
Abstract
Introduction
Primary care is an emerging area of practice for allied health practitioners. The effective integration of primary care services provided by different professions using diverse funding sources is challenging. Ireland has implemented a primary care strategy and set up primary care teams to address this. Acknowledging the ageing population in the community, fall prevention needs to be a core function of these services. This study aimed to explore the perceptions of general practitioners, occupational therapists and physiotherapists working in the primary care setting about falls prevention in their practice.
Method
Three general practitioners, five occupational therapists and three physiotherapists were interviewed from primary care teams in the counties of Limerick, Clare and North Tipperary, Ireland. Interviews were in person or by telephone and audiotaped, transcribed and analysed thematically.
Results
Two key themes emerged from the data: the level of primary care team integration and the nature of community fall prevention, linked by referral mechanisms.
Conclusion
Providing comprehensive falls prevention services in the primary care context is complex. Integrated processes and pathways in primary care teams are needed to identify older people at risk of falls and to engage a whole of primary care approach to fall prevention.
Introduction
Primary care refers to the first level of contact for people with the health system which often focuses on the services provided by a local general practitioner (World Health Organization, 1978). Primary health care is a broader concept that includes individual and public health initiatives and services (Muldoon et al., 2006). For the purposes of this study, the term primary care will be used to signify the relationship between general practitioners and allied health professionals in providing services. A strong, accessible primary care service is essential for the management of health needs in the community; however, it is sometimes characterised by complex and fragmented service provision, diversity of funding and variation in the workforce.
In common with other developed countries, Ireland’s population is ageing, and the risk of falling increases with age. For Ireland, the mean prevalence of people over 65 years was 13.5% in 2016 and is predicted to rise to 15.3% by 2021 (National Council on Ageing and Older People, 2004). For the west of Ireland, encompassing County Clare, Limerick County and North Tipperary for the purposes of study, the proportion of the population that is ageing is higher. For instance in County Clare, the proportion of those aged ≥65 years was 14.2% in 2016 and is predicted to rise to 15.8% by 2021, in County Limerick, the 2016 proportion was 14.4% and is predicted to rise to 17.2% by 2021, and in Tipperary North, the 2016 proportion is 16% and is predicted to rise to 18.5% by 2021 (National Council on Ageing and Older People, 2004). For the whole of Ireland, around 7000 older people needed hospital admission after a fall injury (2800 due to hip fracture) each year, and their average length of stay was 12.7 days. The cost of hospitalisations related to fall-related injury among older people is estimated at €59 m (Health Services Executive, 2008). Clearly, there is a need to find ways to address falls prevention prior to an injury, as falls are anticipated to increase as the population ages.
General practitioners are in a key position to identify older people at risk of falls in their everyday practice; however, there are barriers to this (Jones et al., 2011; Kielich et al., 2017) and there are currently no clear models for engaging general practitioners in falls with allied health practitioners at the primary care level (Clemson et al., 2017). Moncada (2011) identified that primary falls prevention involved conducting a multifactorial risk assessment with older people who have not yet had a fall but may have some difficulties with walking, and secondary falls prevention is concerned with older people who have already experienced single or multiple falls and are seeking medical attention. In community-based settings, it is likely that health professionals will be providing both primary and secondary forms of falls prevention interventions. There are several sets of guidelines to help direct primary and secondary falls prevention service delivery in community settings, such as the American Geriatrics Society and British Geriatrics Society (2011) clinical practice guidelines, and the National Institute for Health and Clinical Excellence (2013) guidelines. These guidelines provide direction about falls risk screening, assessment and intervention. Recommendations include asking all older people aged over 65 years if they have had a fall in the previous year, and if they have difficulty walking or with balance. If a fall is reported, a gait and balance assessment should be undertaken such as the Timed Up and Go test (Herman et al., 2011), and a multifactorial risk assessment and individually tailored multifactorial intervention should follow (Moncada, 2011).
In Ireland, primary care is delivered via multi-disciplinary primary care teams, each consisting of general practitioners, nurses and allied health practitioners, with the goal of providing integrated care for the community (Department of Health and Children, 2001; Garvey et al., 2015). Therefore, our research question was: How are general practitioners and allied health practitioners working together in primary care teams to prevent falls amongst older people? The aim of the study was to explore the perceptions of general practitioners, occupational therapists and physiotherapists working in the primary care setting about the management of falls risk in their practice.
Literature review
Primary care requires health professionals to provide integrated and accessible services to address the health needs of the community. To be successful, this involves a coordinated team-based approach, collaborative care, and sustainable partnerships between health professionals, their clients and with other community services. Multifactorial interventions are recommended to prevent falls in the community (Gillespie et al., 2012), and providing these depends on collaboration between a range of health professionals and health care provider organisations in the community (Ganz et al., 2008). The primary care context is where primary falls prevention can take place. However, there are studies indicating that evidence-based interventions to prevent falls, such as balance and strength exercise and home assessment and modification, may not be well integrated into primary care, especially when referrals are needed from general practice (Grant et al., 2015; Kielich et al., 2017). Phelan et al. (2016) further suggest that falls management in primary care is of low quality, with only half of older people with an established falls risk receiving 50% of the recommended assessments within 12 months, and only 24% of home safety and 21% of identified medication risks being addressed, in a retrospective audit of medical records in the United States (US).
One issue is that older people tend not to be asked routinely by their general practitioner or other health professional about falls, and therefore may not be identified as in need of interventions. Even if older people are identified at risk of falls, they may not be offered interventions to prevent falls (Wenger et al., 2003). This may be due to a lack of knowledge of how to address falls (Kielich et al., 2017), a lack of knowledge of what allied health practitioners can offer (Wilson, 2004) or a lack of allied health practitioners to refer to or not being clear who to refer to locally. Even if general practitioners do address falls in their practice, they may not base their falls prevention practice on recognised clinical guidelines (Jones et al., 2011; Kielich et al., 2017). General practitioners also report barriers to undertaking evidence-based care such as lack of time during consultations, other priorities for intervention and few educational materials (Jones et al., 2011; Kielich et al., 2017). These are also barriers to multi-disciplinary collaboration in providing falls prevention services in primary care settings.
Studies have identified the structures and processes that are needed to develop effective multi-disciplinary primary care teams (Belle Brown et al., 2010; Sargeant et al., 2008). These include informal and formal communication opportunities such as meetings or social occasions, structures to enable professionals to understand each other’s roles, developing a common language, sharing care and developing respectful attitudes across the team (Belle Brown et al., 2010; Sargeant et al., 2008). This is in contrast to traditional models of community practice where professionals practice in isolation and roles tend to be more focused on the rehabilitation of individuals (McColl et al., 2009; Tse et al., 2003). Other studies have identified the importance of understanding health professional roles, and the use of electronic medical records accessible by the whole team, to help integrate occupational therapy into primary care teams (Donnelly et al., 2013).
Primary care in Ireland is currently undergoing structural change as local primary care teams are being established. The Irish health care system consists of a mix of public and private funding, and primary health care is free to people who qualify through the Primary Care Reimbursement Scheme (around 35% of the population). Those who are ineligible will pay around €50 per session (Garvey et al., 2015: 3). There are limited published examples of how occupational therapy and physiotherapy falls prevention programs are adapting to the primary care team context in Ireland. The OPTIMAL study was a group self-management program for people with multi-morbidity, led by occupational therapists, which may have included people at risk of falls (Garvey et al., 2015). This program was effective in improving activity participation and self-efficacy, although sustainability of the improvements over time was unknown (Garvey et al., 2015). A Delphi study was conducted amongst primary care physiotherapists working in one Irish province to test the feasibility of a physical activity pathway for implementation in primary care settings, which could also include people at risk of falls (Barrett et al., 2017). This pathway was deemed to be feasible by respondents and recommendations were made for more staff resources and additional training to support the pathway, as well as establishing referral mechanisms from other team members (Barrett et al., 2017). Finally, a national survey of primary care physiotherapy managers in local health offices was conducted to explore the establishment of bone health or falls prevention exercise programs (Madigan et al., 2014). Most programs were implemented relatively recently at the time of the survey, and the key referral source was general practitioners, with some allied health practitioners or other medical specialists. Most programs were group based and generally followed evidence-based guidelines. Barriers reported were lack of staff resources to develop the programs or provide follow-up, lack of transport for older people to venues or inadequate venues (Madigan et al., 2014).
In the absence of studies specifically focused on falls prevention by the primary care team, this study aimed to explore the perceptions of general practitioners, occupational therapists and physiotherapists working in the primary care setting in one area of Ireland, about the management of falls risk in their practice.
Method
As little was known about the practice of general practitioners and allied health professionals in primary care settings, a qualitative descriptive approach was used (Neergaard et al., 2009; Sandelowski, 2000). Ethics approval was granted by the Health Services Executive West Human Research Ethics Committee. All participants gave written informed consent prior to participating in the study.
Participation in the study was voluntary, and recruitment involved purposeful sampling. General practitioners, occupational therapists and physiotherapists from the west of Ireland (County Clare, Limerick and North Tipperary) were invited to participate in the study. There were 33 primary care teams identified in this area. Occupational therapists and physiotherapists were invited via a general email including a consent form, if they supervised occupational therapy and physiotherapy students from the University of Limerick database. This amounted to seven physiotherapists and eight occupational therapists at the time of the study, all of whom worked in different primary care teams (a total of 15 teams out of 33). General practitioners were invited via letter through publicly available contact information. Data from the Irish College of General Practitioners indicated that there were 107 general practitioners in the primary care teams identified. Participants who returned consent forms to the researchers were contacted to arrange an interview, either in person at their workplace or by telephone.
Data were collected through semi-structured, in-depth interviews, which were shared between both authors. An interview schedule using open-ended questions was designed by the authors to encourage participants to elaborate on their responses. The schedule was pre-tested with a physiotherapist and an occupational therapist prior to use, and minor changes were made to the schedule, such as the order of questions and small changes in the choice of words used. Interviews lasted between 20 and 40 minutes. All interviews were audio-taped, and transcribed verbatim. All transcriptions were de-identified by the researcher.
Data were analysed by the first author using thematic analysis. This involved identifying the meanings that emerged from the interviews (Braun and Clarke, 2006). Field diaries were kept by the researchers to record thoughts and reflections after each interview, and at different stages of the data analysis. Data analysis involved reading and re-reading the transcripts to gain an understanding of falls prevention practice from the perspective of the participant. Line-by-line coding of each transcript followed using the NVivo™ program, and then the data were categorised according to emerging patterns and themes. Fully independent consensus coding did not take place, but the second author reviewed the codes and analysis conducted by the first author for accuracy and meaning.
As stated in Neergaard et al. (2009), the following strategies were used to enhance rigour of the analysis: (a) the informants were free to respond however they wished to the questions, (b) sampling was purposeful and flexible, (c) the participants’ voices are heard, (d) their perceptions were accurately described, (e) transcriptions were accurate, and (f) peer review and researcher triangulation took place through discussion between both authors. It was not possible to undertake formal member checking, although debriefing of participants took place immediately after the interviews concluded to gain their reflections on the interview.
Results
Three general practitioners (GP, all male), five occupational therapists (OT, all female) and three physiotherapists (PT, two male and one female) were interviewed. Two main themes emerged from the data: the level of primary care team integration and perceptions about the nature of community fall prevention. These themes are linked by the referral mechanisms that were described by participants (see Figure 1).
Interview themes identified. GP: general practitioner.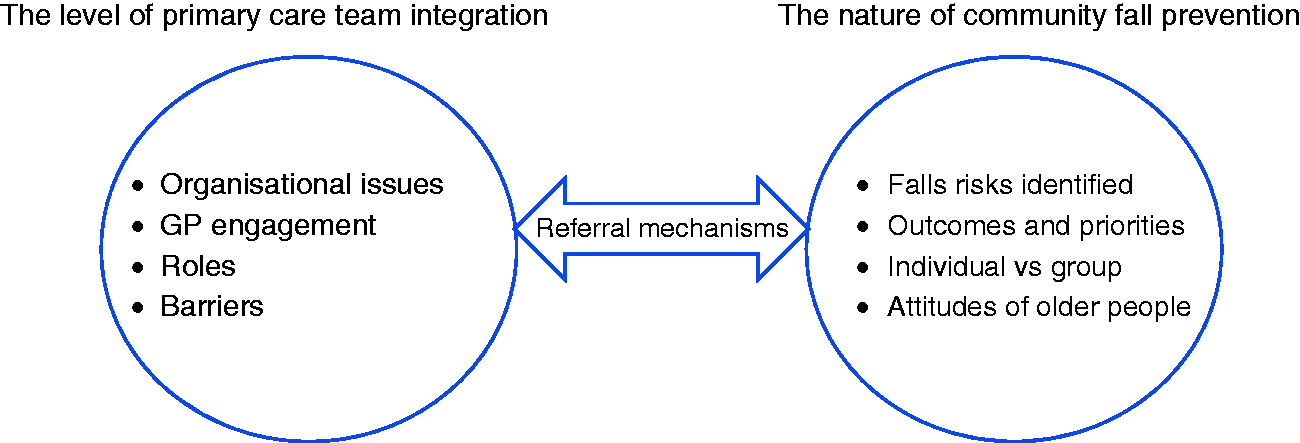
Theme 1: The level of primary care team integration
Organisational issues
Participants described several organisational issues that affected how well they worked as a primary care team. Many of the participants were not co-located with the other members of the team, which made collaboration and communication difficult and promoted a more individual professional approach to falls prevention: No premises for the service is the biggest drawback. Co-location would have been the icing on the cake (PT1). Because there are so many things to do, it takes energy to get up and do something different. But it’s always interesting to…challenge yourself to learn (OT4). We had to be pushed to actually start the clinical meetings. But now you can’t keep us away (GP2).
Access to allied health practitioners was considered insufficient by all three general practitioners who were interviewed, and they described a range of issues relating to allied health practitioners such as poor staffing of allied health practitioner positions and lack of ongoing funding: Initially we were very well resourced, but now they’ve been robbing Peter to pay Paul and if people go off for maternity leave….they’re not replaced (GP2). Well you see the thing is that physiotherapists don’t exist. Occupational therapy is a cloud service….we pray to her for intervention…. You could say you need to see an occupational therapist but it could be a year before you see her – the woman [the patient] could be dead and buried in that year (GP3).
General practitioner engagement with allied health practitioners
The perceptions of allied health practitioners varied about the level of engagement they had with general practitioners. They felt that some general practitioners embraced the services offered by allied health practitioners and others rarely referred or had contact with allied health practitioners. Engagement by general practitioners was believed to be related to the number of referrals that allied health practitioners might receive for falls prevention. Frequently, allied health participants mentioned that they tended to liaise with each other rather than with the general practitioner directly. Some participants suggested that they believed that general practitioners were not always supportive of the primary care team model: I think there’s probably been a little bit of resistance from the general practitioners to be part of the primary care team just because its time consuming with meetings not necessarily with outcomes (OT2). They [general practitioners] seem to be juggling an awful lot by themselves, and that’s come up recently with a few cases, and I think, well I could have looked at that with you (OT1). I think it’s important for us to maybe identify the opportunities that exist that we may not have known existed and also the limitations. Equally that they [other team members] recognise our limitations – we’re only human too (GP2).
Roles
All participants discussed the importance of understanding each other’s roles for the primary care model to work for falls prevention services in the community. Working together enabled different disciplines to gain an appreciation for the whole process of care and how different roles fitted together. Participants recognised that this was dependent on the quality of relationships within the team. Occupational therapists expressed frustrations about how team members perceived their role: I think that probably they [general practitioners] don’t realise the scope of what we do half the time – I think there’s been a history of the equipment providers and that’s all we are (OT5). I had an extremely poor understanding of what an occupational therapist did until I started working with an occupational therapist…like their cognitive assessments and things that I’d never have thought of (GP2). Physiotherapists have gone off on their own tangent and not come back and had mutual discussions….so I’m very disappointed about that to be honest (OT4).
Barriers
Barriers to providing falls prevention interventions were noted by participants in the primary care setting. For general practitioners, falls were not always recognised as a risk for some of their patients: When you’ve got someone who is frail with multiple pathology…often falls mightn’t be the first in your mind…maybe it only comes up when the person has a fall (GP2). If somebody comes in with a good idea, unless it makes my life easier and takes work off me, I cannot co-operate with it because I just don’t have the space (GP2). I found that I had difficulty identifying suitable candidates [for falls prevention programs] – when we make a referral you’re committing yourself to an extra bit of work so you need to be sure there’s a significant benefit to be gained (GP2).
Several participants described the challenges of providing a falls prevention service in a rural area: Our main barriers would be geographic – it is a dispersed population on the west coast of Ireland and the road network is not good and there are a lot of older people living in isolated farmhouses or poor housing conditions (PT3).
Resources to fund home environmental interventions and staff falls prevention services were identified as barriers, as there was no perceived capacity to follow people up and there was little administration support available.
Referral mechanisms
Allied health participants suggested that they did not often get specific referrals for falls prevention interventions, other than for a falls prevention group. Therefore, the onus was on the allied health practitioner to include falls prevention as part of their initial assessment as part of the bigger picture for an older person, and to ask about falls. There was variation in the number of referrals received from general practitioners, and the public health nurse was considered a good source of referrals. The use of a universal referral form or screening tool was discussed by several participants, although the use of a screening tool had to be sensitive to identifying falls risk factors that were amenable to change if a person was being referred. Communication and meetings were essential within the primary care team to generate high-quality referrals that could be acted upon.
Theme 2: Perceptions about the nature of community fall prevention
Falls risks identified
The allied health participants described a comprehensive approach to identifying and intervening with falls risks. Occupational therapists were very much home based, and home visits were emphasised as important to observe how an older person moved around their home and to make appropriate recommendations. This was alongside involvement in falls prevention groups. Physiotherapy participants also visited older people to make an initial assessment or to establish a home exercise program. Again, resources were identified as lacking so that older people had one or two visits and then allied health practitioners ‘hoped for the best’ (PT3), as there was limited capacity for follow-up and supervision.
There was a recognition from the allied health practitioners that interventions needed to go beyond the home environment and exercise, and needed to include: Staying active and looking at different ways to increase confidence…to change their psychology behind it [falls] as well.….. I have to look at their personal safety awareness and their cognition as well…..so it has to be across the board (OT2).
Outcomes and priorities
General practitioners indicated that falls prevention came into the category of chronic and non-life-threatening conditions, so received less of a priority to be addressed. Consequently, they tended to see older people after a fall and this would ‘wake them up’ (GP3) to address potential contributors such as medications. Three of the allied health participants described how their falls prevention programs had ‘‘gone by the wayside’ (OT2) or had ‘been parked’ (OT4), despite initial enthusiasm to embed falls prevention into primary care. This was attributed to health professionals being too busy: People are just so busy that the initial drive has waned somewhat……people aren’t too willing to take on new projects (OT4). People who have been through the falls prevention program are more stable and are more empowered themselves (GP2). You see functional change and I guess that would imply they’ve probably altered their falls risk (PT3).
Individual versus group
The most popular falls prevention intervention offered by allied health professionals was a falls prevention group, which often ran weekly or twice weekly for 8 to 12 weeks. Initial assessments were carried out by different allied health professionals and then groups appeared to consist of an exercise session and an education segment each week, run by several allied health practitioners. Some were more exercise focused than others. The social element of the group appeared to be valued by the attendees who shared their experiences with each other: ….because most of the people involved are about the same age group, from the same parish, they’ve known each other for years, so there’d be great camaraderie between them (GP2). It’s been a bit hit and miss. We’ve had about three [groups] in the area in the last four years – kind of more or less about one a year (GP2).
Perceived attitudes of older people
Participants had mixed views about how they perceived older people accepted falls prevention interventions. Some felt that older people were generally resistant to change, especially with something unfamiliar. Without prolonged engagement with allied health practitioners or any follow-up, they were unlikely to change their behaviour to prevent falls. Making education sessions very practical, trialling recommendations in the home and involving carers and family members seemed to be keys to successful implementation. Others found older people very receptive to falls prevention advice, especially if they had control over changes in the home, and if they had experienced a fall previously. Participants acknowledged aspects of their patients that might make the take up of falls prevention advice more difficult, such as many older people being lonely and depressed, experiencing low activity, being bereaved and experiencing poverty – all contributing to increased social isolation and less mobility. Falls prevention might also not be a high priority for older people: They’re not saying they need to be prevented from falling. We’re deciding…that we’re going to make your life better by preventing you from falling (OT4).
Discussion
This study set out to describe falls prevention management in primary care teams in the west of Ireland. General practitioners, occupational therapists and physiotherapists who are commonly involved in falls prevention interventions provided insight into the primary care environment and how falls prevention services were incorporated into the primary care context. Findings suggest that primary care services are very complex and are subject to similar issues and barriers as those described in other primary care settings outside of Ireland. The west of Ireland is considered a rural area, with 65% of the western region living in rural areas, compared with 37% for Ireland as a whole (Western Development Commission, 2017). It is clear from the findings that participants in this study faced additional pressures to provide equitable access to services, due to distance, the lack of transport options for older people and some clients living in isolated areas or in poor housing. Although falls risk factors may be similar for older people in rural areas, their effect can be greater due to less access to fall prevention programs, more time needed to travel to and from programs, distances and expense involved in travelling and differences in socioeconomic status (Smith et al., 2012). In a study in the USA comparing falls prevention outcomes between urban and rural dwelling participants, rural older people came into the falls prevention program with higher risk scores, and made the most improvement at the end of the program (Smith et al., 2012). This suggests that there may be more need to address falls prevention in rural areas and that the cost–benefit outcome may make increased investment in rural areas more feasible.
The findings did not describe a positive approach to falls prevention, with some participants suggesting that falls prevention was a low-level priority at the primary care level. Although there was an initial commitment from primary health care teams for multi-disciplinary falls prevention interventions, this was not always sustained. Sustainability can be defined as ‘the extent to which successful program components and activities are integrated into the regular activities of community agencies’ (Barnett et al., 2003: 481), and the sustainability capacity of an organisation is defined as ‘existence of structures and processes that allow a program to leverage resources to effectively implement and maintain evidence-based policies and activities.’ (Schell et al., 2013: 2). The findings suggested that although falls prevention components were based on evidence, they were not part of routine practice for many of the participants. Furthermore, structures did not seem to be available to fund primary care teams to fully provide the services needed. Schell et al. (2013) proposed a framework that defined the factors that contribute to a sustainable program. Internal factors involved organisational capacity, program adaptation, program evaluation, communications and strategic planning, and external factors involved effects on public health, funding stability, political support and community partnerships. Study findings identified some limitations with the organisational capacity of the primary care teams and communication within the teams. Findings also suggested that the initial introduction of the new primary care services were well-resourced, but that this level of investment had not been continued. Adequate resourcing and staffing would assist primary care teams to take a more active and sustainable role in falls prevention in the community.
Falls prevention interventions have the potential to unite the skills of many health professionals working in primary care teams, enabling a multi-disciplinary approach to a multifactorial issue. Unfortunately, many study participants appeared to be working primarily in isolation, with little team support. This appeared to have a direct effect on the referral mechanisms in place within the primary care teams. The level of primary care team integration appeared to be ineffective in linking the general practitioners with health professionals possessing skills in falls prevention through referrals made. There also appeared to be a lack of return communication from the allied health professionals to the general practitioners to facilitate more referrals. This underpins the need to enhance communication and collaboration in primary care settings (Belle Brown et al., 2010; Sargeant et al., 2008). Some participants gave examples of how they had come to understand the roles of other team members better, but this was not true of all participants.
Falls prevention interventions described by study participants were predominantly exercise and home assessment and modification. Effective exercise interventions for falls prevention depend on dosage and balance components, and a review of exercise trials indicated the most effective programs included highly challenging balance training, and had higher dosages of exercise (>50 h or > 2 h per week), and included exercise for people at high and lower risk of falls, and group and individual exercise (Sherrington et al., 2008; Sherrington et al., 2011). Given the high incidence of fallers amongst the older population, interventions that require a high level of contact with health professionals may not be feasible in primary care without further funding and staffing. A meta-analysis of randomised trials of environmental interventions (Clemson et al., 2008) found a significant reduction of 21% of falls, with highest effects demonstrated for those at high risk of falls. This supports home safety interventions as a viable and clinically effective fall reduction method if a comprehensive evaluation is conducted using a validated hazard identification tool with adequate follow-up. The lack of follow-up or outcome measurement described by study participants may impair the demonstration of effectiveness of their interventions.
A US review of falls interventions in primary care settings supported (a) multifactorial interventions addressing primary risk factors for falls that were identifiable during clinical evaluation; (b) exercise interventions including gait, balance or functional training (exercises designed to develop dynamic strength, flexibility and agility needed for everyday activities), strength or resistance exercise, and general exercise (including walking, cycling, aerobic activity and endurance exercise); (c) vitamin D supplementation; (d) vision correction; (e) medication assessment and withdrawal; (f) home hazard modification and (g) education or behaviour counselling, but not in isolation (Michael et al., 2010). These interventions are consistent with recommendations in the Irish falls prevention strategy (Health Services Executive, 2008). Although a start has been made, further work will be needed to implement the falls strategy in a consistent way across primary care settings.
Study limitations
This study included the views of 11 health professionals working in primary care setting in the west of Ireland. Therefore, the findings of this study may not be generalisable to all health professionals in all primary care teams. The response rate of general practitioners to the study was particularly low. This is not unusual, as general practitioners frequently do not volunteer for studies that require their time or do not provide them with monetary incentives (Fielding et al., 2005; Pit et al., 2014). Unfortunately, the provision of payment for an interview was beyond the scope of this study. Future studies should consider the use of participant observation or action research methods to gain more insights into the influence of the working environment on the provision of effective falls prevention interventions.
Implications for occupational therapists working in primary care
The occupational therapy participants in this study described a highly variable understanding of their role in primary care by other professionals in the team. To be able to operate beyond the role of provider of equipment, occupational therapists need to consciously take responsibility for educating the team about the breadth of their role (Donnelly et al., 2013). The occupational therapy role in primary care is recognised as going beyond addressing deficits for older people at high risk of falls, but also promoting healthy living and preventing falls in the general population (Metzler et al., 2012). To facilitate appropriate referrals, occupational therapists in primary care teams need to engage effectively with general practitioners who can champion their skills to others (Donnelly et al., 2013). As identified in the study findings, challenges for occupational therapists in communicating with other health professionals in primary care could be ameliorated by co-location, the use of shared electronic medical records, regular meetings and case conferences and having shared goals for older people (Donnelly et al., 2013; Donnelly et al., 2016).
One key aspect of sustaining falls prevention interventions in primary care is to demonstrate the outcomes of the interventions to the rest of the team and to funding bodies. Several study participants did not routinely use standardised tools or outcome measures in their practice. The inconsistent use of standardised tools has been noted in other studies of Irish occupational therapists (Brangan and O’Neill, 1998; Stapleton and McBrearty, 2009), and barriers to their use include time restraints, the utility of tools for use in practice and difficulty reconciling their use with client-centred practice. To show that occupational therapy interventions are effective, the use of outcome measures and recording client data need to be part of routine practice (Unsworth, 2011).
Based on the falls prevention clinical guidelines produced by the American Geriatrics Society and British Geriatrics Society (2011), as well as the National Institute for Health and Clinical Excellence (2013) guidelines, there are some simple, inexpensive actions that all health professionals working in primary care can take to improve the access of older people to falls prevention interventions. Asking every person over the age of 65 years, irrespective of the reason for their referral, about their history of falls over the past year will identify many older people who should have a falls risk assessment. Furthermore, the regular use of a simple test such as the Timed Up and Go test as part of an initial assessment of an older person over the age of 65 would yield important information about their potential risk of falls. Individualised falls risk factors can then be determined followed by an individualised falls intervention program.
Conclusion
Providing comprehensive falls prevention services in the primary care context is a complex task. The routine use of allied health services in fall prevention in primary care settings has been slow, both in Ireland and internationally, which has limited how broadly falls prevention interventions have been applied (Clemson et al., 2017). What is needed are integrated processes and pathways in primary care teams that can identify older people at risk of falls and engage a whole of primary care approach to fall prevention.
Key findings
Participants described lost opportunities to provide effective falls prevention in primary care teams due to staffing needs, time demands and the need for better communication. Multi-disciplinary approaches to falls prevention are variable across primary care teams. Barriers were identified in providing falls prevention services in the primary care context.
What the study has added
This study has revealed that the management of falls prevention interventions in the primary care context is complex and service delivery is often fragmented. The development of individual collegial relationships across discipline boundaries can provide a more integrated service.
Footnotes
Research ethics
Ethical approval was obtained from Health Services Executive West Human Research Ethics Committee, Limerick (6.10, 2010). All participants provided written informed consent to be involved in the research study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.