
Abstract
Family Support Groups (FSGs) are developed for family members of mentally ill offenders. This study investigates family treatment expectations and experiences of an FSG. Family members were interviewed before (n = 20) and after (n = 17) attending an FSG. Results show that family members hesitated or were curious about the FSG, expected to receive peer support and universality of problems, to receive information and advice and thought about the safety and respect of the group. Family members experienced the treatment as helpful because it was supportive, they gained new insights and they felt relieved and satisfied. Many family members see the guidance of the therapists and the differences in family and gender roles as an added value of attending an FSG. However, considering the limitations of the study, future studies should gain insight in and stress the importance of the meaning of therapeutic processes for family members confronted with different psychiatric disorders and/or situations.
Keywords
Introduction
In Belgium, mentally ill offenders are simultaneously considered as a potential danger to society (“offenders”) and as a person who needs treatment and care (“patients”), for which they are placed under an “internment measure” (Vandevelde et al., 2011). Since October 1, 2016, The Law on Internment of Mentally Ill Offenders (May 5, 2014, amended by the Potpourri III-law of May 4, 2016) came into force, describing the measure of “internment” as “a safety measure to protect society and that simultaneously aims to ensure that the mentally ill offender is provided with the care his/her condition requires in view of his/her reintegration into society” (Casselman, De Rycke, Heimans, & Verpoorten, 2017; Heimans, Vander Beken, & Schipaanboord, 2015, p. 1051). This Law states that persons can be subjected to an internment measure: (a) if their criminal offense harms the psychical and psychological integrity of a third party, (b) if they have a mental illness at the time of the offense, and (c) if there is a danger of committing new offenses. The internment measure can be enforced for an unlimited period in time (Casselman et al., 2017; Vander Beken, Heimans, & Schipaanboord, 2016). Internationally, a large number of studies have addressed the challenges that mentally ill offenders are confronted with, their recovery process and the shift from a burden-oriented perspective toward more strengths-based approaches (e.g., Aga, Vander Laenen, Vandevelde, Vermeersch, & Vanderplasschen, 2017; Barnao & Ward, 2015; Robertson, Barnao, & Ward, 2011). However, it is important to be aware that not only the mentally ill offenders, but also their social network (more in particular their family members) are confronted with both a relative’s mental illness and criminal offense, causing different emotional, social and psychological burdens (Rowaert et al., 2016; Rowaert, Vandevelde, Lemmens & Audenaert, 2017; Tsang, Pearson, & Yuen, 2002). Raised levels of stress are mentioned by the family members, because of the violence within the family, the double stigmatization and the disintegration of family relationships (Absalom-Hornby, Gooding, & Tarrier, 2011; Ferriter & Huband, 2003; James, 1996; McCann, McKeown, & Porter, 1996; Pearson & Tsang, 2004; Tsang et al., 2002). Yet, many of these family members—the majority of whom are parents—take on an ongoing caregiving role for which they often feel unprepared (Corsentino, Molinari, Gum, Roscoe, & Mills, 2008; Marsh & Johnson, 1997; Wynaden, 2007). About 70% of mentally ill offenders residing in a forensic psychiatric setting in (Northwest) England and Wales have contact with their family members and 56% of them is involved in the discharge planning (Absalom, McGovern, Gooding, & Tarrier, 2010; Canning, O’Reilly, Wressell, Cannon, & Walker, 2009). But, many often lack sufficient support from friends, family members or professionals, and thus have little opportunities to disclose their concerns such as who will take care of their relative in the future (Corsentino et al., 2008; MacInnes & Watson, 2002; Nordström, Kullgren, & Dahlgren, 2006). Moreover, many family members are in need for information, peer support and recognition (Nordström et al., 2006; Ridley et al., 2014; Rowaert et al., 2017).
The last decade, research has focused on the role of social network members in relation to offender risk assessment and management (Pomp, Spreen, Bogaerts, & Völker, 2010) and the prevention of crime (Martin, 2002; Oberwittler, 2004). Several studies have shown that increased levels of social support are associated with a reduction in criminal behavior (Colvin, Cullen, & Vander Ven, 2002; Cullen, 1994; Nakhaie & Sacco, 2009; Pflueger, Franke, Graf, & Hachtel, 2015). In forensic psychiatric settings, Forensic Social Network Analysis (FSNA) is used to define social relationships in terms of risk (and severity) of recidivism (Pomp et al., 2010; Ter Haar-Pomp, Spreen, Bogaerts, & Völker, 2015). Yet, it is crucial to differentiate between positive social (e.g., stable friendships) and risk-increasing resources (e.g., friends lacking social skills) (see e.g., Bolger, Zuckerman, & Kessler, 2000; Resnick, Ireland, & Borowsky, 2004). Based on the results of FSNA, interventions matching with the risk profile of the patient can be selected (ter Haar-Pomp, de Beer, van der Lem, Spreen, & Bogaerts, 2015). Family treatment programs addressing the relationship and the normative dimensions of family therapy (e.g., Functional Family Therapy [FFT] or Multisystemic Therapy [MST]) have positive effects on the reduction of antisocial behaviour of delinquents (Andrews & Bonta, 2010). Absalom and colleagues (2010) stated that “frequent contact between families and patients, and in this population between families and the forensic services, is a prerequisite for family interventions” (p. 358). Although social support and family interventions are considered to be essential, there is a dearth of family interventions in forensic psychiatric settings (Absalom-Hornby, Hare, Gooding, & Tarrier, 2012). Studies conducted in England and Wales show that a minority of medium secure settings make family therapy available for family members of mentally ill offenders (Absalom et al., 2010; Davies, Mallows, Easton, Morrey, & Wood, 2014; Geelan & Nickford, 1999). Barriers to introducing family interventions in these settings are the fixed and inappropriate visiting hours, the limited contact with and engagement of family members and the lack of sufficiently trained staff members (Absalom-Hornby et al., 2012; Davies et al., 2014; Geelan & Nickford, 1999). However, secure settings do not only focus on family interventions, but also connect with family members in other ways to “bridge the gap between the unit and the community,” as Davies and colleagues (2014, p. 527) have stated. Examples include “Family and Friends days, advocacy services, increasing the contact with families at the point of the patients’ admission via ‘welcome meetings’ and ‘family link meetings’” (Davies et al., 2014, pp. 527-528).
Only recently, Family Support Groups (FSGs) have been developed for family members of mentally ill offenders and aim to support them in dealing with both the relative’s mental illness and the internment measure (Rowaert, Hanssens, Audenaert, Vandevelde, & Lemmens, submitted). These FSGs were held on a neutral location, without the involvement of the patients and a forensic psychiatric setting. An FSG is subdivided into four sessions, each consisting of a particular prescribed theme: Session 1 focuses on self-care of the family members, Session 2 on who is going to take care of their relative in the future, Session 3 on their strengths and capabilities for coping with the situation, and Session 4 is a reflection of the previous sessions. Furthermore, homework assignments are given after each session to have the participants reflect upon the previous themes and the effect on their own lives (Rowaert et al., submitted).
FSGs are conceptually based on systemic Multi-Family Group therapy (MFG) format, which is adapted to a forensic context (Rowaert et al., submitted). MFGs aim to bring families together to reduce stigma and enable participants to expand their social network, as they have become socially isolated because of the situation (Asen, 2002; Asen, Dawson, & McHugh, 2001; McFarlane, 2002). The therapists take on the role of catalyst to help family members connect with each other. In this respect, peer support is very powerful and can promote change, as family members are seen as advisors to one another (Asen, 2002; Asen & Schuff, 2006; McFarlane, 2002). Family members can indirectly learn from each other by being provided psycho-education and mutual support and feedback (Asen et al., 2001; McFarlane, 2002).
A process-pilot study investigating the outcomes of FSG’s has shown that families experience less self-blame as they could learn from and observe others, have greater emotional well-being because they received support from the group, and experience less loss of control over their lives by feeling similar to others and seeing the universality of the problems (Rowaert, Vandevelde, Audenaert, & Lemmens, submitted after revision; Rowaert, Vandevelde, Audenaert & Lemmens, 2018). Furthermore, therapeutic factors regarding relational climate (e.g., group cohesion, support from group, confidence in therapists) were considered to be particularly helpful from the start of the sessions; whereas therapeutic factors such as expressing and experiencing positive feelings, forgetting one’s own problems through helping others, hope from seeing progress in others, guidance from therapists, and getting interpersonal feedback gradually increased over the various sessions (Rowaert et al., 2018).
Although the quantitative studies examined specific helpful therapeutic factors, less is known about the expectations and experiences of family members before and after attending family group therapy. Nonetheless, it is important to “give voice” to family members through qualitative interviews, because there is a need for more profound research on treatment expectations and experiences before and after attending family group therapy (Tighe, Pistrang, Casdagli, Baruch, & Butler, 2012). To our knowledge, this has only been studied within MST and FFT research, which are different from MFG as these family therapies focus on adolescents’ antisocial behaviors. More specific, MST is a family and community-based treatment that empowers family members to obtain resources to cope with adolescents’ antisocial behavior such as substance abuse and criminal offenses (Henggeler & Schaeffer, 2016; Kaur, Pote, Fox, & Paradisopoulos, 2017; Sheridan, Peterson, & Rosen, 2010). FFT is an evidence-based family therapy treatment for adolescents with behavioral problems and their families—it focuses on understanding familial relationships and developing adaptive behaviors that can change maladaptive ones (Hartnett, Carr, Hamilton, & Sexton, 2017; Robbins, Alexander, Turner, & Hollimon, 2016). Although these results are not generalizable to our research context as such—because some aspects are specifically linked to the MST or FFT context—they are important to mention because no other research is available (Hartnett et al., 2017; Kaur et al., 2017). Researchers report that families were reluctant at the beginning, as they were tired, stressed, and felt that they had already tried everything (Tighe et al., 2012). When asked about expectations, they mainly inquired about what was going to happen (Sheridan et al., 2010). When taking part in the family therapy intervention, many family members appreciated the new ideas and the concrete advice they were given, their increase in reflection, the changes in their beliefs, and the improvements in their family functioning (e.g., parenting and communication skills) (Hartnett et al., 2017; Kaur et al., 2017; Tighe et al., 2012). Family members felt heard and supported by the therapists and liked their guidance, as they were empathic, understanding, and sincere. The nonblaming, sincere and encouraging approach used by the therapists led to feelings of being respected and accepted, which created stronger self-confidence and improved mental well-being, and reintroduced hope into the lives of the participants. Through therapy, participants become more resilient and unburdened, as it provides a safe place to ask questions and exchange experiences (Asen & Schuff, 2006; Hartnett et al., 2017; Kaur et al., 2017; Sheridan et al., 2010; Tighe et al., 2012).
Family members’ treatment expectations and experiences are important for identifying potential problems or limitations of an intervention, and they can provide insight into how it can be improved in the future (Tighe et al., 2012). The present study focused on treatment expectations and experiences of family members before and after attending an FSG. The study considers the views of family members with regard to the changes the FSG brought into their lives.
Method
Sample
An information leaflet was disseminated in several settings in Flanders—for example, (forensic) psychiatric facilities, prisons, nonprofit organizations for family members of persons with a mental illness, and ambulatory mental health services—to recruit participants for two FSGs. These setting were assumed to provide contact with family members of mentally ill offenders. Participants were selected based on the following inclusion criteria: (a) having a relative with a current or past internment measure who has a diagnosis of schizophrenia, psychotic or bipolar disorder, and (b) being 18 or older. The inclusion criteria were limited to persons with schizophrenia, psychotic, or bipolar disorder because (a) the current article relates to a pilot study in which the application of FSGs was adjusted to the forensic context; (b) the FSG in the current article is based on family therapy for family members of schizophrenic patients (Asen, 2002; McFarlane, 2002); (c) research has indicated that family interventions are essential, especially for patients with a diagnosis of schizophrenia or psychosis (Davies et al., 2014); and (d) the focus on specific disorders leads to homogeneity within the data.
The Ethics Committee of the Ghent University Hospital approved the study (EC decision: B670201526897).
Participants
In total, 20 persons with a mean age of 59.5 years (SD = 12.66, range: 28-75) gave informed consent to participate in the study. Before the start of the first session, every participant (n = 20) was interviewed about their expectations, which were then analyzed. Still, during treatment, three persons dropped out: one father did not attend any session, and two mothers attended only one session. Therefore, after treatment, only 17 interviews were conducted and analyzed concerning the participants’ treatment experiences. Most of the family members were female: 11 mothers, two sisters and one daughter. In addition, five fathers and one brother participated.
Data Collection
One week before the start of the first session (pretreatment) of the FSG, in-depth interviews were conducted about the expectations family members had about participating in an FSG. Posttreatment in-depth interviews were conducted 1 week after the last session. These interviews aimed to map the treatment experiences family members had when attending an FSG. Topic lists were used (see Appendix 1) with questions about the current situation of their relative and their expectations toward the FSG (pretreatment) and about the impact that the FSG had on their lives and how they experienced the treatment (posttreatment).
Data Analysis
In this study, it was considered important to “give voice” to the treatment expectations and experiences of family members who attended an FSG. A qualitative research method was chosen to represent the richness and the complexity of the family members’ lived experiences (Elliott, 2010; Pistrang & Barker, 2010). The pre- and posttreatment in-depth interviews were transcribed verbatim and analyzed using Nvivo 11 (QSR International Pty Ltd, 2015). Thematic analysis was used, because it is “a method for identifying, analysing, and reporting patterns (themes) within data. It minimally organises and describes your data set in rich detail” (Braun & Clarke, 2006, p. 6; Pistrang & Barker, 2010). An inductive approach was used to derive themes closely linked to the data (Braun & Clarke, 2006, 2012; Mortelmans, 2011), which was important as this study aimed at capturing the expectations and experiences of family members who participated in an FSG. The first author of this research paper analyzed the data of both pre- and posttreatment separately, by using an open coding process closely linked to what the family members said. Afterwards, these codes were generated to (a) pretreatment themes (e.g., emotions, support, general prospects) and (b) posttreatment themes (e.g., quality of the treatment, emotions, experiences, lessons learned from the sessions, roles in the group, and homework assignments) to form two separate tree structures which were discussed with the coauthors of this study. The analysis was subdivided into two domains—(a) expectations and (b) experiences—each generating four themes (see Table 1).
Expectations and Experiences of Family Members Participating in an FSG.
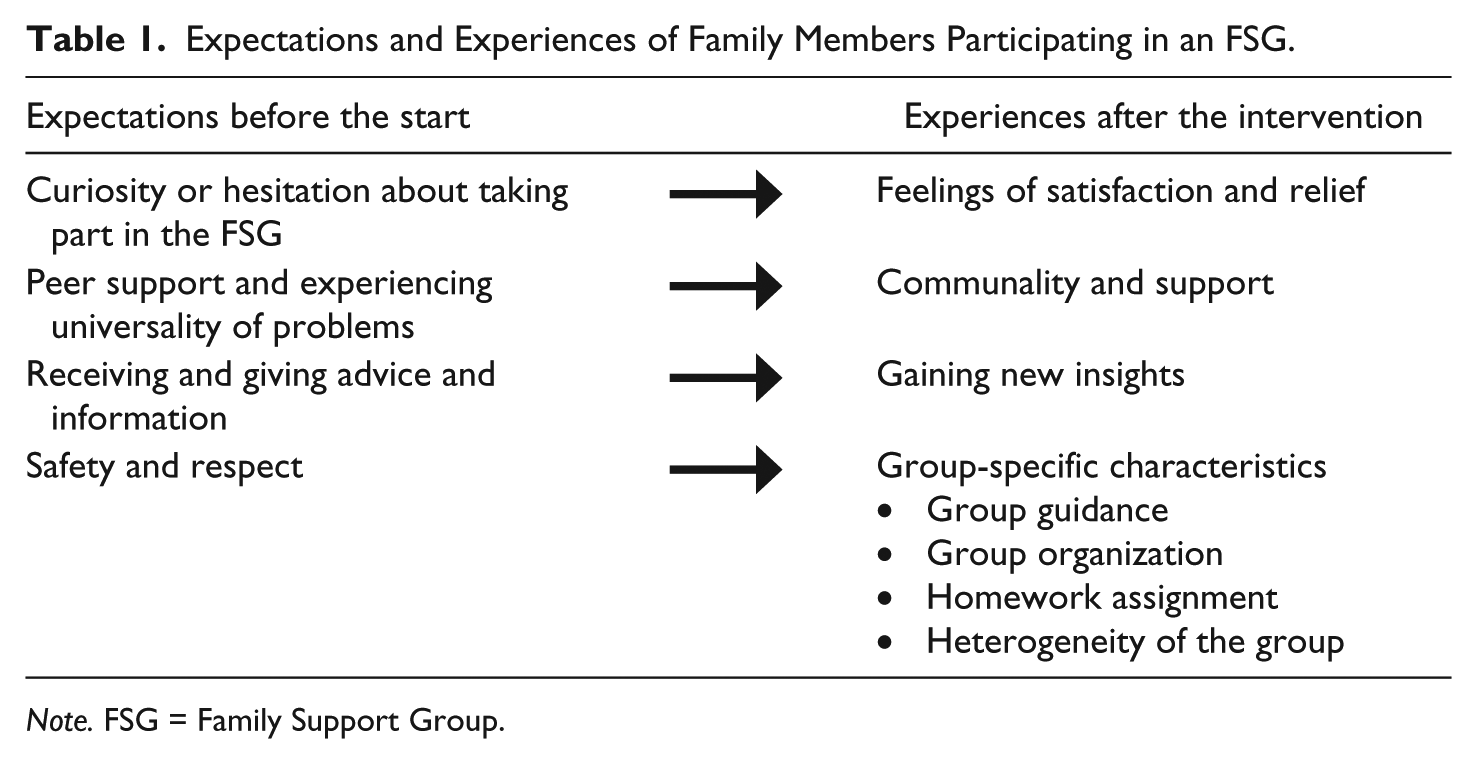
Note. FSG = Family Support Group.
Results
Treatment Expectations
When family members were asked about their expectations of the FSG, they described various topics: (a) curiosity or hesitation about taking part in the FSG, (b) peer support and experiencing universality of problems, (c) receiving and giving advice and information, and (d) safety and respect. Some did not have any expectation and went with an open mind.
I do not have any expectation, but I think it will give me in a way a satisfied feeling. (Mother)
Curiosity or hesitation about taking part in the FSG
Some family members said they hesitated to participate in the FSG because of some practical concerns (e.g., combination with working hours) or because they did not know what they had to do in an FSG or what they should expect from it. Yet, the majority did not hesitate and were curious about what the FSG was about.
The first time I received the information about the FSG, I did not react, because I thought what can I say or do there? […] But I always have the idea that, by telling my story, I can make other people understand about communicating with professionals or about the confrontation with the internment measure. (Mother)
Peer support and experiencing universality of problems
Peer support and coming into contact with others in the same situation is mentioned by many family members. However, this expectation gives some family members an ambivalent feeling: on one hand, they find peer support very positive; but on the other hand, they are afraid about possible differences in coping among the participants.
On the one hand, peer support can give you a pleasant feeling, because nobody really can understand what the situation [having a mentally ill offender as a relative] is about, unless you have to deal with it yourself. On the other hand, they are all people who are coping with their situation in a different way. Many are at a different stage in getting over it. Perhaps anger can dominate the group and demands energy from the others. (Daughter)
Some family members expect to learn from other participants by hearing other stories and getting to know how others cope with the situation. They hope to recognize their own situation in other stories and to receive recognition from other family members in how they cope with the situation. Furthermore, many also want to help others from their own (positive) experiences.
To hear the experiences of other families and to share my experience, which is now more or less positive. To know I am not alone in my situation, because before I always blamed myself for what happened to my son. (Mother) I want to learn from others and hear which course they have followed, which I think, in many cases, will not be very positive […] Not only how they have dealt with it emotionally, but also practically. (Sister)
Meeting others is important for many family members as they have a need to feel they are not alone in their situation.
Alone is still alone, but with more you are stronger. (Mother)
One participant also has the feeling that attending an FSG will not only help herself, but also her relative. Besides, many family members hope that some things will change in the future. Moreover, they argue that other family members should not be confronted with the same problems they have had to deal with.
I think that contact between families will not only help ourselves, but will also be positive for the patient. As we will know more about how we can cope with the situation.(Mother)
Receiving and giving advice and information
Some participants hope that they can receive information that will help their relative’s situation. Others also express the hope of receiving tools, not only from other participants, but also from the therapists leading the group. Furthermore, some want to get advice about what they can do for their relative in the future, because many—especially parent—are very worried about what will happen to their child if they are no longer around.
I hope the other family members will give me answers to my questions, especially about what will happen in the future and how they think about it. (Mother)
Safety and respect
The majority express the desire to actively participate in the FSG—however, a few family members prefer to listen to others instead of speaking themselves. Others say that they hope there will be attention to safety in the group and respect for the integrity of the participants.
I think participating actively is important. […] I hope that, besides telling our stories, attention is also given to safety, respect and the tempo of the participants. (Brother)
Experiences and Feelings After Attending the FSG
When family members were asked about their treatment experiences, some of their answers showed their expectations were fulfilled. They mentioned more helpful (therapeutic) experiences than before attending the FSG. Family members experienced (a) communality and support, (b) gaining new insights, (c) feelings of satisfaction and relief, and (d) group-specific characteristics.
Communality and support
Participants report that experiencing feelings of communality is helpful, because in the FSG they get the opportunity to discuss their situation with others in the same (or similar) situation. This is experienced as useful, as many family members often do not have the possibility to talk about their situation with friends or family members. Within this group, they are confronted with people who are dealing with a similar situation and understand what they are going through. This helps them to tell their story easily, as they are aware that the others know how it feels. A daughter described the FSG as a mirror for my own feelings and coping strategies.
You all went through similar situations, which you cannot discuss with outsiders. In this group, you meet people who understand the situation you are dealing with. (Father) People who attend this group all know how it feels. The recognition is very supportive.(Sister)
Many family members had the feeling, often for the first time, that they are not alone in having to deal with both a relative’s mental illness and internment measure. By meeting others, family members feel supported and are able to experience solidarity and universality with the problems and situation.
We always thought we were the only ones who were confronted with a mentally ill offender. And attending this group made me aware that we are not alone. You start thinking of the fact that everyone has to deal with the same issues. (Mother) Meeting others who are confronted with the same misery, that is somehow supportive. Especially seeing people who were very combative and had already tried everything to make sure their child would receive the treatment he needed. (Mother)
Gaining new insights
Family members found the content of the treatment sessions interesting and helpful as they gained insight into their challenges and problems. The treatment within an FSG helped them reflect upon their own lives and the lives of their relatives. Especially because the discussion included the fact that they are stuck between the reality of the law and the reality of the patient’s needs.
This group [FSG] is made of people who are involved and who are living in the situation. While usually everything is kept superficial, the content of these sessions was always very thoroughly discussed. You are sitting there between people you do not know and you commit yourself. Something I basically never do. (Mother)
Some family members also put their own situation into perspective by hearing others tell their story. This helped many of them reflect on their situation by telling themselves: It can get a great deal worse than the situation we are in now. Many family members compared situations of others with their own and found that, in general, the problems others were confronted with were more severe.
I found others had to deal with a much more severe situation than mine. But then I thought “we are companions in misfortune.” I have realized that other family members also keep on fighting [. . .] So, the interaction between my situation and the situation of others induced something like confidence. I got the feeling that you do not have to think it is all lost with those children and with those problems. It is still liveable, even as difficult as it is − and that is something I have learned from the other participants. (Father)
Feelings of satisfaction and relief
When asked about their emotions after the sessions, family members reported that they were relieved and satisfied—one mother even described it as a satisfied tiredness. The sessions also energized many of the participants—but, because the sessions were also experienced as very intense, “tired” and “energized” often went hand-in-hand.
Usually I was very tired, but in a strange way the sessions also gave me energy. It is tiring to sit there for two hours, to listen and to tell your story. But when I drove home, I thought about the session and the things other participants had said, and how I could move on in my own situation. (Sister)
Not withstanding the intensity of the sessions, many family members had a good feeling about the FSG, as they learned from other participants’ situations by observing and learning about how others cope with their situation.
The fact that people come to these sessions—even if they won’t help their relative’s situation—shows how important it is for people to relieve their feelings. (Mother)
Group-specific characteristics
Many family members also point to the significance of an FSG and are convinced this format can be useful for other family members. Some also feel that an FSG should be something permanent for family members to go to—because, for some, four sessions were too short. The sessions merely started some reflections that the participants should take further and work on themselves.
Four sessions are definitely too short. You have planted a seed and we need to let it germinate now.(Mother)
In this regard, almost all of the participants conveyed their thoughts about some specific group characteristics, such as group guidance, group organization and homework assignments, which are discussed below.
Group guidance
The guidance from the therapists was deemed necessary by every family member. In particular, the therapists’ way of focusing on specific subjects and guiding the group toward prescribed themes, focusing on the strengths and capabilities of family members, was considered especially important.
I think the guidance from the therapists is essential − otherwise, the FSG would become a lamentation, with everyone recounting his misery. Then, it would no longer have been a supportive group.(Daughter)
Family members described the therapists as respectful and understanding, as good listeners, and as persons who were able to bring in a positive note and also acted firmly to give each participant an equal chance to tell their story.
They were very good listeners […] Now and then, it was humorous with smiles and laughs. People should be able to laugh, despite the difficult situation. (Father)
Many family members experienced the therapists as added value for the group, because they gave feedback and could anticipate each other. Some family members were of the opinion that they would not have told each other so many details if no therapists were involved.
Getting feedback from the two psychiatrists was interesting, because you are so emotionally involved in your own situation that it’s often hard to see the reality. They can communicate things in a simple way, so that you can get another image of certain situations.(Sister) For us, this was new [attending an FSG], because in all those years we never searched for help for ourselves. Maybe we should have done it sooner.(Mother and Father)
Group organization
Most of the family members felt that 10 participants was a maximum number, because more participants would make the session too short for everyone to be able to ventilate about their situation. Family members have the feeling that more participants would undo the profundity of the FSG and would not lead to the reflection they have now experienced. However, a small number of participants would also be a problem, because then people can go into greater detail, which can be too confronting and too heavy to bear. On the contrary, fewer participants can also be an advantage, as that would make it easier to remember each participant’s situation.
The size of the group was perfect. I think there should not be more people, because then it would take more time and would weaken the connection between the participants. (Mother) Being with a small group can be confronting. For example, if you are a group of only four persons, the FSG can be emotionally charged. (Mother)
Many family members liked the break between the first and the last parts of the session. It helped them have more spontaneous contacts with others, to catch their breath, and to let the first part “sink in.”
Especially when there are severe stories being told, it is important to have a break. So that you can drink a coffee, and people can talk one-on-one with each other. (Daughter)
When family members were asked if they would also want their relative to be involved in the FSG, different reactions were given. Some are of the opinion that they would restrain themselves to say particular things about their relative, so that he or she would not feel offended. Others feel that their relatives could be present, but they do not know if this would bring added value, especially because the content of the sessions would perhaps focus more on the patients than on the family members. Most family members do not express a need to involve their relative, and they also do not know if their relative would be willing to come.
I do not know if it would have added value, because the conversations would be guided in a different way when the person with a mental illness is also involved. The questions that would then be asked could be confronting for the person and even burden him or her. Perhaps it would also give us a sense of guilt when talking about certain aspects of the situation. So, personally, I do not have a need to have my relative involved in an FSG. (Mother)
Homework assignment
Family members liked the homework assignments, as they helped them reflect upon self-care, caring in the future, and using their own strengths to cope with the situation. For some, it was a tool used in the sessions to let you know what the subject during the next session would be. At first, many family members found the homework assignments very simple. Yet afterwards, they were surprised to find that they made them reflect and take action.
When I first heard the assignment, I thought it was childish. But when you start thinking about it and searching for something you can do, then it means more than you thought it did. (Mother) A homework assignment gives you the opportunity to prepare something for the next session and to reflect upon it. It was not explicitly said that this would be the next subject − we were only told that we should think about it. […] A difficult exercise for me was about who will take care of my son in the future? Who will have that responsibility? I do not want to burden my children with it. Therefore, these sessions taught me that I must search for a solution for the future. As long as I live, I will search for a permanent solution for my son − and that is an understanding I have received by following these sessions. (Mother)
Especially the task of the third session—in which family members had to recognize other participants’ strengths and capabilities, which were afterward written down on a Post-it note—has stayed in many family members’ memory. Some of them even kept the Post-it.
There was a lot of truth in that task, we have not yet thrown the Post-it away. […] We have talked about it with each other, and we’ve found a lot of truth in it. I even reflected upon myself, because I need to deal with some things in a different way. And I will work on it. (Mother and Father)
Heterogeneity of the group
During the interview, more than half of the family members said something about how they experienced the different family and gender roles in the FSG. Especially the presence of mothers and fathers was discussed. The majority of the participants were mothers, but a few fathers also attended the group, which made many participants happy. One participant said that a mother is seen as someone who never gives up, and a father as someone who is more powerful in his opinion and distances himself more often from the situation.
The fact that a man will also come to such a group to tell his story and show his vulnerability is very important! I mean the fathers in this group do not hide the problems. My son was no longer welcome with his father. (Mother)
Participants describe the difference in family and gender roles as a “healthy mix” within the FSG. They value the heterogeneity of family roles: not only parents, but also sisters, a brother and a daughter participated in the FSG. Various family members specifically pointed out that an FSG should not be unilateral.
There were a lot of mothers, but that is because they feel more involved with the problems of their child […] But eventually I became aware that my family role as daughter is not very different from the role of parents, because of the parentification. (Daughter) A mixed group is important, because it should not be too unilateral. The “main themes” of the stories are all the same. If, in the beginning, suitable treatment is not immediately available, you all are confronted with the same situations [prison and (forensic) psychiatric care]. (Mother)
There were only a few couples attending the FSG. One couple was struck by the fact that they were the only husband and wife in the group. The couples who attended the group together found it very interesting, as they could discuss the session with their partner. They also found participating together supportive.
I think attending the group as a couple is very interesting, because when we drove home, we discussed what was said […] We could share it together. (Mother and Father)
Discussion
This study investigated the treatment expectations and experiences of family members of mentally ill offenders attending a FSG. Many family members were curious about what the FSG was about before it started. Only a few mentioned that they hesitated a while, due to practical or emotional reasons. This differs from the study of Tighe and colleagues (2012), because they report that family members were at first reluctant to participate in a family intervention because they were stressed, tired and had the feeling that they had already tried everything. This can be due to the fact that family members in this study already had a long history of coping with their relative’s mental illness and the internment measure. Moreover, for the greater part, family members were selected from nonprofit organizations that organize activities for family members, which could have made it easier for these family members to participate in the FSG. Another explanation could be that an FSG aims to support and empower family members without the mentally ill persons being involved. This differs from an MFG, which aims to help the patient in his or her recovery process by engaging family members in the treatment and rehabilitation (McFarlane, 2002).
The results show that, at the end of the four sessions, family members had a satisfied feeling, as their (limited) expectations were fulfilled (see Table 1). Yet, it is noteworthy that most of their expectations (experiencing universality of problems, peer support, and receiving advice and information) were in line with the difficulties (double stigma, social isolation, and no or incorrect information) they had experienced in the years before (Nordström et al., 2006; Tsang et al., 2002; Rowaert et al., 2017). Looking at the experiences, the same trend can be observed, as family members valued the communality, the support from the group, and gaining new insights. The latter helped them to reflect upon their lives and the lives of their relatives, which was developed further in the homework assignments. The homework assignment about taking care of their relative in the future was considered especially important, because many family members had never planned for what will happen to their relative when they are no longer around (Corsentino et al., 2008).
In the interviews, family members mainly mention therapeutic factors considering the relational climate of the FSG, as they talk about support from the group, communality, and the confidence they have in the therapists. This is in line with previous quantitative research reporting that group cohesion, universality of problems, and similarity with others are important from the start of the FSG (Rowaert et al., 2018). Experiencing communality is regarded as important by many family members—not only confronted with a relative’s mental illness—because they want to meet persons dealing with similar situations, as that is destigmatizing and helps build up a social network (Asen, 2002; Asen & Schuff, 2006; McFarlane, 2002). Family members of mentally ill offenders are often socially, emotionally, and psychologically burdened due to the situation they are confronted with—and attending an FSG creates for them the opportunity to talk to other family members in a safe and supportive environment, which can improve their emotional well-being (Asen & Schuff, 2006; McFarlane, 2002; Tsang et al., 2002). Family members can observe others and indirectly learn from their behavior and coping strategies, which in a way is also supportive, as this helps reduce their self-blame and rebuilds self-confidence (Lemmens et al., 2003; McFarlane, 2002; Rowaert et al., submitted after revision). Furthermore, family members develop feelings of solidarity and experience less loss of control over their lives, because participants inspire each other by informal psycho-education and sharing experiences (Asen, 2002; Asen & Schuff, 2006; Rowaert et al., submitted after revision).
Furthermore, this study highlights the important role of the therapists within an FSG. Their respectfulness and understanding are especially highly valued. Many family members often experienced these values with professionals for the first time, as previously they had been confronted with mental health care workers or psychiatrists who did not want to listen to their story or involve them in the treatment of their relative (MacInnes & Watson, 2002; Nordström et al., 2006; Rowaert et al., 2017). Also, in other MFG research studies, the nonblaming and encouraging approach of therapists is considered to be very important (Sheridan et al., 2010; Tighe et al., 2012). Thanks to this, a therapy group can become a safe place for family members to exchange experiences, observe others, and change their beliefs (Sheridan et al., 2010).
Based on the idea of social support and its risk-reducing effect on criminal behavior, studies acknowledge the importance of involving the social network of the patient (i.e., family members) in forensic psychiatric treatment (Colvin et al., 2002; Cullen, 1994; Pomp et al., 2010; ter Haar-Pomp et al., 2015). From this perspective, the FSG is helpful in supporting family members to engage in relationships with their offending relative. An important avenue for future research is to examine the influence of the FSG on recidivism rates of mentally ill offenders. Yet, the difficulties mental health professionals are confronted with—such as professional confidentiality vis-à-vis the mentally ill person, and how they can involve family members—will be important to explore further. This involves that mental health professionals will need to balance between the interests of the patients and those of family members in treatment and care. In this perspective, the idea of a shared partnership, with professionals working together with patients and their families, based on the concept of relational recovery, is important, especially in the light of strengths-based approaches. Relational recovery considers the need to move beyond “individual journeys” and places emphasis on the development of interpersonal acts within offender therapeutic and family therapeutic research (Price-Robertson, Obradovic, & Morgan, 2017). A shared partnership accepts the complexity of people’s lives and of our society, in which concepts like social integration, inclusive citizenship and socialization are amply present (Dewaele et al., 2015). Shared partnerships, however, are still challenged by barriers in the health care system (e.g., patient confidentiality regulations) and barriers relating to family contact (e.g., disruptiveness, poor contact and over-involvement) (Quah, 2017). In our view, professionals should further be encouraged to (re)think and reflect on the vision of their setting with regard to the involvement of, and mutual collaboration with family members (Riebschleger, 2005).
As this is a pilot study, the results are not generalizable, and some limitations of the study need to be mentioned. First of all, the study consists of 2 FSG cycles, with only 17 participants engaged in the complete duration of the FSG. Based on the inclusion criteria, many participants are selected from nonprofit organizations for family members of mentally ill persons, which could have biased the results. The small sample size can also be explained by the fact that some family members do not express a need to participate in an FSG because they have enough support or have the feeling they can cope with the situation they face. Although the FSG is created as a supportive and empowering treatment for family members, the format can also generate a barrier to participation by family members, because they do not want to be regarded by therapists as “second patients” who are in need of treatment. Second, the experiences of family members can be biased, as most of them had a long-standing history with mental health care and had already developed some coping strategies. Third, by only focusing on empowering and supporting family members, the study did not (yet) investigate if attending an FSG may have an influence on the situation and rehabilitation of the mentally ill offenders.
To conclude, this study shows that family members are in need for information and collaboration with professionals. They look for advice and new pathways to improve the situation of their relative. Therefore, this study is important in understanding family treatment expectations and experiences toward a FSG. Future family groups should focus on communality, peer support, and differences in family and gender roles, as the latter was important for many family members to experience solidarity through a heterogeneity of family roles. Therapists will play an important role, guiding the group toward gaining new insights and experiencing positive feelings, like satisfaction and energy. Moreover, homework assignments can help by having family members further reflect upon certain themes being discussed within the group. Future research about FSG should pay attention to different psychiatric disorders, as the hypothesis is raised as to whether other family members experience the same therapeutic factors as helpful. Furthermore, future research should also try to include family members who do not have a long-standing history of taking care of their relative, by trying to contact family members who have only recently been confronted with the mental illness and/or the criminal offense of their relative.
Footnotes
Appendix
Acknowledgements
This study is funded by the Special Research Fund of Ghent University for concerted research actions from 2014 till 2019 entitled: ‘Developing multidisciplinary strengths-based strategies for mentally ill offenders’. We would like to thank the family members who were willing to participate in this study during 3 months.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Special Research Fund of Ghent University.