
Abstract
Introduction
Although it is accepted that individuals with Parkinson’s disease must navigate challenges such as receiving their diagnosis and changing daily occupations, little is known about how they navigate. The purpose of this study is to deepen the current understanding of the experience of living with Parkinson’s disease and its implications for occupation through a narrative visual methodology (photo-elicitation).
Method
Six individuals with Parkinson’s disease were asked to take photographs and share verbal narrative accounts to illustrate their experience of living with Parkinson’s disease.
Findings
Results highlight the interrelationship between occupation and identity, as many of the participants’ stories were interpreted as foregrounding the negotiation of occupation, and how such negotiation shaped their sense of identity. Overall, three major themes were identified: (1) Framing the meaning of Parkinson’s disease (accepting the disease as part of who they were); (2) Negotiating engagement in occupation (ongoing deliberation over whether to continue engaging in certain aspects of life as Parkinson’s disease progressed); and (3) Being ready to accept changes that impact personal or social identity (readiness to accept help and to identify as someone with Parkinson’s disease).
Conclusion
Attending to insights regarding the lived experience of Parkinson’s disease will enhance quality of care through informing an enriched client-centered, occupation-based approach.
Introduction
While research has begun to highlight the psychosocial challenges of Parkinson’s disease (PD), there remains a lack of attention to the experience and daily negotiation of such challenges. Thus, while we know that individuals with PD face challenges related to issues such as receiving their diagnosis, losing physical capacities, changing their daily occupations, and accepting supports (Benharoch and Wiseman, 2004; Hartley et al., 2014; Holmes et al., 2013; Murdock et al., 2015), little is known about how such issues are navigated or the implications of such navigation (Soundy et al., 2014). Previous research has highlighted that challenges to occupation resulting from chronic illness have implications for one’s identity and wellbeing (Bryson-Campbell et al., 2016; Vrkljan and Polgar, 2007). Thus, occupation-focused research addressing the experience of PD can provide insight into how persons with PD negotiate daily life through occupations, and how this negotiation interacts with identity. Within this constructivist narrative study, six individuals were asked to story what living with PD was like for them, using photos and providing a verbal narrative. In this article, we highlight results of a narrative analysis that was guided by an occupational lens, highlighting how the interrelated negotiation of identity and occupation were a key part of the experiences shared.
Literature review
PD is a progressive neurodegenerative condition, traditionally conceptualized as a disorder affecting movement and motor control (Jankovic, 2008). Cardinal symptoms include tremor, rigidity, bradykinesia, and postural instability (Jankovic, 2008). At the same time, there has been increasing attention to non-motoric aspects of PD, such as neuropsychiatric, autonomic, sleep, and sensory symptoms (Macphee and Stewart, 2012). Symptoms are heterogeneous, and their presence, severity, and impact on function varies across individuals (Lewis et al., 2005).
Each person’s experience of PD is situated in a particular sociobiographical history, set of personal traits, and life circumstances; research points to particular events and issues that persons with PD often have to negotiate. For example, there are diverse ways persons with PD react to receiving their diagnosis (Reese, 2007). Some individuals report feelings of relief resulting from having a name for their symptoms, while others describe feelings of devastation, confusion, and fear (Phillips, 2006; Reese, 2007). In one study, participants with PD discussed their diagnosis as equivalent to a bomb being dropped on their sense of existence, and described the need to reconstruct their identity following this event (Phillips, 2006). While such identity concerns have begun to emerge out of the literature, they have not yet been a key focus.
A review of literature addressing psychosocial aspects of the lived experience of PD identified seven major issues, including: unpredictability; preoccupation with time and scheduling; fatigue resulting from cognitive demands; fighting to maintain independence; social and interpersonal consequences; emotional concerns; and body image insecurities (Holmes et al., 2013). Although much of this research did not focus on occupation, the ways in which these various issues had implications for the negotiation for occupation often surfaced in study findings; for example, Haahr et al. (2011) share the following account of a participant with PD who reveals her reluctance to go shopping at certain times of the day: When we go shopping downtown, locally … I say to my husband, I don’t want to go at noon, because it is medication-time, and it takes some time before it works … I will stand there like a statue unable to move anywhere. People are looking strangely, they really are, and I don’t like it. Even if people in town know that I am slow … you really don’t feel good … I simply don’t want to advertise for the disease (Haahr et al., 2011: 412).
Haahr et al. (2011) also highlight how the unpredictability of PD can lead to withdrawal from social occupations. This is particularly evident in the more advanced stages of the disease when unpredictability escalates, and individuals with advanced PD report feeling that most of their personal control has been taken away and that they are totally at the mercy of their bodies (Haahr et al., 2011). This is evidenced by the following account of a participant with PD who described the unpredictable on/off fluctuations of the disease as being awkward: It is awkward … you cannot plan that in 1 1/2 hours you will be doing this and this, because if the medication doesn’t work, whether it is too little or too much, then you are not well. Everything falls apart (Haahr et al., 2011: 413).
Some research has focused more specifically on occupational challenges, including work, self-care, and leisure (Benharoch and Wiseman, 2004; Murdock et al., 2015; Wressle et al., 2007). Such research has pointed to the psychological consequences associated with occupational loss, such as depression, anxiety, and decreased self-esteem, as well as relationship changes and financial impacts. Moreover, this research suggests that challenges to occupation associated with PD can also present challenges to the maintenance of acceptable personal and social identity.
Taken together, existing research has identified a number of psychosocial challenges a person with PD may face throughout the course of their illness. To build on this discussion, it is important that research more fully engages with the experiences of people living with the condition. To date, research methods have been concentrated in semi-structured interviews, with researchers dictating the flow of questions (Eccles et al., 2011; Wressle et al., 2007). By shifting research to narrative methodologies, participants have a more active role in sharing their experiences (Bukhave and Huniche, 2016). Moreover, given that narratives provide a means to actively shape and convey identity as well as to story occupation (Connelly and Clandinin, 1990; Molineux and Richard, 2003), this approach also has the potential to provide insights into how identity and occupation are negotiated within the daily lives of persons with PD. Thus, we conducted a visual narrative inquiry using an open elicitation approach to capture people’s stories of life with PD.
Method
Design and methodology
We conducted a visual narrative inquiry (Bach, 2008) situated within social constructionism (Crotty, 1998). Narrative methodology assumes that humans are driven to construct an overarching sense of meaning and purpose for themselves through story. A constructionist approach assumes that narratives are co-constructed through dialog between participants and researchers. Thus, narratives do not provide an unmediated picture of a static reality, but rather are dynamic, context-dependent accounts in which people actively construct and convey who they are, what they do, and how they make sense of their experiences (Riessman, 2008).
Narrative reconstruction has been proposed to be part of living with chronic illness, particularly when such illness leads to biographical disruption (Bury, 1982; Roussi and Avidi, 2008). Thus, a narrative approach was chosen to provide a means to not only understand participants’ lived experiences of PD, but also to further attend to interactions between living with PD and identity (Connelly and Clandinin, 1990; Hyden, 1997). Moreover, narratives provide a means to explore occupation (Molineux and Richard, 2003). Within occupational therapy and occupational science, narratives can provide key information regarding the range and type of occupations people participate in, a person’s experience of occupational change and transition over time, and how a person’s perception of him or herself is enacted and shaped through their occupations (Josephsson et al., 2009; Wicks and Whiteford, 2003). Thus, using narrative in this study also enabled us to consider the occupational dimensions of living with PD.
Visual narrative inquiry combines stories and visuals to explore experience and the construction of identity, and has been shown to enhance participants’ reflections on everyday experiences (Bach, 2008; Bukhave and Huniche, 2016; Clark-Ibanez, 2004; Harper, 2002). Photos are useful for encouraging continuous reflection, and for supporting deeper interpretations of experiences (Clandinin and Huber, 2010; Harrison, 2002).
Participant recruitment
Participant profiles at the time of their individual interview.

Data collection
Prior to data collection, each participant attended a meeting with the first author to discuss study procedures, and to receive a digital camera, undergo camera training, and provide informed written consent, including authorization to publish their photographs. Following this, participants spent four weeks taking photos to illustrate their experience of living with PD. Participants could direct a friend or care partner to take photos for them should they be physically incapable at a particular moment or if they would like to appear in a photograph. Participants were also invited to select existing photos from their personal collection. Individuals using photos that included the face of an individual were required to have a signed consent and release form from those individuals. Participants were not given a recommended minimum or maximum number of photos to capture.
After they had finished taking their photographs, participants participated in an individual narrative interview with the first author, either at the research institution or at the participant’s home. During the interviews, which lasted from approximately 50 to 90 minutes and were audio-recorded, participant-generated photographs were used to elicit participants’ stories (Clandinin and Huber, 2010; Harper, 2002; Harrison, 2002). Specifically, participants were asked to describe each photo, their reasons for taking it, what the photo meant to them, and how it conveyed their experience of living with PD. To further elicit narratives that placed the photo within the participants’ broader experiences of living with PD, probes were used to elicit more in-depth descriptions (for example, how does the photo connect with living with PD? What is difficult/positive about living with PD? What are your symptoms like and how do they affect your everyday life? How has the object in the photo led to changes in the activities or things you do over time?).
Data analysis
SL analyzed the data; at the time, SL was a student in occupational therapy, with research experience in topics surrounding mental health and the psychosocial experience of persons with neurodegenerative disorders. DR and KL provided guidance throughout the data analysis process.
Following professional transcription, interview transcripts, photographs, and notes made during interviews were included in the analysis. Data were analyzed in an iterative, inductive process, first attending to the voices within narratives, and then addressing voices across narratives (Riessman, 2008). The present paper focuses on the across-narrative analysis. Data coding and synthesis were managed through the use of NVivo© 10 software.
To consider the cross-narrative experience of participants, a thematic narrative analysis was conducted, which focused on the “what” of the stories told and sought to identify commonalities to theorize across cases (Riessman, 2008). Using a story analyst approach embedded in a constructionist paradigm (Smith and Sparkes, 2008), this thematic analysis was framed with an occupational perspective, aiming to focus on the ways in which participants portrayed and talked about occupation as part of the experience of living with PD. Following the process outlined by Braun and Clarke (2006), the first step in the analysis involved immersion through repeated and active readings of transcripts. Next, initial codes were generated through line-by-line coding of the transcripts, as well as analysis of contents within the photographs. Themes and subthemes were developed out of the list of codes, and interpreted through a lens informed by an occupational perspective and narrative theory attending to identity (Bury, 1982; Roussi and Avidi, 2008).
Findings
Three major themes were identified: (1) Framing the meaning of PD; (2) Negotiating engagement in occupation; and (3) Being ready to accept changes that impact personal or social identity. Overall, our analysis highlights the interrelationship between occupation and identity, as many of the participant’ stories were interpreted as foregrounding the negotiation of occupation and how such negotiation shaped their sense of identity. In turn, participants’ sense of identity often shaped their chosen occupations.
Framing the meaning of PD
In narrating stories about daily life with PD, participants incorporated ways of talking about PD that served as a means to frame their illness. Illnesses were framed in ways that facilitated processes of making sense of their life circumstances, and it appeared that this framing influenced how each person addressed if and how having PD was integrated into their identity. Participants discussed a continuum of framing that spanned accepting the disease as part of who they were to striving to maintain their sense of continuity with their pre-PD self and being a person with PD. Moreover, participants explained that their ways of framing PD were not static. For example, Gail stated: “I keep telling myself that it’s a make work project.”
Participants focused on the need to accept PD as part of their reality and how they saw themselves, that is, their identity. Participants tried not to let negative emotions control their everyday experiences. For example, as Robert described: Because what can you do about it? You got Parkinson’s. Well, you can say well, I hate it, but you got it. It’s not that you’re going to hate that much then it is gone. It’s going to stay with you. I say accept it and you live with it.
In negotiating this acceptance of PD, Clint made comparisons to other diseases, and considered himself lucky for having PD: “But, as someone once said to me, if I’m going to have a chronic illness, Parkinson’s is probably the one I’d choose, rather than cancer, or strokes, or anything like that.”
Participants also spoke of the importance of appreciation while living with PD. Lawrence explained that his photos represented both the challenges associated with PD and the positive memories of things he had previously accomplished. For example, as seen in Figure 1, Lawrence took a picture of electrical work he had completed prior to his diagnosis and used this photo to story how he appreciates having maintained the mental capacity to understand how to complete the electrical wiring despite having lost the physical dexterity to actually perform the task. For Lawrence: When I’m having a down day or just an off day, I just think about my old electrical days or roofing houses or buying properties. And my mind will go on a trip. And it’s an appreciation. […] with Parkinson’s, it’s not a lot of fun. And I just think that it’s not all negative.
Lawrence’s representation of an occupation he has given up as a consequence of progressing PD.
For those participants who positioned themselves as striving for continuity with the person they were prior to PD, stories were often paired with statements that indicated that PD was not a large influence within daily life. As Trevor stated: “I don’t really try to think about it. I don’t try to talk about it. It’s just something that I have.” In this form of framing of PD, participants often communicated a desire to remain the same person they were prior to the onset of PD. As Meg noted: “I’m still [Meg]. I’m not Mrs. Parkinson’s.”
Negotiating engagement in occupation
The drive to maintain engagement in daily occupations, conveyed as meaningful activities, pervaded many of the participants’ stories. Participants shared both stories of engagement in new occupations that developed out of a period of transition following the onset of PD, as well as stories of maintaining engagement in pre-existing occupations and stories of loss. Concepts of identity negotiation were found to permeate each story of engagement, thus providing insights into the interrelationship between identity and occupation.
For Gail, the initiation of a new leisure occupation was important for reconstructing her sense of who she was amidst a life transition. As she described, she was experiencing a time where important relationships were changing as a partial consequence of recently having received her diagnosis of PD. At that point, she began to engage in gardening and found that it gave her a sense of mental and physical strength (see Figure 2): Oh, when it [the garden] started was like my new life. And it really was because I don’t think I went out there and said, “oh I really want to make a garden.” I just thought, “I should put some plants in, some color or something.” And it was just – I think it was the thing that kept me going when I was all by myself […]. And I just thought, “I have to have something my own. And I have to be able to do it myself, by myself, with no other input.” And that’s how it happened. It just happened. And I surprised myself by being so – strong, I suppose, mentally and physically.
Gail’s representation of a new occupation that she initiated once being diagnosed with PD.
Participants also storied their negotiation of engagement in occupations that existed prior to the onset of PD. Stories of engagement were frequently positioned within a space of ongoing deliberation regarding whether to continue or to stop engaging in certain aspects of life as PD progressed. Each participant discussed how he or she devised personal methods for engaging in activities in spite of their PD-related symptoms. For example, participants strategized ways to facilitate their engagement in self-care tasks such as negotiating dressing and personal hygiene, connecting the importance of these tasks to maintaining a sense of independence. For example, Trevor described the process he developed for putting on different items of clothing, which was crucial for managing his challenges with balance. As seen in Figure 3, Trevor captured a series of five photos that he used to describe the strategy he uses to maintain independence with donning socks: That’s the stepping stool I use to get my socks on. Then the next one is starting my socks. I have to bend over. I get them about halfway up my foot – then, you get the next picture – I have to get on my toe and get them slid up. Then, the next picture is just emphasizing that I have difficulty getting it around my heel. The shorter the socks, the better off. Then, I got the sock up there in the last picture.
(a–e). Trevor uses a step stool to maintain engagement in dressing.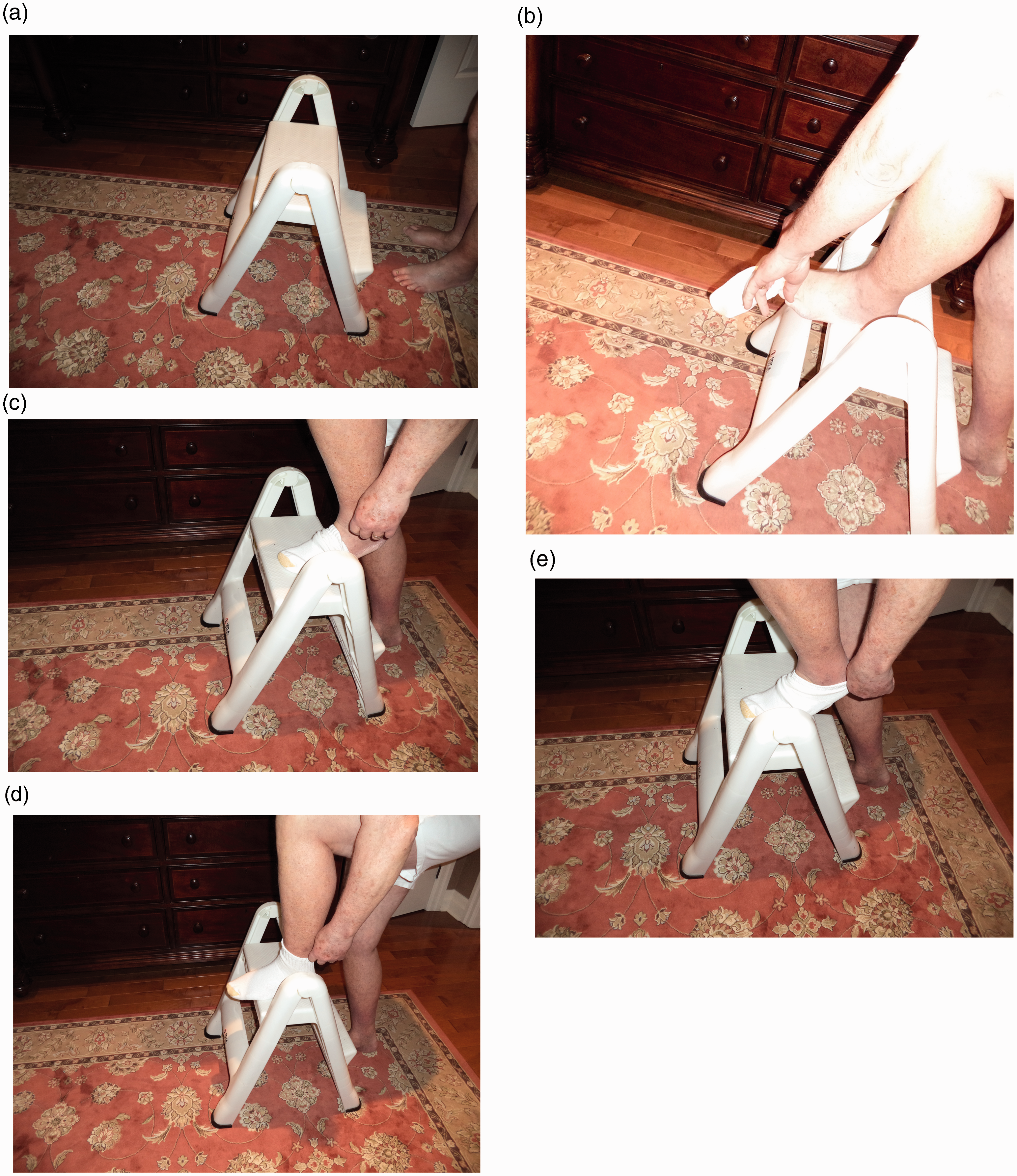
Across participants, stories revealed ways that maintaining engagement in occupations acted as a means to maintain the participants’ desired identities. For example, it was important to Meg’s identity to be a helper, leader, and teacher. Thus, she maintained involvement in various volunteer, leadership, and teaching roles, such as leading yoga classes and providing reflexology services at a local hospice. Meg maintains her engagement in them, appearing to resist negotiating a change in this part of her identity: “I’m too stubborn, too determined. And I’m – maybe things change so you accept it, but right now I wouldn’t like that to happen. I’m not ready for that to happen.”
Participants storied tensions between wanting to continue with previous occupations, and being restricted by their symptoms. When making decisions about whether to maintain or give up engagement in a particular occupation, participants often took into consideration whether the activity in question was meaningful to how they viewed themselves or wanted to be viewed by others. For example, Gail used a photo of her piano to express that music had been a constant part of her life and a way she defined who she was; thus, she continued to play the piano in spite of the PD-related difficulties (see Figure 4): Well, I have a degree in music education. And I’ve been playing the piano since I was 11. So it’s a real big part of my life. And I thought, you know when I move out of this house, “oh I better, I’ve got to have room for my piano.” So it’s just – and it’s another way of sort of saying, “I still have this,” you know, “I can still do this.”
Gail maintains engagement in music because it is meaningful to her, and important for her to “have that there.”.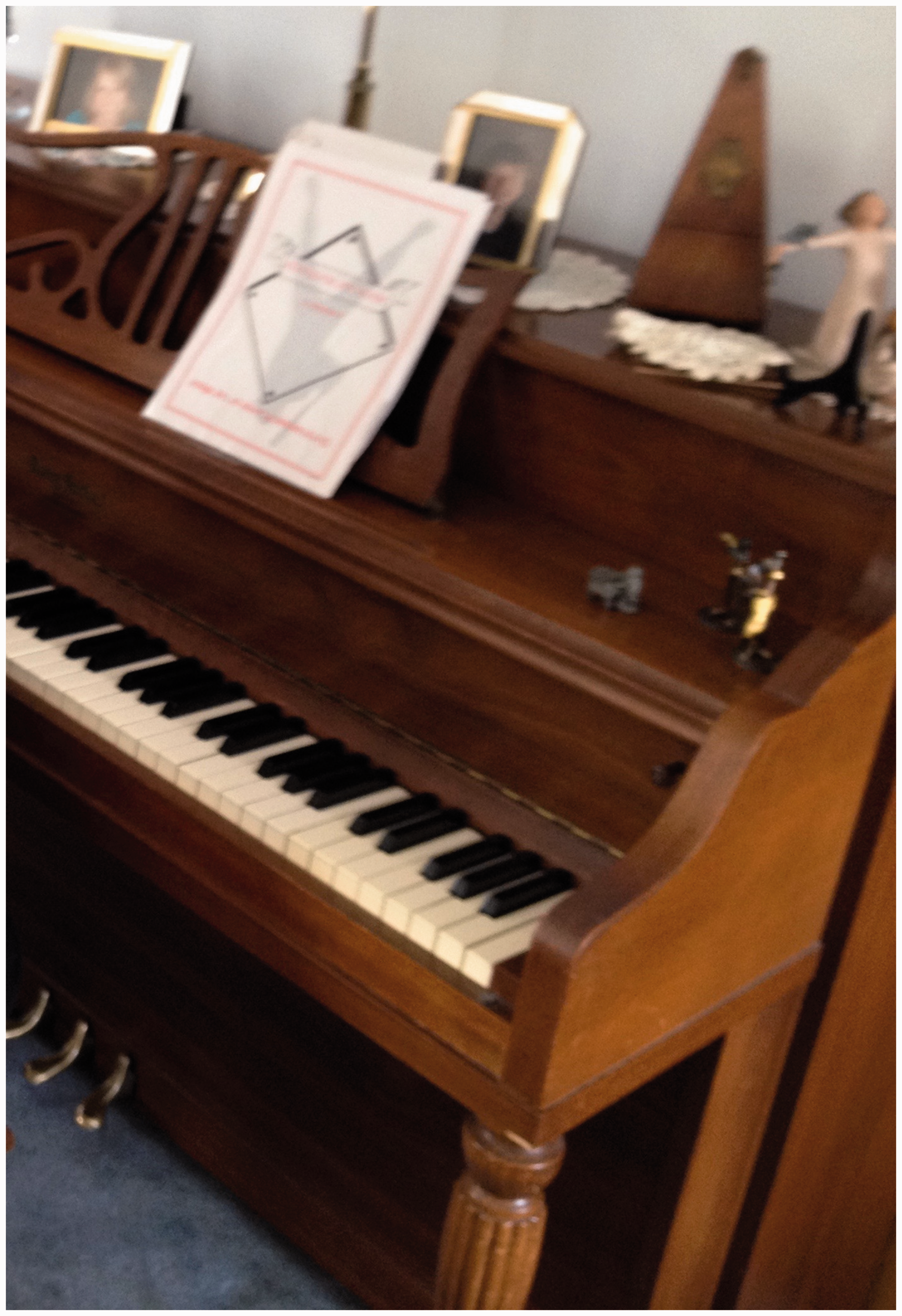
Adaptations were discussed as a way to facilitate continuation with occupations key to identity. For many participants, physical activity was an important part of life that was continually impacted by PD. Clint, Trevor, and Robert all took photos while on the golf course to describe how they found ways to continue golfing through adaptations. For example, Robert adapted his routine by playing nine holes instead of 18 and by using a golf cart to travel between holes. Robert also found ways to continue his identity as a worker. For Robert, work was an important part of life, and he had founded a welding business. Although he was no longer able to do the physical labor, Robert used a photo taken at his welding shop (see Figure 5) to discuss continuing with his work by going into the workplace and involving himself in the environment, thereby maintaining his identity as part of the shop and as someone able to contribute: “Go into the shop, talk to the guys and be re-involved in it, certain – to a certain extent. If there’s a problem, they know where I am.”
Robert adapts his engagement in work by still going into his shop, talking to the employees, and making himself available to provide help.
Participants also discussed moments when they decided that they could no longer continue an activity. Decisions to stop were often described alongside feelings of frustrations and mourning, especially when an aspect of identity was threatened. For example, Lawrence described the struggle he experienced hiring someone to do electrical work he would usually do himself: The size of the project has a bearing on whether I will attempt to do it. And it’s a fight or a struggle within me because part of me wants to be able to do these things forever, and the other part of me says maybe you shouldn’t do it.
Lawrence, however, negotiated ways to keep electrical work as part of his identity by recognizing the value of mentally remembering how to do the work: “And so just the understanding. It gives you self-worth. It makes you feel good about what you’ve accomplished, what you’re capable of thinking about.”
Being ready to accept changes that impact personal or social identity
Participants discussed having to negotiate several types of changes in relation to maintaining personal and social identity. The extent to which they were ready to accept changes arising out their illness, given their potential implications for how they saw themselves and were seen by others, appears to influence how they navigated such tensions. Overall, readiness emerged as a fluid and context-dependent concept in relation to changes associated with accepting help, physical changes, and taking up the identity of being a person with PD.
Accepting and receiving help from others was an issue that participants frequently narrated through a discussion of readiness. Participants often described their readiness to accept help as variable and dependent on the context. For example, Meg used a picture of herself walking with the support of a family member (see Figure 6) to explain that receiving help from a close, trusted person was both comfortable and necessary for her to manage PD. For Meg, having an arm from a trusted family member facilitated going for a walk along her favorite trail, which she expressed was a meaningful activity for her to continue. Accepting help from strangers or in public spaces, however, was often a difficult and uneasy task for Meg, which appeared to threaten her identity as a helper to others: “it’s that little old lady thing. I’m the one that should be taking care of somebody. You know, I worked with seniors all my life. […] it’s hard to do it the other way around.” Thus, for Meg, the degree of readiness to accept help was connected to both who was providing the help and in what context, as these features influenced whether the acceptance threatened Meg’s sense of herself as a person who helps rather than a person who is dependent on others.
Meg is comfortable accepting help from trusted friends and family members, which allows her to maintain engagement in meaningful occupations.
Participants also discussed issues of readiness with regards to tensions associated with accepting physical changes, particularly when such changes threatened how they saw themselves and how others saw them in relation to age. Both Meg and Gail discussed the difficulties of using a mobility device given that they perceived themselves as too young for a device: “I’m not even 60 yet. I’m not going in a wheelchair” (Gail). Meg indicated that her ego partly explained her resistance toward mobility device use, but that she needed to weigh this against being at a point in her illness where she needed such equipment for her own safety. Meg also described the challenge of accepting her limitations, comparing herself to a same age or older peer: “I have friends who are in the mid-80 s and they can walk faster than I can. That makes me mad sometimes.”
A last type of change discussed in relation to readiness was that of being ready to identify oneself, and be identified by others, as a person with PD. Lawrence discussed his readiness to talk about his condition, as well as his readiness for people to see him as a person with PD. For Lawrence, engaging with close friends and family was a comfortable situation, and he felt he could talk openly with these individuals about his challenges with PD. Lawrence, however, felt uncomfortable engaging with or seeing individuals who were not a part of his close circle of friends and family. For example, Lawrence used a picture of his computer to explain that he prefers to communicate with people who he has not seen in a while via email rather than face to face as he is fearful of them seeing him as a person with PD: People I haven’t seen for a while, and I meet them, and they knew me the way I was before. And I’m afraid to meet them […] I don’t want them to see me different than I used to be.
Some participants also provided narratives regarding their feelings toward socializing with other individuals with PD, and reflected on their readiness to engage and identify with them. For example, Gail used a photo taken at a support group to discuss how she feels more comfortable in settings with individuals with regular-onset PD, as opposed to early-onset. As a person with early-onset PD herself, Gail discussed her discomfort after attending a conference for individuals with early-onset PD: That had quite an effect on me, that early onset. Like up to now I’ve just had […] support group members as being older people, and you think, “Okay, that’s acceptable” […] I don’t know why I felt more comfortable with the older age group, but this – this conference I looked around and I thought, all these people are my age and all of the sudden I got really, really scared.
Discussion
A key way that the participants storied their experience of life with PD was as an ongoing navigation of occupation and identity, situated within how they framed the meaning of having PD. Participants’ narratives contained many occupational engagement stories, highlighting the centrality of occupation in daily life. Participants centered their narratives around their occupations, reflecting on occupations initiated, maintained, adapted, and lost throughout their journey with PD. As participants conveyed occupational engagement stories, the link between occupation and identity became apparent; as occupations were negotiated, one’s sense of identity was also impacted. For example, Meg viewed herself as a helper and caretaker to others. Receiving help, and not being able to provide help to others, was difficult for her to conceptualize as it ran counter to her personal identity. Identity also played a key role in determining which occupations the participants chose to maintain. If a particular occupation was strongly linked to a participant’s sense of self or its loss could threaten a desired social identity, they storied how they worked to keep that occupation in their life, even if at a lesser or different extent. For example, although Robert could no longer work directly in his welding business, he visited the shop and stayed involved in social and consulting roles.
The finding that occupation and identity are interrelated and mutually shaping complements other research within occupational science and therapy, which uses the term occupational identity to describe the relationship between a person’s perceived sense of self and their occupational history, current repertoire, and expected future (Kielhofner, 2004; Laliberte-Rudman, 2002; Unruh, 2004). Qualitative investigations addressing occupational identity have shown that the ability, or inability, to engage in occupation molds how a person perceives themself and is perceived by others (Klinger, 2005; Vrkljan and Polgar, 2007). Further, research has uncovered that individuals aim to engage in occupations that contribute to a sense of identity that is both acceptable and fulfilling to them (Laliberte-Rudman, 2002).
Studies on identity following a life transition, including chronic illness onset, have pointed to the potential for occupational disruption or a temporary state of restricted participation in desired occupations (Vrkljan and Polgar, 2007). Occupational disruption can threaten occupational identity and lead to a period of identity reconstruction, where a person may adapt their occupational engagement to redefine their sense of identity (Vrkljan and Polgar, 2007). In an investigation of occupational adaptation following traumatic brain injury, Klinger (2005) concluded that brain injury survivors negotiated a new sense of self in order to adapt their occupations and initiate a new way of engaging in activities (Klinger, 2005). In the present study, participants with PD often positioned themselves as striving for continuity in key aspects of identity, where they wished to be viewed by themselves and others as the same person they were prior to PD. As articulated by Meg, who stated “I’m not Mrs. Parkinson’s,” these participants storied a need for their identity not to be based on having PD, but rather on the occupations that they engage in, or engaged in prior to the onset of PD. In many cases, maintenance of occupations allowed for the maintenance of their identity. This finding is similar to that of Habermann (1999), who found it was important for participants to manage their PD by maintaining continuity, or “[carry] on as usual.” In addition, this study shows that participants were able to creatively adapt occupations in ways that also supported key aspects of identity, such that continuity does not always necessitate doing occupations in the same ways as before. These findings support a recent phenomenological investigation conducted by Smith and Shaw (2017), wherein people living with PD and their care partners described the importance of coming to terms with PD and adapting routine to overcome the barriers PD presents: “Well you just take it as it comes and you change your routine, as you need to ….” (18).
The present study, however, is not without limitations. An important limitation is that participants were at similar stages of disease progression (years living with PD ranged from 5–10 years); as such, this study does not encompass experiences of those newly diagnosed or those in later stages of the disease process. This study was also limited in that it only captured the experiences of one participant who had young-onset status (that is, received diagnosis before 50 years of age). Given that younger individuals are more likely to be employed for pay and to have young dependents, the occupational disruptions they experience are likely to differ from those of older adults living with PD. As a constructivist narrative study which employed an occupational and narrative lens in the analysis phase, the objective was not to obtain generalizable results via the use of a representative sample; rather, this study provides insights into the inter-connections between occupation and identity that are part of the daily negotiation of PD. Further research with more diverse participants is required to achieve more complex understandings.
Conclusion
This study contributes to the occupation-based literature by supporting findings that occupation and identity are interrelated, and adds an occupational lens to the body of work addressing lived experiences of PD. In this study, participants told stories of engagement in occupations that were critically linked to the negotiation of their identity. Occupational therapists working with clients with PD should be aware of the threats that occupational disruption can cause to identity. When therapists approach subjects such as changing, altering, or giving up occupations, it is recommended that they are empathetic toward the threats that such occupational changes can have on one’s identity, and strive for collaboration in their relationship with the client and to supporting maintenance of occupations defined as central to identity by clients. Importantly, help-seeking and help-accepting behaviors appear to be woven within a person’s occupational identity, and may be related to an individual’s willingness to accept the changes that are frequently associated with PD (for example rigidity, postural instability, bradyphrenia, etc.). This underscores the importance of supporting individuals with PD as they navigate maintaining independence while balancing safety concerns. This may also suggest that there is value in speaking with caregivers and family members about the importance of being sensitive to the specific needs of the individual with PD – and the critical role that valued aspects of identity, such as independence, may play in how daily life, including occupation, is negotiated by persons with PD.
Key messages
Individuals with PD navigate living with their diagnosis by forming a strong interrelationship between occupational engagement and their identity. Occupational therapists should strive to support maintenance of occupations that their clients define as central to their identity.
What the study has added
This study is the first to use visual narratives to examine the interrelationship of occupation and identity among individuals with PD. Participants told stories of engagement in occupations that were critically linked to the negotiation of their sense of identity such that disruptions to occupational attainment threatened their identity.
Footnotes
Research ethics
Ethics approval was obtained from the The University of Western Ontario Health Sciences Research Ethics Board # 103356, 2013. All participants provided written informed consent, in addition to providing consent to use their photographs.
Declaration of conflicting interests
The authors confirm there is no conflict of interest.
Funding
This research received funding from the Canadian Institutes of Health Research Operating Grant #326065 Neurosciences, Mental Health and Addiction.