV (Ozer & Weinstein, 2004). Notably, Leshem et al. (2016) showed that family support could moderate the prevalence of post-traumatic stress disorder (PTSD) symptoms among Palestinian youth exposed to CV. In addition, family support played a significant moderating role of signs of distress after ECV among inner-city urban high school students in the United States (Howard et al., 2010), as well as post-ECV symptoms of depression among African American youth (Kaynak et al., 2011), and post-polyvictimization anxiety among youth in the United States (Turner, Shattuck, Finkelhor, & Hamby, 2017). It also moderated PTSD symptoms, depression, and aggression associated with war and CV exposure in four African countries (Foster & Brooks-Gunn, 2015). Furthermore, research has revealed that family support played a significant moderating role of the relationship between exposure to school violence and anxiety, even in cases where adolescents were exposed to intimate partner violence (IPV; Kennedy, Bybee, Sullivan, & Greeson, 2010). In addition, family support was found to moderate the relationship between depression and violent behavior among Israeli youth exposed to rocket attacks (Shahar & Henrich, 2015). Nonetheless, parental support did not moderate mental health symptoms among Palestinian children exposed to military violence (Punamäki et al., 2011), and family support did not moderate post-ECV externalized problems among American high school students (Logan-Greene et al., 2011). In addition, neither kinship support nor parental involvement played a significant moderating role of the association between ECV and externalized behavior problems among African American adolescents (Hardaway et al., 2016). Hence, the need for further exploration of this issue.
Teacher Support
Children and adolescents spend a major part of the day at school, where their teachers function as significant adults. In light of findings indicating that emotional, cognitive, and instrumental support from teachers predicts emotional well-being among students (Suldo et al., 2009), teachers could be a source of support that protects the children from the effects of ECV. Another salient factor that has been found to enhance the emotional well-being of students at school is a sense of belonging (Eccles, Early, Fraser, Belansky, & McCarthy, 1997; Ozer, 2005), which protects students from risk behaviors (Brookmeyer, Fanti, & Henrich, 2006; Garcia-Reid, Reid, & Peterson, 2005). Studies have revealed a higher sense of belonging among students whose teachers create a supportive environment (McNeely, Nonnemaker, & Blum, 2002). Research among Jewish and Arab adolescents in Israel has shown that low teacher support correlated with higher involvement in school violence (Berkowitz & Benbenishty, 2012), whereas high teacher support correlated with lower school violence victimization (Marachi, Astor, & Benbenishty, 2007). This suggests that teacher support could also have an indirect effect, through lowering the prevalence of ECV among students. Specifically, support from teachers may moderate the rate of ECV-related PTSD symptoms among adolescents (Leshem et al., 2016; Löfving-Gupta, Lindblad, Stickley, Schwab-Stone, & Ruchkin, 2014). One study found that school climate moderated ECV-related PTSD symptoms, depression, and aggression among adolescents in Africa (Turner et al., 2017), whereas another study found that school climate did not moderate post-ECV internalized and externalized problems (Hardaway, McLoyd, & Wood, 2012). Clearly, there is a shortage of research on the role of teacher support as a protective factor against the effects of ECV.
Sociodemographic Factors
Distinct gender differences in ECV and its effects have also been documented. Findings indicate that girls are less exposed to violence than boys, and that they display more internalized behavior problems than boys after ECV (Chen, 2010), whereas boys are exposed to more violence and show more externalized behavior problems than girls (Rescorla et al., 2007). Age has also been recognized as a possible moderator of the relationship between ECV and internalized behavior problems (Buckner, Beardslee, & Bassuk, 2004). According to Fowler et al. (2009), age does not moderate the relationship between ECV and PTSD. However, these researchers identified higher levels of PTSD symptoms among older girls, and suggested that this could be a direct result of the cumulative effect of multiple exposures. Rescorla et al. (2007) argued that the higher levels of internalized behavior problems observed among older girls can be directly associated with the girls’ physical and emotional maturation, regardless of their exposure to violence.
Perceived family support (PFS) among Palestinian adolescents of both genders is comparable, although boys have reported higher levels of teacher support than girls (Leshem et al., 2016). Family support was found to moderate post-ECV internalized problems among girls and externalized problems among boys (Bacchini, Miranda, & Affuso, 2011). Furthermore, findings have shown that although family support moderates the association between ECV and depression among boys as well as among girls, the moderation effect is stronger among girls than among boys, especially following high levels of ECV (Quiroga, López-Rodríguez, & Willis, 2017). A longitudinal study conducted among a representative sample of children and adolescents in the United States showed that a positive relationship with the mother can moderate antisocial behavior after experiencing peer violence among girls, but not among boys (Yang & McLoyd, 2015). Against this background, the present study examined the role of support from parents and teachers in the relationship of adolescent ECV to internalized and externalized problems.
Socioeconomic Status (SES)
Poverty, low education, low parental presence, low literacy, and poor health are all attributes of low SES that contribute to child maldevelopment (Aikens & Barbarin, 2008). Moreover, research has shown that low SES, which is associated with urban residential settings, may contribute to ECV (Cooley, Turner, & Beidel, 1995; Scarpa et al., 2002). Low SES and its correlates (e.g., adverse childhood, lack of education, and life stress) have also been found to increase the risk of PTSD among adults who have been exposed to trauma (Brewin, Andrews, & Valentine, 2000). A large share of the existing research on ECV and its consequences has been conducted in inner-city communities among samples of at-risk adolescents. However, studies conducted in communities at various SES levels, including high-SES suburban communities, have yielded results comparable with those conducted in low-SES communities. In both cases, the prevalence and rates of post-ECV mental health problems were found to be similar (Leshem et al., 2016; Löfving-Gupta et al., 2014). Thus, we hypothesized that even though low SES contributes to ECV, it has no direct effect on the associations of ECV with internalized and externalized problems. Moreover, we hypothesized that SES has little or no effect on the ability of support systems to protect the adolescents.
Study Objectives
ECV was defined in this study as witnessing and/or personally experiencing physical violent events that occurred within the community, including the neighborhood, school, youth club, and at the home of others. In view of the alarming levels of ECV and its documented effects, we examined the effect of family and teacher support on the associations of ECV characteristics with internalized and externalized problems among Arab and Jewish adolescents in Israel.
Two key models, the compensatory and protective models, explain the contribution of external factors to the relationship between ECV and its effects. Compensatory factors react directly and indirectly to externalized and internalized behavior problems, but do not interact with risk factors (Masten et al., 1988). Protective factors react to risk factors and change the responses of individuals to ECV (Brook, Nomura, & Cohen, 1989). This study tested a combined path model. The model includes direct paths that connect gender, family support, and teacher support to internalized and externalized problems, and indicate a compensatory contribution. The model also includes direct paths connecting gender, family support, and teacher support with ECV, which indicate a direct protective contribution. Indirect contributions are indicated by two-segment paths, such as the path connecting gender to internalized problems through witnessing CV.
Method
Participants and Procedure
The study was conducted among 1,832 junior and senior high school students (805 boys, 1,027 girls) aged 12 to 19 years (M = 16.29, SD = 1.05). Participants were sampled from two Israeli populations: 855 Arabs (360 boys, 495 girls), and 977 Jews (445 boys, 532 girls). To reach demographically systematic samples, communities were selected by type and size of locality, socioeconomic rating of locality, and religious heterogeneity. The sample included localities ranging from 4,000 to 250,000 residents (M = 122,036, SD = 107,442). One junior and one senior high school were selected randomly in each sampled district, and every school sample included at least one class of each age-group. Participants completed anonymous paper–pencil self-administered questionnaires at school during 1 school hour, in the presence of a researcher (the teacher left the classroom for the duration of filling out the questionnaire). Student participation was subject to written parental consent. The questionnaire consisted of demographic questions, as well as measures used in the past and adapted for this study, as described below. The study was approved by the ethics committees at the academic institutes of the authors as well as by the Israeli Ministry of Education.
Measures
Standard measures were translated from English to Arabic and Hebrew, and evaluated for suitability, clarity, and relevance of the questions by Arab and Hebrew speaking professionals who were experts in the fields of sociology, psychology, social work, and education, and who specialized in the topics of violence, family, and adolescence. The translated versions were then pilot tested among Arab and Jewish adolescents from Israel, and further refined for clarity.
ECV
This variable was measured using an adapted version of the My Exposure to Violence Scale (Selner-O’Hagan, Kindlon, Buka, Raudenbush, & Earls, 1998). Some of the original items (home violence, sexual violence, political violence, terror events, and accidents) were removed to conform to the definition of CV in this study. Participants’ ECV over the previous year was rated on a 12-item scale (Cronbach’s α = .83), with two subscales: a 7-item Frequency of Witnessing CV Past Year subscale (Cronbach’s α = .76), and a 5-item Frequency of Personally Experienced CV Past Year subscale (Cronbach’s α = .69).
Internalized and externalized behavior problems
This variable was measured by Arabic and Hebrew translated versions of the Youth Self-Report (YSR) questionnaire (Achenbach, 1991). The 29-item internalized scale, measures the psychological and emotional state of youth (range = 0-58, M = 13.04, SD = 10.66, Cronbach’s α = .92), and the 29-item externalized scale measures behavioral and somatic factors (range = 0-58, M = 12.39, SD = 8.48, Cronbach’s α = .88): The higher the score, the higher the prevalence of internalized and externalized problems.
PFS
PFS was measured using the Perceived Social Support (PSS)–Family tool (Procidano & Heller, 1983). The tool assesses the participants’ subjective perceptions of family support. The translated versions included 20 agree/disagree items (range = 0-20). The Cronbach’s alpha reliability of the Arabic version was .84 (M = 15.23, SD = 3.99), and the reliability of the Hebrew version was .83 (M = 14.56, SD = 2.67).
Perceived teacher support (PTS)
The items in the PTS questionnaire were adapted from the PSS-Family and PSS-Friends questionnaires (Procidano & Heller, 1983), to reflect participants’ perceptions of the support they receive from their teachers. The PTS measure in this study consisted of 13 agree/disagree items (range = 0-13). The Cronbach’s alpha reliability of the Arabic version was .74 (M = 6.40, SD = 2.88), and the reliability of the Hebrew version was .77 (M = 5.27, SD = 2.12). The Arabic and Hebrew translations of the measures were evaluated by Arabic and Hebrew speaking professionals with expertise in the fields of psychology, social work, sociology, and education; and the reviewed versions were pilot tested among Jewish and Palestinian adolescents.
Sociodemographic and socioeconomic characteristics
Participants were asked about the following characteristics: age, gender, parents’ levels of education, and residential density (the number of persons living in the family home divided by the number of rooms at home).
Data Analysis
The tools for data analysis included SPSS and AMOS version 21. The t tests were used to examine demographic differences in the measures; correlations were calculated to examine the relationships among all measures; and multiple regression analyses were conducted to examine the ability of ECV, sociodemographic factors, and support factors to predict externalized and internalized behavior problems. Structural equations model (SEM) analysis was conducted to test the validity of the proposed path model, suggesting direct and indirect links between ECV, sociodemographic variables, support variables, externalized behavior problems, and internalized behavior problems.
Results
Table 1 summarizes the means and standard errors of all study variables, comparing means of the measures for Arab versus Jewish adolescents living in Israel, and using t tests.
Means and Standard Error Mean of Frequency of Study Measures Among Arab and Jewish Adolescents.
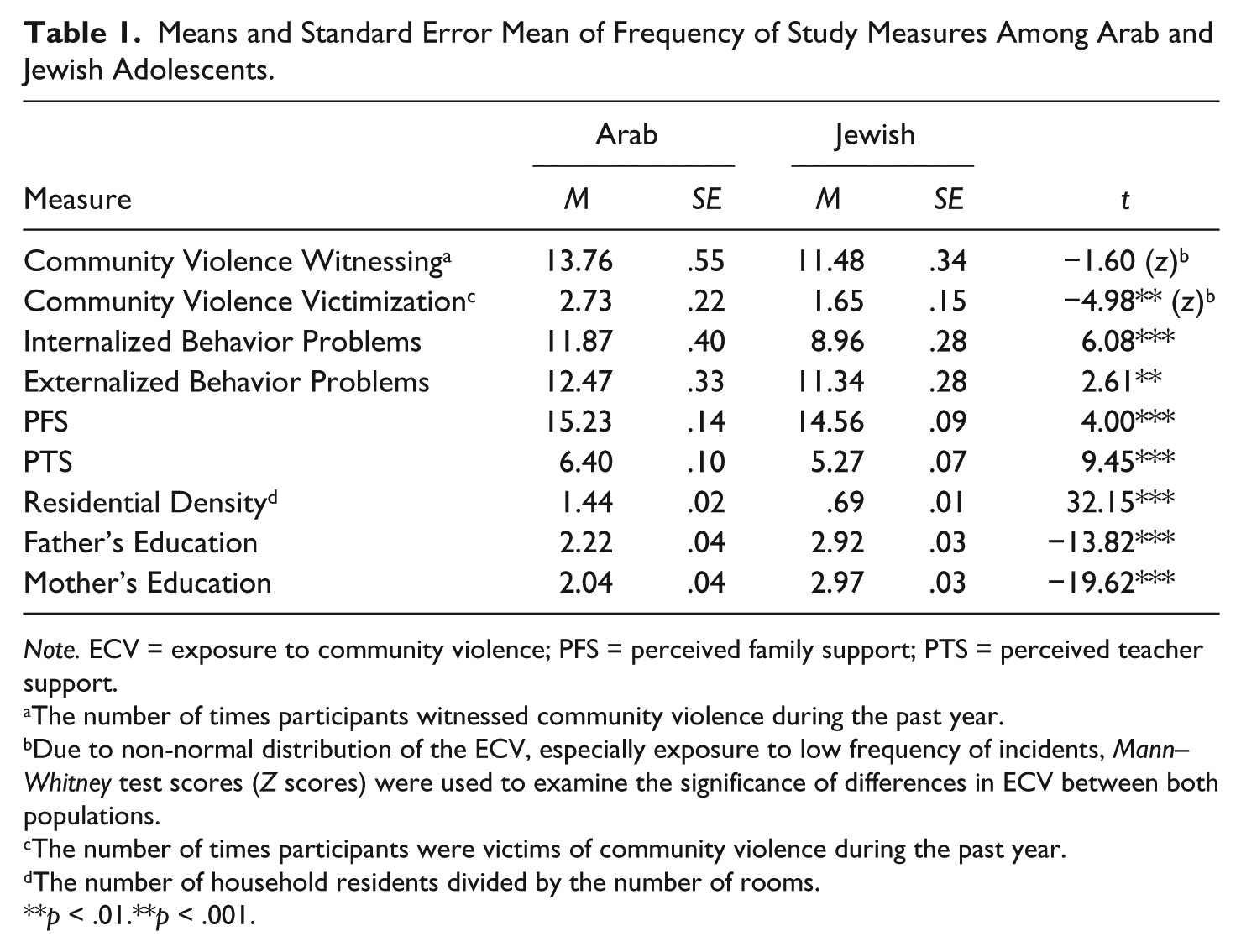
Note. ECV = exposure to community violence; PFS = perceived family support; PTS = perceived teacher support.
The number of times participants witnessed community violence during the past year.
Due to non-normal distribution of the ECV, especially exposure to low frequency of incidents, Mann–Whitney test scores (Z scores) were used to examine the significance of differences in ECV between both populations.
The number of times participants were victims of community violence during the past year.
The number of household residents divided by the number of rooms.
p < .01.**p < .001.
Previous Year Prevalence of ECV
Both Arab and Jewish adolescents reported similar rates of witnessing CV events (M [Arab] = 13.76; M [Jewish] = 11.48.70; Z = −1.60; p > .05). Arab youth reported significantly higher rates of CV victimization during the previous year (M [Arab] = 2.73, SD = .22; M [Jewish] = 1.65, SD = .15; Z = −4.98; p < .001).
Effects of ECV
Arab participants reported significantly higher levels of internalized behavior problems than Jewish participants, (M [Arab] = 11.87; M [Jewish] = 8.96; t = 6.08;p < .001) and higher levels of externalized behavior problems (M [Arab] = 12.47; M [Jewish] = 11.34; t = 2.61; p < .01). Jewish girls displayed higher levels of internalized problems than Jewish boys (M [Girls] = 17.85; M [Boys] = 13.42; t = 6.38; p < .001), whereas Jewish boys reported higher levels of externalized problems than Jewish girls (M [Boys] = 13.54; M [Girls] = 11.64; t = 3.52; p < .001). Arab boys also reported higher externalized problems than Arab girls (M [Boys] = 14.74; M [Girls] = 10.85; t = 5.91; p < .001), with no significant gender differences in the levels of internalized problems among Arab boys and girls (M [Boys] = 11.73; M [Girls] = 11.95; t = 2.63; p > .05).
Perceived Support
Arab adolescents perceived their family support as significantly higher than Jewish adolescents (M [Arab] = 15.23; M [Jewish] = 14.56; t = 4.00; p < .001). The Arab students also reported significantly higher levels of PTS than their Jewish counterparts (M [Arab] = 6.40; M [Jewish] = 5.27; t = 9.45; p < .001).
Sociodemographic Factors
Residential density (the number of people living in the home divided by the number of rooms at home) was significantly higher for the Arab than for the Jewish participants (M [Arab] = 1.44; M [Jewish] =.69; t = 32.15; p < .001), and the parental level of education was significantly higher among the Jewish youth, than among Arab youth, for both fathers (M [Arab] = 2.22; M [Jewish] = 2.92; t = 13.82; p < .001) and mothers (M [Arab] = 2.04; M [Jewish] = 2.97; t = 19.62; p < .001).
Table 2 presents the correlations among all of the study variables. Except for variations in r values, the correlations were similar for the Arab and Jewish participants. For adolescents from both populations, internalized and externalized problems correlated positively with ECV (witnessing and victimization) and negatively with family support, gender, and age. Parents’ education level correlated negatively with residential density (see Table 2).
Bivariate Analysis: Correlations Among ECV, Internalized and Externalized Behavior Problems, Support Variables, and Sociodemographic Characteristics.
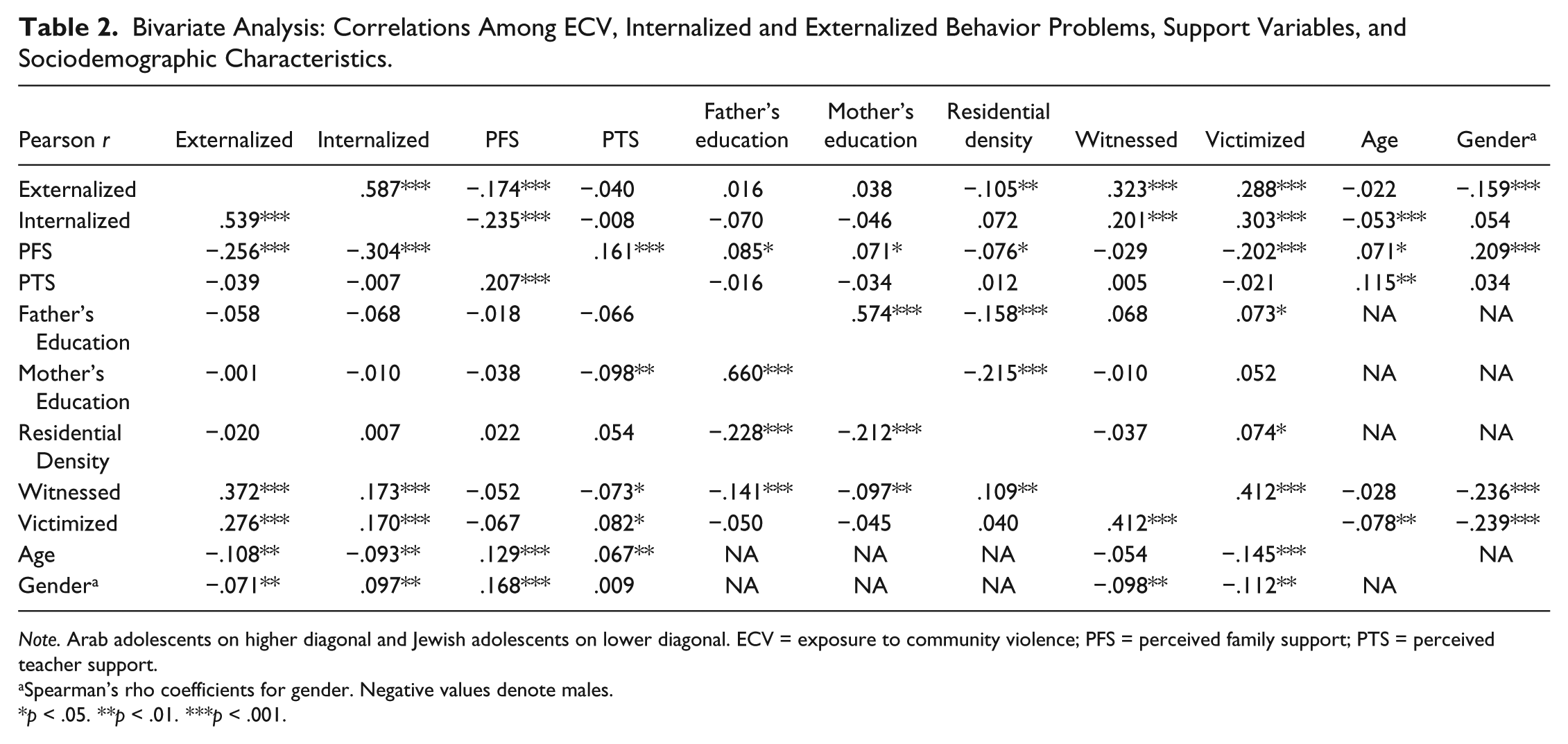
Note. Arab adolescents on higher diagonal and Jewish adolescents on lower diagonal. ECV = exposure to community violence; PFS = perceived family support; PTS = perceived teacher support.
Spearman’s rho coefficients for gender. Negative values denote males.
p < .05. **p < .01. ***p < .001.
Predictors of Internalized and Externalized Problems
The results in Table 3 indicate that externalized as well as internalized problems among youth in Israel could be predicted by some of the tested sociodemographic factors (R2Externalized = .057, p < .001; R2Internalized = .036, p < .001). Ethnicity predicted both externalized (β = −.130, p < .01) and internalized (β = −.112, p < .01) problems, whereas gender (β = −.195, p < .001) and residential density (β = −.103, p < .01) had additional significant roles in predicting externalized problems. When ECV was entered into the model, the explained variance increased by .104 (R2 = .161, p < .001) for externalized problems, and by .054 for internalized problems (R2 = .090, p < .001). Witnessing CV (β = .243, p < .001) was the strongest predictor of externalized problems, and victimization of CV (β = .198, p < .001) was the strongest predictor of internalized problems, whereas ethnicity remained a significant predictor of both types of problems (βExternalized = −.100, p < .01; βInternalized = −.096, p < .05). The addition of support factors increased the explained variance by .040 (R2 = .161, p < .001) for externalized problems, and by .077 for internalized problems (R2 = .161, p < .001). However, family support was the only factor that had a significant predictive role (βExternalized = −.206, p < .001; βInternalized = −.287, p < .001). In the last model, the interaction between teacher support and witnessing CV had significant role in predicting internalized problems (β = −.105, p < .01). Ethnicity maintained a significant role in all models, where it predicted higher levels of externalized and internalized problems among Arab youth.
Regression Analysis: Ethnicity, Sociodemographic Characteristics, ECV, and Support Variables as Predictors of Externalized and Internalized Problems.
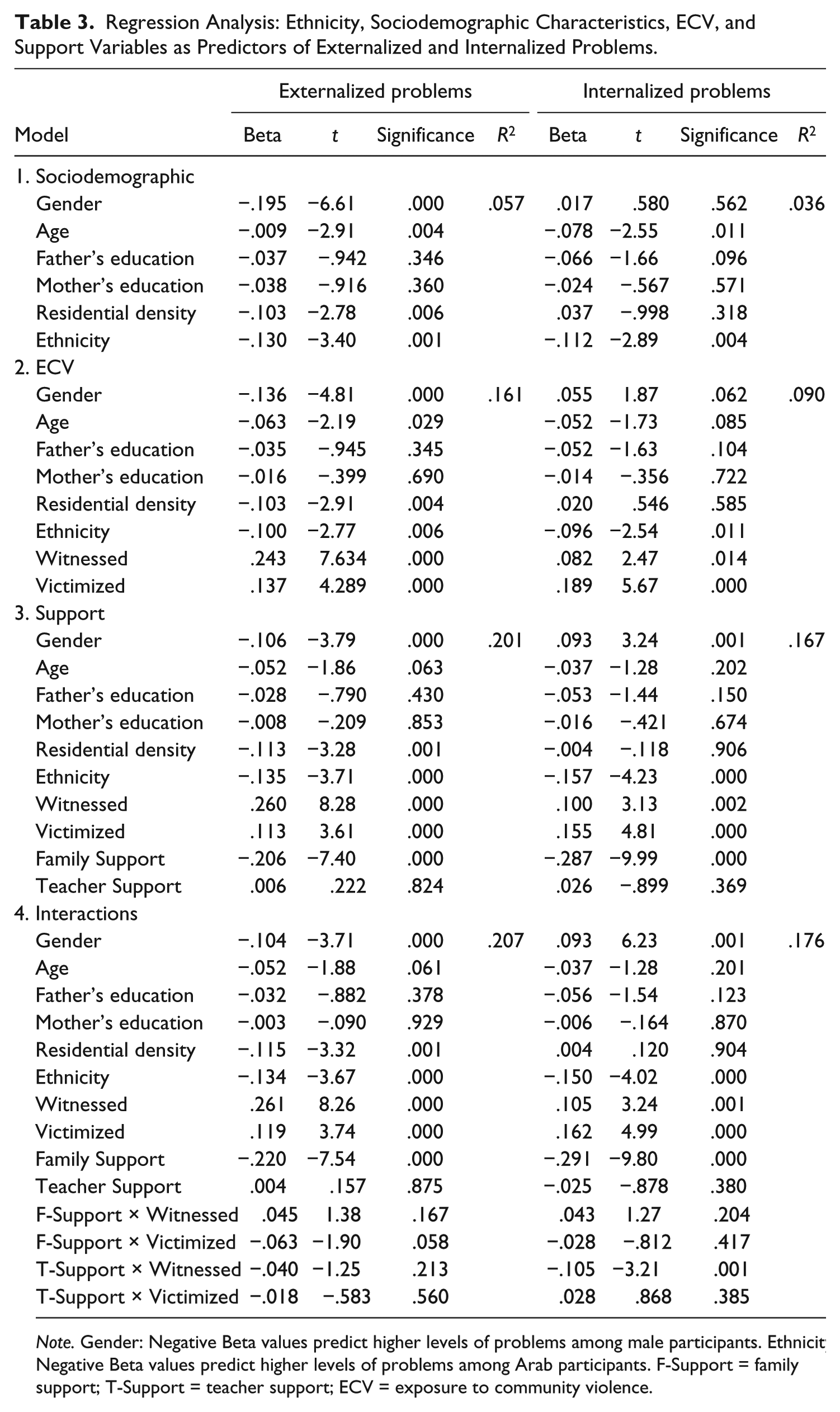
Note. Gender: Negative Beta values predict higher levels of problems among male participants. Ethnicity: Negative Beta values predict higher levels of problems among Arab participants. F-Support = family support; T-Support = teacher support; ECV = exposure to community violence.
Path Model Validation
The model proposed in this study presents a set of relationships among ECV, internalized behavior problems, externalized behavior problems, PFS, PTS, and sociodemographic factors. Based on the results of the multiple regression, we adjusted the model to reflect the tested relationships. Figure 1 summarizes the results of the SEM for both populations. We found a good model fit between the empirical data and the proposed path model: χ2 = 22.89, df = 8, χ2/df = 2.86, p < .01, comparative fit index (CFI) = .993. It is important to examine the path indices and their significance to provide additional criteria for assessing the model. Figure 1 shows the standardized regression coefficients and significance levels for Arab and Jewish adolescents. The regression coefficients in the model indicate that witnessing CV (β [Arab] = .11, p < .01; β [Jewish] = .14, p < .001) and CV victimization (β [Arab] = .23, p < .001; β [Jewish] = .11, p < .001) played a statistically significant positive role in predicting internalized behavior problems and externalized behavior problems for youth from both populations (see Figure 1). Of the two support variables tested in the model, only PFS was significantly related to the effects of ECV: Higher PFS scores were linked with lower levels of externalized behavior problems (β [Arab] =.12, p < .001; β [Jewish] = −.24, p < .001) and internalized behavior problems (β [Arab] = −.21, p < .001; β [Jewish] = −.31, p < .001) among youth from both populations. PFS was also associated with lower levels of CV victimization among Arab youth (β = −.18, p < .001), producing an indirect effect on externalized and internalized behavior problems. PTS was not significantly related to ECV effects, but it was related to lower rates of witnessing CV among Jewish youth (β = −.10, p < .001). This suggests that higher rates of PTS are indirectly linked with lower internalized and externalized behavior problems. Gender was the only demographic factor with significant path effects: Arab boys were found to have significantly higher ECV rates than Arab girls (Witnessing β = −.13, p < .001; Victimization β = −.09, p < .05) as well as higher levels of externalized behavior problems (β = −.13, p < .001), whereas Jewish boys showed higher rates of ECV than Jewish girls (Witnessing β = −.17, p < .001; Victimization β = −.14, p < .001), but no significant difference was found in externalized behavior problems. Both Arab and Jewish girls showed a significantly higher prevalence of internalized problems (β [Arab] = −.08, p < .05; β [Jewish] = .12, p < .001) as well as higher levels of PFS than boys (β [Arab] = .18, p < .001; β [Jewish] = .12, p < .001).

Path model for predicting the relationship between exposure to CV, internalized behavior problems, externalized behavior problems, sociodemographic characteristics, PFS, and PTS among Arab and Jewish Youth in Israel.
Discussion
The main objective of this study was to examine the extent to which family and teacher support could moderate and/or mediate the relationship between ECV and internalized and externalized problems among Jewish and Arab adolescents in Israel. Our results confirm the hypothesis that support from family and teachers mediates the relationships between ECV and externalized as well as internalized problems, and that support from teachers moderates the relationships between ECV and internalized problems. A comparison of ethnic groups while statistically controlling for the contribution of socioeconomic factors revealed that the levels of externalized and internalized problems were higher among Arab youth than among Jewish youth, whereas the levels of ECV and support were similar. Jews and Arabs in Israel typically live in separate municipalities or in separate neighborhoods in the same city. They attend separate schools, use different religious and community services, and spend their free time in separate settings. Arab youth (especially boys) reported higher rates of personal experience with CV than Jewish youth, but no significant differences between Arab and Jewish youth were found with regard to witnessing CV. Among both groups, the prevalence of witnessing CV was significantly higher than the prevalence of personal victimization, supporting the findings of previous studies conducted among various populations (Haj-Yahia et al., 2013; Salzinger et al., 2011). The lower SES indicators found among the Arab youth participating in this study coincide with the general lower SES of the Arab population in Israel, where most Arab communities are in the lowest socioeconomic groups (Israel Central Bureau of Statistics, 2008) as low earning power and economic disadvantages are characteristics of national-ethnic minorities. These characteristics can be attributed to the ethnic segregation rooted within the social structure, where minorities have limited employment opportunities and limited abilities to integrate into the majority economic structure (Yonay & Kraus, 2001). Furthermore, many Arab men in Israel are unskilled workers, and they find it difficult to keep their jobs after age 45 years. Thus, unemployment rates among Arab men in Israel are 75% higher than among Jewish men (Sa’di & Lewin-Epstein, 2001).
The Arab participants in the study reported higher levels of both internalized and externalized behavior problems than the Jewish participants. We believe that this finding could be explained by psychological difficulties that national-ethnic minorities experience while reacting to and dealing with exposure to violence, as documented in previous studies. For example, the Hispanic population in the United States reported higher prevalence of PTSD symptoms and depression symptoms than non-Hispanics after the events of September 11th (Galea et al., 2004), and Muslim Palestinians in Israel reported a higher prevalence of PTSD symptoms and depression symptoms than Jews after exposure to terror events (Hobfoll, Canetti-Nisim, & Johnson, 2006). The researchers concluded that the differences between ethnic minorities and the majority population are related to the lower level of personal resources among national-ethnic minorities. This impairs their resilience and places them “closer to the edge” when they require additional internal resources, to the point where the lack of resources becomes critical (Hobfoll et al., 2006). Furthermore, the Arab minority in Israel is characterized as a collectivistic society, where individual-coping mechanisms are less functional than in individualistic societies (Yeh, Arora, & Wu, 2006). That is, individuals tend to refrain from seeking help (Hall, 2003), especially from formal sources that are associated with the majority society (Cauce et al., 2002).
Arab adolescents in this society also reported higher levels of PFS and PTS than Jewish youth. We assumed that the higher levels of perceived support are related to the central role of the family and the community in the collectivist Arab society. Regarding the relationship of individualism and collectivism to coping, social support, anxiety, and avoidance, participants from collectivistic societies were found to have lower coping skills and higher PFS than those from individualistic societies (Frías, Shaver, & Díaz-Loving, 2014). These findings can be attributed to the individual’s commitment to the group, as well as to the expectations that individuals in collectivistic societies will cope passively, without group support. These assumptions are also supported by a study that focused on differences in coping among members of collectivistic versus individualistic societies in Israel. In that study, Arab students were found to be less assertive than Jewish students in expressing their needs, and they were more likely to end social relationships as a tool for dealing with stress (Peleg & Zoabi, 2014).
The results of the multivariate model indicate that witnessing ECV and personal experience with ECV predicted externalized behavior problems among Arab as well as Jewish youth, whereas witnessing ECV predicted internalized behavior problems only among the Jewish youth. Our findings revealed that among Arab youth, the correlation between witnessing ECV and externalized problems was stronger than the correlation between witnessing ECV and internalized problems, whereas the negative correlation of family support with internalized problems was stronger than its correlation with externalized problems. The higher levels of PFS could explain why witnessing ECV failed to predict internalized problems among Arab youth following exposure.
The findings of the current study showed that PFS contributed significantly to predicting effects of ECV: Higher PFS predicted a lower prevalence of internalized and externalized problems among youth from both populations. In addition to supporting one of the study hypotheses, the significance of these results is also highlighted by the fact that the Arab population in Israel constitutes a collectivistic national-ethnic minority, which differs from the individualistic Jewish majority. Furthermore, we found that the ability of family support to protect teenagers from internalized and externalized problems after ECV can cross national-ethnic boundaries. This finding supports the universal contribution of family support as a protective factor that can promote mental health among youth regardless of national, ethnic, cultural, demographic, and socioeconomic boundaries.
In this study, PTS did not predict the effects of ECV, and there were no correlations between PTS and internalized or externalized problems, contrary to previous studies which have shown that teacher support can moderate the relationship between ECV and PTSD symptoms (Leshem et al., 2016; Löfving-Gupta et al., 2014). Thus, it is possible that teacher support moderates the relationships between ECV and specific consequences from the full range of internalized and externalized problems. Therefore, future studies should examine each effect separately, and seek to determine whether there are distinct protective mechanisms for different problems and different patterns of ECV.
Path model analysis supported the above findings, and added further insights about gender roles. Arab and Jewish boys showed higher rates of ECV and lower PFS than did the girls in both societies. The girls in both populations showed more internalized behavior problems than the boys, whereas the Arab boys showed a higher prevalence of externalized behavior problems than did the Arab girls (there was no gender difference in the prevalence of externalized problems among Jewish youth). The model highlighted the contribution of gender through multiple concurrent paths: Externalized behavior problems were directly related to gender (males → more externalized behavior problems), ECV (higher exposure → higher externalized behavior problems), and family support (higher support → fewer externalizing problems). Gender was also directly related to ECV (boys → higher exposure) and family support (boys → lower family support). The combined effect of the gender-related paths contributed to the overall results: Boys had more externalized problems, and girls had more internalized problems.
The path model results demonstrated the ability of family support to mitigate the effects of ECV on adolescents. However, all of the tested variables explained 16.2% of the variance in the levels of internalized behavior problems among Arab youth (14.7% among Jewish youth), and 19.4% of the variance in the levels of externalized behavior problems among Arab youth (24.5% of the variance among Jewish youth). These results, together with the results of the path model, reflect the power of family support to mitigate the effects of ECV among youth. However, they also point to additional significant factors that affect the prediction of ECV-related internalized and externalized behavior problems, and indicate that these factors should be identified and examined among youth in both populations. The ecological model for CV discusses factors in systems at four levels (Cicchetti & Lynch, 1993). CV occurs in the exosystem, where it interacts with macrosystem variables (such as cultural factors, sociopolitical factors, social status, and religious factors) as well as with microsystem variables (such as family support and social support, as well as variables in the children’s schools, clubs, and sports teams). It is also related to mesosystem factors, which include the relationships between microsystems in a person’s social environment, such as relationships between the nuclear family and the children’s school, their extended family, or their network of peers. Factors related to these systems may play a significant role in increasing or reducing the chances of ECV among children and youth as well as the mental health consequences of such exposure (Cummings, Goeke-Morey, Schermerhorn, Merrilees, & Cairns, 2009). As we only examined microsystem factors, it would be worthwhile to examine the role of factors from a broader range of ecological systems in the future.
Limitations of the Study
This was a pioneer study that examined the psychological and behavioral effects of ECV, and explored the potential of family and teacher support to mitigate the relationships between ECV and its effects among Jewish versus Arab adolescents. Therefore, the current study contributes substantially to cross-population research on ECV and mental health, based on a large and socioeconomically diverse sample. This is in contrast to previous studies, which have focused specifically on inner-city communities and on minorities. However, some limitations of the research need to be mentioned.
First, the data were collected using self-report questionnaires as an exclusive source of information, so that the participants’ reports about their past personal experiences of ECV and perceptions of social support could be biased. Although this is the common methodology for data collection in studies on ECV, the findings should be taken with caution.
Second, this study measured the rates of ECV based on the quantity of violent events, but did not measure the types, intensity, or contexts of the events. Moreover, the study focused primarily on exposure to physical violence, and excluded other types of violence (i.e., verbal, sexual, psychological, economic, and social violence) in the community at large as well as in the media, school, and cyberspace. As these types of exposure to violence might contribute substantially to the prevalence of internalized and externalized behavior problems among adolescents, future studies should examine exposure to a wider range of violent events in various spheres. Finally, due to the cross-sectional nature of this study, causal relationships between the variables cannot be determined. Hence, there is a need to conduct longitudinal studies, which provide insights into the diverse characteristics of ECV, its causes, effects, and possible mitigating factors in an attempt to broaden theoretical, empirical, and practical knowledge.
Third, the comparisons in this study were conducted between Jewish and Arab adolescents in Israel. However, comparisons have not been conducted among groups of youth within each of these two ethnic-national societies. The lack of comparisons may diminish the reliability of the results of this study, and may increase the risk of overgeneralizing its results. Hence, future studies on the rates and risk factors of adolescents’ ECV and on the effects of ECV among youth in Israel should carry out comparisons among youth from different groups within Jewish society (e.g., secular vs. traditional vs. religious youth, Israeli-born vs. immigrant youth, Ashkanazi vs. Sephardi youth, youth from different types of localities, that is, youth from cities, development towns, moshavim, kibbutzim, etc.). In addition, comparisons should be carried out among groups within Arab society (e.g., Muslim vs. Christian and Druze youth, youth from different types of localities, that is, youth from rural areas, Bedouin areas, towns, mixed Jewish Arab cities, etc.). Such comparisons can not only contribute to enhancing the reliability and validity of the results of such studies and overcoming the risk of overgeneralizing their results but can also enrich the theoretical and empirical knowledge about the rates, risk factors, and mental health effects of the exposure of Arab and Jewish youth in Israel to CV.
Practical Implications
The findings of this study highlight the significance of family support as a protective factor against the negative effects of ECV. To reduce the risk of ECV on one hand and increase protection against its effects on the other, we recommend implementing family care and enrichment programs to enhance the feeling of family support among youth. It is important that youth and family care agencies, teachers, school counselors, social workers, and other mental health practitioners recognize family support as a central empowerment agent that could support adolescents and help them cope successfully with ECV, while moderating its negative effects. In addition to improving the family support intervention programs that are currently available for at-risk families, we recommend adopting similar programs for the population at large. These programs should focus on three levels of intervention: increasing parents’ awareness of the high levels of exposure of youth to violence in the community, enhancing parents’ awareness of the importance of family support as a focal point for dealing with the negative effects of ECV, and providing families and parents with tools to improve their support to their children while increasing the adolescents’ levels of PFS.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grants from the CRB Bronfman Foundation, the Sara Moses Fund, the Sondra and Chen Feldman Fund, and the Milton Rosenbaum Fund.