
Abstract
Introduction
Despite clear compatibilities between the tenets of occupational therapy and re-ablement, there is limited research on occupational therapy in homecare reablement services. This article describes an occupational therapy intervention that was delivered as part of a feasibility randomised controlled trial (Occupational Therapy intervention in HomEcare Re-ablement Services), and evaluates whether the intervention was acceptable to participants.
Method
There were three phases: (1) a bespoke pro forma was completed, recording the activities undertaken after each therapy visit; (2) an acceptability questionnaire was sent to every intervention participant and (3) semi-structured interviews were completed with key informants who received the intervention.
Results
The principal activities undertaken were assessment, case management, goal-setting, advice and support, and practising activities in relation to bathing/showering or kitchen activities. Participants particularly valued the advice and support provided. However, there were difficulties due to fluctuations in circumstances and with activities of daily living outside the home within the 6 week timescale.
Conclusion
An intervention focusing on activities of daily living within the home was acceptable for participants and consistent with their goals; however, they also had goals beyond personal activities of daily living and the timescale of the re-ablement episode. Further research should focus on extended activities of daily living, beyond this time-limited period.
Introduction
Re-ablement has been identified as one of the ‘top 10’ prevention interventions for older adults (Allen and Glasby, 2013) and is highlighted within the statutory guidance to support The Care Act 2014 as an example of a tertiary prevention service (Department of Health, 2017). Although the Royal College of Occupational Therapists (2010) argued that the involvement of occupational therapists in re-ablement services is essential to successful outcomes for service users and service providers, there is a dearth of evidence regarding the effectiveness of re-ablement in general (Aspinal et al., 2016), and the specific roles of individual professionals and staff groups within re-ablement services (Pettersson and Iwarsson, 2017). The Social Care Institute for Excellence (2011) stated that comparing the effectiveness and cost-effectiveness of re-ablement teams employing occupational therapists with those that do not was a research priority. To evaluate effectiveness, we conducted a feasibility randomised controlled trial (RCT) of Occupational Therapy in HomEcare Re-ablement Services (OTHERS) (Whitehead et al., 2014). The OTHERS trial aimed to determine the feasibility of randomising re-ablement service users to receive an occupational therapy intervention or usual care, which did not involve routine occupational therapy input. The results showed improvements from baseline in both groups across a range of activities of daily living (ADL) and quality of life outcomes, although overall trends were stronger in the occupational therapy intervention group. We concluded that the RCT was feasible, subject to certain caveats, and these results are reported elsewhere (Whitehead et al., 2016).
Feasibility studies are essential for the future evidence base underpinning occupational therapy; an essential component of such studies is to determine the practicalities of delivering an intervention in the context of a research study (Drummond, 2017). Guidelines from the Medical Research Council highlight the importance of providing a clear description of the intervention alongside the processes involved in delivering it (Craig et al., 2013). Thus, reports of RCTs may be criticised if they provide incomplete descriptions of interventions (Walker et al., 2017). Insufficient description can cause difficulties with replicating that intervention in clinical practice or in further research (Hasson et al., 2012; Hoffmann et al., 2014; Wilkins et al., 2003). Furthermore, in a feasibility study it is important to evaluate whether the intervention itself was viable and practical, such that it could be delivered as intended. It is also important to investigate whether the participants in the study found the intervention to be acceptable. Problems with acceptability often undermine evaluations of interventions (Craig et al., 2013) because the participants may not adhere. It is therefore important to specifically examine acceptability when reporting the findings from an RCT.
The National Audit for Intermediate Care defines re-ablement as being predominantly delivered by social care professionals (NHS England, 2014). It is commonly linked with homecare services and often staffed by former homecare workers who are urged to ‘stand back’ and encourage the user to carry out tasks independently wherever possible (Le Mesurier and Cumella, 1999). The OTHERS trial was conducted within a defined geographical patch of a single-site local authority homecare re-ablement team. The service did not routinely provide input from therapists and was staffed primarily by social care re-ablement workers. For the OTHERS trial, inclusion criterion was the ability to provide informed written consent. Exclusion criteria were inability to speak English, on an end-of-life care pathway, requiring assistance from two or more people to assist with a transfer or receiving input from another community rehabilitation team (such as the community stroke team).
The aim of this article is to provide a detailed description of the content of the occupational therapy intervention that was provided in the OTHERS trial, and to evaluate whether the intervention was acceptable to the participants who received it.
Method
There were three phases to this evaluation of intervention content and acceptability: (1) the activities undertaken by the occupational therapist were recorded with a bespoke pro forma, (2) an acceptability questionnaire was sent to each participant who received the intervention and (3) qualitative interviews were completed with key informants who received the intervention. Ethical approval was obtained from the Social Care Research Ethics Committee (reference number 13/IEC08/002). Data collection was completed in January 2015.
Recording and analysing the content of the intervention
To describe the content of the intervention, a bespoke pro forma was designed to capture and record the visit content and actions undertaken by the occupational therapist. The pro forma was designed with reference to previous studies describing occupational therapists’ interventions within evaluative studies (Grant et al., 2014; Phillips et al., 2010). It covered the following areas: the length of time spent on the visit, the goals set and goals reviewed (achieved, partially achieved or not achieved), and any equipment or minor adaptations provided. Free-text notes on the visits were also completed. Each visit was categorised (in 5-minute intervals) into time spent on the following activities, listed as key intervention components in the published protocol: assessment, goal-setting, goal reviewing, teaching techniques, practising activities and providing advice or generic ‘case management’.
The focus of the intervention was on ADL within the home and this was based on the findings of previous work (Whitehead et al., 2015; Whitehead, 2016). In addition, the overall visit was categorised into the proportion of time spent on specific ADL: indoor mobility, transfers, bathing or showering, strip washing, dressing, kitchen activities, stair mobility, outdoor mobility, toileting, access and any other activities.
The visit pro forma was completed electronically by the occupational therapist immediately after each visit. In addition to the activities completed on the visits (visit content and ADL), information was recorded on the amount of administration and office-based liaison time and travel time. The data were entered into a Microsoft Excel spreadsheet and analysed using Microsoft Excel and Stata (version 13) to produce summary statistics.
Acceptability questionnaire
An acceptability questionnaire was designed by the research team. The design was informed based on a previous acceptability study (Fletcher-Smith, 2011) and was piloted with lay members of the research team. The questionnaire was sent by post to each participant who received the occupational therapy intervention after their discharge from the re-ablement service and at the end of the occupational therapy intervention. The questionnaire was designed to identify experiences of the intervention and asked the following questions:
Do you think the occupational therapist helped you to manage activities more easily? (Response options ranged from not at all to very much so) If yes, specify which particular tasks. Do you think that the number of visits made by the occupational therapist was: too few, about right, too many? Do you think that the time spent on each visit made by the occupational therapist was: not long enough, about right, too long? Overall, how satisfied were you with the occupational therapy treatment you received? (Response options ranged from ‘not at all satisfied’ to ‘extremely satisfied’).
Open-ended questions were included at the end to allow participants to comment freely (Kelley et al., 2003) on any aspect of the intervention. Questionnaires were accompanied by a letter and stamped return envelope from one author (MFW) who was not directly involved in delivering the intervention. If no reply was received within 2 weeks, a second copy was mailed. No further contact attempts were made. Data from completed questionnaires were entered into a Microsoft Excel spreadsheet. Data were analysed using Microsoft Excel and Stata to produce summary statistics.
Key informant interviews
Key informants are people who are identified because of their position and status within the population of interest (Gilchrist and Williams, 1999). The aim was to interview up to five key informants who had received the intervention. They were individuals who, from the occupational therapist’s perspective, had received the intervention as planned and also those where there had been difficulties in delivering the intervention. The aim was to supplement and add depth to the findings from the acceptability questionnaire. The purpose of the interviews was to explore issues related to the acceptability of the intervention in greater detail than in the questionnaire.
Semi-structured interviews were selected to ensure that all relevant areas were covered and so that additional information could be volunteered from participants. A topic guide was developed and adapted from a previous study by Glendinning et al. (2010) in which re-ablement service users were interviewed. The topic guide is available by contacting the corresponding author by email. In addition to general questions about the re-ablement service, particular emphasis was placed on the intervention provided by the occupational therapist, including the particular ADL that the occupational therapist focussed on, how goals were decided or agreed, whether the occupational therapy input helped them to manage activities more easily and in an ideal world, whether there was anything else that the occupational therapist could or should have done.
Interviews were completed by a research assistant who was not otherwise involved in the study or in delivering the intervention. Interviews were audio recorded, transcribed verbatim. They were analysed thematically, using the six-stage process outlined by Braun and Clarke (2006). An inductive data-led approach was used to carry out the analysis and the intention was to be led by the data with a focus on exploring aspects of the intervention that ‘worked well’ and where there had been difficulties. All recordings were listened to several times and each transcript was read several times. Initial notes were made as ideas emerged and particular sections of interest were highlighted for close attention and scrutiny. Data were then coded and all items that were relevant to the topic were given an initial code. Items were grouped together based on the initial codes to form themes. The themes were checked and cross-referenced to the initial coded extracts and then named. This process was conducted by the first author who was the occupational therapist who delivered the intervention.
Results
Thirty participants were included in the OTHERS study, 15 were randomised to receive the intervention. The participant numbers included in the report are the original study ID numbers from OTHERS and range from 1 to 30.
Content of the occupational therapy intervention
Thirteen participants (87%) in the intervention group completed the re-ablement episode and their data were analysed. The median length of the re-ablement episode was 56 days (range: 20 to 126 days). Seventy-one visits were made to the participants by the occupational therapist. The median number of visits was 5 (range: 2 to 13). The total time spent on all visits was 53 hours; therefore, on average each participant received 4 hours occupational therapy contact time. The median visit length was 45 minutes (range: 15 to 90). For every hour of contact time the occupational therapist spent an average of 45 minutes completing office-based tasks, including note writing and liaising with the wider re-ablement team and other health and social care professionals and ordering equipment and adaptations. Some of this liaising related to the research procedures and processes, in addition to the direct occupational therapy component. Each visit involved travel time of 35 minutes on average (return journey). Overall, each participant received an average of 10 hours of occupational therapy time (4 hours direct contact, 3 hours administration and liaison and 3 hours travel time).
A total of 28 goals were set for the 13 participants; the median number of goals set was 2 (range: 1 to 4). Goals were categorised into groups based on ADL. The most common goal was in bathing/showering, with eight participants (62%) having a goal in this area. Six (46%) had a goal in relation to kitchen activities, four (31%) for strip washing and three (23%) for outdoor mobility. Figure 1 shows the total number of goals in each ADL category. In addition, two goals were set in relation to ongoing falls prevention, however, these could not be reviewed within the re-ablement episode as the outcome is a long-term goal. Sixteen goals (57%) were fully achieved by the participants. Nine goals (32%) were partially achieved. The main reasons why goals were partially achieved were that they concerned outdoor mobility and where the participant was not well enough to participate in this or the weather was too inclement. Three goals (11%) were not achieved. Two of these were in relation to the participants’ deterioration in condition, such that they were not well enough to work on the goals. One was in relation to the participant moving to a different property and not being able to work on the goal that had originally been set.
Goals by activities of daily living category.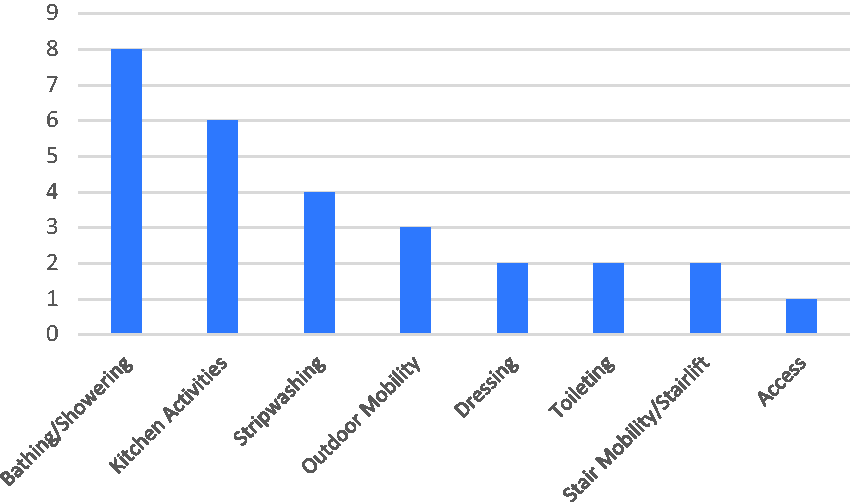
Figure 2 shows the overall content of the visits split into the percentage of the occupational therapist’s time spent on particular activities: assessment, goal-setting, goal reviewing, teaching techniques, practicing activities and general advice. The majority of time was spent on assessment (29%), followed by case management and advice and support (24%), and practicing activities (19%). Considerable time was spent on initial assessment and all participants received this full initial assessment. Some had a low number of subsequent visits following the assessment, which has increased the overall proportion of time spent on assessment. Time not allocated to individual categories was coded as general advice and case management, and this formed a large component of the intervention. Although the latter might seem lengthy, it is consistent with other studies that have reported occupational therapy time use within interventional studies (Phillips et al., 2010; Sackley et al., 2015). Review of equipment and adaptations was coded as practising activities as this involved demonstration of use.
Visit content – overall.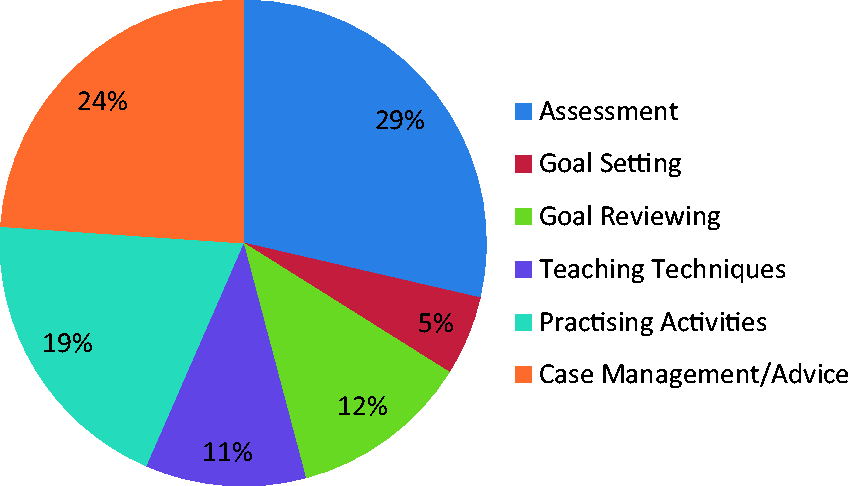
Figure 3 shows the content of the visits categorised in respect of the various ADL activities that were worked on. These ADL categories are consistent with the goals that were set, with bathing and showering being the principal area followed by kitchen activities. ‘Other’ included categories of ADL that were too small to form standalone categories (for example, transfers and pressure care).
Visit content – activities of daily living.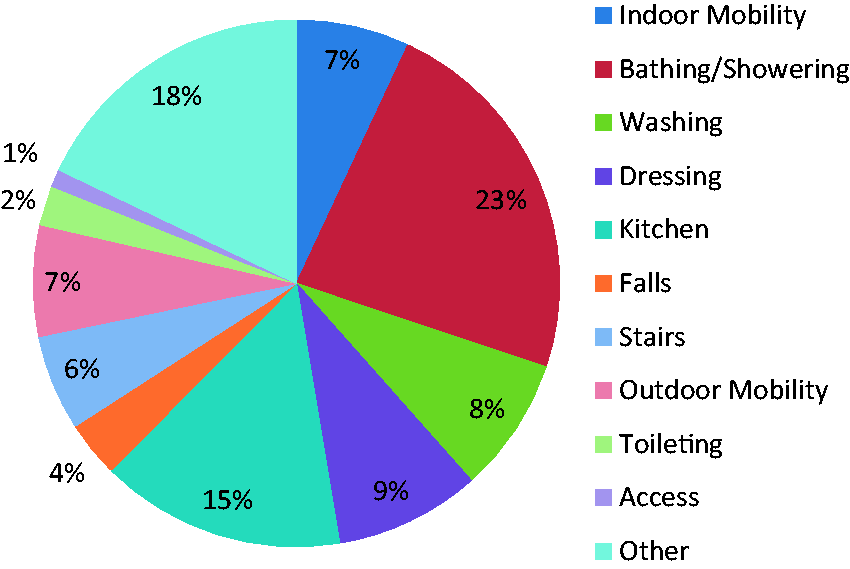
Acceptability questionnaire
Managing to shower myself independently (Participant 08).
Characteristics of questionnaire responders and interviewees.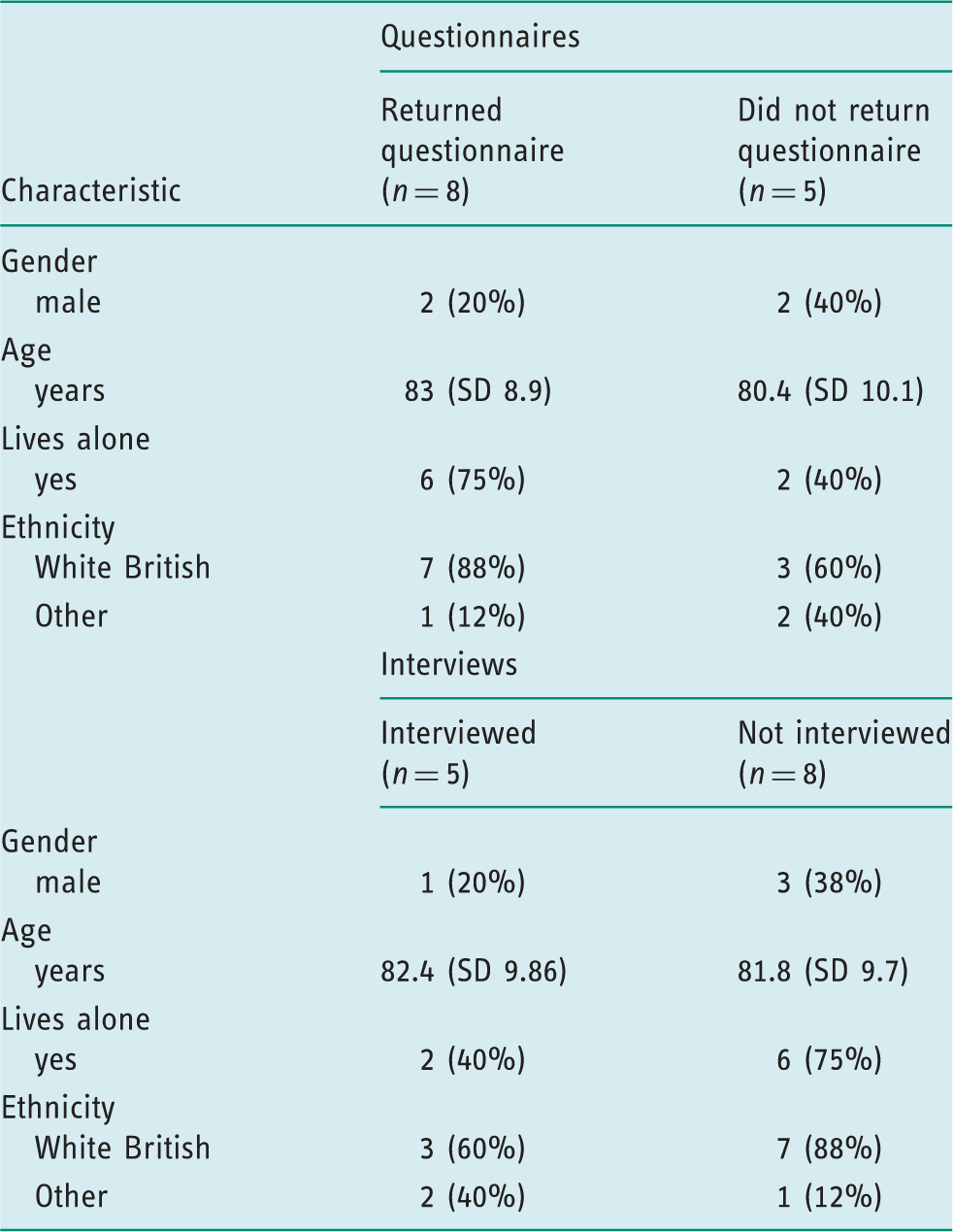
Help with the shower with wall seat fitted and useful tips (Participant 13).
All participants reported being satisfied with the occupational therapy intervention received: four (50%) were ‘satisfied’ and four (50%) were ‘extremely satisfied’. Seven participants (88%) reported that the number of visits made by the occupational therapist was ‘about right’. One reported that the number of visits was ‘too few’; this participant also took part in a qualitative interview in which she clarified that she would have liked the occupational therapy treatment to continue after the re-ablement service had ended. No participants reported there were too many visits. All respondents said that time spent on each visit was ‘about right’. Participants were asked to describe, in free text, the most helpful things that the occupational therapist did. The responses were divided between items that were provided (such as stairlift referral and long-handled sponge) and advice, talking and reassurance. On the whole, the results from the acceptability questionnaire suggest that the occupational therapy intervention was acceptable, and that the respondents believed it helped them to carry out activities independently, with particular reference to personal care activities.Key informant interviews
Five participants from the intervention group were interviewed and their characteristics are shown in Table 1. Two interview participants had poor memory, so they had difficulty recalling specific information as to what happened during the intervention period, therefore the data collected from these interviewees was limited. The interviews ranged in duration from 18 to 49 minutes, with a mean of 32 (SD 12) minutes. The findings have been categorised into four themes: experiencing homecare re-ablement, difficulties encountered with homecare re-ablement, boosting confidence and ability to cope, and extending homecare re-ablement beyond personal ADL.
Theme one: Experiencing homecare reablement
The first theme focussed on the activities assisted with by the occupational therapist and re-ablement team, within a programme that was gradually reduced. Two participants described a programme whereby they were supported to regain independence with showering and kitchen activities and a third participant (with poor memory) partially described a graded dressing intervention. The quotation below illustrates the graded ADL programme that was described for ADL within the home: [the occupational therapist] came and got me a seat put in [the shower]... I had the carers come just to watch me at first, you see, to see how I went on. But... err, it come to a point where I didn’t really need them, so... err, I manage it alright now (Participant 013).
Theme two: Difficulties encountered with homecare re-ablement
Some participants within the intervention group as a whole were too unwell to participate fully in the occupational therapy and re-ablement programme. One participant described being unable to participate because of fatigue and weakness, as the quotation below demonstrates: I was so tired at the time, I didn’t work (Participant 026). Yeah, I was at a very low ebb, not crying all over the place but you know really low, and I’d got to the point where I thought ‘this is it, I’m not bothered, there’s not much going off here’ (Participant 016). [the occupational therapist] come and took me a walk round... We only went ‘round the block, but, erm, you know, I haven’t managed it again on my own, I keep thinking I will do but as I say my arthritis has got worse (Participant 013).
Theme three: Boosting confidence and ability to cope
All five participants spoke about the support, advice and encouragement received by the occupational therapist as being valuable and assisting to boost their confidence to manage activities and/or to cope at home. The mental support and encouraging approach were appreciated and were believed to be key facilitators. In these interviews all the key informants spoke about the advice, support and encouragement that they received from the occupational therapist as being beneficial to them: I can remember [the occupational therapist] explaining and telling me things... at the time it helped me, it helped me... His attitude was that if I wanted to, I could... do, the thing I wanted to. He encouraged me... (Participant 030).
Theme four: Beyond personal ADL
In response to the question, ‘In an ideal world, is there anything else the occupational therapist could have done?’, four of the participants stated that they could not think of any additional actions that would have been needed. They indicated that the time limit of the intervention was appropriate in that they were able to manage independently by the end of the re-ablement episode such that further input was not needed or that their aspiration for further achievements were limited. However, Participant 016, discharged with an ongoing homecare service, stated that continued, ongoing support from the occupational therapist would have been valuable beyond the end of the intervention period. This was to respond to her changing needs and situation, as the quotation below illustrates: Whereas I think with occupational therapy... it could be more valuable than what people or what the authorities or what health people think. I think it could be a lot more valuable to people like myself if we saw OT not just for a certain period of time but... ongoing...my needs might be different. I might need different equipment, I don’t know what I might need (Participant 016).
Discussion and implications
The principal strength of this study is that, to our knowledge, no previous studies have described or evaluated occupational therapy involvement within homecare reablement services. The results from the OTHERS feasibility RCT suggested that there were positive trends associated with the occupational therapy intervention compared with the control group (Whitehead et al., 2016). This article has provided additional detail on the content of the occupational therapy intervention and evaluated participants views and experiences of it.
The main activities prioritised by participants were personal ADL (bathing, showering and strip washing) and kitchen activities. The focus on these activities worked particularly well and participants reported that they valued the combination of equipment/adaptation provision, the graded approach and the mental support that facilitated confidence boosting and their ability to cope. It is possible that these activities were prioritised by participants as these were inextricably linked with the need for an ongoing homecare service, that is, these were the activities that that homecare workers would have provided on a continuing basis after the re-ablement episode had ended. In order to resume independent living, participants had to regain independence with ADL within the home. By the time these goals had been achieved, the re-ablement service was coming to an end, which meant that there was insufficient time to focus on additional or extended ADL goals
Although overall the intervention worked well and was acceptable, there were aspects that were difficult. Participants’ fluctuating physical and mental health affected their ability to participate, particularly following the initial event that had led to the need for the service. Furthermore, three participants had an outdoor mobility goal, emphasising the importance of outdoor mobility and community access to the participants. However, there were difficulties in achieving these goals with all participants due to fluctuations in their health conditions or inclement weather. Although they prioritised ADL within the home, they were left with ongoing, concurrent goals in relation to ADL outside the home, which could not be addressed within the timescale of the re-ablement episode.
Findings from the interviews suggested that a further review or reviews, by an occupational therapist, after people have been discharged from the re-ablement service might assist with the maintenance of people’s independence at home and promote further progress. The recent National Institute for Health and Care Excellence Guideline for Intermediate Care including Re-ablement has made a research recommendation for further studies to evaluate the effectiveness of reablement beyond 6 weeks (National Institute for Health and Care Excellence, 2017), and this is consistent with our findings from the interviews. The Guideline also states that ‘Social and leisure goals should be legitimate goals of an Intermediate Care [including re-ablement] service’. However, this study identified practical issues in delivering such goals within the context of a short-term re-ablement episode that was tied to a homecare service in which there was a prevailing focus on ADL within the home.
Notwithstanding the clear and obvious compatibilities between the tenets of occupational therapy practice and re-ablement services, there is limited empirical research on occupational therapy in re-ablement. This study provides additional detailed information on the content of an occupational therapy intervention and the perspectives of the people who received it. It highlights that, although occupational therapists and re-ablement service users may consider wider holistic goals and needs, there are often practical considerations and time constraints that affect what can be achieved within the confines of a re-ablement episode.
There are some limitations to this study. The majority of data collection and analysis was completed by one occupational therapist who delivered the intervention in the RCT. This means that there was a possibility for bias. However, this was minimised where possible, by having another researcher conduct the interviews and receive the returned questionnaires (not the treating occupational therapist directly). Although the findings from the acceptability of the intervention were unequivocally positive, they were based on 62% of intervention participants and the sample was small. Although there is no reason to indicate that these respondents were not representative of the intervention participant group, it is important to note that the data do not represent the complete sample.
Conclusion
We found that it was possible to deliver a graded ADL programme within the home, particularly focusing on personal care and kitchen activities, for the majority of participants in a way that was acceptable to them. Participants valued the intervention and appreciated the support, advice and confidence building provided by the occupational therapist. There were, however, some difficulties in delivering the intervention as planned, which were primarily due to the vulnerable and fragile nature of the group. Where participants had goals in relation to activities outside the home, it was difficult to incorporate these within the timescales of the re-ablement service. Occupational therapists should also consider research on outdoor mobility and wider community participation as part of re-ablement services; this would be consistent with the wishes and person-centred goals of the participants in this study. It might be pertinent to focus on extended ADL, including social, leisure and outdoor mobility, at a later stage, which should be explored by further research.
Key findings
An intervention focusing on ADL within the home was acceptable, although some participants also had extended ADL goals, which could not be achieved in the timescale. Participants particularly valued the advice, support and reassurance provided by the occupational therapist. Further research focussing beyond ADL within the home and a 6 week time period is warranted.
What the study has added
This study has provided a detailed description of the content and analysis of the acceptability of an occupational therapy intervention in homecare re-ablement. Although the intervention was acceptable to participants, an additional focus beyond 6 weeks and on activities outside the home is warranted.
Footnotes
Acknowledgements
The authors would like to thank the following for their assistance in conducting this research: the project steering group, consisting of Professor Jill Manthorpe (chair), Stuart Belshaw, Dr Adam Gordon, Zaid Latif, Ian McGeorge, Joanne Martinsons and Rachel Mellor; the participants and their families; Nottingham City Council and particularly the occupational therapy and Intake Re-ablement teams; and Dr Clare Mann for her assistance with the data collection.
Research ethics
Ethical approval was obtained from the Social Care Research Ethics Committee (reference number 13/IEC08/002). All participants provided written informed consent to be interviewed for, and have their anonymised data used in the research study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article is independent research supported by the National Institute for Health Research (doctoral research fellowship, DRF-2012-05-131). The views expressed are those of the authors and not necessarily those of the National Health Service, the National Institute for Health Research or the Department of Health.