
Abstract
Introduction
Emotional intelligence competencies assist occupational therapists in responding in a manner that enables them to be effective healthcare practitioners.
Method
This longitudinal study tracked the emotional intelligence of occupational therapy and business students using the Emotional Quotient Inventory 2.0 at three time-points over the final 16 months of their university programme.
Results
Undergraduate occupational therapy students (n = 139 at time-point 1; n = 52 at time-point 3) completed a mean of 117 days of practice education. Before occupational therapy students commenced placements, emotional intelligence scores were significantly lower than population norms in self-regard, self-expression, assertiveness, independence, problem-solving, stress management, stress tolerance and flexibility. By the end of their programme, students reported significant increases in the emotional intelligence realms of total emotional intelligence score, self-perception, decision-making, self-actualisation, emotional self-awareness, independence and reality testing. However, assertiveness, problem-solving and stress tolerance remained relatively low, and other emotional intelligence domains remained below the population norms. The business students who did zero practice placements showed no increase in any emotional intelligence domains over the same period.
Conclusion
Emotional intelligence skills are malleable and can improve during practice placements. Supervisors and employers should encourage students and new graduates to practice their emotional intelligence skills under supervision and then provide feedback, so they are better prepared for the emotional demands of healthcare workplaces.
Introduction
People who experience pain and distress need healthcare professionals, including students undertaking practice education, who can understand their emotional state, can respond with emotional sensitivity and strength and make clinical decisions that takes into account the emotional milieu (Howe, 2008). Tickle-Degnen (1998: 133) purports that the ‘… complexity and requirements of the delivery of occupational therapy services present a challenge to even the most emotionally mature and experienced therapist’. Unfortunately, healthcare programmes in universities currently place a substantial emphasis on the cognitive and skill-based components, including theory and clinical reasoning, with less time spent on developing the emotional and social skills that are also pivotal for the healthcare practitioner to be successful (Parker et al., 2009). Emotional intelligence underpins these demands and is considered a core competency for emerging occupational therapy students to develop and experienced practitioners to use on a daily basis (Gordon-Handler, 2009).
Emotional intelligence is defined as a ‘… set of emotional and social skills that influence the way we perceive and express ourselves, develop and maintain social relationships, cope with challenges and use emotional information in an effective way’ (Stein and Book, 2011: 13). Emotional intelligence allows individuals to identify emotions, decode complex emotional reactions from others, problem-solve (taking into account the emotional milieu) and regulate our own emotions. Healthcare practitioners use emotional intelligence to build rapport, maintain therapeutic relationships, make clinical decisions that need to encompass the emotional milieu and do so when working in a pressured team environment (Howe, 2008). Previous studies show that mature emotional intelligence competencies are positively correlated with reduced stress (McCloughen and Foster, 2017), enhanced caring behaviours (Morales, 2014), increased patient satisfaction (Azimi et al., 2010) and, for healthcare students, better performance in practice placements (Andonian, 2013) and teamwork skills (Brown et al., 2017). With emotional intelligence shown to have multiple benefits for healthcare practitioners and students, further research into emotional intelligence in occupational therapy students is warranted. To date, there has been no longitudinal research on the development of emotional intelligence competencies of occupational therapy students.
Emotional intelligence
Emotional intelligence is well recognised as a realm of human cognitive capability, with emotional intelligence now included as a second-stratum factor of intelligence, similar in importance to fluid intelligence and visual processing (MacCann et al., 2014). A meta-analysis of 395 studies that all included healthcare professionals concluded that emotional intelligence is positively correlated with critical thinking skills and emotional competency (Michelangelo, 2015). Teams with higher emotional intelligence have been shown to have a positive effect on team cohesion and their ability to deal with conflicts (Brown et al., 2017). Similarly, emotional intelligence has been shown to be imperative for graduates who need emotional intelligence skills to be work-ready so they can communicate effectively with colleagues, handle daily stressors, generate and maintain relationships with industry partners and ultimately, make decisions under emotional pressure (Boyatzis and Saatcioglu, 2008). Many occupational therapy graduates aspire to management and leadership roles, with research showing that leaders with higher emotional intelligence skills are often more effective in leadership roles (Zeidner et al., 2010).
Only a few studies have used longitudinal methods to track the changes in emotional intelligence of healthcare students. Health science students have been shown to improve their emotional intelligence and caring abilities between the commencement and completion of their university programme (Larin et al., 2014). More recently, a study tracked changes in emotional intelligence in Australian nursing students (N = 111) over a 3-year period (Foster et al., 2017). The findings showed a significant positive change in emotional intelligence over this period. However, Lewis (2010), who tracked 87 physiotherapy students over 3 years, reported no significant changes in emotional intelligence competencies but did report that students who performed poorly on practice placements tended to have lower emotional intelligence scores. Previous studies have reported that some students in healthcare programmes have high emotional intelligence skills, whereas others have low emotional intelligence skills. A study of nursing students reported that 21% of the cohort (n = 165) had a total emotional intelligence score of <90, which indicated that their emotional intelligence needs ‘required development or required improvement’ (Reemts, 2015). Only 16% of the same cohort had total emotional intelligence scores that were considered in the skilled or expert range. Another study that included nursing students showed similar results, whereby 34% (n = 35) of student participants had scores considered low (Marvos and Hale, 2015). Thus, it is feasible that some occupational therapy students might undertake practice placements with lower than expected emotional intelligence competencies; however, no studies have reported the range of emotional intelligence scores for occupational therapy students.
Practice placements
Occupational therapy students are required to complete a minimum of 1000 hours of practice education during their university programme (World Federation of Occupational Therapists, 2016). Practice placements for occupational therapy students is critical for students to transition from the role of student to entry-level practitioner, build confidence in direct patient care and develop their professional identity (McCloughen and Foster, 2017). During placements, occupational therapy students are required to make clinical decisions for people in emotionally vulnerable situations. For example, during paediatric placements students work with children who are upset and families who are frustrated, during an orthopaedic placement they work with consumers who are in pain and distress and during mental health placements, consumers might be confused or emotionally labile. Occupational therapy students are evaluated during practice placements on a range of practical and communication skills, self-management, clinical reasoning and professional behaviours (Andonian, 2013). To pass a practice placement, occupational therapy students are expected to demonstrate competency in an array of skills and behaviours, many of which require emotional intelligence abilities such as assertiveness, empathy, independence, problem-solving and stress management. Occupational therapy students' emotional intelligence has been reported as a significant predictor of their performance during practice placements; however, their personality traits did not predict performance (Brown et al., 2017). Another study showed that emotional intelligence as well as personality traits are positively correlated with occupational therapy students' performance during practice placements (Andonian, 2013).
Importantly to our study, emotional intelligence has been shown to improve via workplace learning. Workplace learning occurs when a person is immersed in an authentic workplace, such as the practice placements that occupational therapy students undertake throughout their university programme. Emotional intelligence competencies can be improved via workplace learning when a student observes a colleague with high emotional intelligence skills, receives on-the-job mentoring and works in a team environment that uses effective emotional intelligence skills (Brown et al., 2017). Research has also shown that that emotional intelligence is malleable and can be improved in adults (Howe, 2008). Emotional intelligence in adults has been shown to increase over time because of natural emotional maturation (Zeidner et al., 2010). Emotional intelligence scores tend to increase through adulthood but level out in the late 40s (Bar-On, 1997), whereas Multi-Health Systems (2011) reported that emotional intelligence continued to increase well into peoples' 60s. Research has also shown that emotional intelligence can be enhanced through participation in emotional intelligence workshops that focus on specific emotional intelligence skills (Boyatzis and Saatcioglu, 2008).
If workplace learning can improve emotional intelligence skills, then it is feasible that the practice education that occupational therapy students undertake might influence emotional intelligence competencies. Thus, longitudinal research that analyses the baseline and changes in the emotional intelligence competencies of occupational therapy students, both before and during their practice placements, will address an important gap in the literature. The purpose of this study was to track changes in emotional intelligence competencies of occupational therapy students during full-time practice placements over the final stages of their university programme, with a focus on the specific emotional intelligence competencies that improve during full-time practice placements. Understanding when various emotional intelligence competencies tend to mature will be of importance to the occupational therapists who supervise students during practice education placements, university educators and employers of occupational therapy graduates.
Method
Our findings are part of a larger study that used a longitudinal, explanatory sequential mixed methods design. Phase one of the study included occupational therapy, physiotherapy and speech pathology students who completed an online questionnaire to measure emotional intelligence over a 16-month period (Gribble et al., 2017a, 2017b). This article reports the results from only the occupational therapy students. Phase two interviewed 24 of the same students to investigate if, and how, practice education influenced changes in emotional intelligence scores (Gribble et al., 2017c).
Participants
Participants were recruited from a convenience sample of third-year undergraduate occupational therapy students enrolled at three Australian universities and second-year business students from one university. To be included, occupational therapy students needed to be enrolled in the third year of the Bachelor of Science (Occupational Therapy) undergraduate courses and scheduled to participate in three or more full-time practice placements of 4 weeks or more duration in the fourth year of their university programme. Business students (the control group) needed to be enrolled in the second year of a Bachelor of Commerce, majoring in commerce, economics or human resource management. These students were not scheduled to participate in any practice or workplace placements as an obligatory part the university programme. To calculate the number of participants needed to achieve a power of 0.8, the method of Larin et al. (2009) was used. This study used the Emotional Quotient Inventory: Short to measure the change in emotional intelligence scores of physical therapy students (total emotional intelligence change: Mean (M) = 3.5, SD = 9.1). Power calculations indicated that for our study, we should recruit and retain 55 students per group.
All three occupational therapy programmes are 4 years in length and use a constructivist approach to the teaching that includes a combination of lectures, tutorials, case-based learning and online formats. All three programmes scaffold practice placements through the course with part-time, shorter placements (for example, 1 day per week; 1 or 2 week placements) early in the programme, with three or more placements of 6 weeks or more scheduled in the final year. Students in all programmes participate in a range of activities in preparation for placement, including simulation and workshops, as well as debriefing sessions after placements are completed.
A homogenous cohort of business students (similar age and stage of progression through university) was selected, as the control group as business courses generally undertake minimal or no practice placements in workplace settings as a compulsory component of their programme. Entry requirements for all three universities into occupational therapy and business courses in Australia are similar with most undergraduates enrolling directly after completing high school (Health Workforce Australia, 2013). A control group of students from occupational therapy (or another healthcare profession) would have been preferred to business students, but given the compulsory requirement of practice education in healthcare programmes, a cohort of therapy or healthcare students who do no practice placements was not able to be identified.
Potential participants were recruited through email and sent information about the study by a research assistant from each university. A monetary prize was offered as motivation to participate. The Human Research and Ethics Committee at Curtin University approved the study, including the monetary prize, with reciprocal approval being attained from the other two universities. The monetary prize adhered to guidelines stipulated in the National Statement of Ethical Conduct in Human Research (The National Health and Medical Research Council, 2015). Students were provided with Participant Information Sheets and they provided consent at the commencement of the online survey.
Measurement of emotional intelligence
A choice of three theoretical emotional intelligence constructs were considered for this study – ability-based, trait-based and mixed models – each with their own evidence base and measurement tools (Bar-On, 1997; Petrides et al., 2007; Salovey et al., 2004). The emotional intelligence construct selected for this study is the Model of Emotional Intelligence, which is a mixed-model and was created by Bar-On (1997) and subsequently amended by Multi-Health Systems (2011). Mixed models encompass ‘…both abilities and qualities such as personality and motivational traits that assist that person in using EI in real life’ (Zeidner et al., 2010: 26). The Model of Emotional Intelligence encompasses a person's capacity to understand their own emotions, express their emotions, form and maintain interpersonal relationships and ultimately, make decisions that take into account the emotional milieu. All of these are critical skills that occupational therapy students and practitioners require to work effectively with service users and in healthcare teams.
To measure emotional intelligence, Bar-On (1997) created the Emotional Quotient Inventory (EQ-i). In 2011, Multi-Health Systems updated Bar-on's original model and measurement tool and renamed the tool the EQ-i2.0. The EQ-i2.0 is a 133-item self-report tool, thus the instrument does not purport to directly measure the student's actual emotional intelligence ability. Questions include ‘I’m aware of how others feel’ and ‘It's hard for me to share my feelings with others’. Each question is answered on a five-point Likert scale from ‘never/rarely’ through to ‘always/almost always’. The online test takes up to 40 min to complete (Multi-Health Systems, 2011). The EQ-i2.0 calculates 22 standard scores for each participant: a total emotional intelligence score, five composite scores, 15 subscale scores and the wellbeing indicator score. Table 3 shows the facets of the Model of Emotional Intelligence and how each composite scale is derived from three subscales. The standard scores are attained by converting the raw scores for all emotional intelligence domains to scores where the mean is 100 (SD = 15) (Multi-Health Systems, 2011).
The highest score on each domain of the EQ-i2.0 is 135 with a lowest possible score of zero (Multi-Health Systems, 2012). Scores of 110 and above are considered high, normal is the range of 90–109 and scores of 89 and below are considered low (Multi-Health Systems, 2011). The rating system was devised during the normative phase of the EQ-i2.0 instrument, which used 4000 North American participants aged 18 to 60 + years. Test-retest reliability for total emotional intelligence was high (r = 0.92) for participants with 2–4 weeks between tests, and lower (r = 0.81) when tested 8 weeks apart. In order to track changes in emotional intelligence, the EQ-i2.0 manual recommends that participants retake the survey at time-points at least 12 weeks apart (Multi-Health Systems, 2011).
Australian normative data for the EQ-i2.0 were used in this study (Multi-Health Systems, 2012). Norms were based on a sample of 1250 Australians and used the same five age ranges as the original North American normative sample. The sample included participants from across Australia and a variety of education levels. Of interest to our study was that the mean total emotional intelligence for the younger age group of 18–29 year olds (M = 93, SD = 14.3) was significantly lower than older group (50 + years: M = 101.9, SD = 14.2). Internal consistency of the EQ-i 2.0 was very good, as demonstrated by Cronbach's alpha scores of 0.97 for total emotional intelligence , 0.88–0.93 for the composite scales and 0.77–0.93 for the 15 subscales.
Data collection
Data collection occurred via online surveys at three time-points over a 16-month period. Data were collected at the same time-points from occupational therapy and business students. The first surveys were administered before the occupational therapy students commenced their full-time extended practice placements (time-point termed T1). For this study, an extended practice placement is defined as 5 weeks or longer. The online surveys were re-administered (time-point termed T2) 6 months later when the occupational therapy students had completed one or two full-time extended placements. The final data collection was administered after the occupational therapy students had completed all their practice placements at the end of their university programme (time-point termed T3).
At T1, T2 and T3, all students completed an online questionnaire where participants provided consent before providing demographic information that included age, gender, programme, year of study, details of practice placements and any previous emotional intelligence training they had undertaken in the last 5 years. Students were excluded if they had undertaken an emotional intelligence training programme of more than 1 day within the previous 5 years. Participation in an extended emotional intelligence-based training programme has been shown to improve emotional intelligence scores (Boyatzis and Saatcioglu, 2008).
Participants were then directed to the EQ-i2.0 website where they completed the emotional intelligence instrument. EQ-i2.0 scores for each respondent were linked to demographic data via the student's university identification number, with the student's consent. Data were not gathered on whether students passed or failed each placement, as the researchers were concerned that participation rates could decline if students had to disclose a failed placement.
Data analysis
Statistical analyses were performed using the SAS version 9.2 software (SAS Institute Inc., 2008) and a p-value < 0.05 was taken to indicate a statistically significant association in all tests. Comparisons of emotional intelligence scores between the two groups at T1 was conducted using either ANOVA or Kruskal–Wallis tests, depending on the normality of the baseline distributions (tested using the Shapiro–Wilk statistic). The changes in total emotional intelligence, composite and subscales scores from T1 to T3 were then calculated. As the changes in scores were found to be close to normally distributed, a paired t-test was used to identify whether there was a significant change in mean total emotional intelligence score from T1 to T3 for both groups. Instead of performing a number of separate t-tests on the composite and subscales scores, one analysis was performed on the five composites and a second was performed on the 15 subscales (with each composite and subscale being treated as a repeated measurement for each participant, with the type of measure as an independent fixed factor. Because of the repeated measurements on each participant, the participant identifier was treated as a random effect in the model. The results from this model were considered more stable than conducting multiple separate t-tests, as the estimated SD against which all the tests are performed would be obtained from consideration of all the composite and subscales together. With the participant identifier named as the random effect, any correlation between scores obtained from the same participant could be taken in to account. By including an interaction between the score type and the student type, p-values were obtained to identify whether there had been any significant change from T1 to T3 (interaction term significantly different from zero) for each particular student type and composite and subscales combination.
Results
A total of 139 occupational therapy students and 93 business students participated at T1; a response rate of 53% for occupational therapy and 26% for business. Fifty-two occupational therapy and 24 business students completed all parts of the surveys at T3; a retention rate of 37% for occupational therapy and 26% for business. At T1, the mean age of the occupational therapy students was 21 years (SD = 2.7) with only eight students aged 24 years or over as Australian undergraduate courses attract a majority of students directly from school. Business students were 21.4 years (SD = 4.7). The percentage of occupational therapy females to males in the study is similar to the demographics of all Australian occupational therapists, where 91.1% are female (Occupational Therapy Board of Australia, 2017), whereas 76% of business students were female. Five students were excluded from data analysis as they exceeded the EQ-i2.0's inconsistency index, positive impression and negative impression parameters. The times between T1 and T2, and from T2 to T3 were 28 to 36 weeks.
Between T1 and T3, occupational therapy students had completed three or four different practice placements (M = 3.1; SD = 0.9) with a mean length of 117 days (SD = 28), which equates to 88% of the obligatory 1000 hours. Practice placements were mostly full-time (94%) in facilities such as hospitals, private practices, schools and aged care residential facilities. Placements occurred in metropolitan, rural and international locations. Over the same period, business students completed no practice education. During placements, students experienced a range of supervisory models including one-to-one or multiple students with one supervisor, as well as one student being supervised by multiple supervisors.
Regression models comparing the changes from T1 to T3 between occupational therapy and business students.

Mean change in emotional intelligence scores calculated by subtracting T1 from the T3 score. Negative values indicates a decrease in score from T1 to T3.
Instead of performing a number of separate t-tests on the composite and subscales scores, one analysis was performed on the five composites and another on the 15 subscales (with each composite and subscale being treated as a repeated measurement for each participant).
p-value for the change from T1 to T3 (from the regression model).
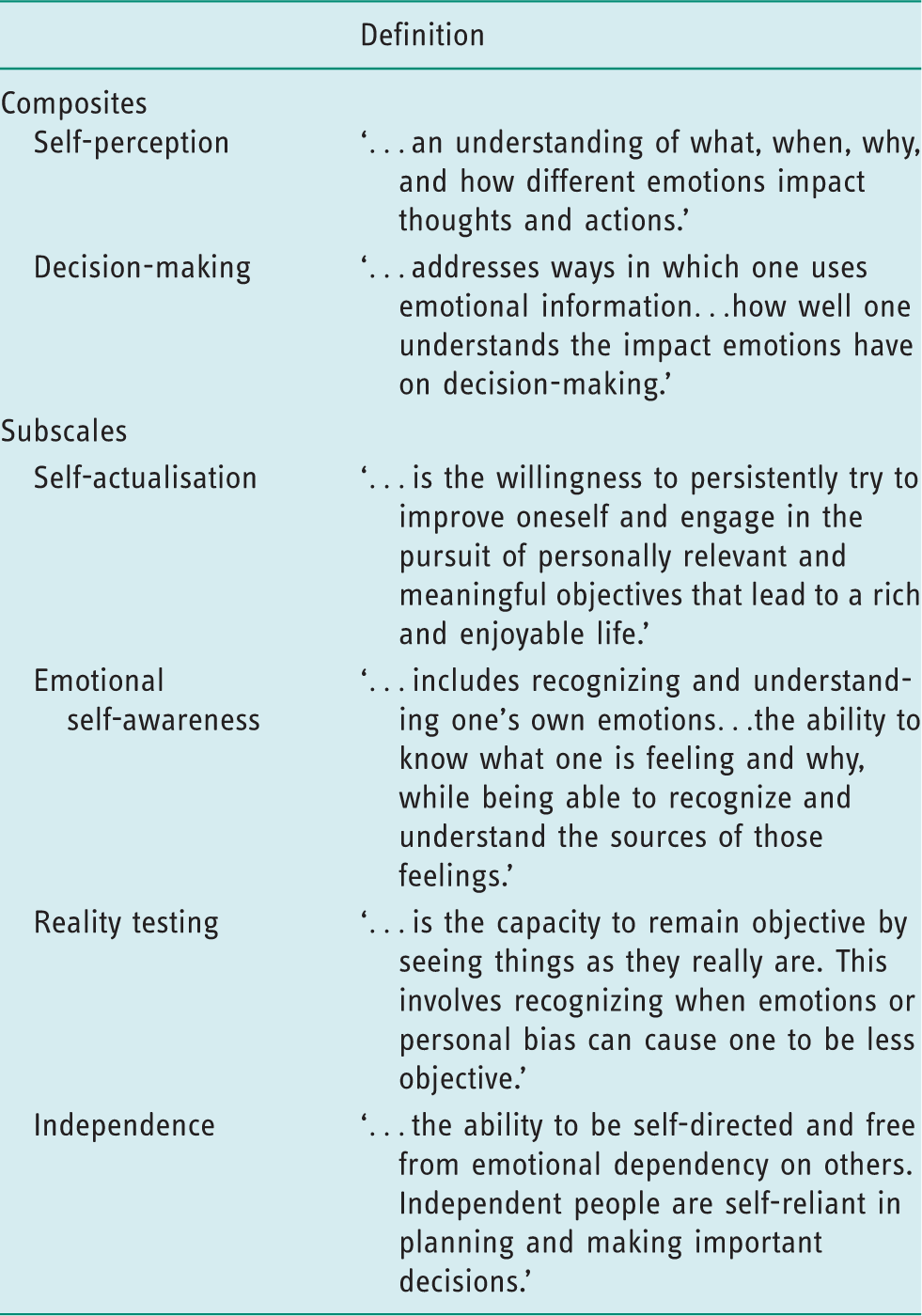
Definitions of emotional intelligence composites and subscales that increased significantly in occupational therapy students (Multi-Health Systems, 2011: 75–78).
Emotional intelligence scores at T1 and T3 for occupational therapy students and comparison to the Australian age-matched (18–29 years old) and population (18–60 + years old) Emotional Quotient Inventory 2.0 norms at T1.
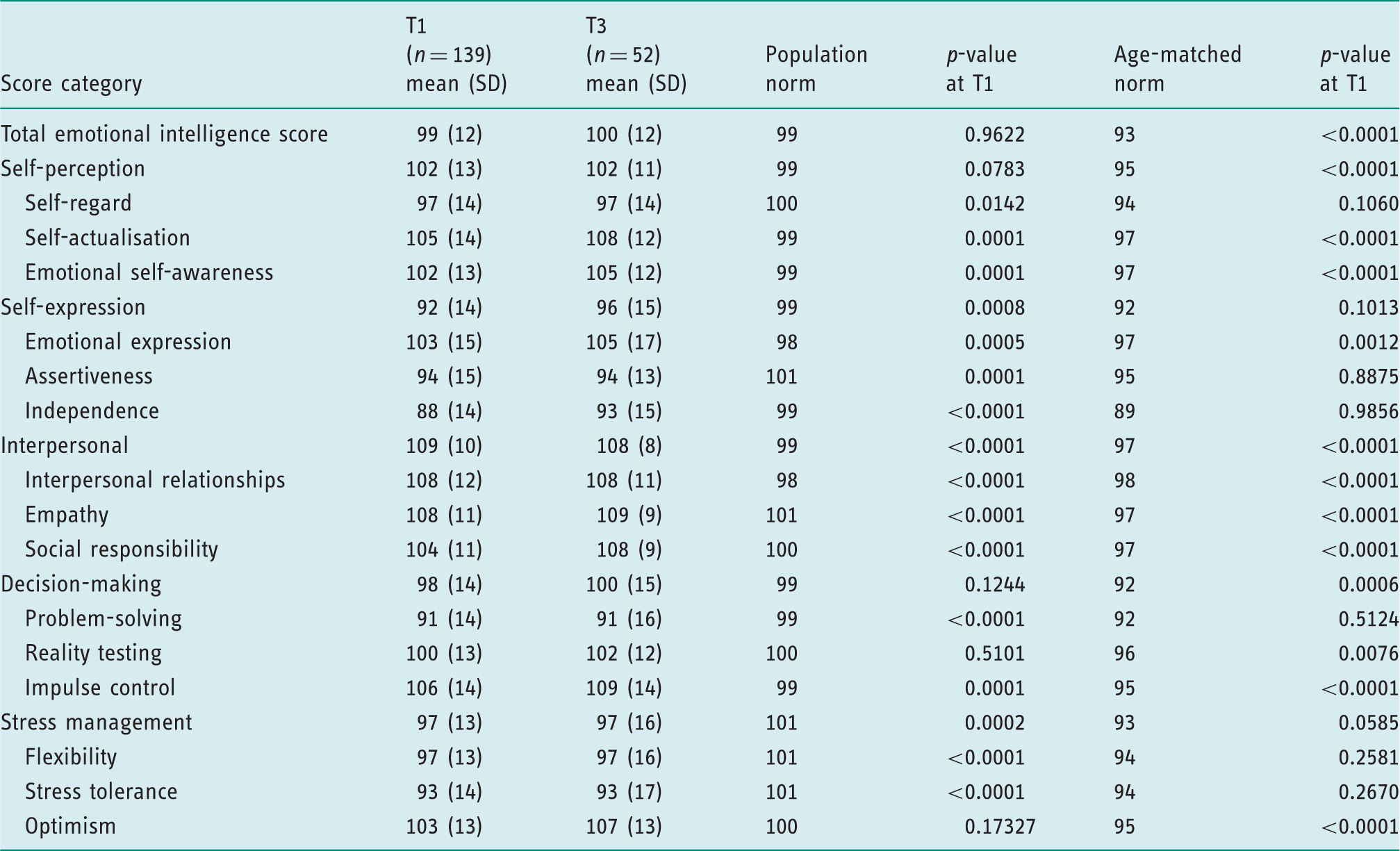
After students completed all their placements (Table 3 shows the T1 and T3 scores of the occupational therapy students), although independence increased significantly, the T3 mean score of 93 is considered in the lower range of normal scores. Other emotional intelligence domains to remain in the lower range of normal scores at T3 were assertiveness, problem-solving and stress tolerance. Emotional intelligence domains at T3 that were in the higher range of normal (where M > 108) were self-actualisation, the Interpersonal Composite and all its subscales and impulse control.
Further analysis compared the occupational therapy students T1 scores to the age-matched and population norms. Table 3 shows the Australian age-matched EQ-i2.0 norms (18–29 year olds, which parallels the mean age of the students in the study) and population EQ-i2.0 norms (18–60 + year olds). No domains for the occupational therapy students were significantly below the Australian age-matched norms. Self-regard, self-expression, assertiveness, independence, problem-solving, stress management and flexibility were similar to the aged-matched norms, with the other 14 emotional intelligence scores being significantly higher than the age-matched norms. The mean emotional intelligence scores of the occupational therapy students were then compared to the Australian population norms. It was important to compare students to the population norms as this is more representative of the healthcare consumers and team members that students work alongside during placements. The emotional intelligence scores that were significantly lower than the Australian population norms were self-regard, self-expression, assertiveness, independence, problem-solving, stress management, stress tolerance and flexibility, whereas self-actualisation, emotional self-awareness, emotional expression, interpersonal relationships, empathy, social responsibility and impulse control were significantly higher.
Discussion and implications
The results of our study show that occupational therapy students' total emotional intelligence score, as well as self-perception, decision-making, self-actualisation, emotional self-awareness, independence and reality testing skills, increased significantly over the final 16 months of their university programme – the same period during which the majority of full-time practice placements occurred. Business students, who completed no practice education, reported no increases in any emotional intelligence scores over the same period. Students were on placements for a mean of 117 days of the 16-month (approximately 480 days) period; thus despite the control group, we cannot conclusively state that the changes in emotional intelligence scores of the occupational therapy students were a direct result of their placements because they were also involved in further teaching at university, paid or volunteer employment, as well as personal life events over the same period. Further qualitative research by (Gribble et al., 2017c) on the development of emotional intelligence in students during practice placement found majority of emotional intelligence changes (95%) were reported to be a direct result of their practice placements, with only 5% perceiving that the emotional intelligence change was due to personal factors external to placements. This study interviewed occupational therapy, physiotherapy and speech pathology students about how practice placements influenced changes in their emotional intelligence. These interview findings add weight to the influence that placements have on emotional intelligence competencies.
Our results align with Clarke (2009), who identified that emotional intelligence competencies can be developed via workplace learning. Our results are also similar to Benson et al. (2012), who tracked the emotional intelligence of 52 nursing students over a 4-year period, reporting that some emotional intelligence domains changed significantly: emotional adaptability, situational coping and flexibility. The improvement in total emotional intelligence and some specific domains during practice education should reassure occupational therapy supervisors and employers because a range of emotional intelligence competencies critical to being an effective therapist matured. During practice education, occupational therapy students have many opportunities to observe their occupational therapy supervisors and other healthcare team members, as they utilise an array of emotional intelligence competencies. Students can then practice the skills, receive feedback from their supervisors and then continue to refine their emotional intelligence abilities.
Before occupational therapy students commence full-time practice placements, 14 of the emotional intelligence competencies were significantly higher than the age-matched norms, including self-actualisation. This finding is not surprising as students in Australia tend to be attracted to university programmes that align with their values and interests (Stagnitti et al., 2010). Similarly, some courses in the UK require students to undergo an interview before being offered a place in an occupational therapy programme, ensuring that the values and level of interest are aligned to the occupational therapy profession. The recent implementation of values-based recruitment in the National Health Service in the UK ensures that employees are recruited with not only with the optimal skills but with values that support effective teamwork and excellent patient care (Health Education England, 2016). The emotional intelligence scores that were significantly lower than the Australian population norms were self-regard, self-expression, assertiveness, independence, problem-solving, stress management, stress tolerance and flexibility, which shows that a range of emotional intelligence competencies are still maturing in some occupational therapy students even at the end of their university programme.
Supervisors of occupational therapy students and university educators need to be aware that some occupational therapy students commence practice placements with some of their emotional intelligence competencies below the population norms, and some are even below age-matched norms. Research shows a positive link between emotional intelligence and performance during practice education (Chew et al., 2013; Lewis, 2010), thus it is feasible that students with lower emotional intelligence scores in our study may perform poorly in scenarios where emotions are at play. This interpretation is supported by Bird and Aukas (1998), who reported that occupational therapy students who fail placements had difficulty with complex and vulnerable healthcare consumers, presented as socially withdrawn and tended to project their problems onto others; difficulties that could be the result of low emotional intelligence competencies.
Employers should be aware that occupational therapy students completed their university course with many emotional intelligence competencies in the normal and even higher ranges of normal. However, assertiveness, problem-solving and stress tolerance remained in the lower range of normal in this study, suggesting that these competencies are still maturing. A student with low assertiveness might be passive in team meetings and lack decisiveness when communicating with patients. Students low in problem-solving may be passive during emotional scenarios and turn to their supervisor or colleagues for strategies to deal with the scenario. Students who experience difficulty during practice placements have been reported to demand additional time from supervisors, therefore students with lower emotional intelligence scores may also require additional support. Employers should support new graduates to develop these emotional intelligence competencies that are critical to being an effective team member, coping with the stressors in the workplace and making decisions under emotional pressure. Research has shown that emotional intelligence can be enhanced through workshops focussed on specific emotional intelligence skills (Boyatzis and Saatcioglu, 2008). With research showing that healthcare professionals with higher emotional intelligence scores achieve better patient outcomes, cope better with stressful scenarios and work well in teams, workshops focussed on upskilling new graduates with lower emotional intelligence scores should be beneficial (Clarke, 2009).
Limitations
The EQ-i2.0 is a self-report tool that measures perceived emotional intelligence competencies in participants instead of actual emotional intelligence ability. Self-report tools have numerous reported limitations, including over- or under-reporting and a tendency for participants to try to provide the optimal answer (Zeidner et al., 2010). There was a notable dropout rate between T1 and T3 in both occupational therapy and business students. This primarily occurred because the T3 data was collected after students had completed their university programmes and had disengaged from university email systems. Consequently, the study may have lacked the power to detect changes from T1 to T3, which increased the chance of a type II error. Being a cohort study means that the T3 sample may be biased toward those who were confident in their emotional intelligence competencies. The use of convenience sampling is also a limitation. This study included only undergraduate students who would be younger than their counterparts in postgraduate occupational therapy programmes, which are commonplace in North America, and therefore results may not be generalisable to post-graduates or older students.
Conclusion
Supervisors and university educators can be reassured that the majority of occupational therapy students will commence their first full-time placements with many emotional intelligence skills well developed, and that total emotional intelligence and some subscale and composite skills tend to improve over the final 16 months of their university programme. The reason for the improvements could be because of the students being immersed in healthcare settings, where they work with consumers in vulnerable situations and communicate within healthcare teams. However, further research is called for that accounts for the changes from the natural maturation of emotional intelligence abilities as well as life experiences external to the practice placements. Although some students commence extended full-time placements with some emotional intelligence skills lower than population norms, at the completion of the university programme, the majority of emotional intelligence skills have matured. Our study raises concerns about assertiveness, problem-solving and stress tolerance, which tend to remain relatively low at the completion of the occupational therapy programme. Supervisors and employers need to encourage students and new graduates to practise their emotional intelligence skills under supervision and then be given feedback and time to reflect, so they are better prepared for the emotional demands of working in healthcare settings.
Key findings
Emotional intelligence is a critical skill for occupational therapy students. Practice placements contribute to improvements in students' emotional intelligence. New graduates may present with many well–matured emotional intelligence competencies; however, assertiveness, problem–solving and stress tolerance remain relatively low.
What the study has added
This study is the first to track longitudinally the emotional intelligence of occupational therapy students over the final 16 months of their university programme, as they undertake full–time practice education placements.
Footnotes
Research ethics
Ethical approval was obtained from Curtin University Human Research Ethics Committee (approval number HR68_2012) on 17 July 2012, with reciprocal approval being attained from the other participating universities. Before the online surveys, participants provided informed consent by checking a box that approved their data to be used for published research. Prior to commencing the interviews, each participant provided written consent for the interview to be recorded and their data to be used for published research.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.