
Abstract
UK veterans with complex needs arrested in police custody can access support through pre-charge diversion into treatment and ancillary services. We consider why veterans in police custody disengaged from a peer-led criminal justice diversionary support service in one UK region that adopted a continuous case management approach. Seven hundred and fifty-seven veterans were assessed to have high levels of comorbid health needs and socio-economic harms, with one-quarter (26.7%, n = 202) subsequently disengaging from the service. A logistic regression model using Multivariate Imputation by Chained Equations identified that veterans of a younger age, no-fixed-abode, a history of incarceration, and those from a Royal Navy background were likelier to disengage from the intervention. We conclude that this peer-based diversionary model has some efficacy in maintaining the engagement of a highly complex, comorbid segment of criminally-justice-exposed UK military veterans. The perceived benefits of an integrated peer-based model predicated on continuous case-management techniques are discussed.
Introduction
The conceptualization of initiatives within the criminal justice system to provide diversionary services encompassing “diversion from” incarceration and further sanctions or penalties or “diversion to” specialist services for treatment to address criminogenic needs (Lange et al., 2011; Maume et al., 2018; Richardson & McSherry, 2010) has formed an essential component of crime reduction approaches. For these services, there have been two separate but interconnected timelines focusing on substance use disorders (SUD) from the 1970s in the United States on the Treatment Alternatives (or Accountability) to Street Crime (or Safer Communities), also known as the TASC model. TASC models for offenders with SUDs were examples of diversion to specialist addiction services based on continuous case-managed referral techniques (Clark et al., 2013; Cook, 1992; Inciardi et al., 1992). Secondly, the development of criminal justice diversionary services for offenders with mental health disorders has been characterized by the similar deployment of case-management techniques with the aim of “jail diversion” away from more punitive sanctions that do not address the underlying pathology (Steadman et al., 1994). For SUD and mental health models, there is some evidence of effectiveness in reducing criminal behavior through engagement with treatment (Kane et al., 2018; Maume et al., 2018; Sirotich, 2009). “Next generation” models have been designed to address the holistic person- and place-level factors associated with vulnerable offenders, considering SUD and mental health needs as co-occurring factors rather than single pathologies (Epperson et al., 2014; Wolff et al., 2013).
The point of contact for offenders within any diversionary program includes stages at pre-arrest before charge, pre-trial (post-charge but referred to treatment before a court appearance), pre- or post-sentence, and pre-release from custody (Lange et al., 2011; Spooner, 2001). The need to view these points as an integrated whole has been made (Lange et al., 2011), and the conceptual Sequential Intercept Model establishes the opportunity to intervene at pivotal intercept points pre-arrest in the community [Intercept 0], law enforcement responses to an incident (e.g., responding to a public call) [Intercept 1], initial detention or initial court hearings [Intercept 2], imprisonment including treatment courts for high need individuals [Intercept 3], reentry from imprisonment back to the community [Intercept 4], and Intercept 5 focuses on community corrections (Munetz & Griffin, 2006).
Veterans have been deemed a vulnerable population susceptible to various specific health morbidities and poor outcomes, requiring an urgent and detailed focus throughout the criminal justice system (Finlay et al., 2019). For ex-military personnel (hereafter defined as “veterans”) known to the criminal justice system, the predominant types of offending tend to be related to violence or sex offences (Baktir et al., 2020; Stacer & Solinas-Saunders, 2020; White et al., 2012). Veteran morbidities are linked to poor mental health, including post-traumatic stress and traumatic brain injuries (Blonigen et al., 2016; Jones, 2022), SUD (Black et al., 2005; Blodgett et al., 2015; Erickson et al., 2008; Wainwright et al., 2017) including an emphasis among UK veterans for problematic alcohol consumption. Other issues included financial problems involving gambling (Harris et al., 2023; Roberts et al., 2020), housing, and relationships (MacManus et al., 2013, 2021; Short et al., 2018). Moreover, Murray (2015) suggests that veterans have specific needs compared to other offending populations, including chronic health issues (Hall et al., 2022), given the risks and vulnerabilities associated with their military roles. The identity of a veteran at the various intercepts is termed “veteranality,” describing the distinctive characteristics of a veteran (Murray, 2015).
Peer support models are effective for criminal justice populations (Bagnall et al., 2015) and for veterans addressing mental health issues, including trauma (Jain et al., 2016; Hundt et al., 2015; Jain et al., 2012), accessing broader health services and support for chronic healthcare management (Arney et al., 2020; Peeples et al., 2020). The use of peers (members of the armed forces community, including ex-service personnel and service family members) as caseworkers is a critical component of the continuous case management approach, enabling veterans to have confidence in a community with whom they have a shared identity with unique characteristics, promoting veteran interaction with dedicated support in a trusted space. However, the development of veteran services, including peer-based models, has proved challenging due to problems with information sharing and broader issues operationalizing diversion activities (Kim et al., 2019; Christy et al., 2012).
Intervention Details
This study is based on a peer-based intervention within one region of the UK. The service intervenes at pre-arrest before charge (Spooner, 2001) within Intercept Level 2 (Munetz & Griffin, 2006) and initially operate within police custody (Fossey et al., 2017). Peer workers were volunteers from an Armed Forces (or police) background who had retired from active service. Managers were paid members of staff who oversaw caseloads on a geographical (regional) basis. Training was provided by the service that included the main areas of need (e.g., mental health and awareness of SUD), and training was also provided to ascertain an understanding of local referral pathways. Peer workers tended to be retired and were considered more experienced and confident in their dealings with ancillary agencies, which was beneficial for onward engagement. The model offers continuous peer-based support across three phases, from initial, informal engagement within police custody settings to an initial screening process, and completion of a full assessment. There are no criteria for completing contact with the service; the individual veteran and key worker decide when to cease contact. Many interactions are informal, often providing updates on progress and emotional well-being. Assessments of need do not focus solely on mental health or SUD but instead offer a holistic support service. All offenders in police custody are routinely asked during the booking-in interview whether they have ever served in HM Forces. The extent to which veterans comply with this question is unknown, and more work is required to assess whether any veteran segment is less likely to engage at this point in the process. An affirmative response to this question results in an automatic referral to the service, which confirms the person’s veteran status, then assesses the individual for any immediate risk and engages the person to understand broader needs often undertaken in a conducive environment away from police custody. The caseworkers then provide a range of interventions, signposting referrals to ancillary services (such as healthcare services) and provision of advice/information at the point of arrest before engaging fully with the service. Once individuals have engaged and have formally been accepted onto the caseload, workers will develop an individualized plan that involves brokerage access to other services problem-solving, emotional support and advocacy (e.g., assisting with legal issues; see Figure 1).
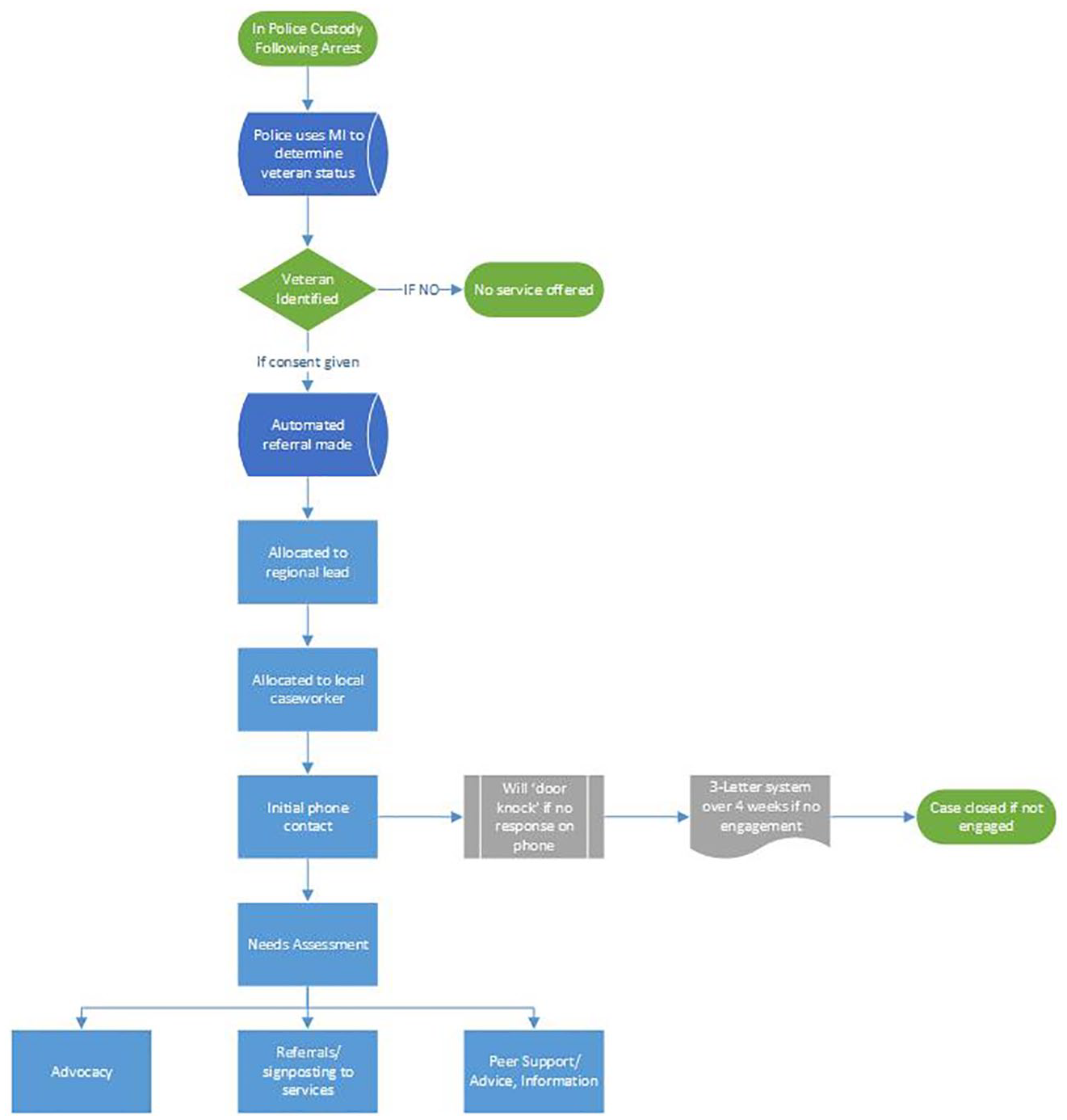
Process summary.
This study assesses the factors associated with why veterans disengage with this peer-based model after completing a full baseline assessment. It is suggested that this group of veterans may be of specific interest by providing empirical evidence of the factors associated with non-engagement for individuals who agreed to be taken onto the caseload. These individuals had committed to being part of the initiative at the point of arrest; therefore, following initial acceptance onto the caseload, individuals who chose to disengage are of considerable interest as the reasons for their withdrawal may help clarify the nature of enhancements needed for a needs-led diversionary service for veterans.
Methods
The analysis involved interrogation of an administrative dataset held on veterans at each stage of the process, including initial engagement, immediate assessment of risks and completion of a full assessment. We applied a battery of validated screening tests to veterans at the point of assessment incorporating over 34 measures, including age, gender, ethnicity, housing need, employment status, previous prison history, military background (army, navy, and Royal Air Force), and whether the veteran had been registered with a community doctor. In addition, there were questions on substance misuse and any specific needs classified into alcohol consumption; anger management; community needs, domestic abuse, drugs, employment, housing, legal; mental health; relationships, and welfare needs (such as claiming benefits), categorized as binary measures. The prognostics also included screens for Post-Traumatic Stress Disorder (PTSD) symptoms, the Short Warwick-Edinburgh Mental Well-Being Scale (SWEMWBS) to measure the prevalence of mental health issues using 7-items on a 5-point Likert scale with higher scores indicating greater levels of well-being; Work and Social Adjustment Scale (WSAS) that measures experienced difficulties on day-to-day activities due to challenges experienced across work, home management, social leisure activities, private leisure activities, family, and relationships. The WSAS is a 5-item scale on a 9-point scale with higher scores indicating increased problem severity. The Alcohol Use Disorder Identification Test (AUDIT-10) screened for problematic alcohol consumption over ten items on a 5-point Likert scale, with higher scores indicating greater severity of problematic alcohol use with scores of 20 or more suggestive of alcohol dependence.
The extent of missing information ranged from less than 5% for ethnicity (n = 0) and previous exposure to prison (n = 0) and for age (n = 11), 4% (n = 27) for sex to 44% (n = 326) for the part of the assessment that focused on the range of identified needs. To avoid dropping any records, we applied a Multivariate Imputation by Chained Equations or MICE (Azur et al., 2011) method, which simulates missing values multiple times to impute values. Recent research has suggested unbiased results are not affected by levels of missing data (Madley-Dowd et al., 2019), with levels of up to 50% missing data that can be considered viable for imputation (Heymans & Twisk, 2022). The database comprised 757 cases allocated to peer caseworkers, and the population description is provided in Tables 1 and 2. Twenty-six veterans who had been allocated a caseworker and initially assessed did not complete the needs assessment process. These cases were deleted from this dataset as no additional information could be used to support the enhanced model. The final dataset consisted of 730 cases and 34 prognostics. In total, there were 27 incomplete risk factors, of which one was continuous (Age), three ordinals (WSAS, AUDIT, and SWEMWBS), and one multinomial (employment status); the remaining 22 variables were binary. Four different imputation models were used for imputing the 27 prognostics with missing values: a logistic model for missing binary prognostics (22), a linear model for missing age, an ordinal model for missing ordinal prognostics (3), and a multinomial model for missing employment status.
Summary of Clients (Assessed), n = 757 Allocated to a Caseworker.
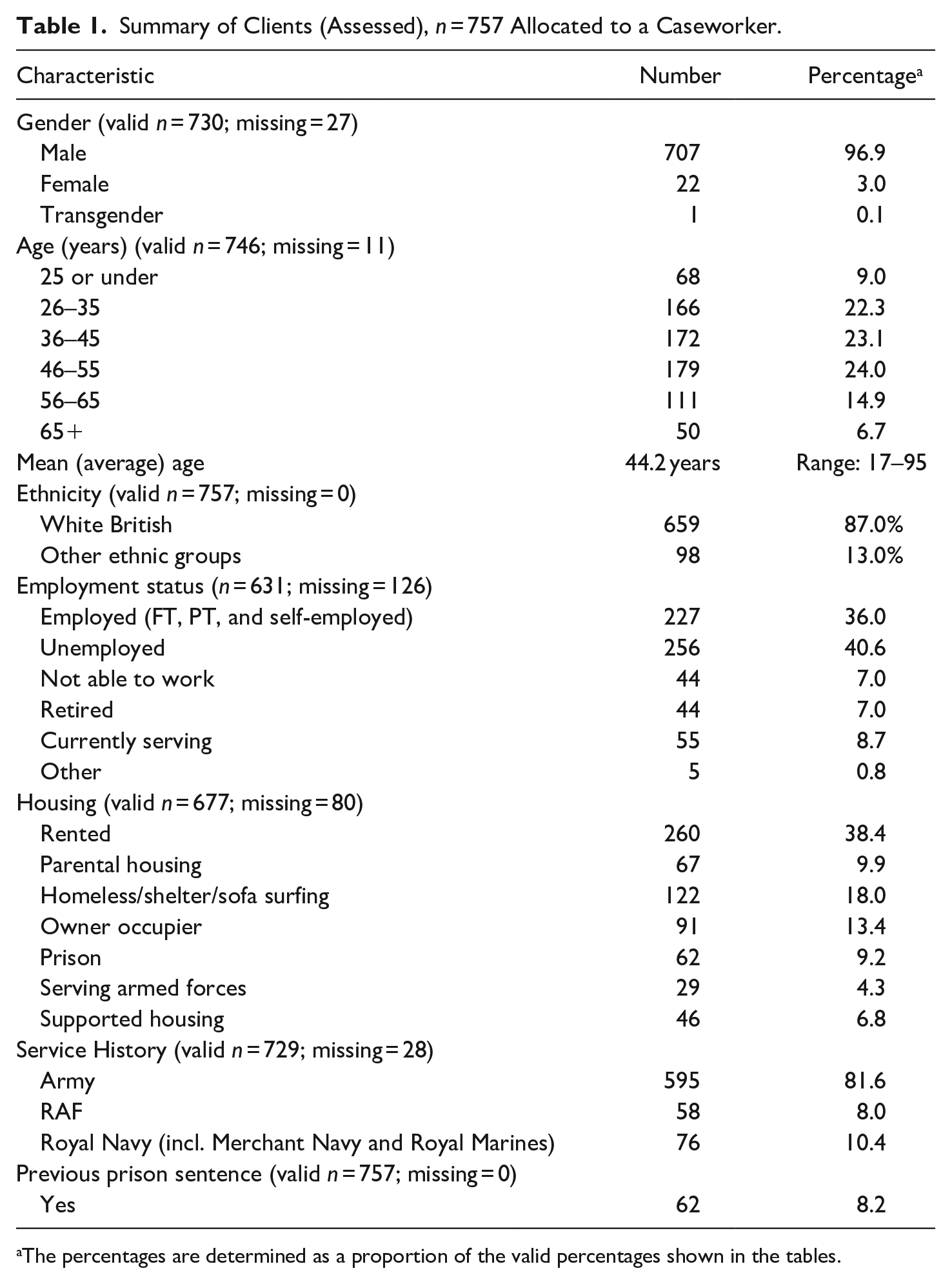
The percentages are determined as a proportion of the valid percentages shown in the tables.
Summary of Clients (Assessed), n = 757 Allocated to a Caseworker.

The percentages are determined as a proportion of the valid percentages shown in the tables.
Based on the correlations across all variables, the missing data mechanism was plausibly assumed to be Missing at Random (Van Buuren, 2011). The appropriateness of the multiple imputations was evaluated informally using diagnostic plots (Eddings & Marchenko, 2012), which showed no apparent departures from the empirical distribution of the non-missing data records. The “mim” imputation method described by Royston et al. (2009) was used to conduct a stepwise backward selection of prognostics on the imputed dataset. All analyses were undertaken in Stata release 16 (StataCorp, 2019).
Findings
For the three- and half-year period (2018-end of June 2021), there were 1,716 individual referrals made to the service, 757 of whom (44.1%) were allocated to a caseworker. Of 926 individuals not assigned a caseworker, 42.0% (n = 398) were “no contact” or “unable to make contact” once the initial referral had been made. A further 40.3% (n = 373) were reported as an “inappropriate referral,” a referral deemed not to require an intervention. About 14.6% disengaged either by declining the support (8.4%, n = 78), did not engage after first contact (1.5%, n = 14), or did not engage at all (4.6%, n = 43). Only a small number (n = 15) of those who did not engage were recorded to have been remanded in prison, reflecting that the intervention was situated pre-trial (Lange et al., 2011; Spooner, 2001).
The vast majority of veterans formally assessed by the service were male (96.8%, n = 706) and white (91.7%, n = 651), with a mean age of 44.2 years across a wide range of clients (between 17 and 95 years). Over one-third of the caseload was reported as unemployed, either full or part-time or self-employed (37.1%, n = 250), with 40% reported as unemployed (n = 250). Veterans were also reported as living in rented accommodation (38.4%, n = 260), and the majority reported having an Army background (81.6%, n = 595).
The needs of veterans were determined in a sub-assessment of 431 cases. In two-thirds of cases where an assessment was made, the veteran’s immediate need identified was mental health (66.1%, n = 285), followed by housing (32.5%, n = 140), financial needs (25.1%, n = 108), alcohol problems (23.9%, n = 103), welfare (23.7%, n = 102), and employment issues (23.0%, n = 99). In total, 1,728 referrals were made for all those assessed, averaging four referrals per person compared to a national estimate of 0.83 per person (Disley et al., 2021). The Work and Social Adjustment Scale (WSAS) identified that more than half (55.9%, n = 278) of those assessed were identified with severe Functional Impairment and also positive for post-traumatic stress disorder symptoms (53.7%, n = 225). Of those veterans screened for an alcohol use disorder, nearly one-quarter (23.6%, n = 113) may have been identified as dependent on alcohol. Over one-quarter (28.5%, n = 136) were reported to have used illicit drugs, including 16.1% (n = 77) using opiates and/or crack cocaine and over one in ten (11.4%, n = 72) of veterans assessed stated that their drug use was related to their offending. Over three-quarters (76.6%. n = 383) of those assessed reported having symptoms of possible or probable depression. Regarding health needs, high levels of General Practitioner registration were noted (84.4%, n = 638), which aligns with offender populations reported elsewhere (Sondhi & Williams, 2018). Just under one-quarter (23.4%, n = 112) were prescribed medication. Following the initial assessment, people who engaged stayed for a mean of 36 weeks (range 0–165) until discharged, with over one-quarter (26.7%, n = 202) of all veterans assessed disengaged from the service (Table 3).
Summary of Selected Factors Associated With Disengagement Derived From—mim— (Royston et al, 2009) Used for Conducting Stepwise Backward Selection on the Imputed Dataset.
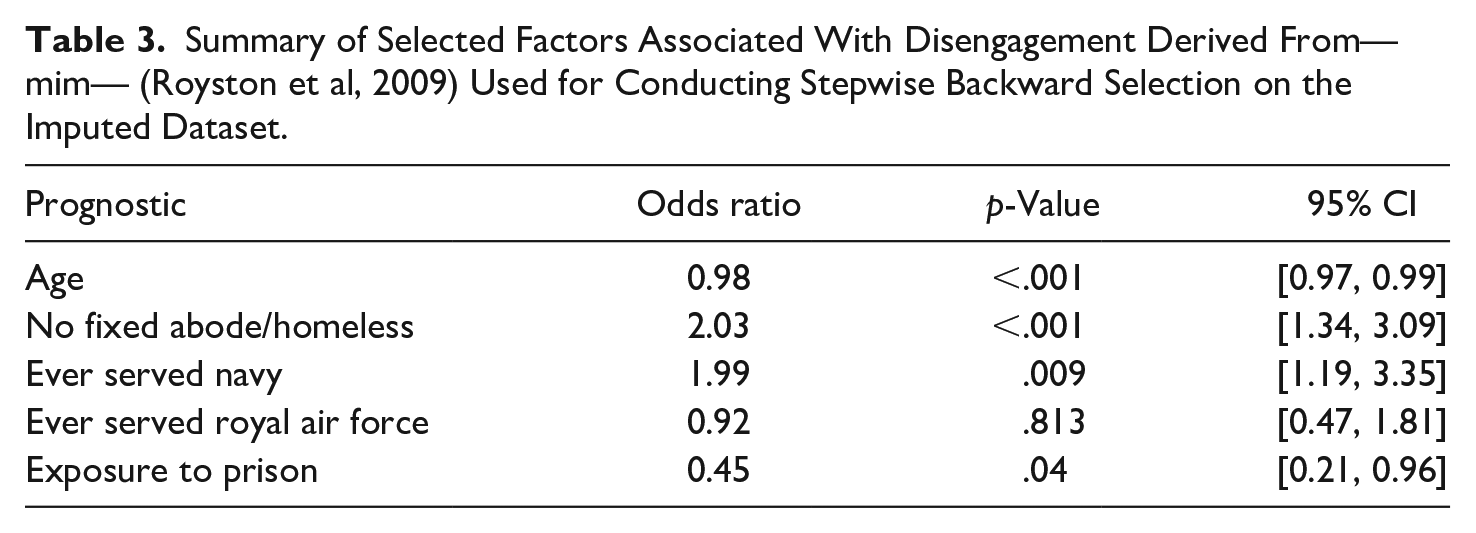
The statistical model suggests that four prognostics (out of a potential 34) were significantly associated with disengagement from the peer-based project following allocation to the caseworker. Namely, age, such that the older a subject, the less likely they are to disengage, by 0.98 times per year of age with a 95% Confidence Interval (0.97, 0.99). Veterans with no fixed abode were 2.03 more likely to disengage (1.34, 3.09) than subjects with fixed abode. Royal Navy veterans were two times more likely to disengage than Army veterans (1.19, 3.35). Finally, veterans exposed to prison sentences were 0.45 times more likely to disengage than veterans who had not been to prison (0.21, 0.96).
Discussion
We examined factors associated with veterans assessed by a peer-based intervention who engaged and continuously case-managed veterans arrested in police custody and who subsequently disengaged from that service. The service differs from the broader literature on diversion by not focusing on a single morbidity (mental health or SUD) but instead providing a support service for a veteran with any health and well-being issue and/or broader socio-economic harms. Overall, we show that this segment of criminally justice-exposed veterans assessed at the point of arrest reported extensive chronic, comorbid health, and socio-economic needs.
The importance of retention in diversionary programing has been shown to reduce recidivism (Brocato & Wagner, 2008; Maume et al., 2018; Ventura & Lambert, 2004) and over one quarter (26.7%) of veterans assessed disengaged following assessment, which compares favorably to just under half of the people who did not complete TASC programing (Maume et al., 2018) or an initial two-third (68%) level of disengagement from a police custody scheme for SUD diversion in the UK at a similar point in police custody (Sondhi & Eastwood, 2021). We therefore conclude that peer-led, continuous case-managed approaches that extend beyond engagement and the initial referral to ancillary services have efficacy in maintaining contact with veterans in the criminal justice system (Turgoose et al., 2018). Key enablers have been shown to emphasize the power of the therapeutic alliance between caseworker and client (Brocato & Wagner, 2008). Studies from SUD diversion schemes have also illustrated that case-management approaches are more than twice as successful in ensuring uptake into addiction services than generic referral-style methods (Sondhi & Eastwood, 2021). For veterans, close-knit peer support networks supplemented by intensive case-management techniques have been shown to reduce mental health stigma, minimize drop-out, and enhance more comprehensive integration into other services (Goetter et al., 2018; Pfeiffer et al., 2012).
Out of 34 potential factors, including socio-demographic characteristics and identified needs, only four factors were shown to be significantly associated with disengagement. Of these factors, none were related to identified criminogenic needs, SUDs, or mental health needs, suggesting that peer-led approaches may be effective in engaging veterans with complex chronic health and social harms. Despite a broad literature emphasizing veterans’ concerns about accessing mental health and other ancillary services for fear of stigmatization (Cornish et al., 2014; Michalopoulou et al., 2017; Sharp et al., 2015; Zinzow et al., 2013), peer-based services can provide a platform to integrate other interventions or referrals by providing social support and addressing practical barriers associated with treatment uptake (Adler et al., 2015; Greden et al., 2010; Hom et al., 2017; Zinzow et al., 2013). Other factors in our model that did not predict disengagement include veterans’ current offending behavior. However, we also highlighted that disengagement increases inversely to exposure to previous incarceration experiences. We speculate that this may reflect a range of available support services within the local area, including enhanced access to prison-based interventions that are aimed at improving in-reach before release (McKenna et al., 2015; Senior et al., 2014), including more personalized arrangements once discharged (Coté et al., 2020). This finding highlights the importance of continuity of care from prison to the community as a requirement for augmenting community-based provision. Further work is required to understand the relationship between previous incarceration and engagement with services at the point of the arrest.
Other factors associated with disengagement included age, such that older veterans were more likely to engage with the service, consistent with other peer-based services provided for veterans (Ellison et al., 2016) and similar for criminal justice engagement in SUD (Shannon et al., 2015). Engagement of older veterans may reflect the age of the peer caseworkers, who tended to be retired ex-servicemen and women, thereby maximizing the therapeutic alliance between veteran and caseworker. Although further work is required to understand the extent to which peer characteristics are relevant to engagement with veterans, we suggest that the inclusion of younger veterans into the model would enhance engagement. Broadly, we suggest that the pool of peers should reflect the population of veterans within an area. Veterans with acute housing needs or living with no-fixed-abode were shown to be significantly more likely to disengage, which is consistent with the broader literature concerning diversion schemes for SUD (Clark et al., 2013; Sondhi & Eastwood, 2021) and veterans (Tsai & Rosenheck, 2013). Homeless veterans disengaged with the service despite being on the caseload and receiving support, including being referred to secondary services.
Consequently, there is a need for tailoring the nature of peer support for veterans in acute housing needs, including homelessness, which may require the development of a housing specialism within the service. The final factor found to be significantly associated with disengagement was whether the veteran had ever served in the Royal Navy (including Royal Marines). The geographical study area included no naval bases compared to other parts of the country, and it may be conjectured that there is a relationship between a veteran’s military identity and a successful transition to civilian life (Herman & Yarwood, 2014). However, further work is required to confirm this hypothesis.
Strengths and Limitations
The study interrogated a comprehensive administrative dataset on veterans’ needs following their arrest and subsequent assessment by a caseworker. The data provided a unique longitudinal insight into the relationship of criminally-justice-exposed veterans with a peer-led volunteer service. We explored engagement over different time periods and assessed the factors associated with veterans’ commitment using a battery of validated tools covering a wide range of social needs and harms. Although there was missing data, the level was considered within acceptable levels (Heymans & Twisk, 2022) to deploy imputation methods to ensure most cases were included in the subsequent analysis. The study was implemented before and during the COVID-19 pandemic. Lockdown restrictions were not perceived to have affected engagement, as support and referral pathways were continuously offered through telephone and online channels. Furthermore, staff were available at the point of arrest, preventing any reduction in the service offered. Understanding peer worker characteristics is also required to provide details on the therapeutic alliance with veterans.
There are several limitations to this study. First, we have no information on the reason for disengagement. It is likely that this will be multifactorial and will include several possibilities, including people who disengage for positive reasons but may not communicate this to their caseworker. Further work, including Cox regression models, could be deployed further to explore the nature of time-to-disengagement. The data captured for this study did not indicate outcomes, including how veterans engaged with services, changes in offending behavior and any improvements in health outcomes. Further work is required to assess the model’s efficacy against these measures.
Conclusions
We conclude that a UK-based peer-support diversionary service located within police custody as part of a pre-arrest before charge/Sequential Intercept 2 model based on continuous case-management techniques is effective in engaging veterans with a range of chronic morbidities, including symptoms of post-traumatic stress, mental health issues, dependent alcohol consumption and severe functional impairment. Four factors associated with disengagement from the service include a veteran of younger age, no fixed abode/homeless, exposure to a prison sentence, and a Royal Navy background. Further work is required to address these four factors.
Footnotes
Acknowledgements
The authors acknowledge the help and support provided by operational members of staff who provided this service.
Author Contributions
Conceptual design: AS. Data acquisition, coding, and cleaning: AS and SL. Data analysis: AS and SL. Literature review: AS and LM. Review and interpretation of findings: AS, LM, SL, and CW. Preparation of first draft: AS, LM, and SL. Writing—reviewing and editing: AS, LM, SL, and CW. The authors read and approved the final manuscript.
Availability of Data and Materials
The data that support the findings of this study are available from Therapeutic Solutions (Addictions) but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of NHS England.
Ethics Approval and Consent to Participate
NHS Health Research Authority classified the study as a service evaluation and therefore ethnic approval was not formally required. Informed consent for the study was obtained through the service provider.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by NHS England.