
Abstract
The aim of the present study was to examine the effects of a 6-week mindfulness training program on mental health, anxiety, depression, aggression, sleep quality, mood states, total mood disturbance, and perceived stress among male Chinese prisoners, and to explore whether the intervention effects differed in long-term and short-term prisoners. Eighty-three male prisoners completed the study, including 39 in the mindfulness training group and 44 in the waitlist control group. Results showed that, compared with the waitlist control group, mindfulness training group showed a significant improvement in mindfulness level (p < .0l), Symptom Checklist-90 (SCL-90; p < .00l), aggression (p < .05), sleep quality (p < .05), and total mood disturbance (p < .0l). Moreover, compared with the short-term prisoners, mindfulness training was more effective on the long-term prisoners in mindfulness level (p < .05), SCL-90 (p < .001), anxiety (p < .05), depression (p < .05), aggression (p < .05), total mood disturbance (p < .0l), and perceived stress (p < .0l). Given the study’s innovation, we discussed its significance and limitations.
Introduction
Mental illness is common among prisoners (Hassan et al., 2011). As a special group, prisoners showed more problems in mental health than people not incarcerated (Sudhinta, 2011). Statistics showed that 70.3% of the prisoners had psychological problems in a mental health screening in China (Lu & Gao, 2015). Studies also showed that inmates displayed high levels of mental distress (Ibrahim, Esena, Aikins, O’Keefe, & Mckay, 2015; Iversen, Sam, & Helvik, 2014), anxiety (Buckaloo, Krug, & Nelson, 2009), depression (Scheyett et al., 2010), and aggressivity (Yuan, Jia, Liu, Liu, & Yang, 2015), which are the four typical mental problems in prisoners (J. X. Liu & Sun, 2005). In addition, inmates were demonstrated to have more obsessive-compulsive symptoms (Calvo et al., 2016), higher sensitivity to the interpersonal relationship (Wulf-Ludden, 2013), less self-esteem (Ireland, 2010), and worse sleep quality (J. Li, 2004). These problems, if not handled properly, may lead to bullying behavior (Ireland, 2010; Unver, Yuce, Bayram, & Bilgel, 2013) and even high possibility of recidivism (Martin, 2016).
Theories that articulate the negative health outcomes of stress explain the relationship between mental illness and imprisonment (Yi, Turney, & Wildeman, 2017). Imprisonment has been conceptualized as a stressful, isolating, and stigmatizing life event (Massoglia & Pridemore, 2015). Although the prevalence of mental health problems is obviously high, inmates seem to be reluctant to seek help. Moreover, the literature suggested that the consequences of the incarceration on mental health can be immediate and persistent (Turney, Wildeman, & Schnittker, 2012), indicating the urgent need of attention to them.
The interventions used to deal with those problems include two main orientations: rectification model and improvement model (Xu, Jia, Liu, & Hofmann, 2016). Rectification model is defined as interventions focusing primarily on the prevention and correction of offensive behaviors to reduce the risk of criminality (Stewart & Gobeil, 2015). However, it may not obtain satisfactory results and, in some instances, even cause the opposite effect (Eason, 2010). Recently, an increasing number of studies have examined the mental health of prisoners (Fazel, Hayes, Bartellas, Clerici, & Trestman, 2016), which is consistent with the improvement model that prisoners can benefit from some therapeutic interventions. Khodayarifard, Shokoohi-Yekta, and Hamot (2010) investigated the effect of individual and group cognitive behavior therapy among male prisoners and found significant improvement in their psychological symptoms. Enright et al. (2016) found that forgiveness therapy was effective in reducing anger and promoting mental health. Gold et al. (2014) adopted music therapy among prisoners and found significant reduction in anxiety and depression.
Among these interventions used in prison, mindfulness-based cognitive therapy (MBCT) is gaining popularity after numerous successful cases (Himelstein, Hastings, Shapiro, & Heery, 2012). One reason is relevant with the settings limitations in prison in which complicated psychological interventions, such as sandplay therapy or hypnotherapy, may be difficult to implement, whereas mindfulness-based training can be easily applied because of its maneuverability. Mindfulness refers to the clear awareness of the outer and inner world, and includes feelings, sensations, thoughts, and emotions of the observer (Brown, Ryan, & Creswell, 2007). Xu et al. (2016) conducted a 6-week mindfulness training program among male Chinese prison inmates and the results displayed significant improvements in mindfulness level, tension-anxiety, depression-dejection, anger-hostility, confusion-bewilderment, and total mood disturbance. The study by Lyons, Cantrell, and Womack (2015) showed that mindfulness-based relapse prevention can reduce anxiety and posttraumatic stress disorder (PTSD) symptoms in male drug-using jail inmates. Samuelson, Carmody, Kabat-Zinn, and Bratt (2016) investigated the effect of mindfulness-based stress reduction (MBSR) in 1,350 inmates and found improvements in hostility, self-esteem, and mood disturbance. Except for satisfactory outcomes in male prisoners, mindfulness interventions had also been found to have pleasing results in female inmates. Ferszt, Miller, Hickey, Maull, and Crisp (2015) found significant improvement in stress, anxiety, and depression among female prisoners after a mindfulness-based intervention. In Kongboonkaew, Bunnrayong, and Srikhamjak’s (2016) study, female inmates reported lower level of anger after participating in a mindfulness-based anger management program. Thus, it can be inferred that mindfulness training is a promising way to improve the mental health of prisoners. In addition, several researchers pointed out the mechanisms by which mindfulness interventions are beneficial for prisoners’ health. Glenn (2012) found that two subscales of mindfulness, namely, acceptance and awareness, were significant predictors of executive functioning in inmates, which was found to show a durable connection with mental health (Akbaryan, 2014).
Nevertheless, most of the studies to date lacked a control group (Xu et al., 2016). Without a control group, we may not be able to clear away other interferences. Moreover, it is still unknown whether prisoners benefit from mindfulness in a similar way. In fact, few studies took the length of imprisonment into consideration, but the literature indicated that the effects of psychiatric treatment for inmates need to differentiate between long- and short-term prisoners (Otte et al., 2017). Adaptation to long-term imprisonment had a deep and profound impact on the prisoner because the process of coping leads to fundamental changes in the self (Hulley, Crewe, & Wright, 2016). It permanently altered their life courses, removed part of their expected life history, and caused harms beyond sentence (Ruth & Adrian, 2006). Compared with short-term imprisonment, more moral and philosophical problems (Liebling, 2014), as well as more severe cognitive impairment (Lapornik et al., 1996), were found in long-term imprisonment. Previous studies showed that inadequate provision of health care in prisons seems to be the cause of poor health in prisoners (Wahbe, 2012), and those long-term prisoners may be influenced in a greater level in comparison with the short-term prisoners. Therefore, long-term prisoners may be in a more urgent need of mindfulness intervention, and there is much room for improvement in mindfulness training (Shinkai, 2012).
In the present study, we examined the effects of mindfulness-based training among long-term and short-term prisoners, respectively, in China. We used the Symptom Checklist-90 (SCL-90, the Aggression Questionnaire (AQ), the Profile of Mood States (POMS), the Five-Facet Mindfulness Questionnaire (FFMQ), the Zung Self-Rating Anxiety Scale (SAS), the Zung Self-Rating Depression Scale (SDS), Pittsburgh Sleep Quality Index (PSQI), and the Chinese Perceived Stress Scale (CPSS) to evaluate their mental problems and how these problems alter. These scales were found to be effective screening tools for severe mental disorders in the prison system (Ignatyev, Fritsch, Priebe, & Mundt, 2016; Terry, Lane, & Fogarty, 2003). We hypothesized that (a) mindfulness training would significantly enhance the level of mindfulness in prisoners, and (b) the effects of mindfulness intervention are significantly better in long-term prisoners than in short-term prisoners.
Method
Participants
Participants were recruited from two prisons in Beijing, China. Ninety-seven prisoners, including both long-term and short-term prisoners, volunteered to take part in the study after participating in the lecture. Among the long-term criminals, 100 prisoners participated in the introduction lecture and 54 of them signed up; 100 short-term prisoners participated in the lecture and 43 of them participated in the study. The long-term male prisoners had remaining prison sentences of at least 10 years. They were imprisoned for serious criminal behaviors such as murder, robbery, kidnapping, or drug trafficking. The short-term prisoners were imprisoned for a maximum of 3 years of sentence. They were randomized into two study groups. Minor adjustments were applied to comply with scheduling conflicts of several prisoners.
Forty-five of them were assigned to the mindfulness training group and 52 of them were assigned to the waitlist control group. Of the 45 in the mindfulness training group, 39 of them completed the entire study. Three participants dropped out because they were not interested anymore in the process, two participants went to hospital because of their sudden health issues, and one participant was transferred to another prison. Finally, 39 (86.7%) of them completed the entire study. In the waitlist group, eight participants were transferred to another prison during the study, so 44 (84.6%) participants completed the entire study. In these two groups (mindfulness training group vs. waitlist control group), the response rate of long-term prisoners is 74.1% and that of short-term prisoners is 100%. The average age of the participants who completed the entire study is 33.3 (SD = 11.0, range = 19-57) and the two groups did not differ in all demographic variables (ps > .05).
Procedure
Participants were recruited through a 1-hr introductory lecture held in the long-term and short-term prisons, respectively. After signing informed consent, they were randomly divided into two study groups (mindfulness training group and waitlist control group). Due to “Prison Law of the People’s Republic of China,” conditions of confinement and prison routines should obey the law, so there isn’t much difference in settings between the two prisons. However, security measures in long-term prisons are stricter. Given the rules and regulations of prisons, we had to shorten the 8-week intervention to a 6-week mindfulness program, which had been successfully applied in an earlier study (X. Liu, Xu, Wang, & Liu, 2013). The pretest assessment was conducted in a quiet classroom in the prison. The posttest assessment was completed by participants after the 6-week mindfulness training or the 6-week waiting period in the same classroom. The waitlist control group received the same mindfulness training after the posttest period (no data were collected this time).
The mindfulness training is derived from MBCT protocol developed by Segal, Williams, and Teasdale (2002). The classic MBCT project is conducted in group settings, including group training, daylong retreat, and homework exercises. Because of the prisoners’ strict daily schedule and limited activity space in Chinese prisons, the training had to make slight modifications in the MBCT integral structure. First, the contents designed for coping with depression were replaced by other meditation practices from the MBSR (Kabat-Zinn, 1990) such as mindfulness yoga. Meanwhile, in Chinese prisons, all prisoners’ group activities were monitored by prison guards, so the guard participated in the intervention process as an observer.
In addition, due to the restraints of privacy and personal space, a daylong retreat and homework exercises, though they are a very important part of the intervention, were difficult to be implemented in the Chinese prison setting. Hence, we replaced them with a short-group mindfulness practice. The mindfulness training with these modifications was found to be of validity in previous studies (Xu et al., 2016; Yuan et al., 2015).
In a word, mindfulness training in the current study is based on a nonjudgmental way of paying attention to the present moment, mostly including silent retreat or intensive experience, such as body scan, sitting meditation, walking meditation, yoga, and group discussions. In group discussions, participants chose one practice by themselves, then they were encouraged to share practice feelings, discuss the training topics, and solve puzzles in practice. The group sessions were held once a week and lasted 2.5 to 3 hr each time. After each group session, participants were assigned 30 to 45 min group mindfulness practice. The whole process was guided by a psychological counselor who had training experience with mindfulness practices for at least 3 years.
This study was approved by the ethics committee of School of Psychology, Nanjing Normal University.
Measures
The FFMQ (Xu, Liu, & Liu, 2015) was accessed to measure mindfulness. We applied the 39-item Chinese version of the original instrument developed by Baer, Smith, Hopkins, Krietemeyer, and Toney (2006). It includes five subscales: (a) observing (e.g., “When I take a shower or bath, I stay alert to the sensations of water on my body”), (b) describing (e.g., “I can easily put my beliefs, opinions, and expectations into words”), (c) acting with awareness (e.g., “When I do things, my mind wanders off and I’m easily distracted”), (d) nonjudging of inner experience (e.g., “I tell myself I shouldn’t be feeling the way I’m feeling”), and (e) nonreactivity to inner experience (e.g., “When I have distressing thoughts or images, I just notice them and let them go”). Items are rated on a 5-point Likert-type scale ranging from 1 (never or very rarely true) to 5 (very often or always true). Higher scores indicate a higher trait mindfulness level. In this study, Cronbach’s alphas of the five subscales ranged from .57 to .81 (Observing, α = .79; Describing, α = .75; Acting with awareness, α = .81; Nonjudging of inner peace, α = .74; and Nonreactivity to inner peace, α = .57.). Cronbach’s alpha coefficient of nonreactivity to inner experience was below .60 and it was consistent with the study conducted by Wu, Shi, Xia, Lu, and Du (2013).
The SCL-90 (Xin, Zhang, & He, 2012) consists of 90 items. The primary symptom dimensions include nine subscales which assess somatization, obsessive-compulsive disorder, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation, and psychoticism. Bulten, Nijman, and van der Staak (2009) suggested that self-report scales such as the SCL-90 may be helpful in screening detainees for important Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV; American Psychiatric Association, 1994) disorders. In the current study, Cronbach’s alpha coefficient was .99. For the nine subscales, Cronbach’s alpha ranged from .84 to .94, which showed a sufficient internal reliability.
The Zung SAS (Zung, 1971) was used to measure anxiety levels. The SAS is a 20-item self-rating scale rated on a 4-point scale, ranging from 1 (none) to 4 (always). The Chinese version of the SAS was translated by Tao and Gao (1994). Higher scores represent more severe symptoms. In the current study, Cronbach’s alpha was .89.
The Zung SDS (Zung, 1965) was used to measure depression. The SDS is a 20-item scale rated on a 4-point scale, ranging from 1 (a little bit of time) to 4 (most of the time). The Chinese version of the SDS was translated by X. Liu et al. (1994). In the current study, Cronbach’s alpha was .85.
The PSQI (H. Q. Wang, Chai, Xu, Wang, & Zhao, 2017) is a self-report questionnaire that assesses sleep quality over a period of 1 month. It was specifically designed for clinical populations (Buysse, Reynolds, Monk, Berman, & Kupfer, 1989). The PSQI consists of 19 self-rated items and five other-evaluated items that are scored on a scale, ranging from 0 (not during the past month) to 3 (three or more times a week). Barring the score of the 19th item, and five other-evaluated items, the whole scale was grouped into seven components that yield one global score. The global score excluded the score of habitual sleep efficiency due to the strict sleep time. Higher scores represent lower sleep quality. Cronbach’s alpha was .84.
The AQ (Buss & Perry, 1992) is a 29-item questionnaire where participants rank certain statements from 0 (none) to 5 (always). The revised Chinese version AQ has good reliability and validity in the study of male prisoners’ aggression (L. Li, Xi, Niu, Wen, & Du, 2010). Cronbach’s alpha of the total scale was .94. For the four subscales, Cronbach’s alpha ranged from .69 to .89.
The POMS (Albrecht & Ewing, 1989) is a 65-item measure of present mood state. Items are rated on a 5-point Likert-type scale ranging from 0 (not at all) to 4 (extremely). It consists of six affective dimensions, namely, tension-anxiety, depression-dejection, anger-hostility, vigor-activity, fatigue-inertia, and confusion-bewilderment. A total mood disturbance score was calculated by adding the five negative subscales (i.e., tension-anxiety, depression-dejection, anger-hostility, fatigue-inertia, and confusion-bewilderment; Xu et al., 2016). The Chinese version is a valid instrument for the assessment of emotion (J. Wang, Lin, Chen, Cui, & Liu, 2000). In the present study, Cronbach’s alpha of total mood disturbance was .96. For the six subscales, Cronbach’s alpha ranged from .57 to .95. Vigor-activity and confusion-bewilderment were the subscales whose Cronbach’s alphas were below .70.
The CPSS (Yang & Huang, 2003) was developed from the original version designed by Cohen, Kamarck, and Mermelstein (1983), which measures the degree to which situations in one’s life are appraised as stressful. Psychological stress has been defined as the extent to which persons perceive that their demands exceed their ability to cope. A 5-point Likert-type rating scale from 1 (never) to 5 (very often) is used to answer each question. Items 4, 5, 6, 7, 9, 10, and 13 are the positively stated items, which are reverse-scored. Thus, higher scores indicate higher perceived stress. Cronbach’s alpha was .74.
Data Analyses
Using SPSS 16.0, we tested whether the mindfulness intervention led to improvements in entire mental health, anxiety, depression, aggression, sleep quality, total mood disturbance, and perceived stress.
Pearson correlations were calculated to examine the association between FFMQ and other scales at pretest. Moreover, the independent-sample t test of changes in dependent variables was to examine whether the mindfulness training group had a significant improvement on scores of FFMQ and a significant reduction on scores of all inventories compared with the waitlist control group.
To examine whether sentence length moderates the effect of intervention between the mindfulness training group and the waitlist control group, hierarchical regression (Baron & Kenny, 1986) was applied by using SPSS 16.0. Compared with the short-term prisoners, the long-term prisoners were significantly older (t = 8.31, p < .001); thus, we set age as a control variable in the regression model. Finally, we controlled the pretest score and the prisoners’ age in the regression model and set group as independent variable, and sentence length as moderator, to predict the posttest score of each dependent variable. The continuous control variables and moderator were z standardized to minimize multicollinearity with the interaction terms in the model. Simple slopes were computed to further determine the moderator effect.
Results
First, we conducted Pearson correlations to examine the association between the dependent variables at pretest (see Table 1). Results demonstrated that the FFMQ total score was significantly negatively correlated with all inventories except vigor-activity. Vigor-activity is a subscale of the POMS. Higher score indicates that the responder is more energetic and it had a significant positive correlation with the FFMQ total score. Among the subscales of FFMQ, acting with awareness was negatively correlated with all inventories except vigor-activity. Meanwhile, describing negatively correlates with the scores of SCL-90, SDS, AQ, and PSS. Pretest and posttest scores of the mindfulness training group and the waitlist control group in dependent variables are shown in Table 2.
Correlations Among Dependent Variables (n = 83).
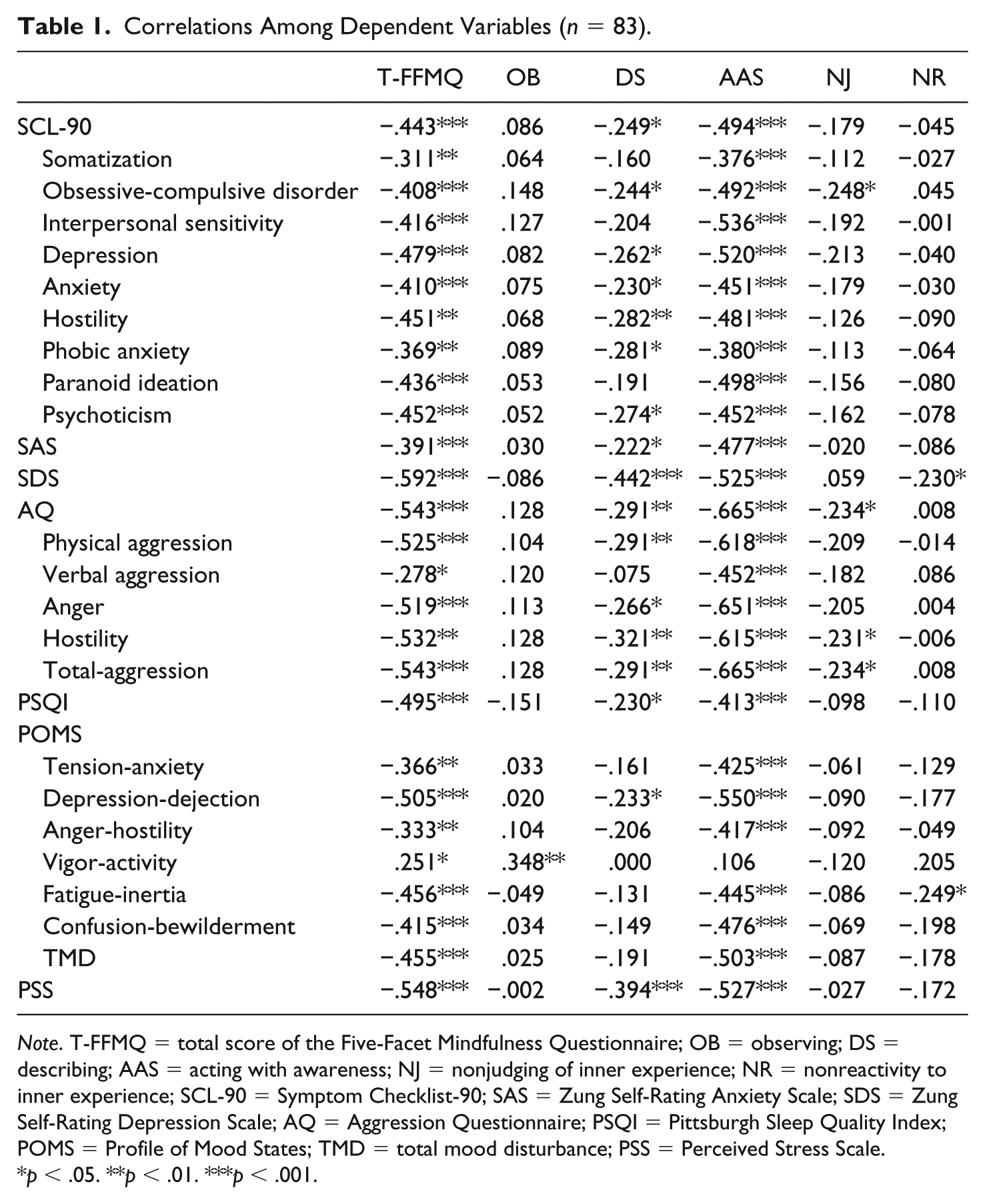
Note. T-FFMQ = total score of the Five-Facet Mindfulness Questionnaire; OB = observing; DS = describing; AAS = acting with awareness; NJ = nonjudging of inner experience; NR = nonreactivity to inner experience; SCL-90 = Symptom Checklist-90; SAS = Zung Self-Rating Anxiety Scale; SDS = Zung Self-Rating Depression Scale; AQ = Aggression Questionnaire; PSQI = Pittsburgh Sleep Quality Index; POMS = Profile of Mood States; TMD = total mood disturbance; PSS = Perceived Stress Scale.
p < .05. **p < .01. ***p < .001.
Pretest and Posttest of Mindfulness Training Group and the Waitlist Control Group in Dependent Variables.
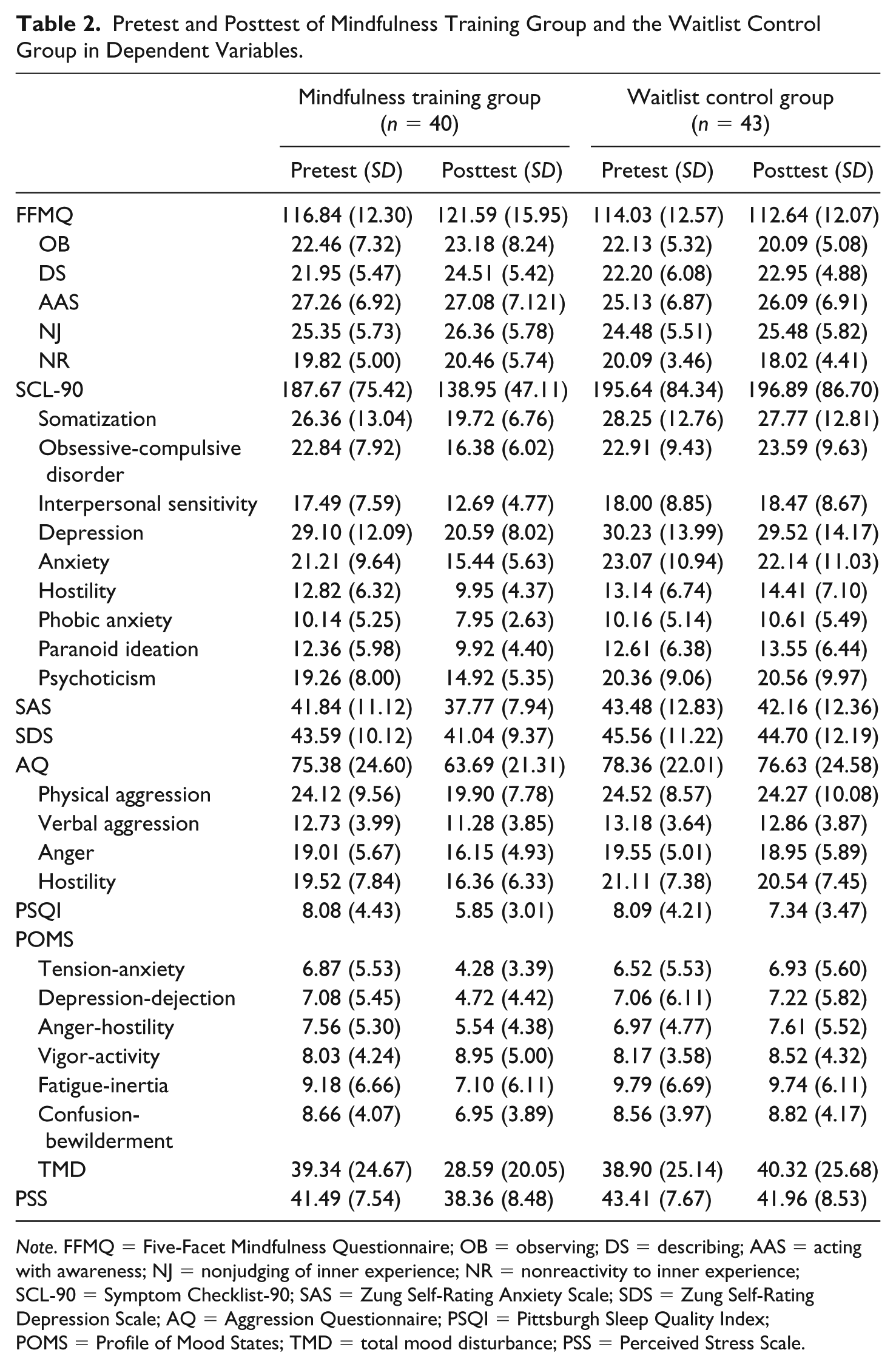
Note. FFMQ = Five-Facet Mindfulness Questionnaire; OB = observing; DS = describing; AAS = acting with awareness; NJ = nonjudging of inner experience; NR = nonreactivity to inner experience; SCL-90 = Symptom Checklist-90; SAS = Zung Self-Rating Anxiety Scale; SDS = Zung Self-Rating Depression Scale; AQ = Aggression Questionnaire; PSQI = Pittsburgh Sleep Quality Index; POMS = Profile of Mood States; TMD = total mood disturbance; PSS = Perceived Stress Scale.
Independent-sample t test (see Table 3) of changes in dependent variables was significant with the scores of FFMQ, SCL-90, AQ, PSQI, and total mood disturbance (TMD). Results suggested that compared with the waitlist control group, the mindfulness training group got a significant enhancement in FFMQ scores and a significant reduction in SCL-90, AQ, PSQI, and TMD scores.
Independent-Sample t Test of Changes in Dependent Variables.
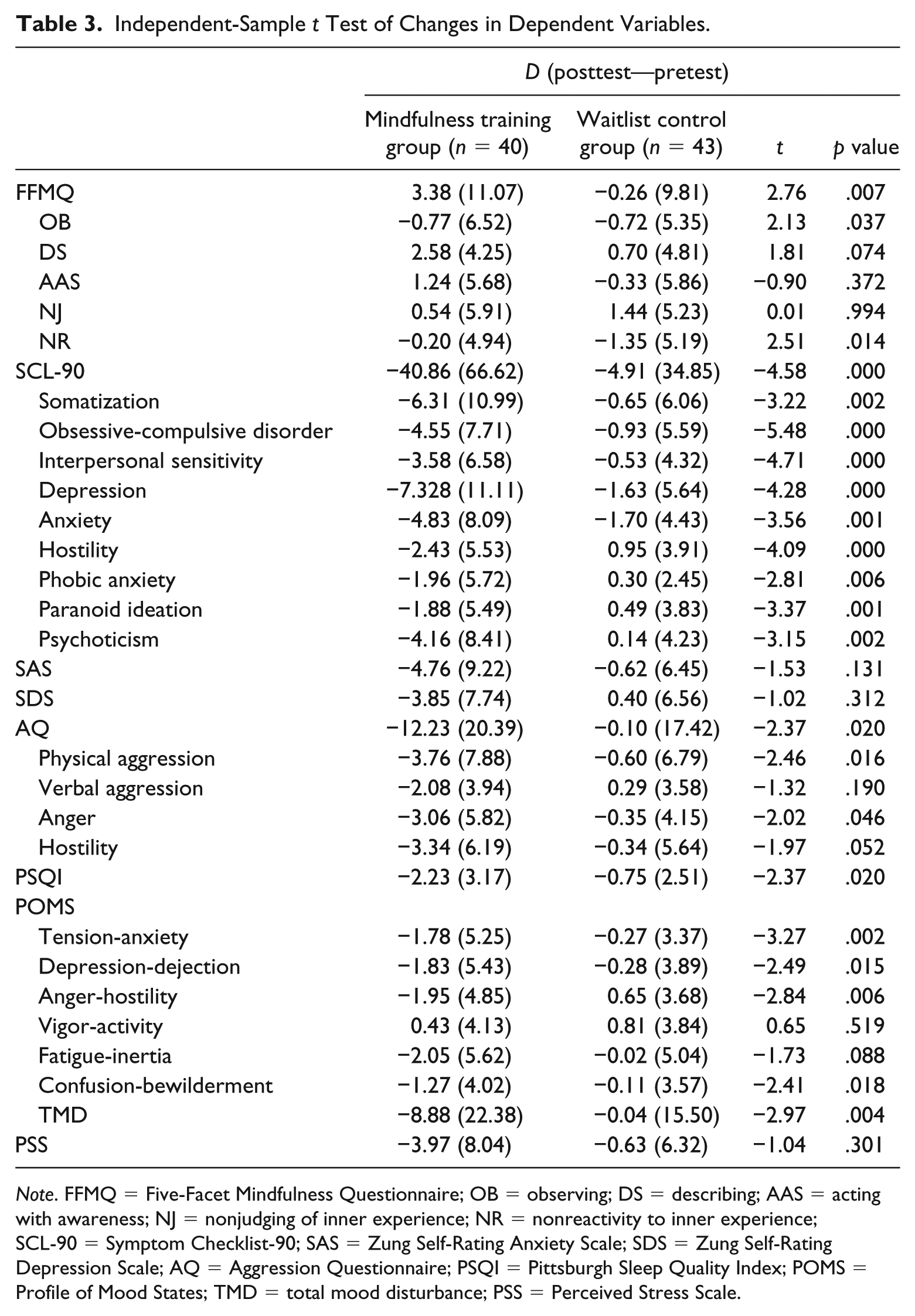
Note. FFMQ = Five-Facet Mindfulness Questionnaire; OB = observing; DS = describing; AAS = acting with awareness; NJ = nonjudging of inner experience; NR = nonreactivity to inner experience; SCL-90 = Symptom Checklist-90; SAS = Zung Self-Rating Anxiety Scale; SDS = Zung Self-Rating Depression Scale; AQ = Aggression Questionnaire; PSQI = Pittsburgh Sleep Quality Index; POMS = Profile of Mood States; TMD = total mood disturbance; PSS = Perceived Stress Scale.
To further declare the intervention effects, we also plot the results of the pretest and posttest score in the mindfulness training group and the waitlist control group of long- and short-term prisoners, respectively, in Tables 4 and 5. Results indicated that, in long-term prisoners who were assigned to the training group, significant improvement was observed in every measured variable, whereas the short-term prisoners only improved in aggression.
Pre- and Posttest Scores of Dependent Variables of Mindfulness Training and Waitlist Control Groups in Long-Term Prisoners.
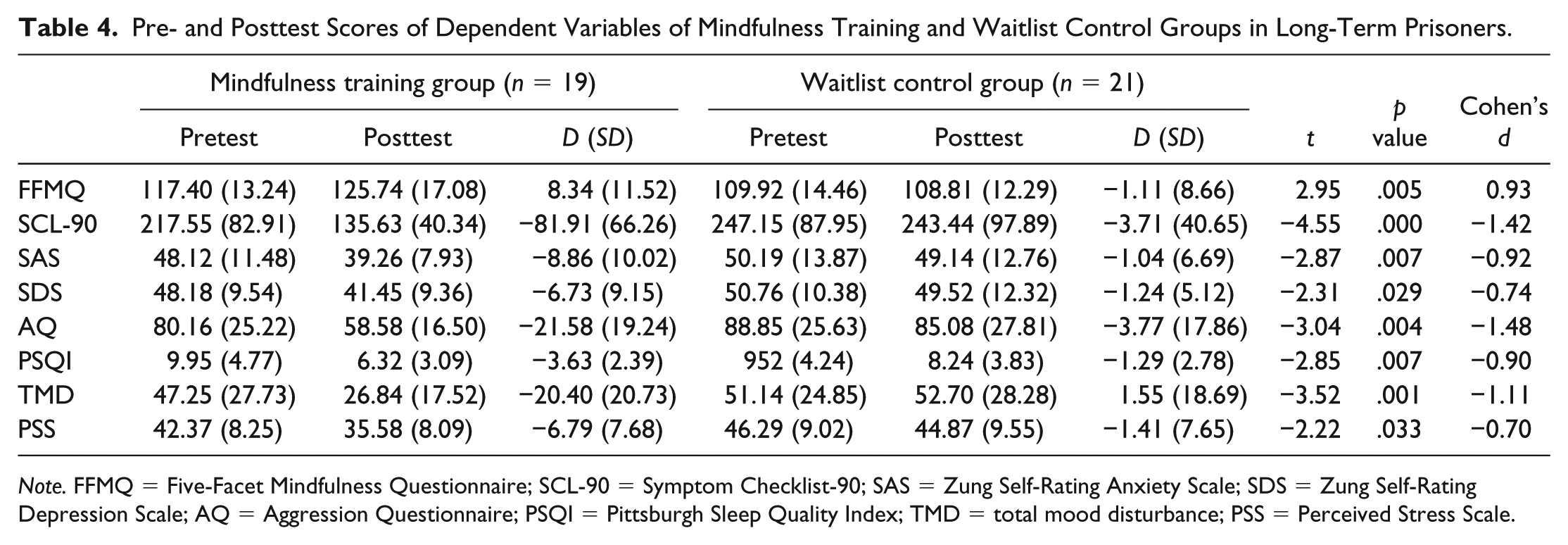
Note. FFMQ = Five-Facet Mindfulness Questionnaire; SCL-90 = Symptom Checklist-90; SAS = Zung Self-Rating Anxiety Scale; SDS = Zung Self-Rating Depression Scale; AQ = Aggression Questionnaire; PSQI = Pittsburgh Sleep Quality Index; TMD = total mood disturbance; PSS = Perceived Stress Scale.
Pre- and Posttest Scores of Dependent Variables of Mindfulness Training and Waitlist Control Groups in Short-Term Prisoners.

Note. FFMQ = Five-Facet Mindfulness Questionnaire; SCL-90 = Symptom Checklist-90; SAS = Zung Self-Rating Anxiety Scale; SDS = Zung Self-Rating Depression Scale; AQ = Aggression Questionnaire; PSQI = Pittsburgh Sleep Quality Index; TMD = total mood disturbance; PSS = Perceived Stress Scale.
In hierarchical regression, we examined the Group × Prison term and found a significant moderate effect on FFMQ (R2 = .56, ΔR2 = .02, β = .25, p = .048), SCL-90 (R2 = .72, ΔR2 = .05, β = −.37, p < .001), SAS (R2 = .62, ΔR2 = .05, β = −.38, p = .002), SDS (R2 = .63, ΔR2 = .02, β = −.24, p = .034), AQ (R2 = .51, ΔR2 = .03, β = −.31, p = .022), TMD (R2 = .55, ΔR2 = .06, β = −.39, p = .002), and PSS (R2 = .43, ΔR2 = .07, β = −.44, p = .003), as shown in Table 6, indicating that mindfulness training intervention will be more beneficial for the long-term prisoners.
Analyses of Moderating Effect of Prison in the Relationships Between Study Groups and Dependent Variables.
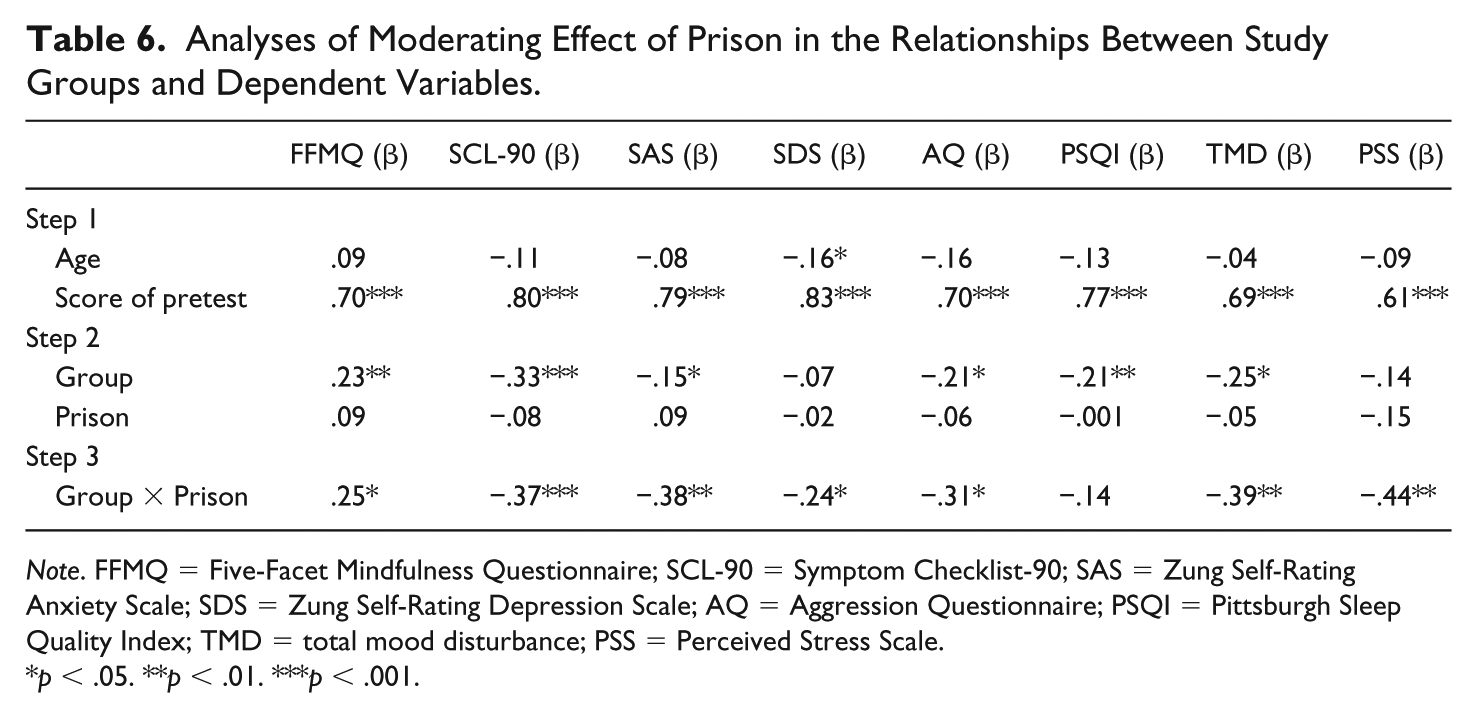
Note. FFMQ = Five-Facet Mindfulness Questionnaire; SCL-90 = Symptom Checklist-90; SAS = Zung Self-Rating Anxiety Scale; SDS = Zung Self-Rating Depression Scale; AQ = Aggression Questionnaire; PSQI = Pittsburgh Sleep Quality Index; TMD = total mood disturbance; PSS = Perceived Stress Scale.
p < .05. **p < .01. ***p < .001.
Considering the significant moderate effect, we tested simple slopes of these dependent variables to examine the differences between participants with a long versus short prison term. The slope was significant for long-term participants, but not for those in short sentence (see Table 7). Thus, the mindfulness training intervention was significantly and negatively associated with mental disorders, anxiety, depression, aggression, total mood disturbance, and perceived stress among long-term prisoners, whereas it was not significant among short-term prisoners.
Simple Slopes of Interaction Effect: Group × Prison.
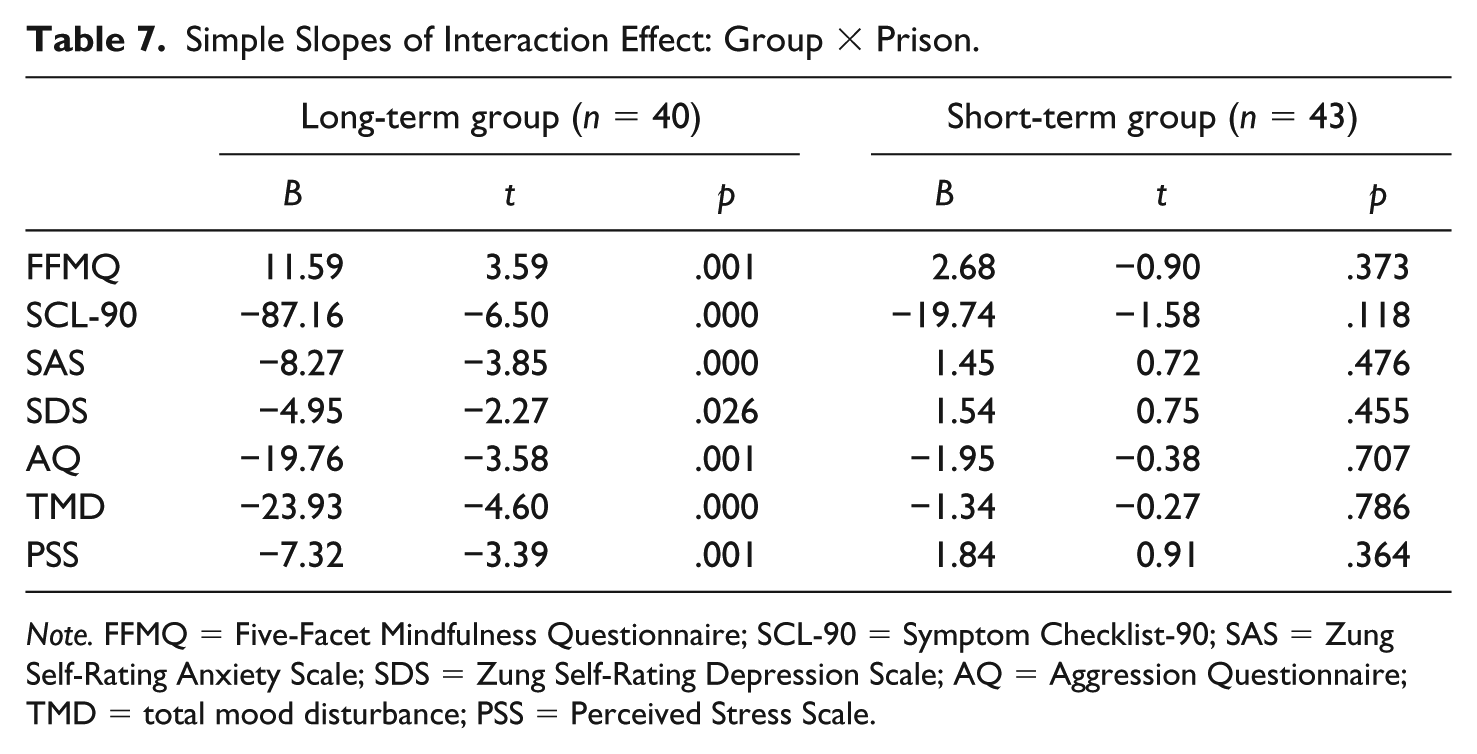
Note. FFMQ = Five-Facet Mindfulness Questionnaire; SCL-90 = Symptom Checklist-90; SAS = Zung Self-Rating Anxiety Scale; SDS = Zung Self-Rating Depression Scale; AQ = Aggression Questionnaire; TMD = total mood disturbance; PSS = Perceived Stress Scale.
Discussion
This study explored the effectiveness of mindfulness training among Chinese male prisoners and made comparisons between long-term and short-term prisoners. Although the present 6-week mindfulness training is a simplified version, it derives from the MBCT, which has been found to be effective in enhancing mindfulness levels and improving mental health (Samuelson et al., 2016) in Western settings. We observed significant negative correlations between mindfulness levels and the scores in SCL-90, AQ, and POMS among male prisoners. Moreover, we found that self-rating anxiety and depression, as well as perceived stress, had obvious negative correlations with the levels of mindfulness among male prisoners, whereas sleep quality was positively correlated with mindfulness. These findings are in line with prior studies in which mindfulness was negatively correlated with negative emotions (Hofmann, Sawyer, Witt, & Oh, 2010; Khoury et al., 2013), psychopathology (Kocovski, Segal, & Battista, 2009), and perceived stress (Baer, Carmody, & Hunsinger, 2012) in other populations. Previous studies also revealed that sleeping quality can be improved by mindfulness-based training (Ong, Ulmer, & Manber, 2012; Winbush, Gross, & Kreitzer, 2007) and it is also in accordance with our results.
We found that the total score of the FFMQ exhibited a significant improvement after participants completed the intervention, and it means that mindfulness-based training enhanced the mindfulness levels of all the prisoners. According to the results of the FFMQ, the factors of Observation and Nonreactivity to Inner Experience increased significantly in the mindfulness training group and this is in line with the study implemented by Yuan et al. (2015). It is confirmed that during the mindfulness training period, the prisoners were trained to keep a clear mind and simple perspective to the outer environment and their own feelings (Singh, Wahler, Adkins, & Myers, 2003). This is the process of being aware and paying attention to the present moment in a nonjudgmental way (Figueiredo, Abreu, & Freitas, 2016) instead of arousing indignation and overreaction. The literature also showed that increasing mindful nonreactivity may be of importance in achieving successful treatment for severe health anxiety (Hedman, Hesser, Andersson, Axelsson, & Ljótsson, 2017).
The results of the t test indicated that all the factors in SCL-90, as well as the total score, decreased significantly after the mindfulness-based intervention. It is worth mentioning that the improvement of depression and obsessive-compulsive disorder is particularly significant, which corroborates the prior findings of the mindfulness-based treatment for depression and obsessive-compulsive disorder (Hale, Strauss, & Taylor, 2013; Wilkinson-Tough, Bocci, Thorne, & Herlihy, 2010). The results also indicated that mindfulness-based intervention helped to decrease aggression and mood disturbance, which in turn enhanced the sleeping quality. Former studies had already reached the conclusion that hostility and bad mood may reduce the quantity and quality of sleep (Ireland & Culpin, 2006). The results of the present study further confirmed this conclusion.
The results of moderating effects are consistent with our hypothesis that the effects of intervention are considerably superior among long-term prisoners than short-term prisoners, and that the moderating effect is supported by all the scales used in this study. For those long-term prisoners, mindfulness-based interventions exert a significant improvement on their mental health (i.e., depression, anxiety, and aggression). For those short-term prisoners, however, no significant relationship between mindfulness-based intervention and improvements on mental health emerged. Possible interpretations may lie in that long- and short-term prisoners differ in engagement. The literature showed that the infraction rates of long-term inmates were significantly lower than the rates for short-term prisoners, even in the early years of confinement (Flanagan, 1980). The long-term prisoners tend to be more disciplined than the short-term prisoners, and they are more likely to have better participation in mindfulness-based training. In the next place, long- and short-term prisoners differ in acceptability of mindfulness-based training. Compared with short-term prisoners, long-term prisoners experience more struggle in adapting to imprisonment and thus suffer from more severe pressure, anxiety, and even cognitive impairment (Lapornik et al., 1996). Therefore, they are more likely to believe in mindfulness training and have a stronger desire to change the current situation. Finally, the intervention was carried out with the participation of the administrators, and the long-term prisoners tended to behave better to lessen the penalty.
Findings from the current study have theoretical and practical significance in clinical practice. First, the results deepened the knowledge of how mindfulness-based training enhances the emotional health and reduces the negative consequences of mental illness. Second, the results supported the improvement model that prisoners can benefit from mindfulness-based interventions. Third, mindfulness-based interventions, such as MBSR, are encouraged routinely among prisoners to enhance their levels of mindfulness.
This study has several limitations in design and results. First, the sample in the current study was not randomized due to scheduling issues of prisoners controlled by the Chinese prison system, and the setting of the control group cannot eliminate the potential impact of Hawthorne effect. Another limitation is that all the measurements in the current study were self-report questionnaires. Neurobiological methods are encouraged in future research. Third, the moderating variable in the present study had only two levels, and further studies need to divide the length of imprisonment into more detailed levels. Fourth, owing to the fact that the posttest was given immediately after the intervention, there might be experimenter effect during the intervention process, which directly affected prisoners’ responses. Finally, this study lacks longitudinal data, and future studies need take the effects of time into consideration and figure out whether the effectiveness of mindfulness intervention lasts for a certain period.
In this study, the results are consistent with the hypothesis of this study. Mindfulness-based training did enhance the level of mindfulness and the emotional health of the prisoners. Meanwhile, mindfulness-based interventions function better in long-term prisoners than in short-term prisoners.
Footnotes
Authors’ Note
Yuanyuan An contributed to the conduct of the study and wrote the article mainly. Qi Huang assisted in writing the article, Yucheng Zhou performed the data analysis, Yuyang Zhou designed the scheme and led the groups, and Wei Xu was in charge of the whole study. Wei Xu is also affiliated with Beijing Normal University, China.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Natural Science Foundation of the Higher Education Institution of Jiangsu Province, China (Project No. BK20171036), by Top-notch Academic Programs Project of Jiangsu Higher Education Institutions (Project No. PPZY2015B118), and by China Postdoctoral Science Foundation (Project No. 2017M610333).