
Abstract
Introduction
Although working with communities using community-centred approaches like community development has been identified as an important occupational therapy domain of practice, occupational therapists continue to struggle to clarify their roles and processes in this area of practice. From a study that aimed to describe the practice process of occupational therapists working in community development, this article presents key findings regarding how occupational therapists described their work with individuals and communities, providing a conceptualization of how to situate their work with individuals within a broad community context.
Method
Using interpretive description, individual interviews and focus group discussions were conducted via telephone with 12 occupational therapists from across Canada between February 2014 and March 2015.
Results
There was some uncertainty amongst participants regarding the definition of community development. Four layers of community-centred practice were inductively derived from the data: individual, group, community of interest, and systems. The latter two touch on community development.
Conclusion
The conceptualization that emerged from this study can assist occupational therapists in reflecting on current practice and furthering an appreciation of how their work with individuals can include a community focus, responding to calls within the profession to look beyond the individual.
Introduction
Literature focusing on occupational therapists engaging in community development (CD) is growing internationally, with examples being generated around the globe of occupational therapists working with communities (Pollard and Sakellarriou, 2017; World Federation of Occupational Therapists [WFOT], 2018). Exploring how occupational therapists engage with communities can deepen our understanding of how occupational therapists conceptualize their work in and with communities (for example by developing conceptual models to guide thinking (McColl et al., 2015)) and identify ways to strengthen the contributions of occupational therapists in this field (for example by developing models of practice to guide assessment and intervention (McColl et al., 2015)). Based on a study of Canadian occupational therapists, the purpose of this article was to conceptualize the multiple levels at which occupational therapists work to bridge individual and community-centred practice within community health practice. While the research focuses on occupational therapists working in a Canadian context, the conceptualizations offered are general enough to apply to a range of contexts and thus can facilitate discussion and critical reflection on community-centred practice to further advance how we think and talk about community development globally.
Literature review
CD is a broad, collective approach that involves working in partnership with community members to prioritize and address community-identified issues (Labonte, 2012). Although identified as an important health approach, disputes regarding definitions of CD and overlap in terms abound. In the occupational therapy literature, the term ‘community-centred practice’ is used to describe work with the community (rather than for the community) on priorities they have identified (Hyett et al., 2016; Scaffa and Reitz, 2014), with a focus on occupation as both the means and the end (Galvaan and Peters, 2017). Community-centred practice differs from typical community-based occupational therapy practice, which focuses on individual interventions. It emphasizes collective strategies guided by the community that have an impact beyond the individual; it also differs from community-level practice, which focuses on population approaches beyond the individual, but which are not necessarily guided by community-identified priorities and active engagement (Scaffa and Reitz, 2014).
It is widely acknowledged that CD, or community-centred practice, and community-based practice lie on a continuum (Jackson et al., 1989; Labonte, 2012). While other authors have made reference to this continuum within the small body of occupational therapy literature focused on CD (Leclair, 2010; Trentham et al., 2007), only one author has described the potential role occupational therapists could play along this continuum (Scaletti, 1999). Therefore, how this continuum unfolds in community occupational therapy practice is not well understood.
Community-centred practice and CD approaches have been identified as an important domain of practice for occupational therapists internationally because these approaches allow occupational therapists to impact groups of people, often the most marginalized, by addressing community health and wellbeing, in addition to working with individuals, thus supporting both health sectors' emphasis on community and the profession's social mandate (Craik et al., 2007; ENOTHE, 2009; Galvaan and Peters, 2017; Hyett et al., 2016; Lorenzo et al., 2006; Townsend and Polatako, 2007; Wilcock and Hocking, 2015). Despite this international support for engaging with communities, some occupational therapists have struggled to differentiate between community-based and CD approaches. In the Canadian context, some have also grappled to clarify their roles in community-centred practice (Lauckner et al., 2007; Restall and Ripat, 2008), reporting not being well prepared for CD through their formal occupational therapy training (Lauckner et al., 2007), with limited skills and knowledge related to enabling occupation with communities (Restall and Ripat, 2008) and lack of clarity on definitions of CD (Lauckner et al., 2007). While the reasons for these struggles are multi-faceted, the lack of preparation and contextual constraints are likely complicated by the lack of conceptual models linking occupation and CD to guide practice (Leclair, 2010). It has been proposed that occupational therapy education can be strengthened by including conceptual frameworks that foster understanding of communities and how they change/develop, along with the practical skills to promote such change (Galvaan and Peters, 2017; Lauckner et al., 2007; Leclair, 2010), essentially heeding McColl and colleagues' call for conceptual models that help us to think and models of practice that guide us in what to do (McColl et al., 2015).
Internationally, there have been efforts to conceptualize how occupational therapists engage in CD along the continuum of community-based to community-centred practice. The World Health Organization (WHO) has proposed community-based rehabilitation (CBR) as a CD strategy for addressing social inclusion of individuals with disabilities (WHO, 2010). While most recent discussions of CBR emphasize CD over service delivery (WHO, 2010), CBR can be more or less community-centred depending on if it is focusing on individual rehabilitation or broader community changes. There is growing attention internationally on working with marginalized communities to promote meaningful participation and justice, as evidenced by international compilations of such work (see, for example, Kronenberg et al., 2005, 2011; Pollard and Sakellarriou, 2017). In Brazil, social occupational therapy is advanced as a community-centred approach for addressing social inequalities (Malfitano et al., 2014), and in South Africa, occupation-based community development (ObCD) is a value-based form of occupational therapy practice with marginalized communities that builds capacities and challenges structural inequalities through equal partnerships and aims for connection and meaningful occupational engagement (Galvaan and Peters, 2017). In the North American/western context (which is the context of the authors and of this research), as early as 1990, Reitz proposed how the Model of Human Occupation could be used as a community empowerment model in a North American context (Scaffa and Reitz, 2014). Since then, a number of models have been proposed to outline occupational therapists' approaches to CD (see, for example, Lauckner et al., 2011; McComas and Carswell, 1994; Restall et al., 2003; Scaletti, 1999; Whiteford and Townsend, 2011). Most recently, Hyett and colleagues (2018) from Australia have applied occupational science concepts to CD cases to propose the Community-Centred Practice Framework, and Leclair and colleagues (Leclair et al., in press) have proposed modifications to the Canadian Practice Process Framework (Townsend and Polatajako, 2007) based on how Canadian occupational therapists work with communities.
Despite almost 30 years of literature on how occupational therapists can and should engage in CD in a range of contexts – literally, across various continents – learning across contexts has been limited to a few notable exceptions (for example Malfitano et al., 2014), and many occupational therapists continue to be criticized for narrowly focusing on individual issues (Hyett et al., 2018; Leclair, 2010) to the exclusion of recognizing the socio-historical and political contexts of occupations (Gerlach et al., 2018; Whalley Hammell, 2014). This focus may in part be due to constraints in the systems within which some occupational therapists work. In their descriptions of exemplars of occupational therapists engaged in CD within a health promotion framework, Trentham and colleagues noted that although many barriers faced by community members were systemic in nature, ‘the majority of community and institutional health care settings provide remuneration only for the provision of interventions aimed at individuals’ (2007: 64). This suggests a distinction in how individual interventions and community-centred approaches are conceptualized and valued in certain settings, with direct individual interventions seen as separate from, and of more value than, indirect community-centred work. Thus, existing conceptualizations and dialogues around occupational therapy's contribution to CD may not be sufficiently relevant to the reality and complexity of community occupational therapy practice. An examination of the experiences and perceptions of occupational therapists currently working in this field is needed to assist in understanding these complexities and bridging the perceived gap between individual and community approaches.
Further work is needed to effectively translate CD frameworks and approaches into community occupational therapy so that conceptual models can be used to inform models of practice to assist therapists in understanding and enhancing their contributions to this field. The authors of this study examined how occupational therapists described their work in and with communities to explore how individual and community-centred approaches inform each other in community practice. This subsequent analysis, which is the focus of this article, aimed to answer the following research question: How do community occupational therapists move beyond an individual focus to address community issues in their practice? As our funding was from a Canadian funding agency, we focused this inquiry on Canadian occupational therapists with the hope that our results would spark discussions and reflections locally and internationally.
Method
Design
Situated in the interpretive paradigm (Fossey et al., 2002), this study used interpretive description as described by Thorne et al. (2004) to detail Canadian occupational therapists' CD practice processes. Within this study, the emerging conceptualizations of CD, community-centred work, and community-based programmes (Hyett et al., 2016; Jackson et al., 1989; Labonte, 2012; Lauckner et al., 2011) and collective occupation (Leclair, 2010) were drawn upon to provide a foundational structure for understanding the data, albeit with an openness to discovery consistent with an inductive analytic lens (Thorne et al., 2004).
Ethical approval for this study was obtained from the University of Manitoba Health Research Ethics Board (H2013:334) and Dalhousie University (2013-3057). All participants in the study provided written informed consent.
Participants
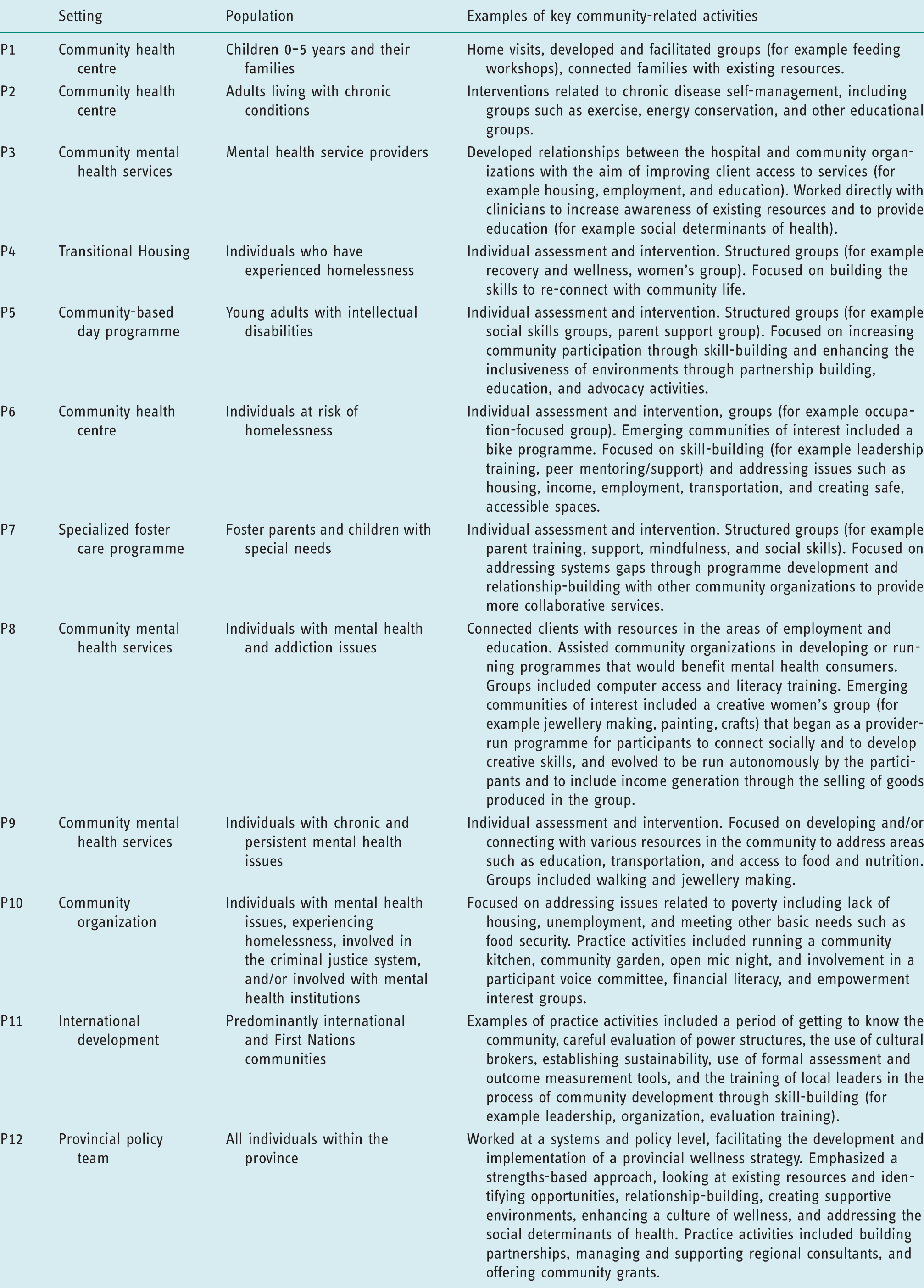
Eligible occupational therapists were identified through purposive, snowball sampling (Patton, 2002). The researchers used the Canadian Association of Occupational Therapists (CAOT) Networker to contact occupational therapists whose primary area of practice was ‘health promotion and wellness’ in the community. The authors also compiled a list of Canadian occupational therapists who have written about CD. A list of 55 occupational therapists potentially working in CD was generated and email invitations were sent. Twelve occupational therapists who met the inclusion criteria and provided some representation from different regions in Canada were recruited to promote maximum variation sampling and to ensure likelihood of applicability of findings to diverse contexts in Canada. Participants were registered occupational therapists, identified as having at least one year's experience in CD practice, and had a working ability in English. Participants self-identified as engaging in CD work, which was defined in recruitment material as working with community organizations or groups to address their community's health and wellness priorities, focusing mainly on the community level.
Data collection
Two data collection methods were used: in-depth semi-structured telephone interviews and follow-up telephone focus groups. Also, socio-demographic information (regarding years' experience and location) were gathered to describe the participants. Individual semi-structured telephone interviews conducted in 2014 were used to gather information about how the occupational therapists engaged in community practice. The interview questions asked about the occupational therapists' roles with the community, community assessment and intervention planning, and the role of occupation in community practice.
Following preliminary analysis, the same individuals were asked to participate in a telephone focus group to engage in critical dialogue around the preliminary findings (Thorne et al., 1997). Between November 2014 and March 2015, five of the 12 participants were available to participate in focus groups (Participant (P) 2, P3, P6, P8, and P12) and an additional three who weren't available at scheduled focus group times were able to participate in a second individual interview using the focus group guide (P5, P9, P11). The focus groups/interviews explored participants' general impressions and clarification of the preliminary analysis and any experiences or key ideas they felt were missing. Data analysis in this article is based on the 12 individual interviews, and the follow-up focus groups and interviews.
Data analysis
Interviews and focus groups were audio recorded and transcribed verbatim. Semantic thematic analysis (Braun and Clark, 2006) was used to analyse the data, initially focusing on practice processes (Leclair et al., in press), then latent thematic analysis occurred to explore how the participants described working in and with the community in order to deepen our interpretation of community practice (Boyatzis, 1998). Each interview was reviewed by at least two team members to identify preliminary themes. Through an iterative process the researchers established consensus on categories, consistent with interpretive description analysis, which focuses on ‘synthesizing, theorizing, and re-contextualizing rather than simply sorting and coding’ (Thorne et al., 1997: 175). At least two researchers analysed each focus group transcript, with the intent to adequately capture the richness of the data across diverse contexts and experiences. Initial categories were further refined to reflect the complexity of CD as engaged in across the participants, which was far less clear than first conceptualized during descriptive analysis (see Leclair et al. (in press) for more detail). As a result of the focus groups and further discussion within the research team, additional analysis ensued in order to be inclusive of the nuances of participants’ varied activities at the individual and community level. All transcripts were considered together to develop the themes.
Several methods were used to ensure methodological and interpretive rigour (Fossey et al., 2002). The researchers demonstrated congruence using a methodology particularly suited to answering the clinical yet socially constructed nature of the research question (Thorne et al., 2004), as the research question arose from examination of the clinical practice of community occupational therapists. The researchers demonstrated responsiveness by continuing their analysis beyond looking only at practice processes to explore the complexity of the relationship between individual and community practice. Data were collected over a prolonged period of time, and sampling aimed to identify participants with adequate community experience from diverse regions of Canada. Interpretive rigour (Fossey et al., 2002) was strengthened through the use of direct quotes, critical reflection by participants on preliminary findings (Thorne et al., 1997), and solicitation of informal peer feedback (Shenton, 2004) on conference presentations that allowed us to gauge if early conceptualizations resonated with others working in community development (Lauckner et al., 2017; Leclair et al., 2015).
Findings
Participant descriptions.
In considering the research question, How do community occupational therapists move beyond an individual focus to address community issues in their practice? two related themes were identified: (a) navigating uncertainty, and (b) linking individual and community issues.
Navigating uncertainty
Although participants were required to self-identify as working in CD, interviews revealed that some participants were uncertain of the extent to which they were in fact engaging in CD. It was noted that occupational therapists sometimes used the terminology of ‘community programmes’, which referred to occupational therapist-led community-based initiatives, interchangeably with ‘CD’, suggesting overlap in understanding of the terms.
The participants were often in new positions that required them to create their
own job description. One participant expressed uncertainty about being an expert
in CD, despite numerous years of experience: I constantly feel… like what I do is a bit of a façade … I work in a
community, I work with the community… but… I don't know… that I'm really
an expert in it … I'm still struggling with how I do that on a
day-to-day basis. (P6)
Occupational therapists spoke of the complexity of working in and with communities. One participant explained that in working with communities it is important to ‘understand the power structure of a community from within and its connections with other communities and the political system’ (P11). Related to this, another therapist spoke of the importance of having time to look at ‘bigger picture issues’ (P6) in the community around patterns of unmet needs amongst clients to understand the complex dynamics impacting community members. The complexity of community issues and the community engagement process were noted, with a constant balancing of individual and community needs and recognition that ‘not everyone is going to be happy’ (P4). This latter issue of complexity, in particular shifting between individual and community needs, is further explored in the next theme.
Linking individual and community issues
Occupational therapists in this study worked primarily for health or social service community organizations at a combination of four levels: individual, community group programmes, communities of interest, and systems/policy. The term ‘level’ was used to describe a change in client focus with a different emphasis in practice. While some participants acknowledged they may not be engaging in CD in its truest form, patterns of involvement at these four different levels were seen amongst all the participants, illustrating potential convergence of these approaches in holistically describing the community work of occupational therapists. The levels and activities engaged in at each level are described.
Individual level: Linking to services
Some participants talked about completing work at the individual and family levels to address client goals around community involvement. One occupational therapist described this work as reacquainting people with the skills needed to be ‘active community member[s]’ (P4). Individual-level interventions included education for the client's family, individual goal-setting and skill development, and a focus on connecting individual clients to existing community resources.
Through such individual work, occupational therapists were able to view their
single client within the context of a broader community. One participant
stated, ‘I’m helping people live in communities’ (P10). Another participant,
engaged in work with children, explained a ‘spreading out’ effect of
individual work that can positively impact the broader community. I hope that by improving occupations of these children who've had
such hard lives, have so many issues, that [the impact] kind of
spreads out. And they end up doing better in school and so their
school community is healthier. (P7) [My work is] all centred around occupation because when you're
looking at the social determinants of health… these are needs, basic
needs, needs that people need to meet in order to engage in
occupation and in order to pursue their recoveries so that they can
explore their occupations, and even just simple self-care tasks
can't be done without meeting these basic needs.
(P3)
Community group programmes: Fostering relationship and skills
As some participants identified similarities amongst individual clients, the need for the development of community-based group programming arose. This programming typically involved a group of clients that shared goals that could be met through a group. Although issues addressed in these groups arose from the priorities of members, the therapists led these groups. Occupational therapist-facilitated groups covered a variety of areas: chronic condition management, walking, recovery and wellness, parent support, feeding, computer access and literacy, relaxing occupations, and cooking.
At this level, control and leadership tended to remain with the occupational therapist and/or the organization offering the programme. While members provided feedback, they were not involved in the planning or leading of the group. These groups served to develop skills in preparation for transfer to situations outside the group, and to offer mutual support.
Similar to the first level, work with communities did not happen at this level; however, important community-building between people with similar concerns began to occur in these groups.
Emerging community of interest: Partnering and local leaders
When participants became aware of larger issues shared by several individuals and potential opportunities to address these issues, the emphasis shifted to working more organically with the emerging community of interest. Communities of interest emerged as people from a range of sectors came together around a common commitment or issue rather than coming together because of a programme. These communities of interest seemed to have the potential of taking on a life of their own as those involved sought innovative ways to address their priorities. The occupational therapist did not lead these programmes, but rather worked in partnership with individuals from the community and/or other community organizations to identify ways to collaboratively address concerns. One occupational therapist stated: ‘I accompany, but I don't lead’ (P11).
Linking with other sectors or organizations through partnerships was central to creating something new that would meet community-identified priorities. Creating new, welcoming, and ‘safe’ spaces (P10) from which these initiatives could grow was important. For example, one therapist and a group of people experiencing housing insecurity identified that the lack of access to transportation was a shared issue. She was able to work with the emerging community of interest, including a variety of community partners, to develop a bicycle repair initiative that offered community residents access to refurbished bicycles. This process involved an intentional partnership with a community member who was supported to take on a leadership role in the training sessions. Another participant worked with a community of interest around issues of financial literacy and another to help develop employment opportunities for women with disabilities through microcredit programmes (small loans that supported business initiatives). With a community of interest, the occupational therapist took on a facilitative role, supporting community members to assume gradually greater leadership roles. As one occupational therapist explained, ‘So it's not me [leading]. I’m never, never at the forefront…. I will do a project only if someone within the community, preferably the group, will take ownership’ (P11). Roles of community members in these emerging communities of interest were sometimes referred to as ‘champions’ or ‘local leaders’.
At this level of emerging communities of interest, participants explicitly named CD principles guiding their work. Some of these principles included allowing time for the process to unfold, learning about and from the community as the first step, recognizing and building upon existing strengths, focusing on relationships and local leadership to ensure sustainability, shedding the expert role, and giving attention to shifting power dynamics. Thus, it was through emerging communities of interest that community-centred approaches began to be more explicit in occupational therapists' work.
Systems/policy: Changing services and systems
Three of the occupational therapists worked at the policy/system level, while others were considering ways to further effect change at this level. One participant's work focused on ‘building partnerships and collaboration… the notion of joining, forming relationships, working together…’ while also ‘building capacity for community development’ (P12) in the region, thus describing her CD work as being ‘more at the systems level and organizational structural level’ (P12). Another participant referred to her focus on the ‘needs of the system’ (P3). Systems/policy level work moved beyond supporting individuals to access programmes and emerging communities of interest, to focusing on the structures and services that support or hinder the community's health and wellbeing. One participant emphasized that in addition to service coordination, she works ‘at the system level to improve socioeconomic environments in supportive wellness’ (Focus Group (FG) 2). At the systems level, the focus was on supporting stakeholders, including other programme and service providers, to increase accessibility and relevance of services for community members.
The focus at this level is the supports available to individuals and groups and those not yet connected at any of these levels. The focus is thus necessarily on the shared environment that either hinders or facilitates health and wellbeing. As another occupational therapist explained, ‘our client is the environment, [as] it's the environments that either hinder or facilitate active healthy living that are going to make the difference’ (FG 2).
Those working at the systems/policy level have an increasingly broad target
population, moving beyond individuals and groups to looking across sectors
to support more inclusive, comprehensive, and relevant structures and
processes for communities. One participant explained, We don't work with individuals. We have more of an enabling role with
schools [and] communities, and that includes organizations within
communities, NGOs, municipalities, First Nations groups, … and
workplaces to help them take action to support wellness within their
context. (P12)
Similarities and interactions between levels
All participants, regardless of level, came to see common occupational issues that impacted their clients, and many of these issues were attributed to the social determinants of health. For example, some of the common occupational issues described included difficulty engaging in meaningful occupations due to lack of accessible spaces, challenges navigating the various health and social services systems due to uncoordinated services and programmes, and difficulty accessing housing and employment due to lack of skills and knowledge about programmes.
Some occupational therapists focused on social occupations, either linking
individuals to existing group services or creating new occupational
opportunities based on identified needs and interests. For example,
occupation-based groups provided opportunities for people to connect with
others through meaningful activities. Such groups included jewellery making,
open mic night, employment workshops, a community garden, and a community
kitchen. The provision of safe occupational spaces in the community was
viewed as important. Further, a unique perspective shared by participants
was their focus on ‘doing’, as explained by one participant, I tell people I'm an occupational therapist. So everything we're
going to do has to take shape into action … And an action that would
actually have an impact on the occupations of the community. (P
11)
Rather than viewing the broadest level of interaction as the ultimate goal, it was noted that participants who were more certain in their community-centred approaches worked across levels to ensure a comprehensive, multi-layered understanding of the community. In particular, the outer rings of emerging communities of interest or the systems/policy level also required an appreciation of, and preliminary work to be done at, the individual and group levels. A comprehensive approach to working with communities involved continuously attending to and moving between each of these levels. As one occupational therapist summarized this approach, ‘At a community level we're trying to … look at what's an elegant solution to a problem that's happened to more than one person – to make it a little bit more multi-layered’ (P6).
In this study, occupational therapists were constantly looking at individual needs, group programming needs, communities of interest, and systems/policy level issues and back again, recognizing the impact of each. An emphasis on any one level might be based on a variety of factors, such as practice setting, mandate, and community priorities. The experiences of the participants highlights that regardless of the focus of one's community practice, therapists are aware of the multiple layers and how each impacts the other, with a unique understanding of the impact on the daily lives of individuals. Thus, participants noted parallel and complementary processes at individual and systems levels: ‘To me, [working at the systems level is] very, very much in tune with what I did as a community occupational therapist…. To me the process is identical’ (P12).
Discussion and implications
The results of this study suggest that some of occupational therapists' uncertainty regarding their role in CD reported in the literature (Lauckner et al., 2011; Restall and Ripat, 2008) is still present. While over the years many in the literature have called for more community-centred approaches (for example Hyett et al., 2018; Scaletti, 1999; Whiteford and Townsend, 2011), few have conceptualized CD based on the experiences of occupational therapists in community practice. This study contributes to a deeper understanding of how we can conceptualize CD within the practice reality of occupational therapists to describe how individual and community needs are navigated.
Apparent amongst the occupational therapists in this study is representation of the continuum of CD proposed by Jackson et al. (1989), which conceptualized how individual interactions can contribute to CD. In this continuum, individual interventions can lead to group programmes, which can lead to discussions of shared issues, which can eventually lead to collective action (Jackson et al., 1989). This study provides examples of what occupational therapists may do at various stages within this continuum.
Recognition of the multiple levels at which occupational therapists work can help to further distinguish between what has been referred to as community-based practice and CD (Labonte, 2012). If an occupational therapist is primarily working at the individual or professional-led programme level in the community, they are engaging in community-based practice. Of note amongst the occupational therapists working at the individual level in this study is the notion of a ‘spreading out’ effect, where work with individuals could have an impact on the broader community. This finding is in keeping with Trentham et al. (2007), who similarly noted interactions between the individual and community level in their CD work. The current study illustrates that, even when focusing predominantly on one level, occupational therapists were aware of and considered potential impacts on the other levels. This study therefore captures the complexity of occupational therapy community practice that can occur at and between levels, offering examples that affirm the various contributions occupational therapists make to CD, either directly through practice with communities and working at the systems level, or indirectly by intentionally working with individuals to connect them to the broader community or link them with others who share their experiences. A conceptual model that reflects one's practice activities provides the opportunity for more occupational therapists to see themselves and their work as contributing to community-centred practice. Rather than thinking that CD is something that other occupational therapists do, it is our hope that occupational therapists in a range of practice settings will see themselves in this conceptualization and thus the distinction between individually focused, community-based practice and CD will be bridged.
The current study's conceptualization can therefore be seen to both complement and expand upon the recent conceptualization of the Community-Centred Practice Framework (Hyett et al., 2018), which identifies four main features: community identity, community occupations, community resources/barriers, and participation enablement. The current study confirms many of the concepts presented in the Community-Centred Practice Framework, including the importance of place/setting, issues of resources and power, and ways to promote participation (Hyett et al., 2018). While Hyett's framework proposes how occupational therapists could work in community-centred practice, the current study goes further in describing the range of levels at which occupational therapists actually work in community practice, illustrating how working with individuals can be embedded in, and/or can contribute to, CD.
Based on the sample of occupational therapists recruited for the current study, there are few in positions that are fully dedicated to CD where a community-centred model, like that proposed by Hyett and colleagues, would apply to all facets of their work. In practice, occupational therapists may strive to be community-centred, but this intention often needs to be balanced with individual work, which the current study also includes. In addition to linking individual and community-centred practice, the unique contribution of the current research is the conceptualization that occupational therapists engage in more than one level at a time, with a unifying focus on occupations. Supporting Hyett and colleagues' focus on community occupations, the occupational therapists in the current study add further to our understanding of how social occupations can be fostered in the community to promote social interactions, an example of Whalley Hammel's call for occupational therapists to focus on occupations that offer opportunities to belong, feel connected, and contribute to others (2014). Within these social occupations, opportunities for developing leadership skills and contributing to others were supported. In this way, occupations acted as a conduit between the individual and the broader community.
Our findings support calls for occupational therapists to look beyond individuals to what Gerlach and colleagues (2018) refer to as a critical orientation that requires ‘occupational therapists [to] continue to attend to and address individual capabilities and priorities while simultaneously recognizing and tackling broader social and structural determinants’ (37). In many ways, this study provides practical examples of how occupational therapists can heed this call. Despite the efforts of the occupational therapists in the current study to recognize and address broad systemic issues that impacted individuals’ lives, the explicit naming of critical factors that challenge the dominant focus on individualism was not unanimously evident amongst the therapists. While the complexity of working with community was acknowledged, critical analysis of the many factors impacting communities and individuals and how therapists worked at these levels requires further exploration. This study is an initial step in describing how occupational therapists can link individual work with clients to broader community issues. Considering these findings in light of recent justice-oriented conceptual models, such as Whiteford and Townsend's Participatory Occupational Justice Framework (2011), would assist occupational therapists in bringing a critical, rights-based lens to their work in and with communities.
Some limitations within the proposed conceptualizations put forth from this study must be considered. This study included Canadian occupational therapists and may not be transferable to other dissimilar contexts. While occupational therapists from various parts of Canada were involved, not all regions were represented and not all participants participated in the focus group process that offered opportunity to clarify or challenge preliminary analysis. Because of the diversity of settings and countries where CD approaches are used, more participants would add additional perspectives, particularly in countries which have health care systems different from Canada. The applicability of this framework for understanding the multiple levels of CD requires further testing and refinement with more occupational therapists working in a wider range of settings and contexts.
Conclusion
Adding to existing conceptualizations of community-centred occupational therapy practice drawing from the general field of CD (Hyett, et al., 2018), the current study describes how community occupational therapists work across individual, group, community, and systems levels. Amidst calls within the profession to challenge our focus on individualism (Gerlach et al., 2018), this research conceptualizes how some occupational therapists move beyond a narrow view of individual practice to situate clients within a broader community context to identify ways to create change with a community.
Key findings
Practising occupational therapists are required to navigate the lack of
conceptual guidance on how to work with communities. This study proposes that it is useful for practising therapists to
consider how individual, group, community, and systems-level approaches
contribute to and impact each other, allowing for an embedded
understanding of individuals within communities.
What the study has added
This study offers a conceptualization of occupational therapy community practice that links individual-level intervention, group programming, and community development approaches, woven together with opportunities for social occupations.
Footnotes
Acknowledgements
Thank you to the Canadian Occupational Therapy Foundation for funding this project. We would also like to thank the occupational therapists involved in this study for their time and thoughtful contributions.
Research ethics
Ethical approval for this study was obtained from the University of Manitoba Health Research Ethics Board (H2013:334) and the Dalhousie University (2013-3057) in 2013.
Consent
All participants provided written informed consent to be interviewed and to participate in focus groups for the study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclose receipt of the following financial support for this research: this project was funded by the Canadian Occupational Therapy Foundation.
Contributorship
Heidi Lauckner and Leanne Leclair co-led the grant application and led their respective applications for ethical approval. Cynthia Yamamoto was a research assistant on the grant. All authors contributed to the development of data collection tools, the updating of recruitment materials, and the methodology of the project. Cynthia Yamamoto assisted with recruitment and conducted the first individual interviews. All authors contributed to the follow-up focus groups and interviews. All authors contributed to data analysis and interpretation. Heidi Lauckner wrote the first draft of the manuscript. All authors reviewed and edited all versions of the manuscript and approved the final version of the manuscript.