
Abstract
Introduction
Goal-setting in client-centred occupational therapy is often problematic. The Assessment of Client's Enablement was developed to measure the gap between an occupational therapist's and client's ratings of occupational performance. This study examines the reliability and convergent validity of the assessment.
Method
The assessment was used by 22 occupational therapists with 44 clients. Convergent validity was examined between the assessment (client, occupational therapist and gap scores), Canadian Occupational Performance Measure performance and Functional Independence Measure scores. Test–retest reliability was assessed by intraclass correlation coefficient. Forty-four clients participated in the test–retest reliability study.
Findings
Good-to-moderate correlation was found in the assessment scores (intraclass correlation coefficients of 0.86, 0.95 and 0.78 for client, occupational therapist and gap scores, respectively). The validation study was completed by 34 clients. The correlation between Canadian Occupational Performance Measure and Assessment of Client's Enablement scores was significant (client score, Spearman’s Rank Order Correlation (rs) = 0.47; occupational therapist score, rs = 0.45). The correlation between Functional Independence Measure and the assessment's occupational therapist scores was significant (rs = 0.43).
Conclusion
The study confirms the reliability and convergent validity of the Assessment of Client's Enablement. The assessment requires less time to administer than similar instruments and requires no formal training, making it feasible in rehabilitation settings.
Introduction
Occupational therapy is a client-centred health profession concerned with promoting health and wellbeing through occupation. The primary goal of occupational therapy is to enable people to participate in the activities of everyday life (World Federation of Occupational Therapists, 2012). To practise client-centred occupational therapy, the occupational therapist must collaborate with the client to set goals (Law 1998; Law et al., 1998; Njelesani et al., 2015). During the collaboration process, an occupational therapist must consider the client's occupational issues and understand a client's desires, values, ability, environment and occupation to ensure the development of appropriate solutions and goals.
To facilitate client-centred practice, Law et al. (1998) designed the Canadian Occupational Performance Measure (COPM) to ensure information about all areas of occupation are discussed during the initial interview with a client. Indeed, there is evidence demonstrating that client-centred occupational therapy utilising the COPM leads to better outcomes across all practice contexts: for clients with hand injuries (Che Daud et al., 2016) dementia (Graff et al., 2006), older adults (Dawson et al., 2014), Parkinson's disease (Sturkenboom et al., 2014), stroke (Polatajko et al., 2011) and traumatic brain injury (Dawson et al., 2013). However, Sumsion and Law (2006) noted that throughout the process of collaboration, barriers can exist that result in the client's goals being subsumed by those developed by the practitioner. To overcome these barriers, Njelesani et al. (2015) argue that a key step is for practitioners to reflect and think critically about their client-centred practice to ensure that all the client's occupational issues are considered in practice. In addition, it is important that practitioners identify if there is a gap between a client's and occupational therapist's rating of occupational performance. McColl et al. (2005) argue that if there is a dissonance, or gap between the client's and occupational therapist's perceptions of occupational performance, the resulting dissonance can lead to client disengagement because of dissatisfaction. The gap can occur when either the client or occupational therapist over- or underestimate occupational performance.
This study builds on previous studies that have investigated the gap between a client's subjective perception of their ability and actual occupational performance (Iwai et al., 2011; Goto et al., 2008). Iwai et al. (2011) clarified that the actual activity levels achieved in activities of daily living (ADL; performance ADL) were lower than the potential level that could be achieved with supervision (capability ADL), based on the Functional Independence Measure (FIM). Furthermore, Goto et al. (2008) researched the gap between the client's and the occupational therapist's recognition of the client's performance ADL by also using the COPM performance score. Their results clarified there were significant differences between the client's and the occupational therapist's performance score. In addition, this study demonstrated FIM motor scores had an insignificant correlation to COPM performance scores. They suggested that the cause of the gap was that occupational therapists did not understand the client's perception of their occupational performance. These studies also indicated that practitioners may not correctly understand the capability of clients to independently identify their occupational performance issues. This, along with the other barriers identified by Colquhoun et al. (2017), can contribute to occupational therapists avoiding the use of standardised instruments and so not collecting client-centred outcome measurement data. These studies highlight the importance of developing an instrument that both identifies and reduces the gap between the client and the occupational therapist's perception of occupational performance. Although the Assessment of Awareness of Disability (AAD) and the Assessment of Compared Quality (ACQ) (Anderson et al., 2010; Center for Innovative Occupational Therapy Solutions, 2016a) are assessments for measuring this gap, it is sometimes difficult to use them in a practical setting because they require formal training and are limited to specific tasks.
The Assessment of Client's Enablement (ACE) has been developed to identify the practitioner's and client's perceptions of occupational performance utilising a visual analogue scale (VAS). The hypothesis underpinning the development of the ACE is that if the occupational therapist is aware of a gap, it can be used to facilitate better collaboration with the client in goal-setting and planning interventions. This hypothesis is supported by a pilot case study by Kitahashi et al. (2017), which utilised the ACE. In this study, the use of a VAS identified a gap between the occupational therapist and their client. In the case study, the VAS highlighted that the client did not feel confident and wanted more intervention, despite rating herself with a COPM performance score of 7/10 and satisfaction score of 7/10. Before the ACE, the occupational therapist had thought the client already had enough capability to perform her occupation. With more therapy intervention, the gap scores (the difference between the occupational therapist's and client's perception of performance) of the ACE decreased. However, although the results of this pilot study supported the hypothesis that the ACE has the possibility to improve the corroboration in a clinical setting, the reliability and convergent validity of the ACE score has not been researched.
In this study, we posed the following questions.
Is there test–retest reliability of the ACE client score (ACE-CL), the ACE occupational therapist score (ACE-OT) and ACE gap score (ACE-GAP)? Is there convergent validity of ACE-CL and ACE-OT, assessed by comparing the performance scores with the COPM and FIM?
Method
The reliability and convergent validity studies took place in a rehabilitation setting (subacute stage) in Japan. Before commencement of the research, approval was gained from the Human Ethics Committee of IMS Itabashi Rehabilitation Hospital (no. A008, 11 July 2014).
Participants
A convenience sampling method was used to recruit patients and occupational therapists from the IMS Itabashi Rehabilitation Hospital. Patients who met the inclusion criteria were invited to participate. The inclusion criteria were as follows: participants with Mini-Mental State Examination scores (Folstein et al., 1983) of > 23; not going out, or staying out overnight during the test–retest period (in the reliability study only); and no new incident, or onset of medical conditions during the test–retest period (in the reliability study only). After the recruitment process, 49 people with a physical disability and 22 occupational therapists volunteered to participate in the study. Before data collection, all participants were given written and oral information about the study (joining the study and data usage) and were included after informed consent was obtained.
Description of the instrument
The ACE consists of five bars (see Figure 1). The score is determined by measuring the distance (millimetres) on the 20 cm bar (as seen on a VAS) between the occupational therapist's mark and client's mark on the ‘perform occupation in life’, providing a range of scores from −100 to 100.
Assessment of Client's Enablement scoring sheet.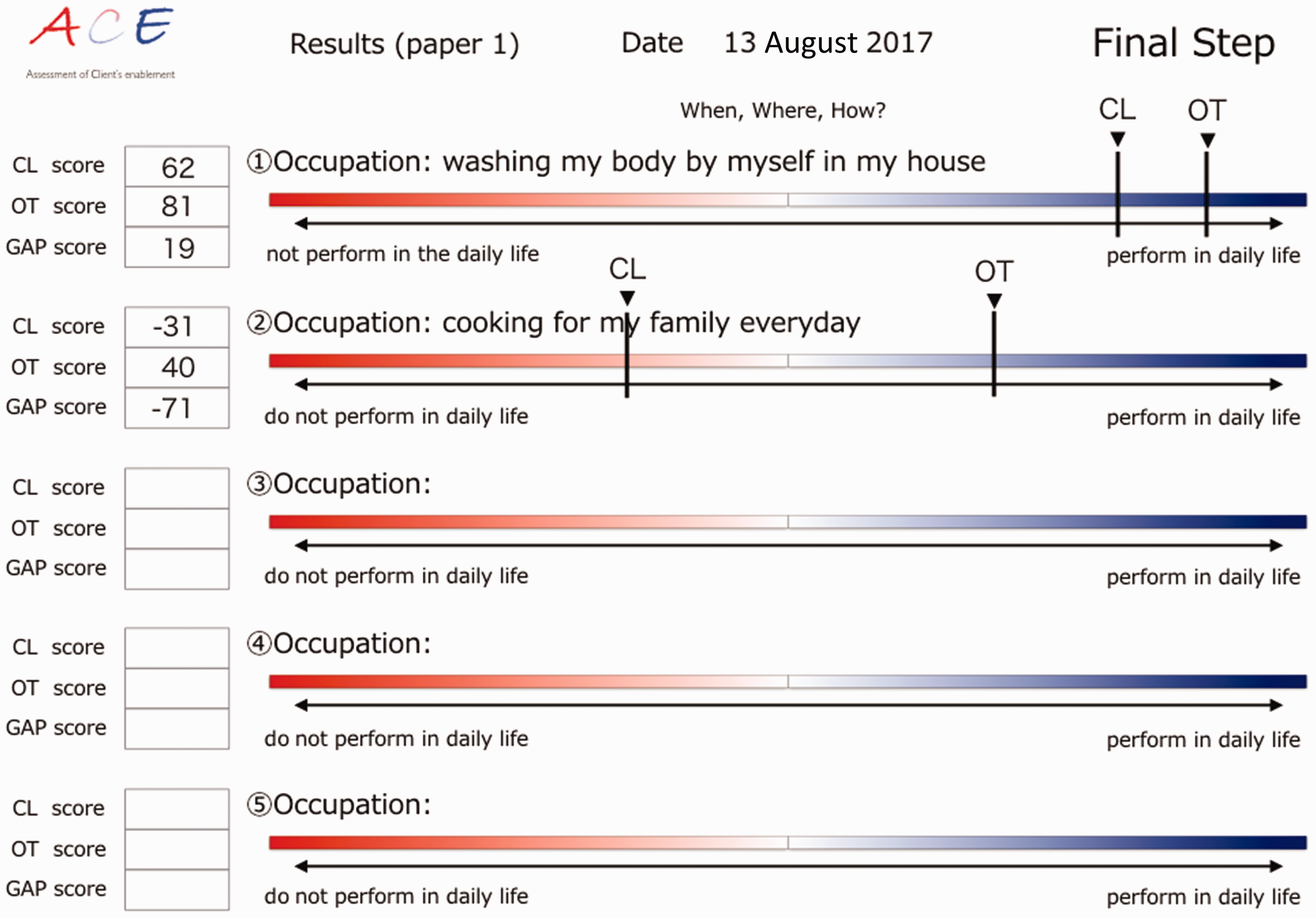
Prior to using the ACE, an occupational therapist would have to identify a client's meaningful occupations through an initial interview such as the COPM, the Aid for Decision-making in Occupation Choice (Tomori et al., 2011) or by informal interview. Occupational therapists must finish the initial interview process before starting the ACE because they have first to correctly understand the client's occupational performance skill and their environment.
The ACE includes the following four steps: (a) the client selects up to five of the most important occupational performance problems during an interview, using a method similar to that proposed in the COPM; (b) the occupational therapist draws a perpendicular line on the visual analogue bar (without showing it to the client), which indicates the degree of performance of the client in each meaningful occupation in their daily life; (c) the client then draws a perpendicular line on the bar regarding their self-assessment of performance in their five meaningful occupations and (d) the occupational therapist shares the result with the client.
The ACE produces three scores: the ACE-CL, the ACE-OT and the ACE-GAP. The ACE-CL and ACE-OT are scored by measuring the distance from the centre line to the client/occupational therapist mark (from −100 mm to + 100 mm). A unit of length is 1 mm. If the mark is on the left of the centre line, the ACE-OT scores the result as a minus. The ACE-GAP is obtained by subtracting the ACE-CL from the ACE-OT.
Reliability and convergent validity
Prior to data collection, the 22 occupational therapists who volunteered to participate in the study were provided with the detailed ACE 12-page manual. The ACE is designed so that no formal training is required. A previous pilot study demonstrated that once familiar with the ACE, it takes an occupational therapist approximately 5 minutes to complete the assessment (Kitahashi et al., 2017).
In the reliability and convergent validity studies the participating clients were evaluated by their occupational therapists, using the COPM (Law et al., 1990, 1998) and the FIM (Ottenbacher et al., 1996). The choice to focus on ADL was because it was considered difficult to investigate the convergent validity of the ACE with the productivity and leisure areas, given that there are limitless occupations that could be chosen as important by clients. In contrast, the ADL identified as important by a client in the COPM are also fully described in the FIM. That is why the FIM was selected for the convergent validity study. In addition, the FIM has been used in similar validity studies of the COPM, comparing its findings with the motor scores on the FIM (Chan and Lee, 1997). Although Chan and Lee used the total number of FIM motor scores, in this study, each FIM motor score was compared with each ADL occupation identified on the COPM.
In addition, the participating clients and their occupational therapist were tested by a researcher (a qualified occupational therapist who was not familiar with the client), using the ACE questions.
Test–retest reliability procedure
The ACE was retested 3 days after the initial assessment. To avoid bias, the initial scores from the ACE were not shown to the participating clients or their occupational therapists until the retest was completed.
The test–retest reliability of the ACE-CL, ACE-OT and ACE-GAP was evaluated using the intraclass correlation coefficient (ICC). The ICC identifies significant differences when p < 0.05. Furthermore, if the ICC is significant between test and retest occasions, ICC ≤ 0.50 indicates poor reliability, ICC = 0.50–0.75 indicates moderate reliability and ICC ≥ 0.75 indicates good reliability (Portney and Watkins, 2000).
Convergent validity procedure
There are a variety of occupations that can be included in goal-setting. It is difficult to examine all occupations in a convergent validity study. Therefore, this research focused only on the client participant's identified ADL issues, which were identified by the client participants with the COPM. Focusing on ADL is appropriate for the study because difficulties with ADL are common occupation performance issues identified by people during the subacute phase of rehabilitation during goal-setting. Convergent validity in the ACE was examined using Spearman's correlation between the FIM score (corresponding with occupational performance problems in COPM), COPM performance score, ACE-CL and ACE-OT. We investigated the convergent validity to test correlation between each FIM item (for example, dressing and eating) and the ACE-CL or ACE-OT (to ascertain if the client's dressing score in FIM items matched the ACE score). This is because the FIM scores have good reliability and validity (Ottenbacher et al., 1996).
Additionally, the minimal detectable change (MDC) is calculated. The MDC means the smallest change can be detected by the instrument beyond measurement error, it is calculated by multiplying the standard error of measurement by 1.96 to correspond to the 95% confidence interval and the square root of 2 to adjust for sampling from two different measurements (Schmitt and di Fabio, 2004).
Results
Reliability study
Participant characteristics.

Test-retest reliability.

ACE: Assessment of Client's Enablement; CL: client score on the ACE; OT: occupational therapist score on the ACE; GAP: gap score on the ACE; ICC: intraclass correlation coefficient. n = 169
p < 0.001.
Validation study
In the reliability study, the 169 occupational issues were identified by the participants using the COPM: these were categorised as self-care (n = 82), productivity (n = 42) and leisure (n = 45). For the validation, the aim was to compare the ACE scores with the FIM; for this reason, 21 of the 82 self-care activities were excluded because they did not match FIM items (for example, the use of public transport). As a result, 61 occupational issues were used in the validation study.
Results of validity.

ACE: Assessment of Client's Enablement; COPM-P: performance score of the Canadian Occupational Performance Measure; CL: client score on the ACE; OT: occupational therapist score on the ACE; FIM: Fundamental Independence Measure; rs: correlation coefficient.
p < 0.001. n = 61
The correlation between the COPM performance score and ACE score was significant (COPM performance score and ACE-CL: Spearman’s Rank Order Correlation (rs) = 0.47, p < 0.001; COPM performance score and ACE-OT: rs = 0.45, p < 0.001; see Table 3). In addition, the correlation between the FIM score and ACE-OT on the ACE was significant (FIM and ACE-OT: rs = 0.43, p < 0.001). ACE-CL on the ACE was insignificantly related to FIM score (FIM and ACE-CL: p > 0.05). The MDC was 69.8; 32.5% of participants were more than MDC and 67.5% were less than MDC.
Discussion
The ACE is an instrument designed to measure the gap between a clinician's and client's perception of their occupational performance. This study examined the ACE's reliability and convergent validity for clients living with physical disabilities.
Reliability and convergent validity
The study showed that for clients with a physical disability the ACE is a reliable and valid instrument. The results demonstrated that the three scores provided by the ACE (the ACE-CL, the ACE-OT and the ACE-GAP) had moderate or good test–retest reliability. The results showed the test–retest ICC was significant at p < 0.001 (see Table 2). Portney and Watkins (2000) argue that this score indicates they were acceptable and had good reliability. In addition, the test–retest ICC scores for the ACE were similar to those found by Pan et al. (2003), who found an ICC of 0.79 and 0.84 for the test–retest of COPM (Law et al., 1998) performance scores. In our study, the higher ICC of the ACE-OT indicates that the occupational therapists were consistent in their objective ratings of client's occupational performance.
This study demonstrated the convergent validity of the ACE for people with physical disabilities, with the ACE-CL and ACE-OT significantly correlated to the COPM performance score. In addition, the results of convergent validity demonstrated that the ACE-OT significantly correlated to the client's FIM, whereas the ACE-CL did not (correlation coefficient of 0.25). However, the FIM measure only records the perspectives of an occupational therapist, so it is viable that this is why the significant correlation was only shown between the ACE-OT and FIM. A previous study demonstrated the validity of COPM by comparing FIM score and COPM performance score (Chan and Lee, 1997). Our methodology is similar to that of their study. Accordingly, our results clarify that the ACE-CL and ACE-OT are valid.
The convergent validity of the ACE-GAP was not tested in this study because there is no comparable assessment that could test convergent validity with the ACE. This is a similar constraint to studies on the validity and reliability of the AAD and ACQ (Anderson et al., 2010; Center for Innovative Occupational Therapy Solutions, 2016a), which were investigated using selected ADL tasks from the Assessment of Motor and Process Skills (Center for Innovative Occupational Therapy Solutions, 2016b).
Clinical utility
This study demonstrates that the ACE is a valid and reliable instrument for the identification of the potential difference (ACE-GAP) between the practitioner's and client's perspectives of occupational performance. The MDC identified is able to record the magnitude of the ACE-GAP. The potential clinical utility of the ACE is that the quantification of this gap can lead to valuable discussions with clients to discuss the potential reasons for differences in perspectives. Njelesani et al. (2015) argue that greater reflexivity is required when working with clients to ensure that all the client's wishes are paramount and are not discounted owing to the practitioner having different values about what requires prioritisation. The ACE provides an additional tool to assist critical reflexivity as it affords an opportunity to gain a greater understanding about the client's perspective about their occupational performance. Although no instrument can overcome the need for critical reflexivity during client-centred practice, the results indicate that the ACE provides a time-efficient instrument to ensure that the client's perspectives are acknowledged.
In addition, the ACE VAS provides a figure to prompt discussion between occupational therapists and their clients during collaborative goal-setting to discuss an identified gap in occupational performance scores. This, in turn, can inform the negotiation of goals and priorities for interventions, which is a key step in the Canadian Practice Process Framework therapy (Townsend and Polatajko, 2007).
The study demonstrates that the ACE provides valid and reliable results and takes approximately 5 minutes to perform. The results also indicate that the ACE can be used by practitioners, including those who are less experienced levels (n = 22, mean age: 25 years) after only reading the 12-page training manual and with no formal training. This is positive when compared with similar instruments that evaluate the discrepancy between a client's and therapist's perception of their performance, such as the AAD and the ACQ (Anderson et al., 2010; Center for Innovative Occupational Therapy Solutions, 2016a). Although the AAD and ACQ are accurate, they require practitioners to be qualified in their assessment protocol, with the AAD interview requiring 5–10 minutes to complete (Kottorp and Petersson, 2011), and the Assessment of Motor and Process Skills (Center for Innovative Occupational Therapy Solutions, 2016b) administration and scoring taking 30–60 minutes (Fisher et al., 1992). Moreover, these assessments also require the occupational therapist to complete an interview prior to completion to identify the client's occupational issues and to undertake the administration and scoring of the Assessment of Motor and Process Skills. These additional components mean that they take longer to complete than the ACE.
Thus, in clinical practice, it is recommended that the ACE be used in conjunction with other instruments that provide objective measurements; however, the need for this additional data will be dependent on the client and practice context.
Limitations and future research
The generalisability of the findings from this study is limited because participants were all from Japan, and it is not known if cultural differences might influence the ACE score. Therefore, further studies of the ACEs cross-cultural validity are needed. Although a previous case-based study (Kitahashi et al., 2017) identified that the ACE can reduce the gap and promote collaboration between a client and an occupational therapist, further research is required into the clinical utility of the ACE in promoting collaboration in the goal-setting process.
Future research is required into the use of the ACE with broader populations and in a range of clinical settings because this study was limited to one facility in Japan and a relatively small sample of clients with physical limitations, reducing occupational performance. In addition, further research is required to understand if a client's condition is correlated with high and low gap scores.
Conclusion
We found that the ACE is a reliable and valid assessment for measuring the gap between an occupational therapist's and a client's ratings of occupational performance, for clients with physical disabilities. The ACE requires less time to administer than similar instruments and does not require formal training, making it feasible in rehabilitation settings. It provides an objective quantification of the differences between client and practitioner evaluation of occupational performance, which can be utilised in collaborative goal-setting. Therefore, it may provide an attractive instrument for occupational therapists who want to enhance their client-centred practice.
Key findings
There was a good-to-moderate correlation in the ACE-OT, ACE-CL and ACE-GAP in test–retest reliability. This study revealed there was convergent validity in the ACE-CL and ACE-OT of the ACE.
What the study has added
The reliability of the ACE is confirmed by test–retest and the convergent validity of the ACE-OT and ACE-CL, clarified by comparing it with the COPM and FIM.
Footnotes
Acknowledgements
We thank all the occupational therapists, patients and caregivers who volunteered to participate in this study. We also thank Bontje P (PhD, OTR), Irishawa K (OTR) and Matsui E (OTR) for their useful advice on drafting this work.
Research ethics
This study was approved by the Ethics Committee of IMS Itabashi Rehabilitation Hospital (no. A008, 11 July 2014), and all participants gave written informed consent to join the study and for their data to be used, after receiving written and oral information on the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was supported by a grant-in-aid from the Japanese Association of Occupational Therapists for Tatsunori Sawada (Grant number 2014-2015 research II).