
Abstract
A logistic regression model for 289 cases of schizophrenic offenders in a Swiss forensic hospital between 1995 and 2016 revealed the following factors for above average levels of antipsychotic overdosing and polypharmacy: Odds for overdosing increased in absence of a personality disorder (237%), for each point increase in emotional withdrawal (63.5%) and motor retardation (71.7%), and decreased for poor rapport (42.3%) recorded at admission. Odds for polypharmacy increased with complaints about physicians (157%), for each point increase in IQ (3.6%; range = 65–131, M = 92, SD = 14), reduction of the security level of the ward (36.8%; four levels), and for each point increase in poor attention (27.6%) at admission. It decreased with each previous conviction (10.9%; range = 1–21, M = 3, SD = 2), breaking of rules (46.4%) and the administration of compulsory measures (55.7%) on the ward, a poor legal prognosis (29.4%, four levels), and each point increase in grandiosity (40.3%), passive social withdrawal (42.3%), and depressive symptoms (38.7%) at admission.
Keywords
Introduction
Treatment of schizophrenia with several antipsychotics at once (polypharmacy) and/or off-label dosing of antipsychotics is considered “non-evidence-based” and is not recommended in the literature except if at least two antipsychotic monotherapies (one of which should be an atypical antipsychotic) and clozapine in the recommended blood plasma concentration have failed to provide sufficient reduction of symptoms (Morrissette & Stahl, 2014; Stahl et al., 2013, 2014). Administering antipsychotics above recommended maximum dosages and may be necessary in cases of pharmacokinetic (e.g., rapid metabolization or poor absorption) or pharmacodynamic (e.g., D2 receptor hypo- or hypersensitivity in certain brain areas) failure (Morrissette & Stahl, 2014) or for treatment of acute violence (Royal College of Psychiatrists, 2014). Similarly, antipsychotic polypharmacy may be useful for rapid tranquilization in treating acute agitation, when switching between antipsychotics (Royal College of Psychiatrists, 2014; Taylor et al., 2018), or to augment clozapine to increase efficacy (Taylor & Smith, 2009; Zink et al., 2010). Yet, both practices are generally associated with the more likely occurrence of extrapyramidal symptoms (EPS) (Parkinsonism, akathisia, acute dystonias, tardive dyskinesia) even in some atypical antipsychotics, increased side effects other than EPS (ranging from sedation, postural hypotension, hyperprolactinaemia, osteoporosis, obesity, hypertension, seizures and cognitive decline to neuroleptic malignant syndrome), a rise in interactions between medication, heightened mortality due to metabolic and cardio vascular disease (including diabetes, coronary heart disease and QTc-prolongation with the risk of sudden death), and the confusion of sedative effects with antipsychotic effects leading to poor compliance of most patients in the long-run (Correll et al., 2007; Elie et al., 2010; Joukamaa et al., 2006; National Institute for Health and Clinical Excellance, 2014; Royal College of Psychiatrists, 2014). Disregarding recommendations, patients with schizophrenia, especially in forensic settings, are frequently treated with polypharmacy (30%–65% in general psychiatry, Morrissette & Stahl, 2014), and dosages above the recommended maximum in treatment guidelines (overdosing, up to 20% in general psychiatry, Harrington et al., 2002) for prolonged periods of time, leading researchers to suspect factors other than treatment resistant psychopathology (due to pharmacokinetic or pharmacodynamic failure, which would allow for higher doses or polypharmacy) may drive psychiatrists’ prescribing practices (Barbui et al., 2006; Barnes & Paton, 2011; Connolly & Taylor, 2014; Margetić et al., 2017; Morrissette & Stahl, 2014; Stahl et al., 2014; Stone-Brown et al., 2016).
For this reason, we hypothesize as follows:
Previous research showed in a group of 1,198 patients with all types of diagnoses on acute psychiatric wards of eight (nonforensic) mental health trusts that higher body weight, a higher number of previous admissions, longer hospitalizations, noncompliance with medication, and the prescription of atypical antipsychotics (except clozapine) were associated with higher dosing of antipsychotics (Connolly & Taylor, 2014). In the same study, Connolly and Taylor found having a higher total dose, a forensic history, or a greater number of previous psychiatric admissions to be predictors for polypharmacy (Connolly & Taylor, 2014). They conferred that chronic illness may promote antipsychotic polypharmacy and overdosing. By contradiction, Stone-Brown and colleagues found a lower prevalence of polypharmacy in 189 U.K. forensic patients in comparison with psychiatric patients in other settings (Stone-Brown et al., 2016). Research focusing on the subgroup of patients with a schizophreniform disorder provided similarly mixed findings on the effect of suicidal ideation and perceived risk of suicide on antipsychotic prescribing (Hettige et al., 2014; Kasckow et al., 2011; Taiminen & Kujari, 1994). We suspect all contradictory findings may be due to the heterogenicity of the studied samples. Further narrowing down the investigated subgroup of patients to schizophrenic offenders in forensic settings, researchers speculated the severity of the crime committed and aggressive behaviour before or during the forensic hospitalization may guide forensic psychiatrists in their prescribing of doses and combinations of antipsychotics—which they may believe to prevent further aggression, instead of being guided by current psychopathological symptoms (Margetić et al., 2017).
Above literature informed the formulation of the following hypothesis for this study:
More specifically, patient behaviour inducing fear of aggression in prescribers may involve the type and number of crime(s) committed or troublesome behaviour on the ward ranging from lack of remorse or sexual deviance, over complaints, breaking of rules, to outright endangerment of other individuals. The security level of the ward, use of compulsory measures, or future legal prognosis may be factors reducing fear in psychiatrists and thus their prescribing of high doses and polypharmacy.
In summary, the aims of this study are threefold: to examine the previously unpublished occurrence of antipsychotic overdosing and polypharmacy in schizophrenic offenders in a Swiss forensic hospital, to (for the first time, to our knowledge) report on whether or not such prescribing practices will change over the course of forensic treatment, and to explore contradictory findings and speculations of previous research on factors possibly leading prescribers towards antipsychotic overdosing and polypharmacy.
Method
Source of Data
The study presented here is part of a larger study, approved by the Zurich Cantonal Ethics Committee. The centre for inpatient forensic therapies at the Zurich University Hospital of Psychiatry is an institution for the treatment of convicts with a mental disorder who are either admitted for the treatment of acute syndromes or were sent to treatment to reduce the risk of reoffending due to illness. Treatment records from patients admitted from 1995 to 2016 were examined to identify 289 treatment cases of patients with a diagnosis of schizophrenia. Their medical records included psychiatric–psychological reports, prosecutions, police reports, court testimonies and proceedings, medical and nursing documentation, as well as reports on previous stays in psychiatric institutions. Legal standards governing the required accuracy of these case files from their first compilation to the end of a forensic treatment are high in Switzerland. Directed qualitative content analysis (Hsieh & Shannon, 2005) was conducted to derive information from these case files including the domains of sociodemographic data, childhood/youth, psychiatric treatment history, criminal history, social and sexual functioning, the offence leading to forensic hospitalization (index offence), prison data, medical treatment throughout current hospitalization, and PANSS-data at admission prior to any antipsychotic treatment in the forensic psychiatric facility. PANSS-data refer to information captured by the Positive and Negative Symptom Scale (Kay et al., 1987) and was measured in three manifestations: symptom is substantially, discretely, or not present. A trained independent rater adhering to a rating protocol conducted initial content analysis of the 289 case files. A second trained independent rater coded a subsample of 10% of the cases chosen at random to provide inter-rater reliability. Cohen’s Kappa value (Brennan & Hays, 1992) was 0.78 which can be regarded as substantial for inter-rater reliability (Lambert & Bergin, 1993). Based on extant literature reviewed above (Margetić et al., 2017), the effects of 53 variables from the domains mentioned (see Supplemental Materials for a detailed listing) on antipsychotic treatment (presence of polypharmacy, dosing) were analysed using R Studio version 1.1.383.
Data Processing
What constitutes antipsychotic overdosing? Recommendations on dosing of antipsychotics in guidelines often rest on estimates of manufacturers approved by regulatory bodies or expert opinion, but not on randomized head-to-head comparisons of antipsychotics at several fixed doses and across diagnostic, illness severity, comorbidity, and demographic variables (Gardner et al., 2010). To make comparability between dosing worse, chlorpromazine (CPZ) equivalence calculations are often inconsistent and show up to threefold variation in CPZ-equivalent values (Rey et al., 1989; Rijcken et al., 2003; Woods, 2003). We defined any cumulative antipsychotic dosage prescribed upon admission, after half of the total hospitalization, or upon release which, converted into olanzapine equivalents, was above 25.72 mg olanzapine as higher than the recommended maximum. For conversion of cumulative antipsychotic dosage into olanzapine equivalents, we relied on conversion factors provided through the classical weighted mean dose method published by Leucht et al. (2015) whenever possible and resorted to the minimum effective dose method also published by Leucht et al. (2014) and finally international experts’ consensus based olanzapine equivalents reported by Gardner et al. (2010) whenever olanzapine equivalents could not be found in our primary source for conversion factors. Long-acting injectable antipsychotics (LAIs) were administered to five patients (1.7%) at admission, to eight patients (2.7%) after half of total inpatient treatment, and to 16 patients (5.5%) upon discharge (in seven cases in combination with an oral antipsychotic) and were converted into daily doses by dividing the administered antipsychotic dose by the number of days of the interval in which the LAI was administered, to then be converted into olanzapine equivalents. Our rationale for setting the cutoff point for overdosing at 25.72 mg, the equivalent of 1,000 mg of chlorpromazine by above conversion method, was informed by Margetić et al. (2017). Other research work on antipsychotic dosing set the cutoff point for a “usual dose range” (Morrissette & Stahl, 2014) or “target dose range” (Gardner et al., 2010) even lower at 20 mg olanzapine. We defined polypharmacy as the concurrent administration of more than one antipsychotic.
A different approach to define antipsychotic overdosing could have relied on the defined daily dose (DDD), which the World Health Organization (WHO) defines for most medication as the assumed average maintenance daily dose for a drug, used for its main indication in adults (Nosè & Barbui, 2008). However, Leucht and colleagues recommend against the use of the DDD in research on dosing equivalents, if “alternative, more ‘scientific’ dose equivalence methods are available for a drug,” because the information the WHO uses to estimate DDDs differs between drugs, is not publicly available to be critically reviewed, and the WHO itself states that DDDs as a measure of dose equivalence can be misleading (Leucht et al., 2016). Similarly, methods of dosage comparison such as the maximum effective dose method (Kong et al., 2014) or percentages of the British National Formulary (BNF) maximum (Sweileh et al., 2014) may involve similar limitations pertaining to transparency and consistency (between drugs and researchers) in their estimation.
Data Analysis
Logistic regression with forward and backward stepwise inclusion and 10-fold cross-validation was employed (Yamashita et al., 2007) to determine the most informative predictors for antipsychotic overdosing and polypharmacy among the 53 items. Both antipsychotic overdosing and polypharmacy were dichotomous variables, where 1 represented “present” and 0 represented “absent.” For 10-fold cross-validation (Arlot & Celisse, 2010; Kohavi, 1995), the entire data set was split into 10 subsets. Subsequently nine out of 10 subsets were assigned to form the training set, and the remaining subset was assigned to from the test set. This procedure was repeated 10 times, so that each subset was used as test set once. Logistic regression was then performed by fitting a generalized linear model (GLM) with binomial distribution to each of the 10 training subsets. Forward and backward stepwise inclusion was based on the Akaike information criterion (AIC), which permits to select the most parsimonious model fit. The accuracy, sensitivity, and specificity of each of the 10 model fits were evaluated by predicting the probabilities of the corresponding test subsets. Here, probabilities of >.5 were categorized into 1, probabilities below were categorized into 0. The average agreement between predicted and actual observations was taken as a measure of accuracy of the model fit. The final logistic regression model was computed by taking the average of the coefficients and standard errors resulting from the 10 model fits. Items that had a p-value < .05 and a standard error smaller than the mean coefficient were considered the most informative predictor items. Confounding parameters are not significant, however lead to a pronounced change in at least one of the coefficients of a significant parameter and are therefore left in the final model. The AIC-based selection accounts for such confounding items, resulting in an effective critical p-value of .157 for inclusion (Heinze et al., 2018).
Results
H1: Antipsychotic Polypharmacy and Overdosing Will Be High and Decrease Only Somewhat Over Forensic Inpatient Treatment
There is evidence in support for Hypothesis 1: 85.8% and 21.5% of patients received antipsychotic polypharmacy or cumulative dosages above the recommended maximum, respectively, upon admission to forensic inpatient treatment. The number of patients with polypharmacy decreased by 16.9% from admission to transfer/release from the forensic wards, while the number of cases with antipsychotic overdosing increased by 7.6% (see Table 1).
Descriptive Statistics on Antipsychotic Polypharmacy and Cumulative Dosing Above Recommended Maximum Dosages.
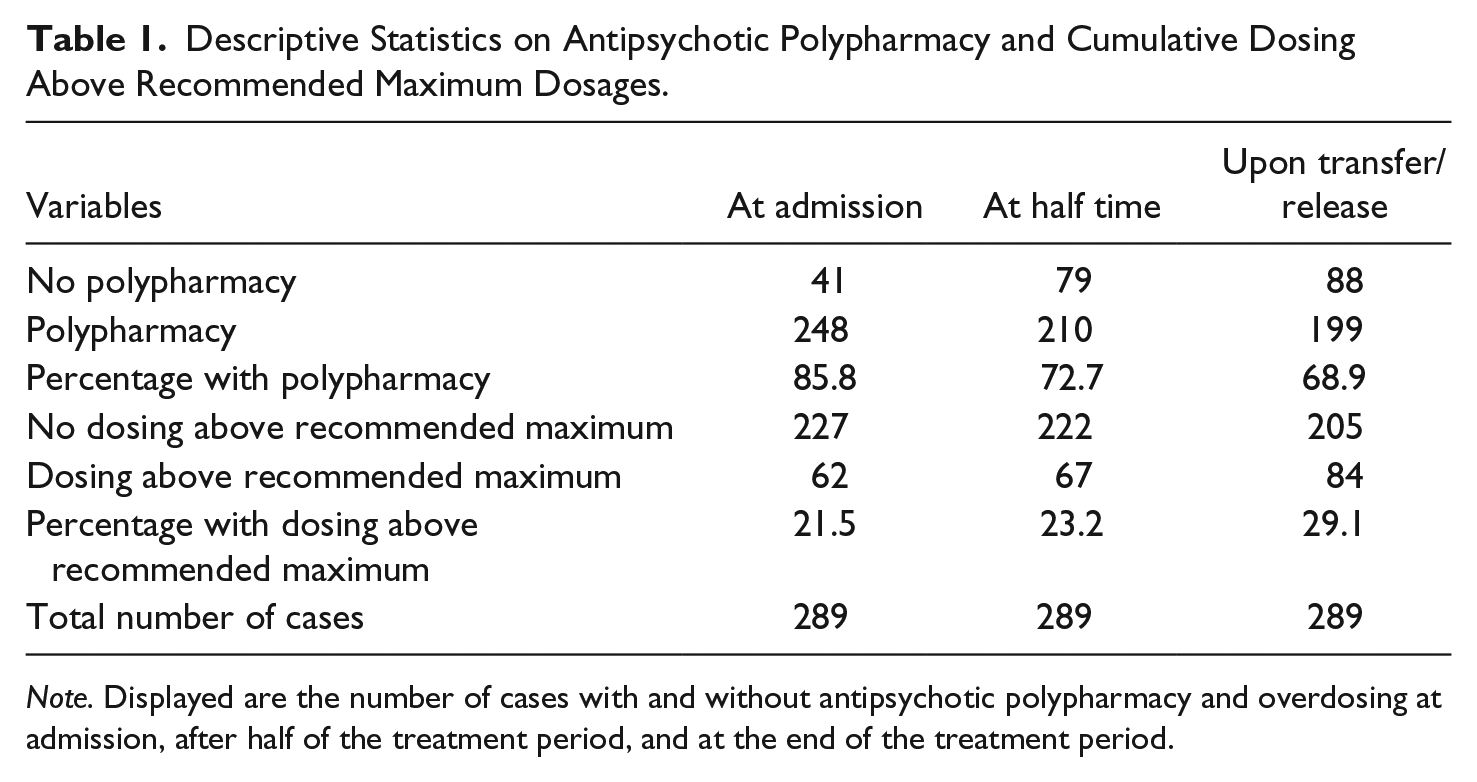
Note. Displayed are the number of cases with and without antipsychotic polypharmacy and overdosing at admission, after half of the treatment period, and at the end of the treatment period.
Excluding patients who were (also) medicated with clozapine at discharge from the sample studied here, because in these cases, polypharmacy may have been in accord with guidelines recommending clozapine augmentation with another atypical antipsychotic to increase its efficacy (Taylor & Smith, 2009; Zink et al., 2010), polypharmacy was still present in 46.7% of all cases.
H2: At Least In Part, Factors Other Than (Treatment Resistant) Psychopathology Will Explain the Occurrence of Antipsychotic Overdosing and Polypharmacy
Results of the logistic regression for antipsychotic overdosing are summarized in Table 2: Odds for antipsychotic overdosing increased by 237% if no personality disorder was diagnosed in addition to the schizophreniform disorder. Each point increase on the three-step scales on emotional withdrawal and motor retardation at admission increased odds for antipsychotic overdosing by 63.5% and 71.7%, respectively. Likelihood for antipsychotic overdosing was reduced by 42.3% for each reduction on the three-step scale on poor rapport at admission.
Coefficients Resulting of the Logistic Regression for Antipsychotic Overdosing.
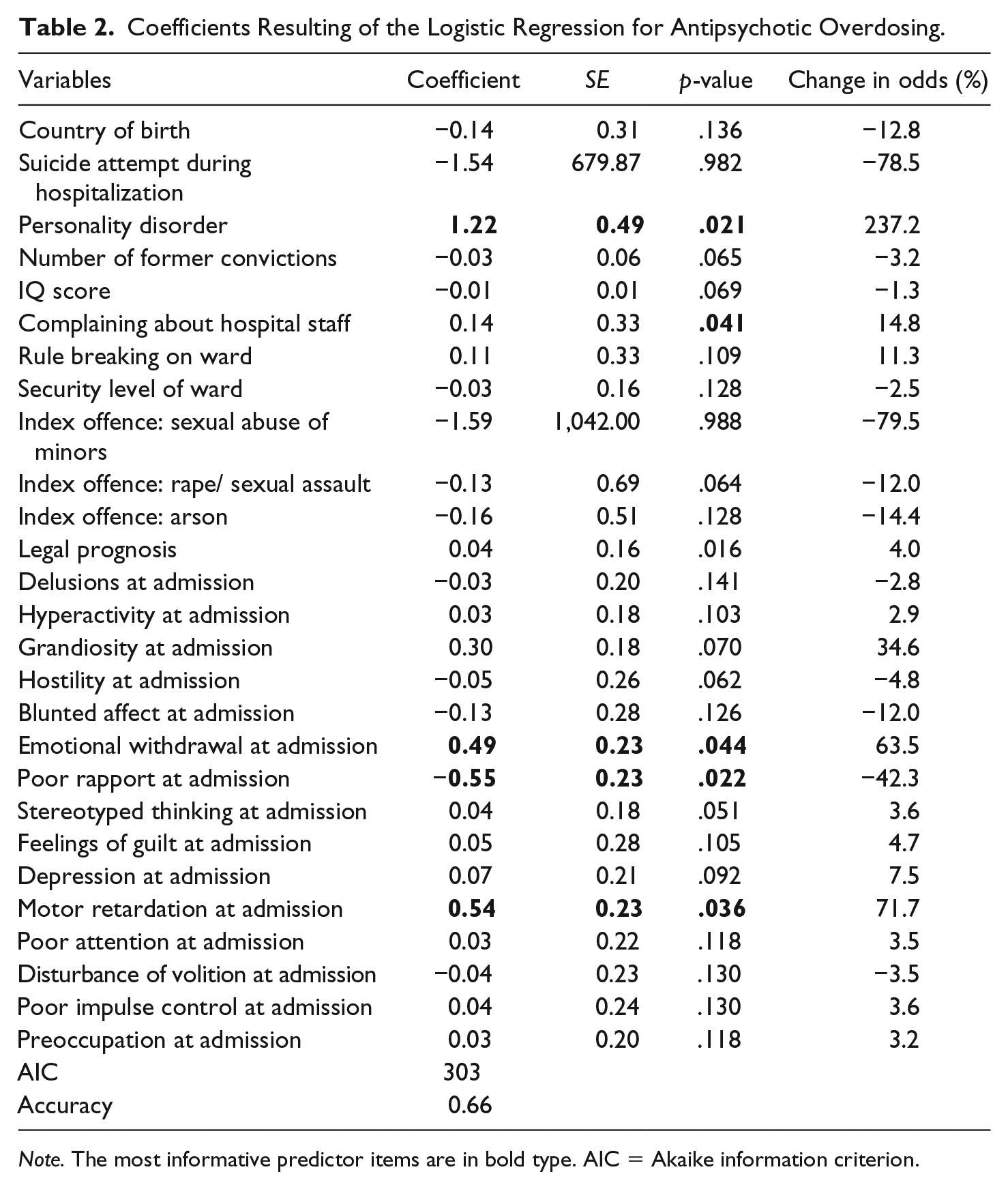
Note. The most informative predictor items are in bold type. AIC = Akaike information criterion.
Results for polypharmacy are summarized in Table 3: Odds for polypharmacy increased by 157% when delinquents complained about the physicians in charge, by 3.6% for each point increase in IQ (range = 65–131, M = 92, SD = 14), by 36.8% for each reduction in the security level of the ward (four levels), and 27.6% for each point increase in the three step scale for poor attention at admission. The number of former convictions to imprisonment (range = 1–21, M = 3, SD = 2), breaking of rules on the ward, the administration of compulsory measures on the ward, and a poor legal prognosis (4 levels) reduced odds for polypharmacy by 10.9%, 46.4%, 55.7%, and 29.4%, respectively. Similarly, when patients displayed grandiosity, passive social withdrawal, or depressive symptoms, this reduced the likelihood for polypharmacy, by 40.3%, 42.3%, and 38.7%, respectively.
Coefficients Resulting of the Logistic Regression for Polypharmacy.

Note. The most informative predictor items are in bold type. AIC = Akaike information criterion.
Overall there is some support for Hypothesis 2. Although psychopathology seems to significantly impact odds for overdosing and polypharmacy, there are other variables also playing an important role. Antipsychotic polypharmacy seems to be more influenced by nonpsychopathology-related factors than overdosing. However, items having no significant effect on non-evidence-based antipsychotic treatment were: country of birth, all remaining 24 psychopathology-related items adopted from the PANSS upon admission to the forensic setting, recordings of being suicidal before (174 patients) or during (51 patients) the forensic detainment, attempted suicide during forensic hospitalization (seven patients), the total number of criminal offences, geographical origin from within or outside the European union, presence of sexually deviant behaviour, extent to which a patient complained about staff (other than physicians) on the ward, the number of years since a psychiatric diagnosis was first reported, the number of years since the first criminal offence, the type of index offence leading to forensic treatment (homicide, sexual abuse of children, other sexual assault or rape, arson), endangerment of other individuals during forensic hospitalization, and amount of insight to the ethical falseness of the crime committed.
H3: Behaviour Generating Fear of Aggression in Prescribers, Chronicity of Schizophrenia, and Suicidal Ideation or Attempted Suicide at Any Point in Time Will Be Positively Correlated With Antipsychotic Overdosing and/or Polypharmacy
Some mildly aggressive behaviour, such as complaining about physicians in charge, distinctly increased the likelihood for polypharmacy. Yet, other behaviour, which may also be expected to be perceived as threatening (such as breaking of rules on the ward) or factors expected to generate fear (such as a high number of former imprisonments or a poor legal prognosis), surprisingly even reduced the odds for polypharmacy. Similarly, the type of index offence and sexually deviant behaviour did not significantly affect dosing or polypharmacy. However, in line with H3, the administration of compulsory measures on the ward and a high level of security reduced odds for polypharmacy.
Duration of illness is operationalized by the number of years having passed since first diagnosis of a psychiatric disease, and suicidal ideation before or during forensic hospitalization did not affect odds for overdosing or polypharmacy. Overall, thus, we can only find moderate evidence in support of H3: Some patient-related factors potentially inducing fear of aggression in psychiatrists responsible for their treatment may have some impact on overdosing and polypharmacy, but not always in the direction hypothesized and not as clear-cut as suggested in previous research (Margetić et al., 2017).
Discussion
Main Findings in Light of Prior Literature
The prevalence of antipsychotic polypharmacy and cumulative dosing above recommended maximum dosages in the present sample of offender patients with schizophrenia being admitted to forensic psychiatric inpatient treatment was similarly high or slightly higher than the upper limits reported for other psychiatric inpatient treatment settings (Harrington et al., 2002; Morrissette & Stahl, 2014). These results confirm prior findings indicating particularly high rates of polypharmacy and overdosing in forensic psychiatric settings (Barnes et al., 2009; Connolly & Taylor, 2014; Lelliott et al., 2002). The decrease in antipsychotic polypharmacy by 16.9% over the course of inpatient treatment and the overall low prevalence of combinations of oral and depot antipsychotics upon discharge (2.4%) may be signs for prescribers’ efforts to reduce non-evidence-based prescribing (Barnes et al., 2009; Barnes & Paton, 2011; Mace & Taylor, 2015). The increase in antipsychotic overdosing over inpatient treatment is unexpected. As a limitation of this study, it did not interview prescribers on their rationales. Prior research mentions covert nonadherence of patients (Connolly & Taylor, 2014), which is unlikely in the strict forensic setting explored here, and prescribers perceived lack of efficacy (Grech & Taylor, 2012; Haw & Stubbs, 2003) as common reasons for non-evidence-based antipsychotic treatment. The latter explanation seems to find support in results evidencing an increase in odds for high dosing in the presence of increased negative symptoms of emotional withdrawal and motor retardation at admission while other explaining factors such as poor rapport or a personality disorder decreased odds for high dosing (see results). However, as another limitation of this study, motor retardation and emotional withdrawal may be both, the result of benzodiazepines (or other grossly sedating medication) administered previous to admission (in prison), or negative symptoms of schizophrenia (Carpenter et al., 1985; Singh et al., 2010)—both triggers for psychiatrists to adjust medication after admission to the forensic ward.
Explaining the high rates of antipsychotic polypharmacy throughout treatment seems more difficult. Results seem to paint a picture of the smart patient, paying poor attention upon admission to a less secure ward, to then complain more than average about the physicians in charge to be most likely to receive polypharmacy. By contrast, patients displaying grandiosity, passive social withdrawal, and depressive symptoms upon admission, while having a high number of previous convictions and a poor legal prognosis, who continue to constantly break rules on the ward and experience compulsory measures, are least likely to be prescribed several antipsychotics at once. These results seem to lend support to the hypothesis that factors other than psychopathology are affecting the occurrence of polypharmacy, as was hypothesized in prior research (Barbui et al., 2006; Barnes & Paton, 2011; Connolly & Taylor, 2014; Margetić et al., 2017; Morrissette & Stahl, 2014; Stahl et al., 2014; Stone-Brown et al., 2016).
However, there appears to be only moderate support for Margetić and colleagues’ (Margetić et al., 2017) speculation on psychiatrists’ non-evidence-based prescribing being guided by their (unconscious) desire to achieve a “patient must remain unaggressive” state, because aggressive patient behaviour during or prior to inpatient treatment, including constant rule breaking on the ward, necessity for compulsory measures, numerous prior convictions and a poor legal prognosis, did not increase (or even decreased) odds for antipsychotic polypharmacy and overdosing. Possibly, it is not so much fear psychiatrists experience towards schizophrenic offenders, but their fear to fail in treating them adequately (on a less secure ward). Such fear may be particularly reinforced by intelligent patients complaining about psychiatrists while presenting with what seem to be more severe negative symptoms, known to be particularly difficult to treat (Roffman et al., 2013; Turkington & Morrison, 2012).
Inconsistencies in prior research concerning the role of suicidal ideation and attempted suicide were also addressed in that there was no evidence on these factors affecting odds on high dosing or polypharmacy at statistical significance, thus supporting previous research with larger sample sizes (Hettige et al., 2014; Kasckow et al., 2011; Margetić et al., 2017). Research suggesting that the chronicity of schizophrenia will positively affect likelihoods for overdosing and polypharmacy (Connolly & Taylor, 2014) was not confirmed. This may be due to chronicity being operationalized with the number of years having passed since the first psychiatric diagnosis in this study and the number and length of previous psychiatric admissions in a prior study, but not other parameters (Connolly & Taylor, 2014).
Further Limitations
What are further limitations of this study? Similar as in prior research on the topic (Connolly & Taylor, 2014), models generated in standard stepwise logistic regression are often too complex, contain redundant information (Van der Borght et al., 2011), and inflated p-values. Besides this study’s exploratory rather than formal modelling focus, these problems were addressed using, instead of p-values, an information criterion (AIC) for stepwise model selection and combined the stepwise selection with 10-fold cross-validation allowing for improved validity and robustness of the selected model (see Tables 2 and 3).
Future studies with an independent test population should also address limitations linked to selection effects due to a relevant part of mentally ill offenders in Switzerland not being able to be admitted to forensic hospitals due to the relative scarcity of such facilities, which may have affected representativeness of the sample studied here. Future research should include data from schizophrenic delinquents in prison. Another limitation is that despite forensic files being extensive, some traits of delinquents we assumed to be absent in the sample, may in fact have been missing because professionals authoring the case files failed to recorded them. However, this effect can be considered small given the high professional merit required to be met by law in the composition of the case files analysed here.
Conclusion
Addressing past inconsistencies in findings, the prevalence for antipsychotic polypharmacy and overdosing was at least as high in the offender patients with schizophrenia studied here as in samples of nonoffender patients in general psychiatry in prior research. As a novel contribution to the field, new factors were identified to increase odds for polypharmacy (complaints about physicians in charge, higher IQ, the security level of the ward, poor attention) and cumulative dosing above recommended maximum (absence of a personality disorder, emotional withdrawal, poor rapport) upon admission to forensic inpatient treatment. Propositions of prior research that suicidal ideation, attempted suicide, psychiatrists’ fear of aggressive behaviour of patients, or the chronicity of schizophrenia may be related to antipsychotic polypharmacy and high dosing were not confirmed, but discussed in light of alternative explanations for past and present findings.
Supplemental Material
Supplementary_materials – Supplemental material for Antipsychotic Overdosing and Polypharmacy in Schizophrenic Delinquents Explored
Supplemental material, Supplementary_materials for Antipsychotic Overdosing and Polypharmacy in Schizophrenic Delinquents Explored by M. P. Günther, J. Kirchebner, S. Kling and S. Lau in International Journal of Offender Therapy and Comparative Criminology
Footnotes
Compliance with Ethical Standards
The study was reviewed and approved by the Cantonal Ethics committee of Zurich, Switzerland (Ref. No. KEK-ZH-NR 2014-0480). All procedures were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This is a retrospective study. For this type of study, formal consent is not required. This article does not contain any studies with animals performed by any of the authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.