
Abstract
Introduction
Little is known about long-term work sustainability of stroke survivors. A feasibility trial of early stroke specialist vocational rehabilitation had 32/46 (69.5%) participants available for follow-up at 12 months post stroke. Of these, 19/32 (59.4%) were in work. This study aims to determine the feasibility of longer-term follow-up and explore work status 6 years post stroke.
Method
Forty-eight participants fitting criteria for the feasibility trial were sent postal questionnaires measuring employment, income, mood, functional ability and quality of life, and were invited for interview to explore working 6 years after stroke. Ethical approval was obtained.
Results
Of the 48 participants, five (10.4%) had died; 19/43 (44.2%) responded. Fourteen were men; mean age 62 (24–78) years. Fourteen (74%) reported working (paid work n = 10, voluntary work n = 3, full-time education n = 1). Five had retired. Most (11/13) remained with preinjury employers. Half (8/15, 53%) reported decreased income since stroke. Compared to one year, median functional ability was marginally higher (extended activities of daily living 63 (IQR 8, range 32–66) to 60 (IQR 9, range 17–66)), but health-related quality of life was lower (EuroQuol Visual Analogue Scale mean 77.4 [SD 11] to 70.7 [SD14]). Six interviewees felt returning to work was the correct decision but struggled with invisible impairments.
Conclusion
This study suggests that long-term follow-up is feasible and that those who made a good recovery were more likely to respond. Work remains important to stroke survivors 6 years post stroke.
Keywords
Introduction
In the United Kingdom (UK), in excess of 100,000 people have a stroke each year (Stroke Association, 2018). Approximately 25% are under 65 years old (Daniel et al., 2009), yet reported return to work (RTW) rates in systematic reviews vary from 7–81% (Baldwin and Brusco, 2011; Wei et al., 2016). Lost UK productivity resulting from stroke is estimated at £1.6 billion per year (Patel et al., 2017). Supporting stroke survivors in RTW could reduce the personal financial and UK economic burden.
The UK government recognises that ‘good’ work has a positive impact on a person’s health and economic status and wants health care services to provide help at the right time to facilitate more people with long-term conditions such as stroke to return to and remain in work (Department for Work & Pensions and Department of Health, 2017). Vocational rehabilitation (VR) is defined as ‘whatever helps someone with a health problem to stay at, return to and remain in work’ (Waddell et al., 2008: 5). Although national guidelines for stroke recommend that the work needs of stroke survivors should be addressed, they also highlight the absence of evidence for the effectiveness of vocational rehabilitation (National Institute for Health and Care Excellence, 2013; Royal College of Physicians, 2016). As few as 15% of the UK’s post-acute services support RTW after stroke (Royal College of Physicians, 2015). Even less is known about longer-term work sustainability. In a survey of unmet need among 1251 community-dwelling stroke survivors, 52% reported a reduction in work activities and 18% reported reduced income 1–5 years post stroke (McKevitt et al., 2011).
Literature review
Stroke severity, greater independence on hospital discharge, younger age, male sex, higher educational level, white collar work, the ability to walk and having preserved cognition have all been shown to increase a person’s chances of RTW (Larsen et al., 2016; Vestling et al., 2003; Wang et al., 2014; Westerlind et al., 2017). Few quantitative studies have examined longer-term work status. Westerlind et al. (2017) followed up 211 participants (18–63 years), 6 years after stroke, using stroke register data and postal questionnaires. The postal response rate was 47% (76/162). The mean age at stroke onset was 53 years. Excluding 37 participants who had retired early, at 6 years 130 (75%) people were working, 10 (6%) had retired due to age, 10 (6%) had died before retirement and 24 (14%) were living on disability benefits. Interestingly, RTW rates continued to increase up to three years post stroke. However, it was unclear whether participants had returned to the same job or the same working hours.
Two qualitative meta-syntheses of barriers and facilitators to RTW after stroke (Brannigan et al., 2017; Schwarz et al., 2017) identified the same 11 studies. They included participants who had and had not returned to work in follow-up periods varying from a few months to nine years. Both meta-syntheses stressed the importance of the initial RTW experience and recommended a ‘dedicated person’ to help facilitate the transition between the hospital, community and the workplace. Both suggested that education by health care professionals was necessary in the community and workplace to ensure that all parties were aware of the stroke survivors’ limitations and abilities.
A UK single centre feasibility randomised controlled trial (fRCT) of an early-stroke-specific vocational rehabilitation intervention recruited 46 trial and two case study participants in 2011/2012 (Grant et al., 2014; Radford et al., 2013). Twenty-five participants had access to an occupational therapist specialising in VR in addition to their usual National Health Service (NHS) rehabilitation (usual care) for up to one year immediately post stroke, and 23 participants received usual care alone. The intervention aimed to support a return to work where possible. At one year, 19/32 (59.4%) respondents were in work or education. However, the feasibility of longer-term follow-up and work status is not known.
Aim
To determine the feasibility of a prospective six-year follow-up after stroke onset. To ascertain at 6 years after stroke:
The proportion of people in work and the proportion living solely on welfare benefits. Participants’ levels of anxiety, depression and health-related quality of life. Participants’ use of health and social care resources. To identify and explore factors affecting long-term work outcomes from the perspective of stroke survivors who were working before stroke onset.
Method
A mixed methods study using both quantitative data gained from a questionnaire survey and in-depth qualitative data from interviews was chosen to ascertain feasibility of follow-up, post-stroke work status and to gain an in-depth understanding of factors affecting work status 6 years post stroke. In 2017, the lead Stroke Clinician screened survivors admitted with stroke to a UK NHS hospital between July 2010 and December 2011. Eligibility criteria for participation matched that of the earlier feasibility trial: aged 16 and over, admitted with new stroke, and in work or full-time education at the time of stroke onset and intending to return. Work was defined as participating in competitive employment, supported work, vocational training or voluntary work for at least one hour per week or full-time education. Hospital records were checked for known deaths. Participants were sent a study pack consisting of an information sheet explaining the study, an invitation for respondents to participate in a telephone interview to explore their experiences of working or not 6 years post stroke, and a questionnaire and consent form. As participants in the earlier study were not asked to consent to later follow-up, they could not be approached directly by the research team. Envelopes returned marked ‘not known at this address’ were checked by the lead clinician. Participants with a known change of address were sent the information pack. Non-respondents were resent the information pack.
Questionnaire survey
The questionnaire was the same as that used in the feasibility randomised trial (Grant, 2016). This included demographic information, and bespoke employment, resource use and benefit status questions. The questions were originally generated in conjunction with stroke survivors, specialist stroke occupational therapists, stroke researchers and a health economist. The questionnaire also included standardised measures of activities of daily living, mood and health-related quality of life. The Nottingham Extended Activities of Daily Living scale (NEADL) (Nouri and Lincoln, 1987) was developed specifically for stroke patients. Validation studies have shown it to be responsive in measuring change in a stroke population (Lin et al., 2011; Wu et al., 2011). The Hospital Anxiety and Depression Scale (HADS) (Zigmond and Snaith, 1983) has been shown to be an accurate measure of depression and anxiety post stroke (Aben et al., 2002). HADS scores were classified as 8–10: mild; 11–14: moderate; 15–21: severe depression or anxiety present (Stern, 2014). Health-related quality of life (HRQOL) measured using the Euroquol 5d-3L (EQ5d-3L) (Brooks, 1996) and NOT EQ-5D-3L (Dolan et al., 1995) was found to be a reliable and responsive measure of HRQOL post stroke (Dorman et al., 1997). Retirement was classified as retired due to ‘age’, due to ‘health’ reasons or any ‘other’ reasons to give a clearer picture of the effect of stroke on work status.
Interviews
The semi-structured telephone interview questions were informed by two theoretical frameworks: The Work Disability Paradigm (Loisel et al., 2001) and the International Classification of Function (World Health Organization, 2011). Interviews were conducted, recorded and transcribed by an independent researcher blinded to allocation in the original fRCT. After checking transcripts for accuracy, transcripts were manually coded and themes identified by codes (KG) (Braun and Clarke, 2006). Themes were independently ratified by a second researcher who read all the transcripts (JP). Further analysis reduced and refined themes through the creation of sub-themes which were agreed by the research team. Themes were identified at a semantic level. Participants did not provide feedback on the transcripts or findings.
Analysis
Quantitative data was recorded and analysed using descriptive statistics: Excel 2010 and SPSS 23. As this was a small feasibility study, tests for statistical significance were not applied. One-year and six-year data were compared where feasible.
Results
Forty-eight eligible participants were identified, all of whom were participants in the earlier trial. Of these, five (10.4%) had died; eight (16.6%) envelopes were returned ‘not known at this address’ and 16 (39.6%) did not respond. Total response rate was 19/48 (39.6%). Excluding participants who had died, the response rate was 19/43 (44.2%) – see Figure 1. As the numbers of participants in each arm of the fRCT were too few to draw meaningful between-group comparisons, only the overall results are reported. Most participants responded following the first mail shot (n = 16). Four envelopes returned ‘not known at this address’ after the first mailing had addresses rechecked and three addresses were changed. Three participants who were lost to follow-up at 1 year responded at 6 years.
Flow diagram.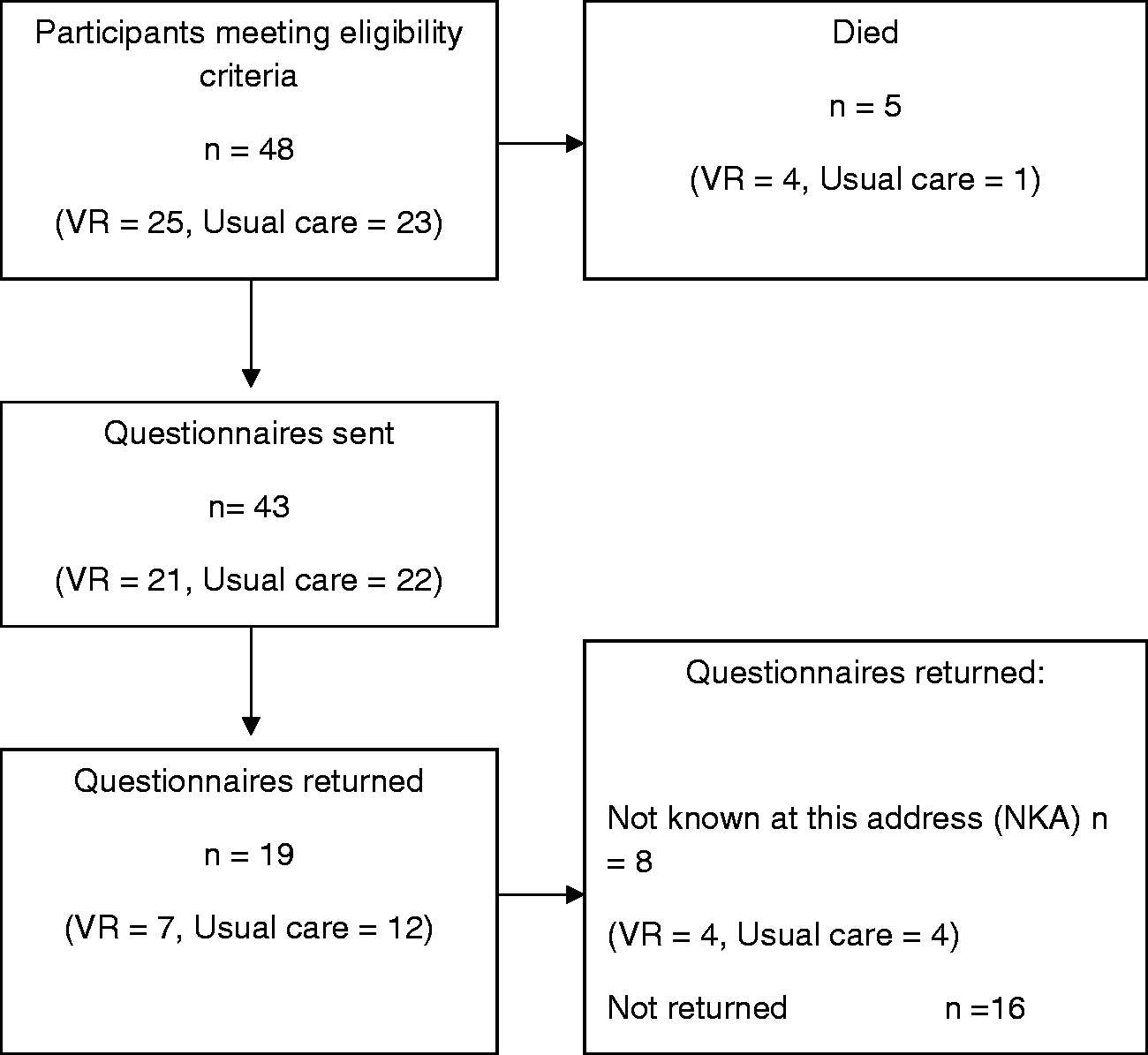
Participants
Participants.
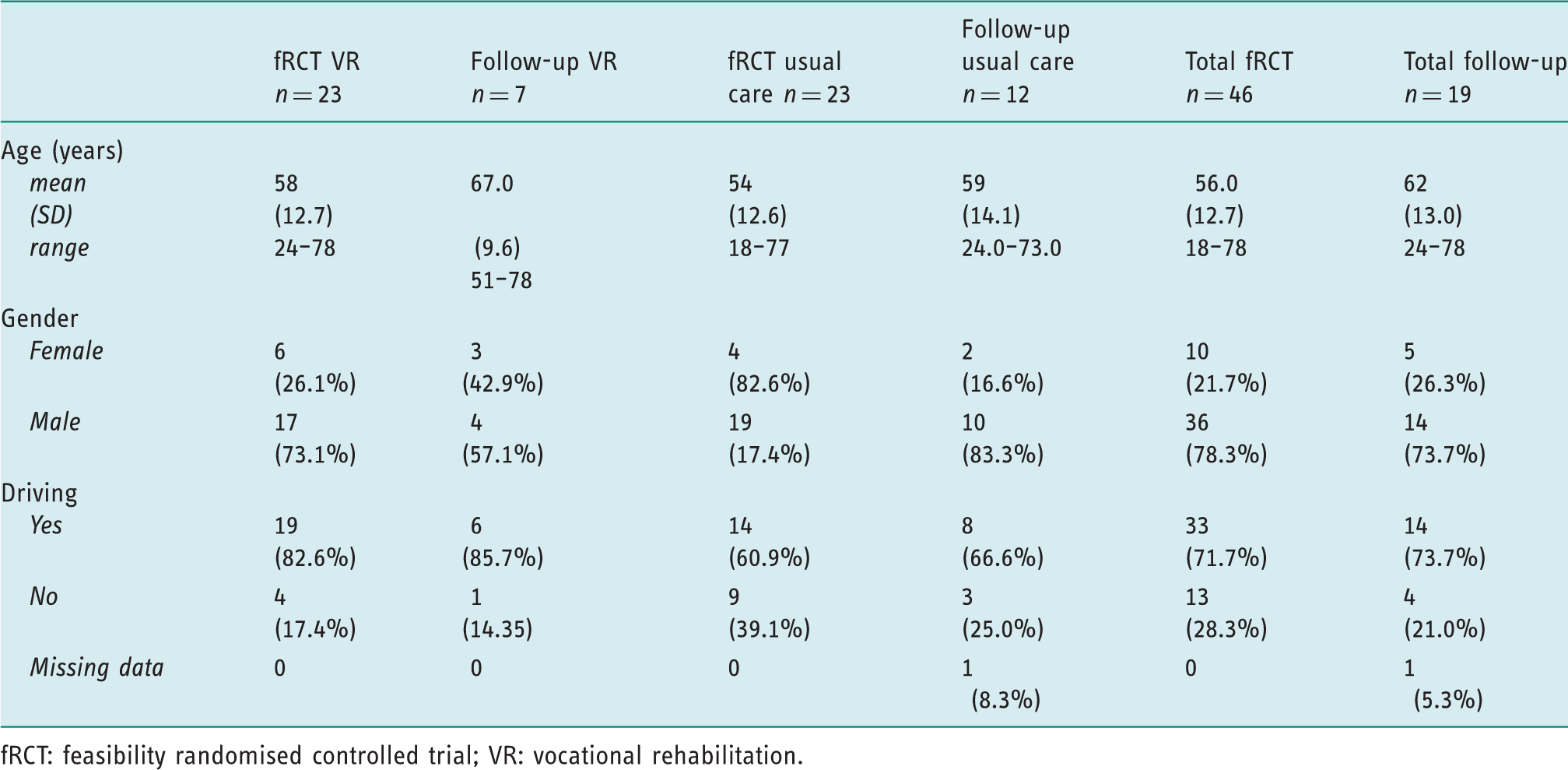
fRCT: feasibility randomised controlled trial; VR: vocational rehabilitation.
Questionnaire results
Summary of questionnaire results – 6 years post stroke.
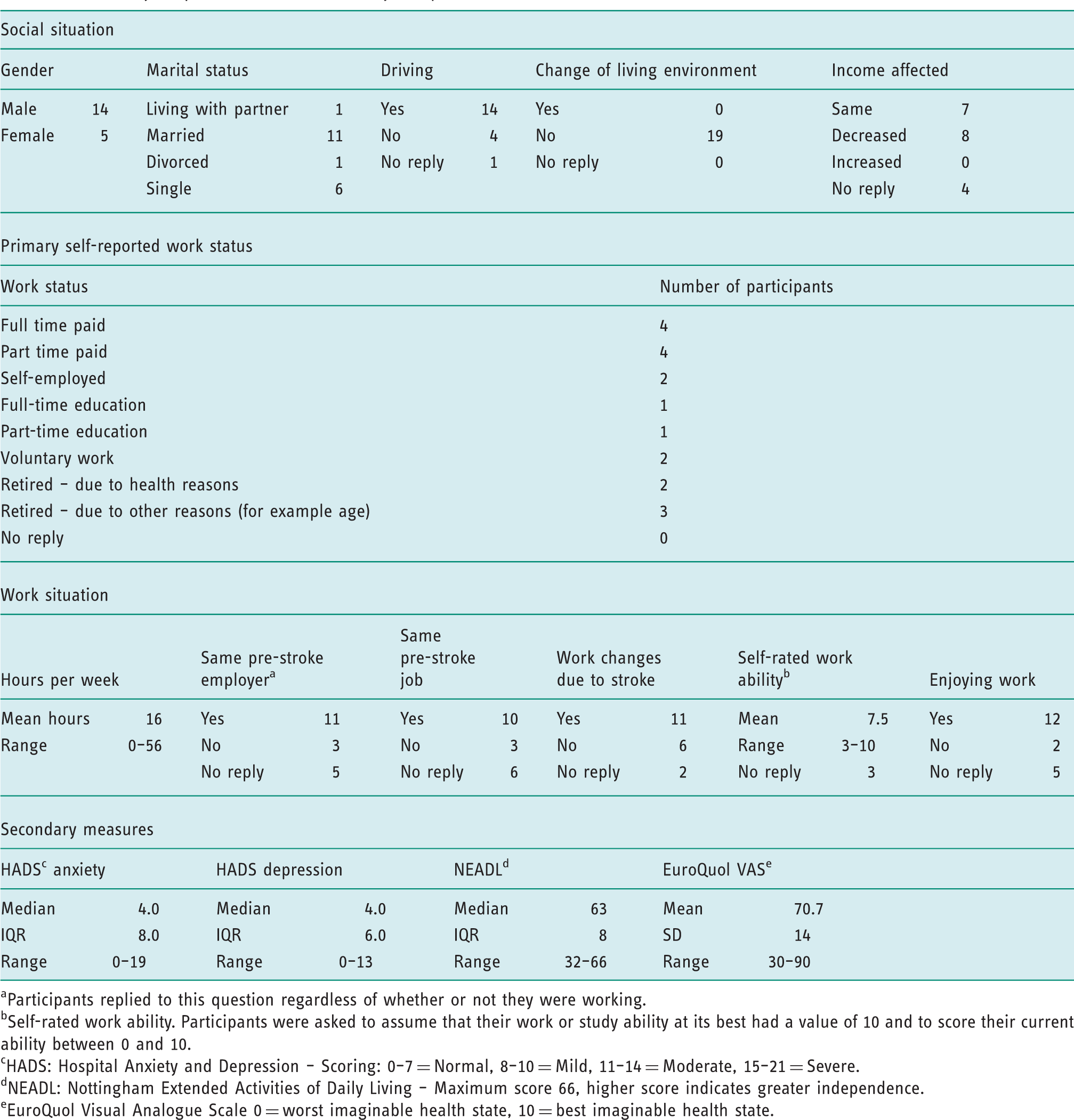
Participants replied to this question regardless of whether or not they were working.
Self-rated work ability. Participants were asked to assume that their work or study ability at its best had a value of 10 and to score their current ability between 0 and 10.
HADS: Hospital Anxiety and Depression – Scoring: 0–7 = Normal, 8–10 = Mild, 11–14 = Moderate, 15–21 = Severe.
NEADL: Nottingham Extended Activities of Daily Living – Maximum score 66, higher score indicates greater independence.
EuroQuol Visual Analogue Scale 0 = worst imaginable health state, 10 = best imaginable health state.
Work status
Participants in work at one year post stroke
Participants in work at 1 year post stroke and their 6 years post stroke work status.
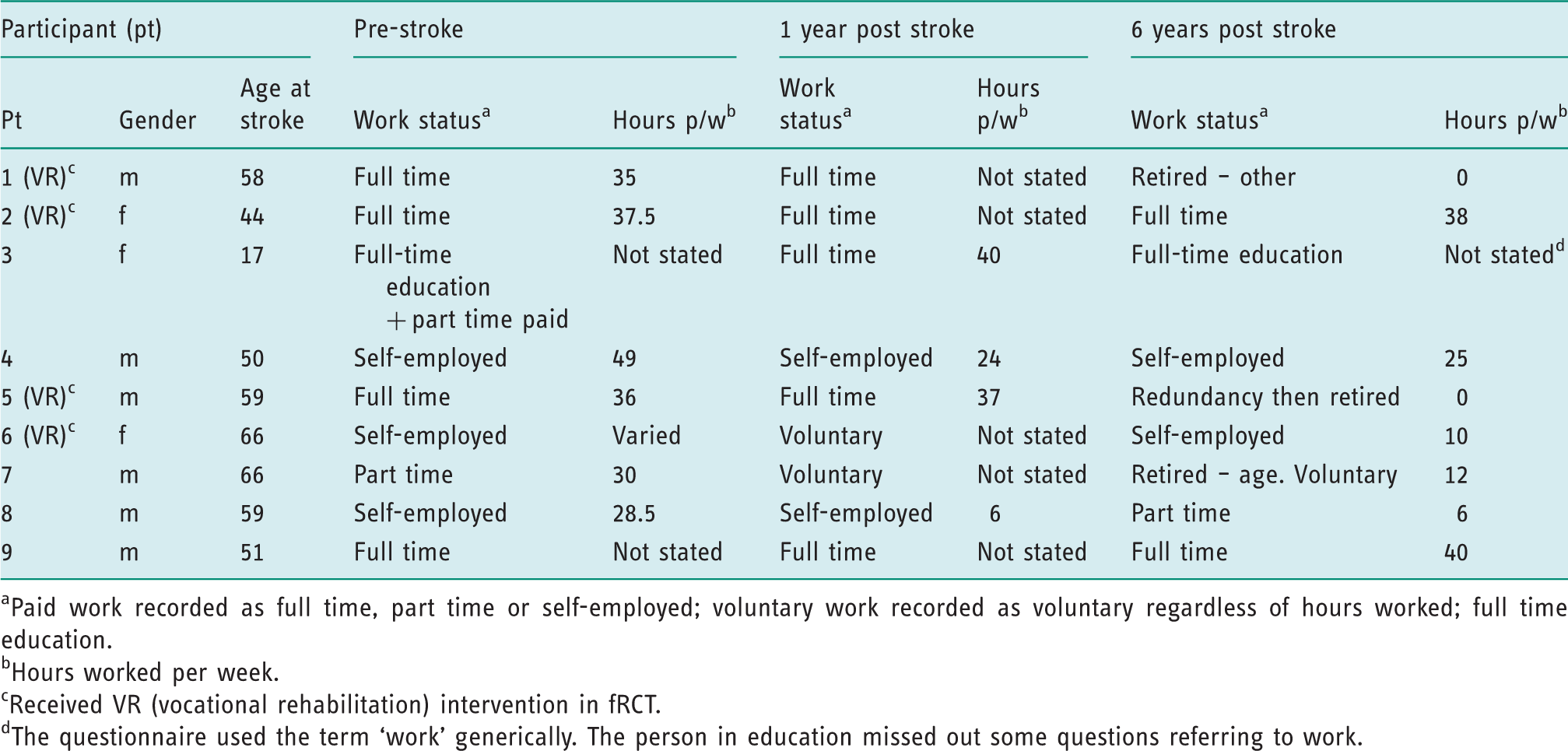
Paid work recorded as full time, part time or self-employed; voluntary work recorded as voluntary regardless of hours worked; full time education.
Hours worked per week.
Received VR (vocational rehabilitation) intervention in fRCT.
The questionnaire used the term ‘work’ generically. The person in education missed out some questions referring to work.
Participants not in work at one year post stroke
Participants not in work at 1 year post stroke and their 6 years post stroke work status.
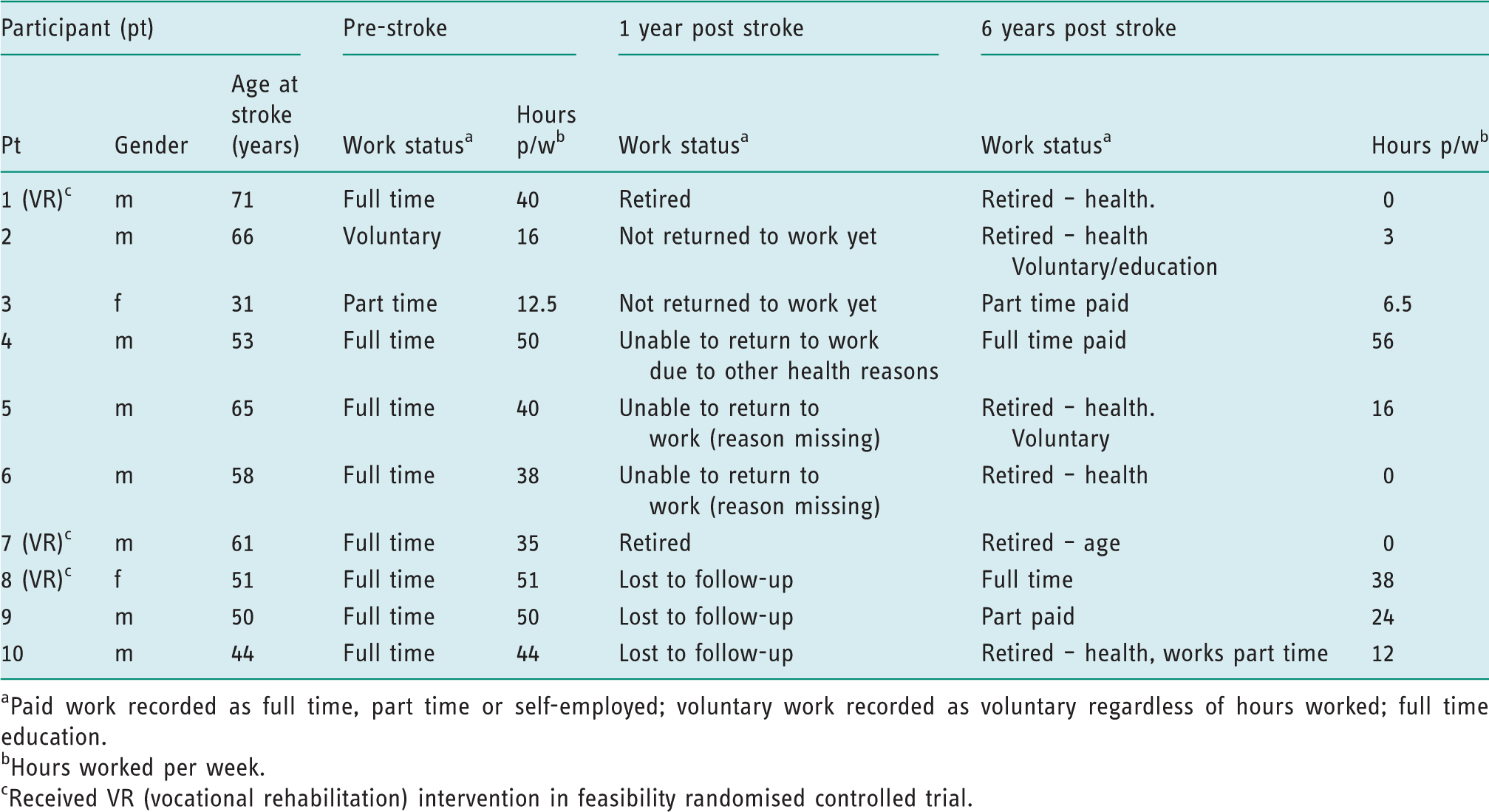
Paid work recorded as full time, part time or self-employed; voluntary work recorded as voluntary regardless of hours worked; full time education.
Hours worked per week.
Received VR (vocational rehabilitation) intervention in feasibility randomised controlled trial.
Three participants whose work status was unknown (lost to follow-up) at one year responded to the six-year follow-up questionnaire – see Table 3. All three were in paid work (two full time and one part time). One of these had initially retired due to health but at 6 years post stroke was working 12 hours a week.
In summary, of the 48 potential participants, five had died and 19 responded. All were in work at the time of stroke. The 12-month work status was known for 16/19 participants. Nine were in work at 12 months (47%). At 6 years post stroke, 14/19 (74%) participants reported that they were in work/education (10 in paid employment (53%), one in full-time education (5%) and three in voluntary work/part education (16%) – see Table 2). Five participants reported that they had retired for health reasons, but at six years one was in paid work and two were doing voluntary work. Six years after stroke, five participants aged 65 years old or older reported that they were working (self-employed n = 2, voluntary work n = 3).
Only one person in paid employment said they were no longer working with the same employer as they had pre-stroke. The rest remained with the pre-stroke employer, retired or moved to full-time education. Most reported that they were doing the same job as before their stroke (see Table 2). Only 3/13 reported that they had changed jobs, one of whom had moved to full-time education. When asked whether any change in work status was due to the stroke, 11 said yes, and six said no (see Table 2). Reasons for changes in work status were: ‘a need to work in a quieter environment’; ‘low energy’ and ‘reduced concentration’. One person said that the ‘stress of having teenage children’ caused them to change jobs.
Reasons for working
The primary reasons given for returning to work were: wanting to return (n = 9); to aid recovery (n = 7); able to work (n = 6); financial (n = 4) and work ‘needed me’ (n = 2). Only 2/14 people said they no longer enjoyed working and were only doing it for the money (see Table 2).
Income
Of those responding (n = 15), just over half (n = 8, 53.3%) reported a decrease in income (see Table 2). The others (46.7%) reported that their income had remained the same. Nobody’s income had increased in the six years since their stroke. The mean income from paid employment reported by 11 respondents was £15,797 (Range £3620 to £31,500). Of those stating the source of their income, 7/14 (50.0%) reported living off their salary with no other income; 1/14 (7.1%) said they relied on salary topped up by benefits; 1/14 (7.1%) reported salary topped up with income protection insurance; 3/14 (21.4%) reported living on a pension and 5/19 (26.3%) did not respond. One person reported that his wife had reduced her working hours to support him.
Effect of stroke
On the questionnaire, respondents reported a myriad of residual problems from their stroke including loss of sensation and weakness on affected side, lower tolerance for loud noises, difficulty with organisational tasks, reduced concentration, memory problems, reduced balance, increased fatigue, word finding difficulties, slow thinking skills, not being ‘robust’, loss of confidence, increased anxiety and being ‘reliant on wife’.
They also reported co-morbidities including vertigo resulting in a fall, non-Hodgkin’s lymphoma, epilepsy and additional difficulties due to ageing.
Secondary measures
For participants with complete data at both 12 months and 6 years, secondary measures scores were compared (n = 16). Self-reported NEADL scores were increased slightly at 6 years (63 interquartile range (IQR) 8.0, range 32–66) compared to 12 months (60 IQR 9, range 17–66).
For respondents with HADS scores available at both time points (n = 16), the median scores for both depression and anxiety at six years post stroke were compared. The mean self-reported HADS depression score (n = 16) at 1 year was 2.0 (IQR 3.0, range 0–9) and at 6 years was 4.0 (IQR 6.0, range 0–13). At 1 year the mean HADS anxiety score was 3.0 (IQR 4.0, range 0–8) and at 6 years it was 4.00 (IQR 6.0, range 0–19).
Individual secondary measure scores – 6 years post stroke.

HADS: Hospital Anxiety and Depression. Scores: 0–7 = normal; 8–10 = mild; 11–14 = moderate; 15–21 = severe.
NEADL: Nottingham Extended Activities of Daily Living: maximum score 66, higher score indicates greater independence.
EuroQuol Visual Analogue Scale: 0 = worst imaginable health state, 100 = best imaginable health state.
Participants rated their health-related quality of life lower at 6 years post stroke (70.7, SD 14, range 30–90) than at 1 year post stroke (77.4, SD 11, range 60–98). At 6 years post stroke, seven people reported no problems in all domains (mobility, self-care, usual activities, pain and anxiety/depression). The rest reported one or more problems with walking (n = 4), self-care (n = 3), usual activities (n = 5), pain (n = 5) and anxiety and depression (n = 6).
At 1 year post stroke, participants reported similar HRQOL scores irrespective of whether they were working or not (participants in work (n = 8) scored 77, participants not in work (n = 5) scored 77.5). However, participants who were in work at 1 year (n = 8) reported better quality of life at 6 years (mean 72.5) compared to participants who were not in work at 1 year. Their 6-year scores were lower (n = 5, mean 67.5).
Services
Fewer than half of respondents at 6 years (9/19, 47.4%) reported seeing a health professional in the last year. Five said they had seen their GP for a general review. Self-reported reasons for seeing a health care professional included Parkinson’s disease and diabetes reviews, fatigue management, anxiety, blood pressure and orthotics.
Qualitative interviews
Nine participants returned the form consenting to a telephone interview. Six interviews were completed. Of the remaining participants, two declined when contacted and one number was unobtainable. Five were men. Overall mean age was 63 (range 51–73). Three had received VR and three had received usual care. Other participants agreed to be contacted by email (n = 3) or letter (n = 9) but did not want to be contacted by phone. Interviews lasted between 20 and 40 minutes.
Three people were in work at 1 and 6 years post stroke (of whom two were self-employed). One person who was not working at 1 year reported that they were working full time at 6 years. One participant was retired at 1 and 6 years post stroke. The final interviewee was lost to follow-up at 1 year but at 6 years reported they had retired for health reasons but had returned to work part time.
Interview results.
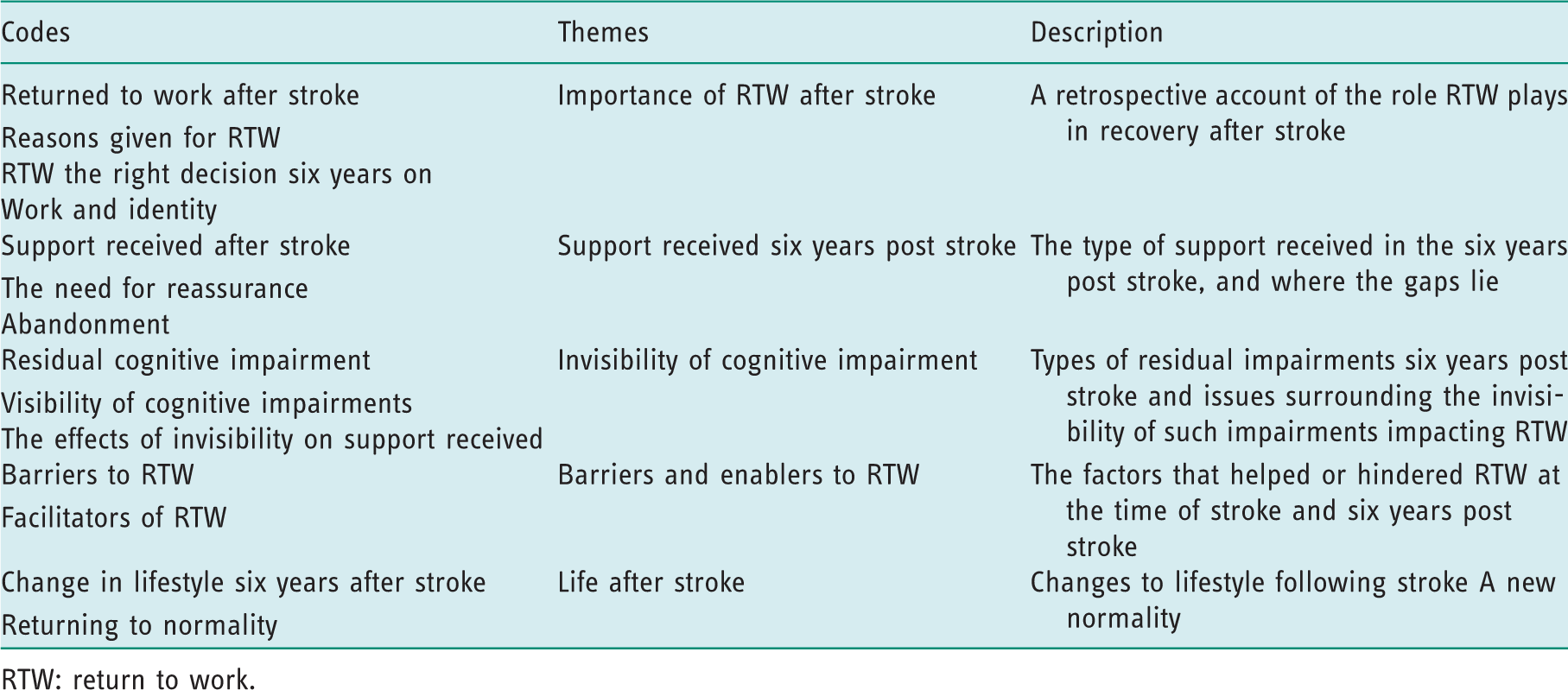
RTW: return to work.
The importance of RTW after stroke
The consensus from the interviewees was that they had made the right decision to return to work. All believed that work was beneficial to their recovery and ‘with the benefit of hindsight, I wouldn’t have done it any different’ (pt 3). They saw it as a return to normality: ‘[working] made me feel as if I wasn’t an invalid, I was back to being the old, the same person I was before even though deep down I knew I wasn’t’ (pt 2). Even when the only option was to RTW, this was still seen as positive: ‘it [work] helps your sanity. And we needed the money so it wasn’t an option for me not to’ (pt 6).
Support received after stroke
Support from occupational therapists initially after stroke was cited as being helpful. However, accessing help was not straightforward and not always seen as important by health care professionals, resulting in feelings of abandonment: [I] went to have a chat to him [GP] because I felt there were odd things that I should be able to do that I wasn’t properly … I can’t even remember them now but and he looked at me and he said if you think you’ve got a problem I’ll take you down to the nearest nursing home from here and you’ll realise you haven’t got any problems at all (pt 2).
The invisibility of impairments
Interviewees reported similar problems to those reported in the questionnaire. All said these impairments were problematic and not obvious: ‘I suppose if you’ve paralysed down one side or [inaudible] then it’s obvious somebody’s got a physical disability. But mentally they’re just not visible are they?’ (pt 3).
Fatigue was a major problem. One person was still trying to find answers 6 years post stroke: ‘I’ve been in and out of my GP for the last six years, saying where has my energy gone and nothing’s really sort of been found, I’ve now had a referral to the chronic fatigue clinic’ (pt 2). Another reported they were declined disability benefits: ‘as I say it’s really, really hard to prove a lack of energy’ (pt 1).
Interviewees said the invisible impairments impacted on quality of life, with respondents reporting taking antidepressants, losing confidence and experiencing mood swings.
Barriers and enablers
Barriers to work included not driving, reduced cognitive abilities, fatigue and employers’ concerns about job pressures: After my stroke because of me, because of my peripheral vision but I got that you know I got cleared for that so well I’ve got my licence and then when I had my seizures I had to send in my licence again (pt 4). I find it hard to pay attention; I find meetings and groups very confusing (pt 3). So I’m quite happy just to do the 12 hours a week (pt 3). Now they filter the calls and any they think I can do they send me an email detailing what the problem is and then ask me to have a look at it and get back to them if I can’t do it, if I can do it I go ahead (p3). I used to, I was a supervisor, a foreman, but my employers asked me just to go back to being a plant operator again because they didn’t want to put any extra pressure on me (pt 4). After the stroke I was able to … access my works pension on ill health grounds … without any reduction for kind of early medical retirement so that took all the pressure off (pt 3).
Life after stroke
Participants were still adapting to changes because the stroke had impacted on life both within and outside of work. Examples mentioned included being unable to dine out due to having to chew slowly and needing an extra hour in bed in the morning to ‘sort out in my mind what I have to do in the day’ (p5). This also included making healthier lifestyle choices to help prevent further strokes: ‘Right well I’ve stopped smoking and I’ve stopped drinking, it may sound daft to you, but it’s the best I can come up with at the moment, right?’ (pt3).
Returning to normality included having to deal with their own and other people’s experiences of stroke, including a work colleague and a spouse having a stroke.
Although many of the participants were in work, they said they were still finding ways to cope with the effects of stroke 6 years after onset.
Discussion
This mixed method study aimed to determine the feasibility of longer-term follow-up of trial participants 6 years post stroke and to explore participants’ work status and factors affecting work 6 years post stroke.
Feasibility
The response rate for this 6-year follow-up study of return to work was 40% (44% of those known to be alive), which is comparable to Westerlind et al. (2017). However, respondents were mostly high functioning and more likely to be in work, therefore there is a possible response bias. Three similar studies recorded higher response in usual care participants who have returned to work and conversely poor response from usual care participants who did not return to work (Grant, 2016; Phillips, 2013; Radford et al., 2018). Ways of encouraging participants who do not receive intervention and do not return to work need to be found.
Participants’ work statuses changed over time. Some people who were not in work at 1 year had returned by 6 years; some had retired due to age, health or redundancy; some moved from paid into voluntary work and many reported changes in their working hours. Defining and measuring ‘work’ remains a thorny issue for those attempting to record or describe work outcomes (Pransky et al., 2005; Wasiak et al., 2007). Consensus in defining work and terminology used to describe it is needed so that meaningful comparisons in return to work rates and changes in work status can be drawn within and across studies and over time.
Work status
Work was clearly important to the participants in this study. All of those who had returned to work reported that this was the ‘right decision’ and felt it had helped them return to some form of ‘normality’. Some even returned to work post retirement. These findings and the proportion reporting that they were in some form of work (74%) in this study are comparable to the findings of Westerlind et al. (2017). Both studies illustrate that work status post stroke can be maintained, is not static, and that some people return to work late after stroke with people often working reduced hours or in adapted roles.
No-one reported their income had increased and half of those responding stated that their income had decreased from 1 year. While changes in status from paid to unpaid work and a move towards retirement for a few explain some of this, it is still greater than the 18% reduction reported in the unmet needs survey by McKevitt et al. (2011). This could be because only 30–42% of people in the unmet needs survey were under 65 years. This means that the remainder of people surveyed would have been receiving state and other pensions which remain static regardless of whether or not a person is working. These findings suggest that having a stroke below retirement age may be financially detrimental even when the person returns to work. Taking early retirement due to poor health is likely to have lifelong financial implications. The true socioeconomic impact of stroke on the younger stroke survivor and their family needs to be further explored.
Enablers to work
Most of those in work at 1 year post stroke continued to work for their pre-stroke employer at 6 years post stroke. Employers were generally regarded as supportive and accommodating. Additionally, some people who were in work reported that early VR from an occupational therapist was helpful. This supports the findings in the qualitative meta-analyses that initial RTW experiences are important (Brannigan et al., 2017; Schwarz et al., 2017). These findings also suggest that positive initial RTW experiences can have lasting benefits for stroke survivors, as well as employers who retain valued staff members. Successfully working at 1 year may contribute to better quality of life in the longer term.
Barriers to work
Consistent with other studies, the ‘invisible impairments’, especially fatigue, were described as problematic, difficult to understand and presenting barriers to working 6 years post stroke (Brannigan et al., 2017; Schwarz et al., 2017). This is unsurprising as fatigue is reported to affect half of all stroke survivors (Stroke Association, 2018). Participants were still seeking solutions 6 years after stroke, supporting recommendations that help is needed to understand and manage these symptoms (Schwarz et al., 2017). Specifically, these findings support the recommendation by Wei et al. (2016) that VR post stroke needs to include management of cognitive problems and fatigue.
Despite high levels of function in this ageing stroke cohort (many of whom were driving and working), respondents reported a reduced quality of life, and over a third reported problems with depression and anxiety that could be classed within the clinical range. This illustrates a highly individualised picture and a complex relationship between function, work outcomes and wellbeing late after stroke that warrants further investigation.
The consequences of stroke, additional personal and family co-morbidities and ‘invisible impairments’ may affect a person’s ability to sustain work in the longer term. Currently, in the UK and internationally, access to stroke specialist occupational therapists that deliver vocational rehabilitation post hospital discharge is limited. Where services do exist, many are time limited and difficult to access late after stroke (Playford et al., 2011). It is believed that having timely access to VR could assist stroke survivors in managing the residual effects of stroke and may facilitate sustainable employment for stroke survivors. However, this assumption needs to be tested in further long-term follow-up of stroke survivors who receive VR in clinical trials.
Strengths and limitations
This feasibility prospective follow-up of participants’ employment and benefit status enabled a comparison of individuals’ work status at 1 and 6 years post stroke. However, selection (participants in the fRCT were employed at stroke onset and motivated to return to work), response bias and the small sample may have influenced the findings. High self-reported work status, instrumental activities of daily living scores and low self-reported health service resource use at 6 years indicate that respondents were fairly independent and high functioning. However, some people were struggling with invisible impairments that were not detected by the chosen tools and obscured by group means.
An additional limitation was the inability to approach participants in the earlier VR study directly or prompt or support follow-up, which may have resulted in a greater response.
Further areas of work
Research is needed to understand the relationship between function, work outcomes and wellbeing late after mild–moderate stroke. Further work should determine the nature and timing of support for stroke survivors and employers in sustaining work. Future research should explore how to define and record work, including changes in work status over time when participants are approaching and past retirement age, so that meaningful comparisons can be drawn between studies. Future VR studies should consider seeking consent for long-term follow-up from participants.
Conclusion
This study suggests long-term follow-up with stroke survivors is feasible, but ways of encouraging a more complete follow-up are required. It also highlights that working after stroke is highly valued and for some people sustainable 6 years post stroke. Many stroke survivors remained with the pre-stroke employer but on reduced hours, in altered roles and with a reduced income. Six years post stroke, participants still report residual ‘invisible’ impairments. These unmet needs are not currently met in the UK or many other countries. A summary of this study is also available on the Royal College of Occupational Therapists website (Phillips, 2018).
Key findings
Many who returned to work stayed in work for 6 years with their pre-stroke employer At 6 years post stroke, stroke survivors identified unmet needs due to invisible impairments
What the study has added
Most people who returned to work stayed with the same employer over the 6-year follow-up period but at reduced hours and consequently reduced income.
Footnotes
Acknowledgements
The authors wish to thank the participants for taking part in this study and Dr Judith Stevens and Martin Coult, PPI representatives, for their input on the findings of this study.
Research ethics
Ethical approval was obtained from NHS Health Research Authority (REC 16/EM/0423) and Derby Teaching Hospitals NHS trust (DHRD/2017/046).
Consent
All participants provided written consent to be interviewed for the study
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
Dr Julie Phillips received funding from the UK Occupational Therapy Research Foundation – The Elizabeth Casson Trust Post-doctoral Award 2015 to conduct this research.
Contributorship
Julie Phillips, Kate Radford and Kathryn Gaffney researched the literature. All the authors contributed to the methodology of the project and reviewed and approved the final version of the manuscript. Julie Phillips and Kate Radford applied for ethical approvals. Kathryn Gaffney conducted the interviews. Kathryn Gaffney and Julie Phillips collected and analysed the data and drafted the paper. Kate Radford reviewed the data, the interviews and added substantially to the paper.