
Abstract
Introduction
People with visual field loss after stroke often experience difficulties in everyday activities. The purpose of this study was to assess the acceptability of search training as used within occupational therapy and the feasibility of possible measures for use in a future trial.
Method
Nine participants took part in a goal oriented intervention that was delivered three times a week for 3 weeks. Patient reports of acceptability and outcomes using the Visual Function Questionnaire-25 were collected. Participants’ room-search behaviour before and after the intervention was recorded using a head-worn camera.
Results
Eight participants completed nine treatment visits. All participants reported improved awareness and attention to the blind side during activities following the intervention. Seven participants’ change scores on the Visual Function Questionnaire-25 exceeded six points. Patterns of head-direction behaviour and overall room-search times were variable across patients; markedly, improved performance was only evident in the most severely affected participant.
Conclusion
The intervention was acceptable. The Visual Function Questionnaire-25 is a feasible measure for assessing patient-reported outcomes. While the room search was informative about individuals’ behaviour, more sophisticated methods of gaze tracking would allow search processes to be determined in real-world activities that are relevant to patients’ goals.
Introduction
An estimated 60% of stroke patients lose part of their visual field or have eye movement problems, with 35% completely losing one half of their visual field (Ali et al., 2013). These deficits often persist, leading to long-term limitations in activities of daily living (ADL). In one survey, people with hemianopia reported poor performance in grooming, eating, mobility, reading, shopping, money management, driving, work and leisure (Warren, 2009). Hemianopia also causes people to bump into things when walking (Gilhotra et al., 2002) and increases the risk of falls (Czernuszenko and Czlonkowska, 2009; Ramrattan et al., 2001).
These limitations may in part be explained by inefficient visual scanning and searching (Warren, 2009). Laboratory based studies have shown that some patients with visual field deficits move their eyes to scan a display in a disorganised way. They make more repeat visits to visual targets than is normal and their eye movements towards the blind field have a reduced amplitude. Patients tend to miss some stimuli and have slower performance than controls in finding targets (Meienberg et al., 1981; Zihl, 1995). Patients looking at images demonstrate some intrinsic compensation for visual field loss; patients spent more time exploring the area of the picture corresponding to the blind hemifield than the seeing side (Pambakian et al., 2000). Problems are exacerbated in patients with visual field deficits who also have visuo-spatial neglect. Studies of search behaviour in patients with neglect show that they fail to explore the side of space contralateral to the cerebral hemisphere affected by the stroke, and in searching they frequently revisit stimuli on the ipsilateral side (Behrmann et al., 2004). Patients with both field loss and neglect have the poorest search performance (Behrmann et al., 2004). Visual search is an integral process within many ADL; for example, in finding items on the supermarket shelves or avoiding hazards when walking along the pavement. If the search and scanning behaviour observed in laboratory tasks is carried over to visual function in everyday life, it is easy to see how occupational performance may be affected.
The consequences of visual field loss are very often long-lasting. Six months after onset, people with hemianopia may be much more limited than people with other post-stroke impairments in terms of social functioning, role limitations and emotional wellbeing (Gall et al., 2010). Despite this, there has been no large-scale clinical trial of rehabilitation for visual field loss after stroke. The recent United Kingdom (UK) National Clinical Guidelines for Stroke (2016) fall short of recommending or even mentioning any specific treatment. The most recent Cochrane review found only limited evidence that training in compensatory visual search strategies may improve scanning and reading performance, and insufficient high quality evidence of effectiveness of treatments for improving independence in ADL (Pollock et al., 2011a). These conclusions are not significantly altered by the number of small studies that have evaluated different interventions since publication of this review (Gillen et al., 2015). There is a recognised need to find better ways to help people with visual problems after stroke; for example, the James Lind Alliance priority setting exercise for stroke rehabilitation research in Scotland has ‘What are the best ways to treat visual problems after stroke?’ at number five in its top 10 research questions (Pollock et al., 2012).
Current interventions, if offered, comprise giving information and directing patients to openly available computer based scanning and searching exercises (Rowe et al., 2016; personal observations: Clatworthy, http://hemianopia.blogspot.co.uk/p/for-patients.html). While computerised training offers a cheap means for self-directed learning, it is uncertain whether learning these abstract search tasks carries over to improved performance in ADL. Visual learning effects tend to be very task-specific (Schuett et al., 2012); it therefore makes sense to train visual searching within occupations. Using their core skills in assessing and facilitating occupational performance, occupational therapists are well placed to provide task-specific vision training. Visual search training is sometimes included within occupational therapy for people with visual problems (Pollock et al., 2011b). However, opportunities to practice extended ADL are limited in hospital; therefore, occupational therapists working in community services should be more active in helping people to improve their visual performance in everyday living. A previous study of an occupational therapy intervention (table top activities), delivered in an outpatient setting, showed promise for improving participants’ psychological adjustment to living with visual field loss (Taylor et al., 2011). However, this intervention was not goal oriented and it is not yet known whether visual scanning and search training in occupational therapy is effective for improving occupational performance in everyday living.
Prior to testing the effectiveness of complex interventions, the UK Medical Research Council recommends defining and modelling the intervention and testing its feasibility for delivery (Craig et al., 2008). We previously described an intervention for hemianopia, based on the practice of a specialist community-based occupational therapist (Turton et al., 2015). Using this description, an intervention guide was written giving the rationale for visual search training using valued activities and process activities. In the present study, we wished to determine the feasibility and acceptability of the intervention to participants when delivered three times a week for 3 weeks by an occupational therapy technician.
Another aspect of this modelling process is to determine the mechanisms by which the intervention works; in this case, how participants’ search and scanning behaviour is changed as a result of the intervention. Methods for measuring patients’ behaviours while searching real environments are not well developed, though this has been done in healthy subjects (Land et al., 1999) and in a single case study (Land et al., 2002). Visual exploration of scenes in the real world involve not only eye but also head and whole body movements, particularly when shifting the point of gaze by more than 10 degrees of visual angle (Freedman, 2008; Guitton and Volle, 1987; Land et al., 1999). A method for measuring where the person is looking with respect to a scene would potentially provide information about how an intervention works. Such measurement might include the search strategies adopted, learning rates, retention and generalisation of learning to untrained tasks. Eye trackers are commonly used in laboratories or other controlled environments (Howard et al., 2011, 2013); however, eye trackers are delicate and expensive. Assessing where people are looking in the wide field searches that are predominant in daily living may not require the precision of eye trackers. Because large gaze shifts involve movements of the head and trunk, a measurement of head position relative to the scene provides a proxy for gaze position. In this study we tested the suitability of using an inexpensive head-worn camera to record search behaviour of participants before and after receiving the occupational therapy intervention.
A further part of the modelling process is to determine the suitability of relevant outcome measures that could be used in a definitive trial. For this purpose, we selected the US National Eye Institute’s Visual Function Questionnaire (VFQ-25), a patient-reported outcome measure comprising vision-related and social constructs (Mangione et al., 2001). The VFQ-25 was not developed specifically for stroke (Hepworth et al., 2015), but it has good reliability and construct validity in patients with age-related macular degeneration (Revicki et al., 2010). We wanted to see whether the questionnaire would be able to measure change in people with visual field loss due to stroke.
In summary, our modelling phase study had three aims:
To test the acceptability of a 3-week home-based occupational therapy programme for training visual search within the context of participants’ goals in everyday living tasks. To evaluate a room-search task for its utility in determining search behaviour in the sample. To test the VFQ-25 as a measure of change after intervention.
Method
This was a small cohort study. Approval was obtained from South West Frenchay NHS Research Ethics Committee (ref. no. 11/SW/0306). All participants gave written informed consent. Written consent was also obtained from other adults in the household since the room-search video recordings were made in their homes.
Participants
Inclusion criteria:
Diagnosis of stroke (physician’s judgement); To be discharged to home; Performance in ADL affected by visual search problems (occupational therapist’s judgement); Failed at least one of the confrontation test (visual fields) (Pattern, 1996) and Star Cancellation task from the Behavioural Inattention Test (Wilson et al., 1987); Judged as able to participate in the research processes and intervention; Able to consent to participation.
Exclusion criteria:
Previous history of severe sight impairment; Previous history of disability affecting personal care (modified Rankin score 4 or more) (van Swieten et al., 1988); Under 18 years old; Discharged to a nursing home or to residential care.
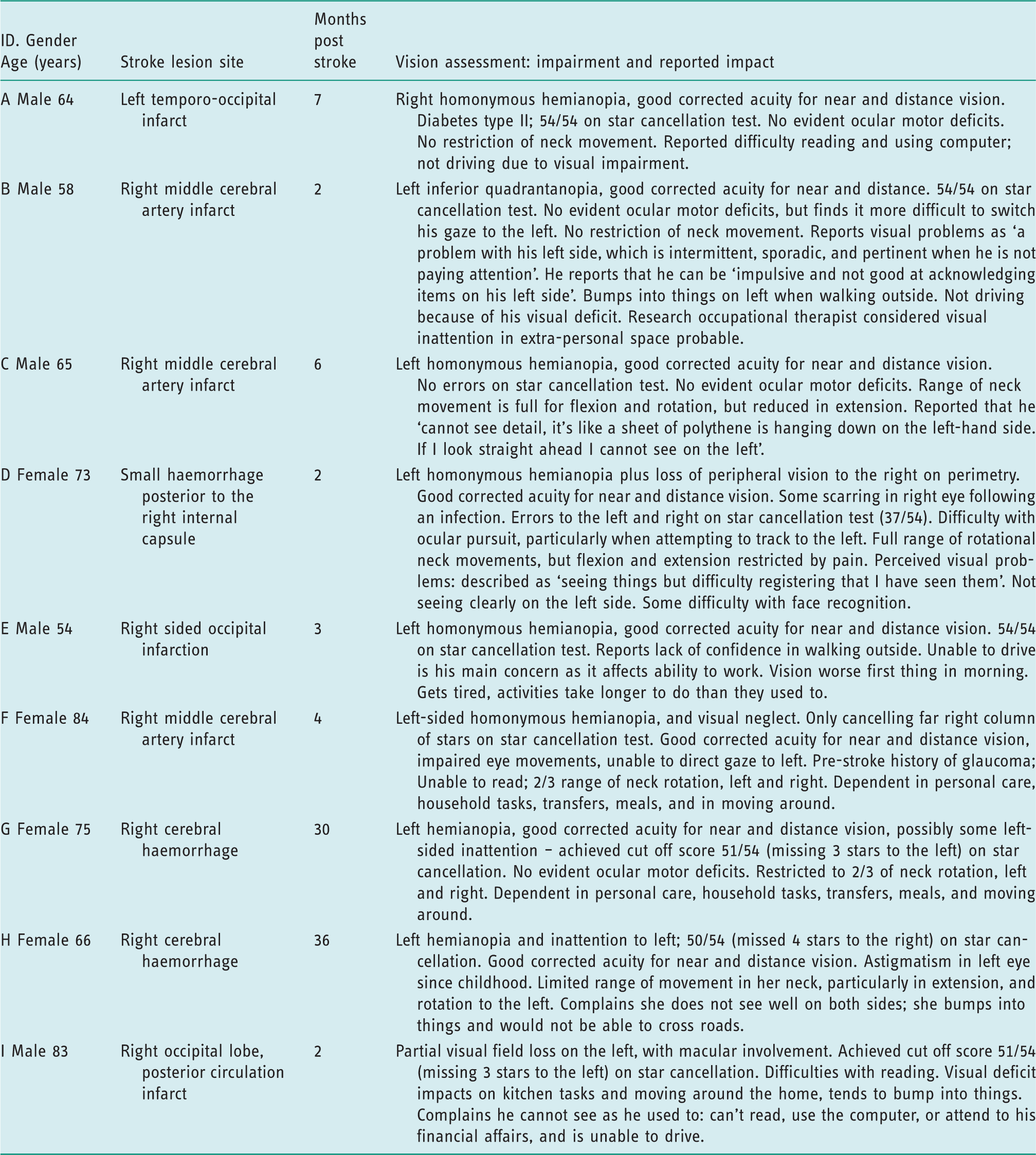
Consecutive service users fitting the eligibility criteria were identified by a community stroke care co-ordinator and from the local hospital’s stroke rehabilitation ward. Participants were recruited by stroke research network officers in the local acute stroke service or by the research occupational therapist in the community. Demographic characteristics of participants were collected: age; gender; side of stroke; lesion site; time since stroke; motor and sensory deficits; results of vision examination including perimetry (orthoptist’s report).
Recruitment took place from 1st January 2013 to 31st January 2014.
Intervention
The main principle of the intervention is that the search training should be specific to and tailored for the participants’ goal occupations. Participants learned to systematically search all relevant areas of the environment for the task, especially their blind side. Before commencing the intervention, an assessment, goal-setting and planning visit was carried out by the research occupational therapist. She used her own vision assessments and goal-setting procedure. Following this visit, participants received an intensive course of scanning and search training using various process activities and occupations. Task-specific learning requires intensive practice and therefore it was decided that the intervention should be delivered in three 1-hour visits each week for 3 weeks. The therapy programme for this study was delivered by two part-time occupational therapy technicians, who were supervised by the research specialist occupational therapist. The intervention guide, written for use in the study, provided direction and examples indicating: how to educate the participant about the effects of their visual problems on ADL performance and the need for compensatory strategies; the use of systematic scanning within the context of meaningful and goal-specific activities; the use of process (or remedial) activities to intensively train search strategies, for example beginning to search a table top or room on the blind side and to systematically search back towards the seeing side; grading difficulty by manipulating distractors and the area of space for the task (Turton et al., 2015). One or two ADL were selected for practice according to the participant’s goals. Examples include preparing food or drinks, playing a card game, steering a powered wheelchair, or outdoor tasks such as walking in the street or shopping. To demonstrate fidelity to the intervention, the occupational therapy technicians completed structured treatment logs giving details of activities used, their purpose, examples of search strategies and comments on participants’ performance.
Participants were encouraged to record their experiences of occupational therapy visits, to act as a reminder when asked to answer a structured questionnaire about their perceptions of the intervention. This questionnaire was completed either by telephone, or face to face if time allowed. It comprised closed questions about the acceptability of the frequency of visits, and whether the benefits justified the effort required to participate. Participants were asked to rate how beneficial they perceived the intervention to be on an 11-point numerical scale (0 being not at all beneficial, 10 being extremely beneficial). They were also asked what difference they thought the intervention had made to them and what they liked and disliked about it. While it is acknowledged that having the therapy team ask the questions risked biasing participants’ responses, the advantage was that the team would gain a more detailed understanding of how the intervention might be improved.
Room-search process measurement
The room-search task was developed by the research team for this study. A small, familiar, unobtrusive object belonging to the participant was searched for, for example a key on a fob. The task was standardised as much as possible within the participant’s home setting. A Go-Pro digital video camera was positioned squarely on the participant’s head and secured with an elastic strap (Figure 1 inset). The position of the camera was aligned using a laser pointer to ensure the camera was facing straight ahead. The participant was seated centrally against one wall of the room, giving scope for searching the room directly in front of them and to their extreme left and right sides. The tester divided the room mentally into eight sections from the point of view of the participant; no physical markers were used. The facing wall and area in front of the participant was divided into central left upper and lower quadrants and each peripheral wall or space was divided into upper and lower halves (see Figure 1). Sixteen searches were performed, with the object being placed twice in each of the eight sections. The order in which locations were used across trials was random.
Room search and head-worn camera (inset).
The participant was seated with eyes closed while the object was very quietly placed to minimise auditory cues. The participant was told when to open eyes to start each search. Each search was recorded from the head camera and timed manually using a stopwatch. Searches were stopped after 120 seconds if the object had not been found, to prevent frustration, demoralisation or boredom. The room-search task was piloted on a sample of 10 healthy volunteers who searched symmetrically across the rooms used (Turton, 2014: 15–17).
The room-search task was carried out at the first assessment visit and in the week after completion of the intervention. The task was administered by the research occupational therapist, with the help of an occupational therapy technician. Resources did not allow for an independent assessor.
VFQ-25
The VFQ-25 was administered on the assessment visits before and after the intervention by the research occupational therapist. The VFQ-25 represents 11 vision-related constructs: general vision; ocular pain; near vision; distance vision; driving; peripheral vision; colour vision; role limitations; dependency; social function; and mental health, plus a general health question. Rasch analysis has suggested that the measure may have better internal consistency without the items for general health, pain around the eyes and driving, and that its constructs could be collapsed into visual functioning and socio-emotional scales, respectively (Marella et al., 2010). The minimal important difference of the total composite VFQ-25 score was 6.13 points in a study of patients with diabetic macular oedema (Lloyd et al., 2013).
Data analysis
To indicate feasibility, the number of intervention visits was counted and the tasks and activities summarised and compared with the intended number and scope of the visits. For assessment of acceptability, responses to the participants’ questionnaire about the intervention were collated.
Video recordings of the room-search task were independently coded by a university researcher. Sports analysis video player software (Kinovea) was used to create crosshairs, which were aligned to the centre of point of view of the camera and therefore the direction that the head was pointing. With reference to a diagram showing the room divisions (as in Figure 1), the video was played slowly so that the assessor could follow the cross hairs as it played and record the head-direction sequence on the diagram. A new head direction was coded when the camera crossed into a new segment, for example upper left, upper central left, upper central right, etc. ‘Head direction’ refers to the position in space to which the centre of the head is pointing; in natural viewing this approximates the region in space to which the eyes (and so the centre of the visual field) are directed. The number of head-directions in each section of the room was calculated for each trial and summed across all 16 trials. From this, a proportion of head-directions in each half of the room was calculated. In addition, the first five head-directions for each trial were used to count the early search head-directions on each side of the room (blind or seeing side). For these frequencies, we calculated 95% confidence intervals for each participant. The durations of trials were summarised as medians with interquartile ranges. A note was made of the trials truncated at 120 s and the position of the object in these failed searches.
In presenting the data we have taken a case series approach to preserve the diversity of the participant sample.
VFQ-25 scoring was carried out in accordance with the test manual: raw scores were recoded as percentages of the maximum scores, and items within each subscale averaged together to create subscale scores; the average of the subscale scores provided an overall composite score. Change scores for each subsection were determined. As suggested by Marella et al. (2010), items relating to general health, pain around the eyes and driving were excluded from the analysis.
Results
Participants.
Goals and activities.
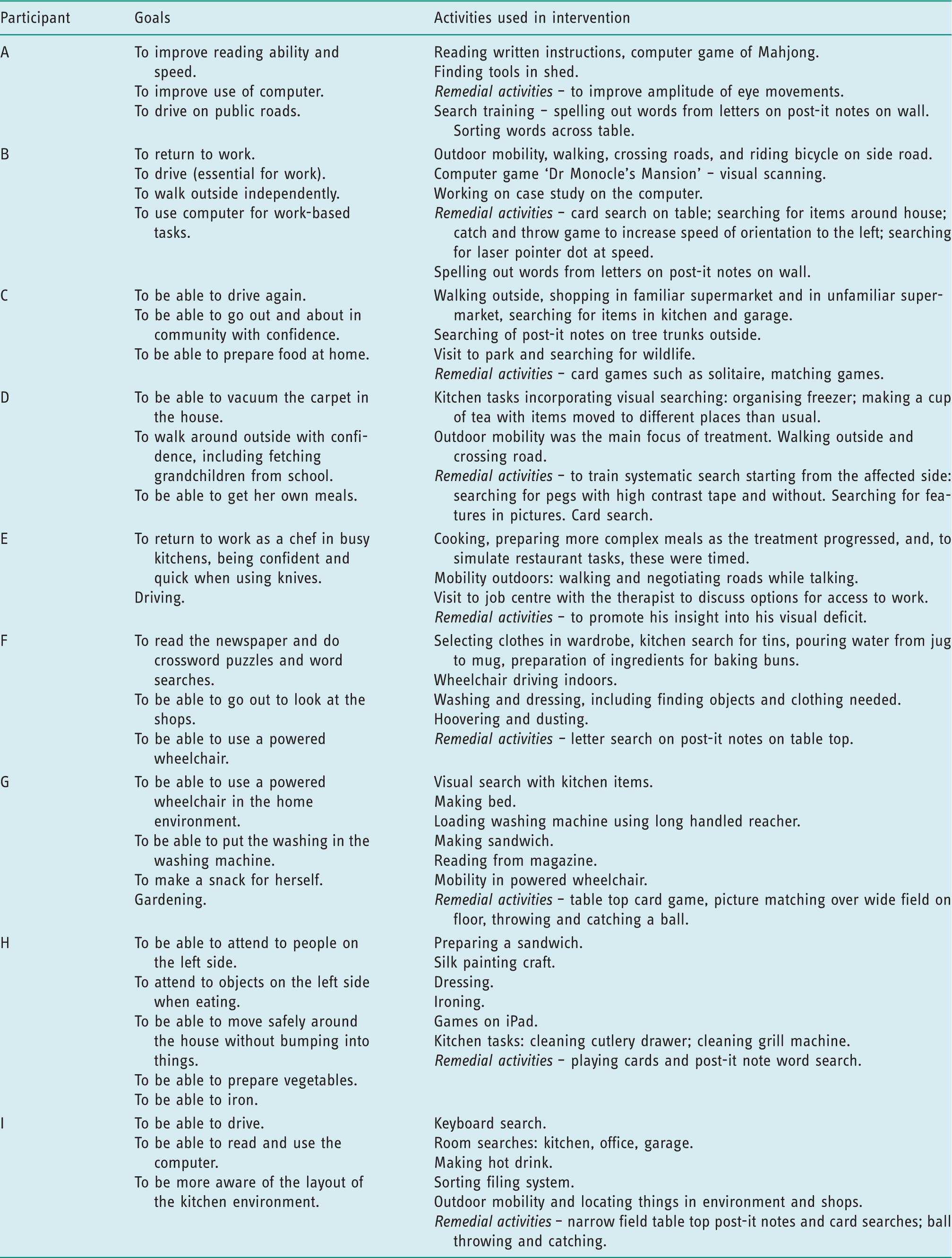
Process training activities such as finding playing cards from an array on a table top or across the floor were used with all participants to increase insight into the effects of visual field loss and to provide intensive practice in using new search strategies before trying them out in goal tasks. Eight participants had all nine intervention visits; participant E received eight visits, after which he returned to work.
Participants’ views of the intervention
Participants’ observations of the benefit of the intervention.
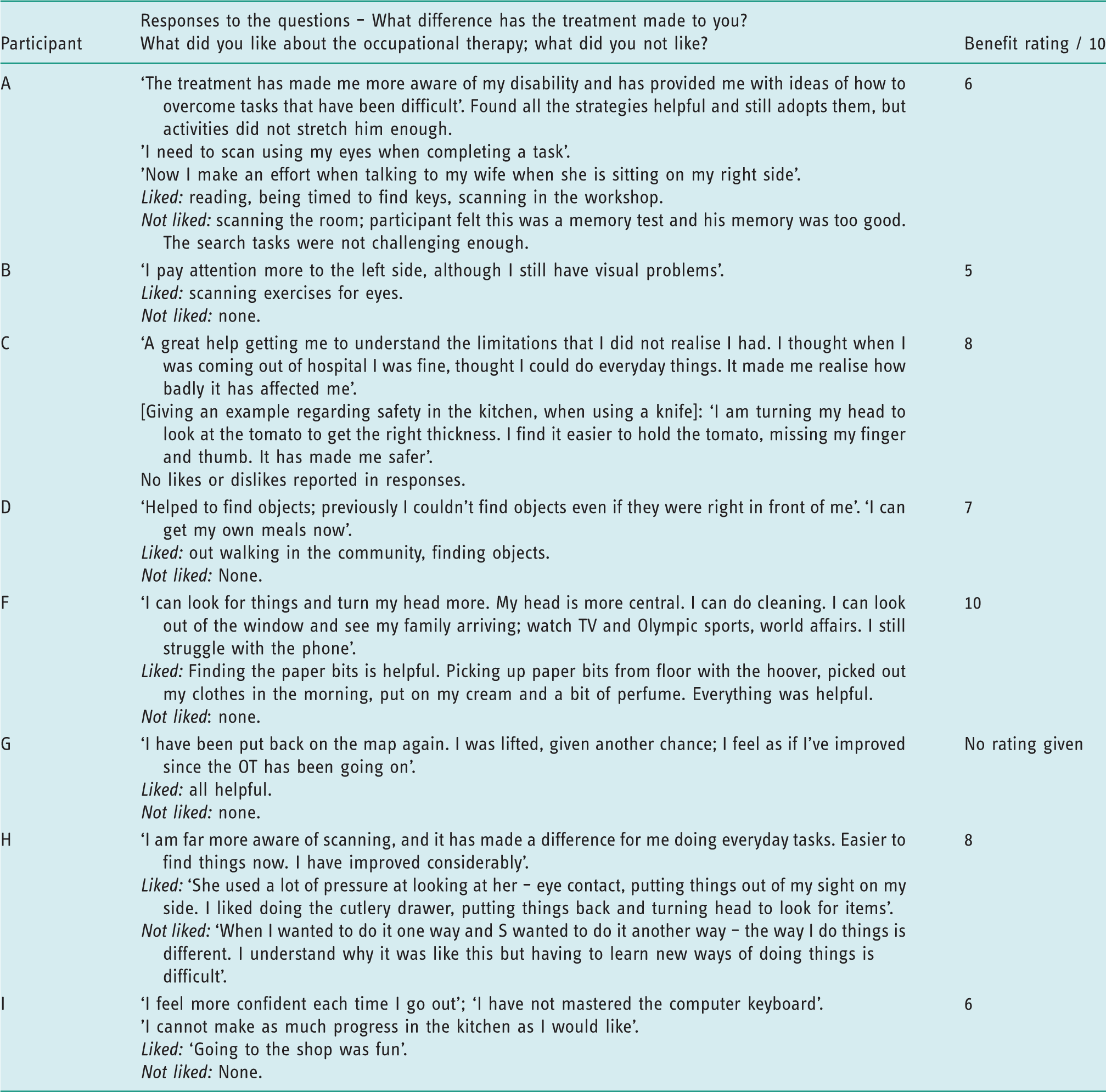
Participant E did not complete the questionnaire.
Room-search results
Figure 2(a) shows the percentage of head-directions in the half of the room on the participants’ blind side before and after intervention. All nine participants directed their head movements to both sides of the room. Figure 2(a) shows evidence of an increase in searching on the blind side following the intervention for participants C, F and G. Participant A appeared to search the blind field less following the intervention. Note that this participant demonstrated a strong bias towards searching the blind field rather than the good field before the intervention; given that the target is equally likely to be in either side of the room this change could be considered adaptive.
Participants’ room-search performances before and after the intervention.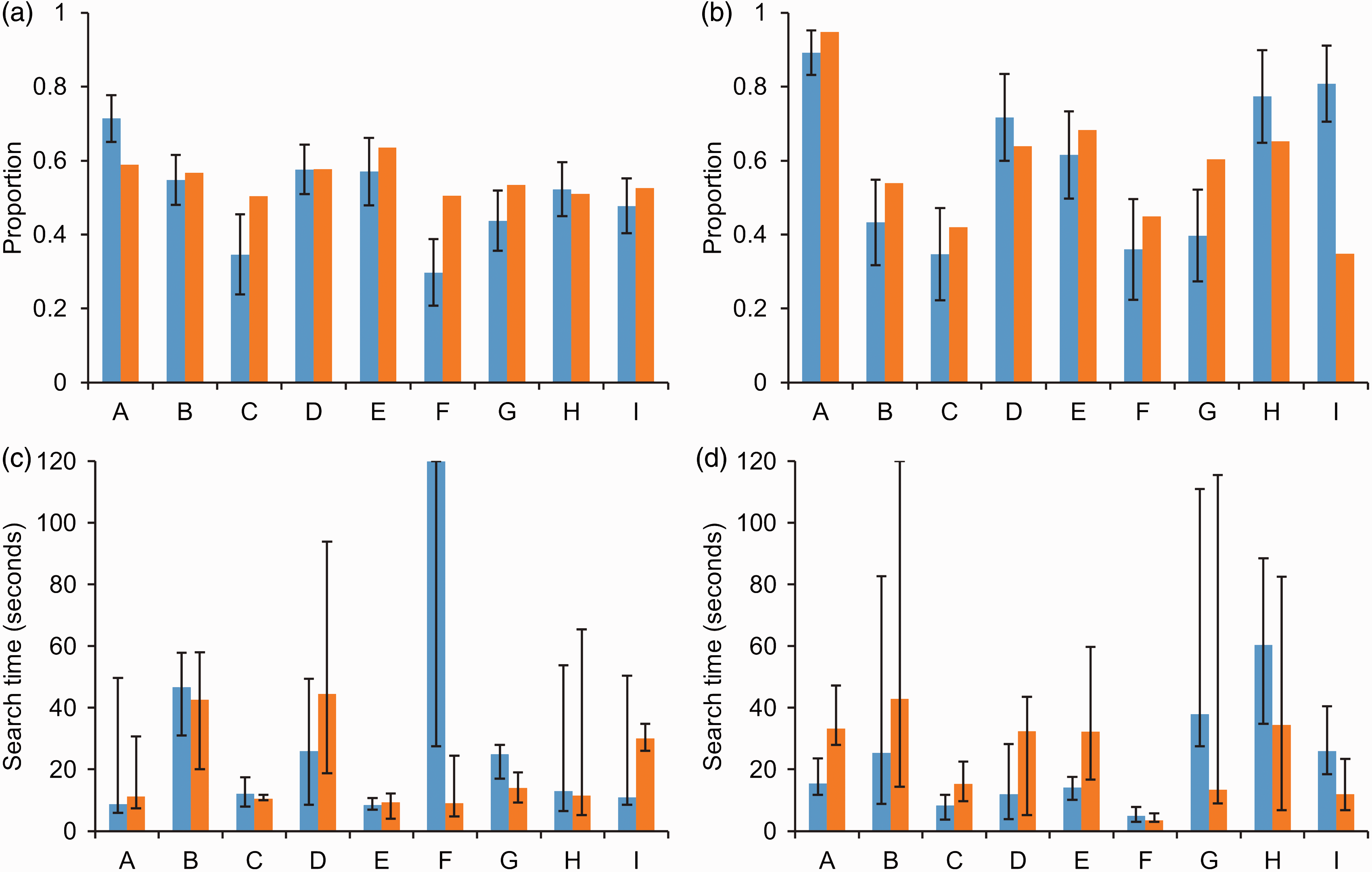
Figure 2(b) shows the same data as Figure 2(a) but for the first five head-directions only. Participant A again displays a strong bias to start the search on the blind side both before and after training. Participant G’s increase in searching the blind field after treatment is evident in this early search phase. Participants H and I show a dramatic decrease in early search of the blind side after treatment, but comparison with Figure 2(a) suggests this must be compensated for by searching the blind side later in the search process.
Figure 2(c) and (d) plot participants’ median search times and interquartile range (IQR). There is little data available here per participant so only qualitative comparisons are appropriate. Search times were very variable overall, with a number of trials being stopped at the 120 second limit. Except for participant F, there is no clear link visible between head-direction behaviour and overall search times across patients.
VFQ-25
VFQ-25 scores.
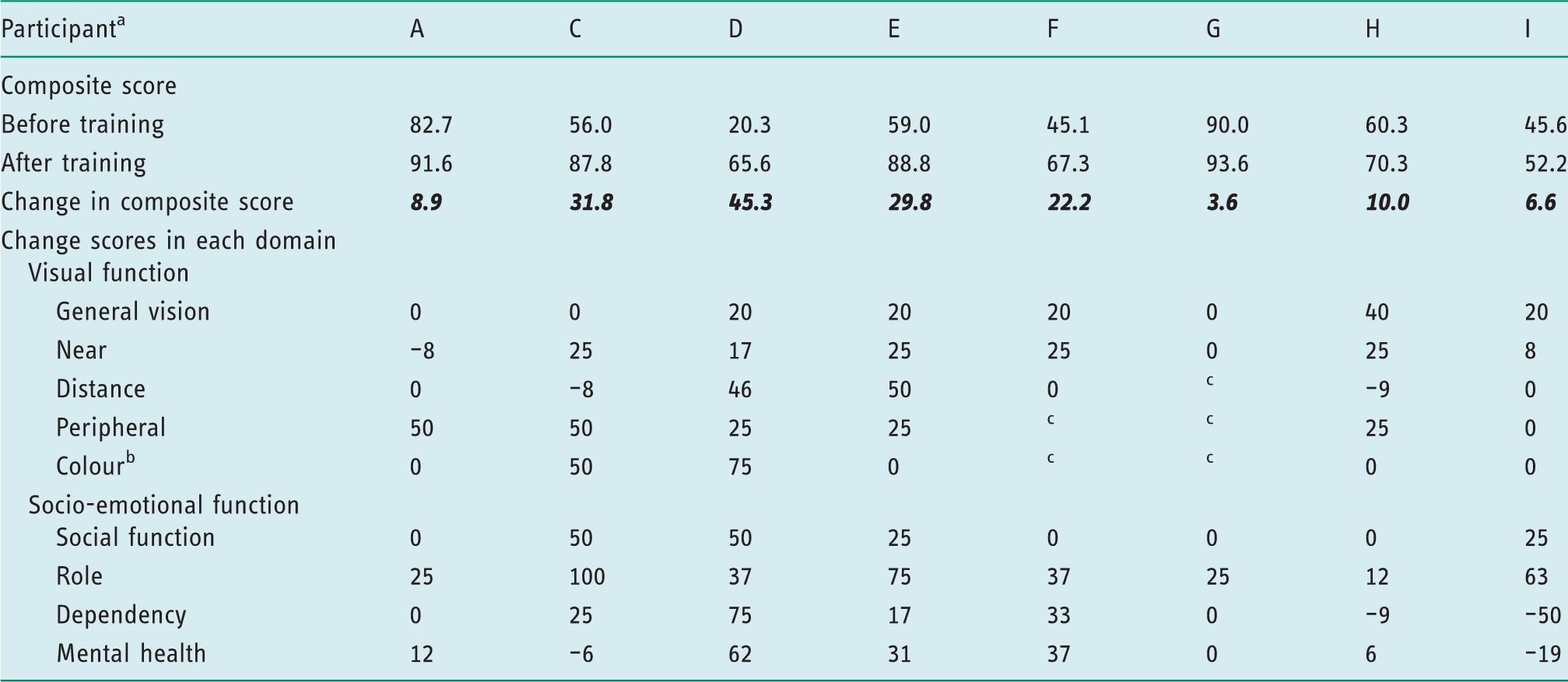
VFQ-25 questionnaire items are scored so that a high score represents better functioning.
Participant B did not complete VFQ-25 post intervention; his composite score before intervention was 83.6.
Colour is a question that asks participants to rate how much difficulty they have picking out and matching clothes because of eyesight. Participants in this study may have difficulty picking out clothing due to search difficulties rather than due to colour vision.
Participants responded to questions about activities in distance, peripheral, and colour with the option: ‘Stopped doing this for other reasons or not interested in doing this’; for example, the peripheral vision item is a question that asks, ‘Because of your eyesight, how much difficulty do you have noticing objects off to the side while you are walking along?’ Participants F and G could not answer this question since they are unable to walk. Bold represents the difference between before and after training scores.
Discussion
Goal-specific visual search training was delivered to nine participants with stroke-affecting visual functioning. This small sample contained a wide range of visual and physical functioning. Consequently, we applied visual search training to a diverse range of everyday activities.
The intervention utilised activities identified as goals by the participants and was delivered intensively in one-hour visits, three times a week for 3 weeks, by occupational therapy technicians. This is more intensive than is usual in the local community occupational therapy service where the research occupational therapist works, where visits to service users with visual problems after stroke are typically once every 2 weeks or once a month over several months. After 3 weeks of more intensive intervention, the study participants reported increased awareness of their visual field loss, and being better able to find things and carry out everyday activities. They found the frequency of visits acceptable and considered the benefits to be worth the work done. Occupational therapy is a complex intervention and may have differing effects and influences on different individuals. While the amount of training given was deemed acceptable by participants and intensity of practice is important for learning, the duration of the therapy programme could be varied according to individual need.
Accurate and sensitive methods for measuring visual search performance in everyday activities are needed to determine learning achieved. The room-search task was designed to capture search behaviour in a familiar space. In training compensatory search strategies, we aim for more efficient and successful searching. The room-search results showed that search behaviour varies between individuals. In concurrence with previous findings of intrinsic compensation in viewing images (Pambakian et al., 2000), our room-search results showed that some individuals had already begun to spend more time searching on their blind side before the start of the intervention. Nevertheless, searching on the blind side was increased after the intervention in some patients, though this did not necessarily decrease search duration. While overall the room-search results demonstrated considerable variation across participants, one participant stood out as having substantially improved success in searching: participant F showed remarkable improvements in the time taken to find objects on her blind side after treatment. This participant was the most impaired in terms of inattention and eye movements; she was unable to direct her gaze to the left and was severely physically impaired. Four months post-stroke she was dependent in personal care and transfers and could not move around her home. The goal-directed intervention included searching for clothes in her wardrobe, kitchen activities, and driving an electric wheelchair. Although we cannot be certain her improved performance was not due to spontaneous recovery (Farne et al., 2004), it is likely to have been influenced by the opportunity the intervention provided to intensively learn to explore her environment.
The room-search task proved to be useful in investigating search behaviour in a real-world space and was low-cost and robust. This is an important departure from tests used in clinical practice where performance is usually confined to narrow field tasks in near space using computer screens or pencil and paper cancellation tasks (Pollock et al., 2011a). We believe the room-search task represents a significant and important improvement on current process measures. However, it still suffers from a number of limitations: It was a stationary task and was very deliberately used to test performance, without the distractions of real ADL. Consequently, participants’ performance may not reflect their behaviour in real life. This static task may also not be very informative about activities in which the participant is moving about, for example walking around outside or in shops, driving a wheelchair, or in kitchen activities.
Different real-world tasks have different speed and accuracy requirements and perhaps different search strategies should be encouraged accordingly. The intervention was substantially goal-directed and performance measures should be relevant to the tasks that the intervention is aiming to influence. Camera technology is improving: in the short space of time since we started this study, affordable spectacles with digital video cameras set into the bridge have become readily available. More sophisticated software for mapping gaze to the environment are also developing (Leelasawassuk, et al., 2015; Lukierski et al., 2017). Currently the technology cannot reliably capture where the viewer is looking in busy environments or poorly lit conditions, but once these challenges are met, understanding search patterns in everyday life may be more accessible and become part of process measurement in occupational therapy practice.
The VFQ-25 measured change after the intervention across participants. Change scores indicated probable clinically important improvements, suggesting greater confidence in everyday living and participation. Of course, these perceived gains may not have been due to the intervention; there was no control group nor methods to reduce bias. Natural recovery, increased attention from the research therapy team, the familiarity and possible bias of the administrator, or other influences may have affected the change in VFQ-25 scores. However, the results suggest the VFQ-25 could be a useful outcome measure in a larger randomised control trial.
In conclusion, this study has established that this visual search training programme is feasible and acceptable within community-based occupational therapy and was generally liked by participants. The VFQ-25 appears to be a good candidate for an outcome measure in a future clinical trial. We have taken a step forwards towards evaluating the intervention and determining an appropriate outcome measure for a future trial.
Key findings
A community-based occupational therapy intervention to train visual search in people affected by stroke is acceptable and feasible. A room-search task was informative about individuals’ performance, but more sophisticated methods are needed to evaluate search processes in a variety of real-world activities.
What the study has added
The study has shown that this intervention is acceptable and feasible. It has also demonstrated measurement of search in the home context.
Footnotes
Acknowledgements
Laura Paterson and Sue Reynolds, Peninsula Community Health Occupational Therapy Service, delivered the intervention, with supervision from Jayne Angilley. We are grateful to the Therapy Services manager, Gill Mead, for her support for this project. Thanks to Dr Iris Terrer Dimwadyo for providing independent analysis of the room-search videos. Thank you to the research team at Truro Hospital. Last but not least, our warmest thanks go to the participants.
Research ethics
Approval for the studies was obtained from South West Frenchay NHS Research Ethics Committee (ref. no. 11/SW/0306, Occupational Therapy Vision After Stroke, 28/10/2011). All participants gave written informed consent to participate and be videoed. Written consent was also obtained from other adults in the household since the room-search video recordings were made in their homes.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a Research Priority Grant from the UK Occupational Therapy Research Foundation.