
Abstract
Introduction
The understanding of the temporal pattern of individuals can add a wider perspective to interventions. Therefore, the present study is aimed toward analysis of the temporal activity pattern of individuals with stroke compared to healthy adults.
Method
This study is a prospective, case–control, analytic research study. The study sample comprised 50 individuals with stroke and 50 individuals without disease, for 80% power with a 5% type 1 error. The Modified Occupational Questionnaire was administered to assess the temporal activity pattern. Individuals identified the activities performed at each hour of the day and data was analyzed.
Results
The temporal activity pattern of individuals with stroke differed from healthy controls; education and play activities were not part of stroke participants’ daily routines. Also, participation in work, leisure and social participation activities was significantly different for people with stroke compared to healthy controls (p < 0.01). The study group assigned very low values to the activities; the value perceived by individuals differed significantly between groups (p < 0.01).
Conclusion
Clinicians are in a position to enable individuals’ time use and help to engage them in meaningful activity. Individuals with stroke may benefit from a program focusing on the temporal aspect of activities.
Stroke is defined as the rapid development of the clinical signs of disturbance of cerebral function with symptoms such weakness of the face, arm or leg, most often one side of the body (WHO, 2018). Despite improvements in stroke rehabilitation, stroke can still cause functional loss in many performance areas (Karataş , 2011). Functional problems occur daily after stroke, and 80% of stroke patients find themselves confronting social and physical limitations after they are discharged home (Anderson and Whitfield, 2013). In time, individuals become aware of chronic limitations and major changes even in their performance of household tasks (Walsh et al., 2015). People often undergo negative experiences such as loss of their jobs and roles, as well as an inability to perform routine activities (Salter et al., 2008; White et al., 2008).
The daily routines of individuals need to be monitored to better understand the nature of personal activities (Kielhofner, 1977). Activities have a structure that is shaped according to people's experiences and it is necessary to examine the subjective structure of activities (Pierce, 2001). Effective utilization of time has been found to be associated with health and wellbeing, which are thus interpreted together in the literature (Wilcock, 2014). Engagement in meaningful occupations that have been structured to achieve satisfying daily activities will enhance wellbeing (Hammell and Iwama, 2012), although further knowledge is needed to develop an understanding of how temporal structures of occupations will influence health (Pemberton and Cox, 2011; Yerxa, 2014).
As a result of a temporal dysfunction, time use can be disrupted and temporal activity pattern can change (Kielhofner, 1977). Temporal activity pattern shows the time aspect of activity performance and investigates personal nature of the activity in relation to frequency, duration, and organization with respect to time. Thus, it is strongly related to self-perception, value and interest (Kielhofner, 1980). Assessment of temporal pattern, placement of activities in the time cycle and time distribution of activities according to the given value can be done through using time diaries (Farnworth, 2003).
There has been an increased interest in the participation of individuals with stroke in daily life. However, there is still little information on the quantity or quality of this participation (Björklund et al., 2015; English et al., 2014; Urimubenshi, 2015). Several studies suggested the need for a greater understanding of the change in performance, activity and participation after stroke (Eilertsen et al., 2013; Wood et al., 2010). Prospective studies are required to understand the link between the person and participation restrictions, the drivers of activity and the context of activity to improve the functional status and participation of individuals with stroke (English et al., 2016; Skolarus et al., 2014; Urimubenshi, 2015).
The understanding of temporal adaptation concept and demonstration of the temporal pattern of individuals can add a wider perspective to interventions, thus enabling clinicians to plan strategies to increase wellness and participation of individuals. Therefore, the present study is aimed toward analysis of the change in temporal activity pattern of individuals with stroke in chronic stage compared to healthy individuals. The study aimed to answer, “What are the activities that form the daily routines of individuals with stroke?” and “How does the time use and temporal activity pattern of stroke individuals differ from that of healthy adults?”
Methods
Participants
This study is a prospective, case–control, analytical research study. The study sample comprised 50 individuals with stroke and 50 individuals without disease, for 80% power with a 5% type 1 error to detect a minimum statistically significant difference. Participants with stroke were identified from the database of the physical medicine clinic in a State Education and Research Hospital. Individuals between the ages of 18 and 65 years who were diagnosed with a stroke by a physical medicine and rehabilitation specialist were invited to participate in the study. The exclusion criteria for the study group were as follows: diagnosis of a psychiatric illness that strongly affects the participation to daily life activities according to medical reports (such as schizophrenia or bipolar disorder), being in the acute phase of the disease (<6 months), aphasia that would affect the time use assessment via interview and a score of <26 on the Montreal Cognitive Assessment (MoCA) test (Julayanont and Nasreddine, 2017). To form the study group, hospital records were examined by the researcher İYT to ensure the inclusion criteria was met, and the eligible stroke individuals were contacted via telephone by the same researcher. None of the individuals had known the researcher before, and the researcher did not have any relationship with the research group. Individuals were briefly informed about the current study on the phone and invited to participate.
Individuals without disease constituted the control group. To create the control group, the impact of the cultural, social and socioeconomic status was taken into consideration. For this reason, the individuals were selected from a sociocultural environment similar to where the individuals in the study group spent their time. One family member per participant was invited to participate to the study via telephone by researcher İYT. Individuals who played a caregiving role for the patient, lived with the patient or had a chronic illness (diabetes, lung disease, cancer, and so on) that affected their independence in performing daily living activities were excluded from the study.
The aim and procedures of the study were explained in detail verbally, and an explanatory statement that explains the study in written form was provided and an informed consent form (Hacettepe University Ethics Committees, 2013) was obtained from all of the individuals who voluntarily agreed to participate and came to assessment for the study. This study was approved by the Non-Interventional Clinical Trials Ethics Committee under the record number GO/941.
Procedures
A total of 62 individuals with stroke were telephoned by the researcher İYT; however, 2 were excluded as they did not meet the criteria and 10 declined to participate in the study. Of the 10 individuals, 4 did not consent as they could not commit to the study timelines, 5 did not consent due to travel commitments being too difficult and 1 declined but did not give a reason. For the control group, 68 individuals were telephoned by the researcher İYT. Four of them had chronic illness (diabetes mellitus and heart rhythm disorder) and therefore were excluded from the study. Additionally, 14 individuals decline to participate in the study; 8 of them could not get permission from work, 4 of them did not have time for this study and 2 of them were out of town. Figure 1 depicts a flow chart showing the inclusion of individuals constituting the two groups.
Study flow chart for participants.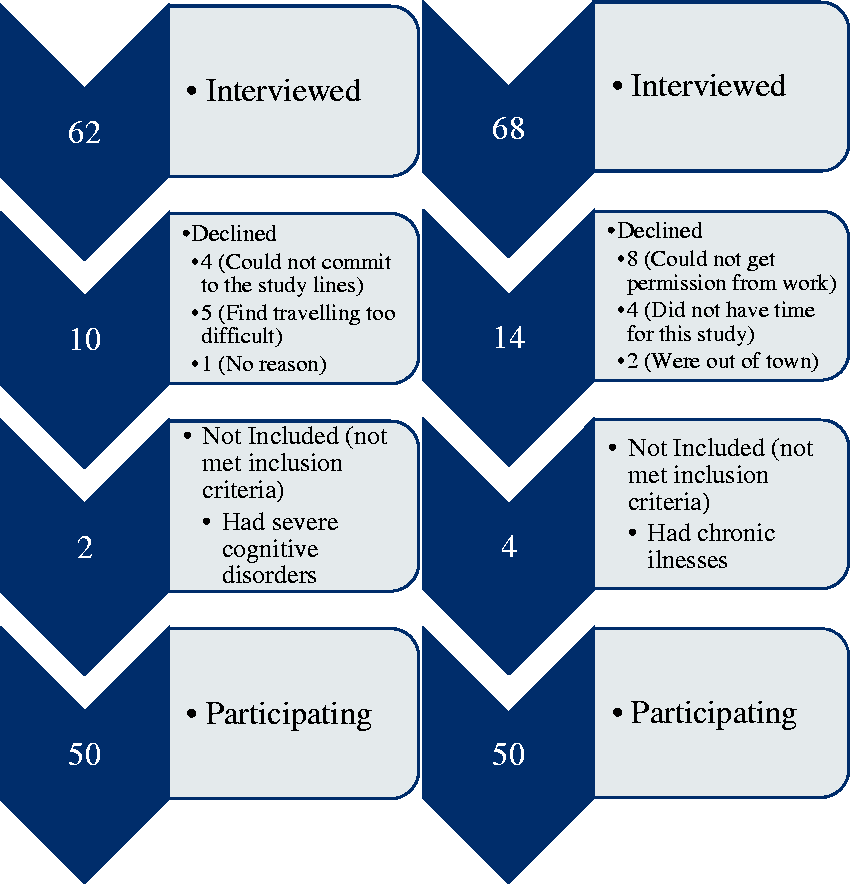
The study was conducted at the Occupational Therapy Unit of a Physical Therapy Clinic at an Education and Research Hospital of a State University. The assessment tools were administered on a face-to-face basis within the official working hours of the public institutions by the first author (İYT) of the study. To eliminate bias, data were analyzed by the second author (BSA) of the study, who did not participate in the interviewing process, and so did not have an assumption for the results.
The assessment lasted between 45 and 60 minutes. Because of its importance as an exclusion criterion, at first, the cognitive function level of all individuals was assessed using the MoCA test. Then, participants were questioned about their age, sex, education level and occupation to gather demographic information; in addition, the disease duration of the study patients was recorded. Before gathering information on temporal activity pattern, the concepts of temporal pattern and activity were explained with examples to the individuals in order to obtain the best results from assessments. The Modified Occupational Questionnaire (MOQ) (Scanlan and Bundy, 2011) was used to assess the temporal activity patterns of individuals.
MoCA
MoCA is a functional rapid screening tool for mild cognitive dysfunction. It facilitates the assessment of different cognitive domains: attention and concentration, executive functions, memory, language, visual-constructional skills, conceptual thinking, calculation and orientation. This test takes approximately 10 minutes to administer. The maximum score is 30 points, and a score of 26 or above is considered normal (Julayanont and Nasreddine, 2017). The MoCA has shown to be an appropriate measure for cognitive screening with high sensitivity, good reliability and factorial, convergent and discriminant validity (Freitas et al., 2012; Shi et al., 2018).
MOQ
The MOQ is a measure of meaningful time use. Basically, the MOQ focuses on two important objectives: what the person was doing or how he/she used their time, and how the person felt about it. The MOQ is a time diary that asks respondents to report on what they do “on a typical day” in hour blocks from 05.00 to 05.00 the following day. The meaningfulness of each activity was investigated according to the following criteria: (a) category of activity, (b) reason why the person engaged in the activity, (c) value of the activity to the person and (d) perceived value of the activity to society. There were three options to answer as to why the activity was performed: “I had to do it,” “I wanted to do it,” or “I had nothing else to do.” Questions related to the value of the activity to individuals and their perception of the value of the activity to society were rated on a 5-point scale (1 = not at all valuable, 2 = not very valuable, 3 = somewhat valuable, 4 = quite valuable and 5 = very valuable) and demonstrate the meaningfulness of each activity (Scanlan and Bundy, 2011). The purpose of this questionnaire is to provide information on the activities of individuals in their daily routines by considering time dimension, as well as the extent to which these activities are valuable and relevant to individuals.
After individuals identified the activities performed at each hour of the day, the activities in each timeline were categorized according to the occupations listed by the American Occupational Therapy Association (AOTA). These occupations are activities of daily living (ADL), instrumental activities of daily living (IADL), rest and sleep, education, work, play, leisure and social participation (Amini et al., 2014).
Statistical analysis
Statistical analysis of data recorded in the study was conducted using the Statistical Package for the Social Sciences (SPSS, v. 21) program. Sociodemographic information of the study individuals and activities performed at every hour were recorded by the MOQ. The frequency of activities performed at each hour was measured for both groups and expressed as a percentage. Recorded activities were divided into groups according to AOTA’s occupational domains. The difference between the frequency of “doing the activity” according to AOTA domains and the “reasons to do activity” was calculated with Pearson chi-squared test or Fisher’s exact test (according to the size of the expected values in 2x2 contingency crosstable).The value for the individual and society was examined by Mann–Whitney U test. A p value of <0.05 (two-tailed test) was considered to be statistically significant for all tests.
Results
The study group included 50 individuals: 56% females (n = 28) and 44% males (n = 22); the control group also included 50 individuals: 60% females (n = 30) and 40% males (n = 20). The mean age of the individuals was 51.24 ± 10.63 years in the study group and 48.40 ± 12.91 years in the control group. According to an independent samples t test, the two groups were similar in terms of age (p > 0.05).
Individuals’ sociodemographic properties.

Job/occupation status shows the timeline before stroke (for stroke individuals).
Regarding the affected sides, the right side of 58% of stroke individuals (n = 29) and the left side of 42% (n = 21) was affected. The average stroke duration was 1.86 ± 0.95 years (range, 1–4 years). Most patients (48%; n = 24) had a stroke history between 1 and 2 years. Individuals were asked about assistive device use and it was found that 60% (n = 30) use three-point walking sticks and other individuals (n = 20) did not use any device.
Modified Occupational Questionnaire results of the groups.
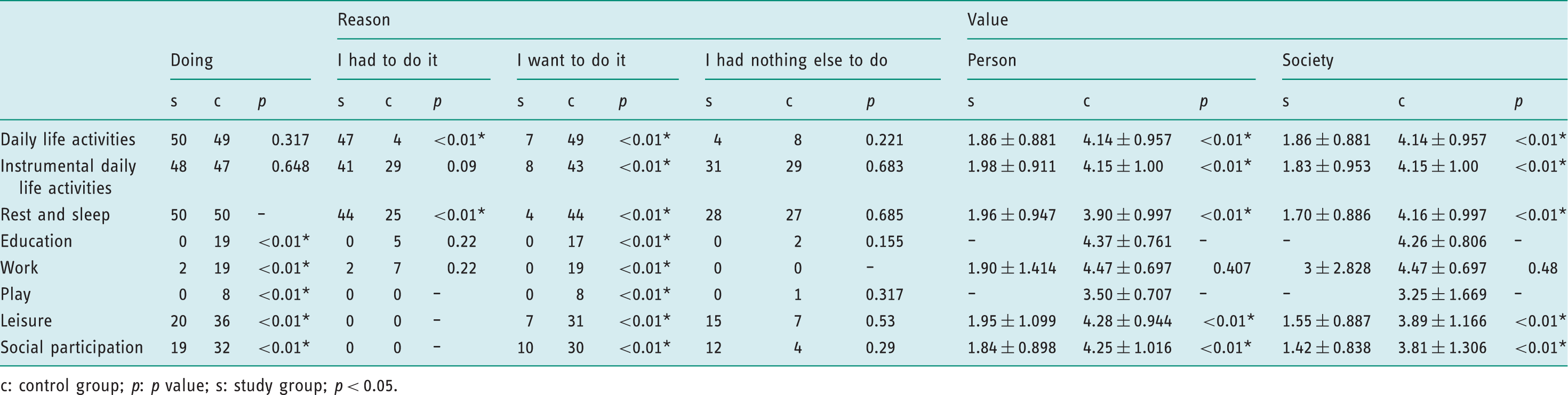
c: control group; p: p value; s: study group; p < 0.05.
The most time-consuming five activities of groups between three different time intervals.
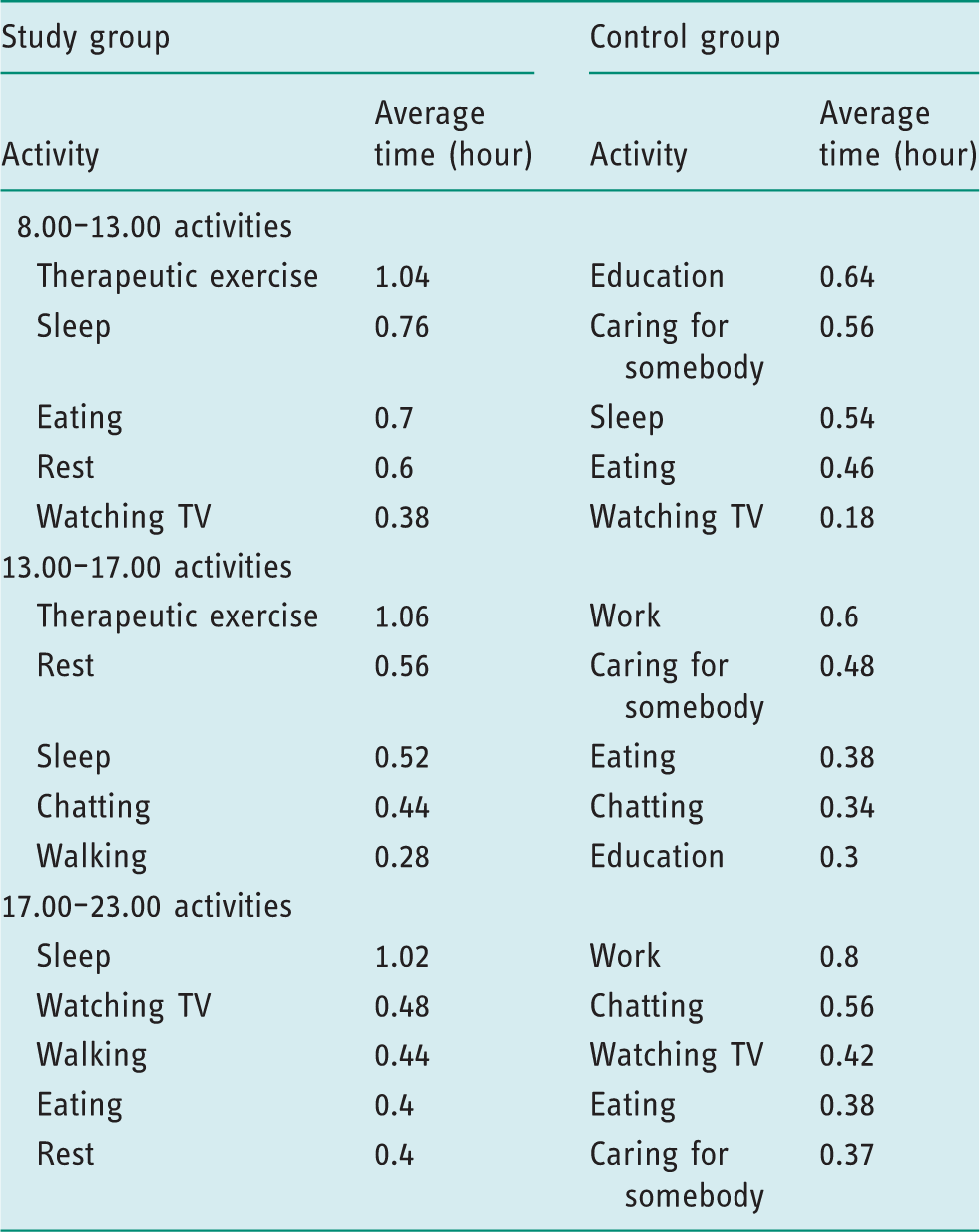
Time intervals and routines stated in the MOQ under each AOTA occupation domain were also analyzed. ADL were basically performed by both groups; however, allocated time and activities differed between groups. The most time-consuming activity in both the groups was eating, but the study group allocated more time for this activity than that allocated by the control group. The control group listed different activities under the domain of self-care activities; however, the study group listed only showering. IADL were also typically performed by both groups. The study group allocated more time for these activities as opposed to the control group. The study group performed very little variety of activity under this occupational domain and spent an average of 4.1 ± 2.38 hours only for therapeutic exercise.
The study group used 45.58% (10.94 ± 2.10 hours) of 24 hours for rest and sleep, did not include any educational activity or play in their routines and only two individuals engaged in any working activity. Control group performed activities such as going to courses, handcraft and playing console game under the educational activity or play domain. The control group participated in leisure activities significantly more than the study group (p < 0.05). Social participation was also less in the study group (p<0.05), but the most preferred activity was the same in both the groups: chatting.
Discussion
Patterns are important for achieving a purpose or goal in life for satisfying personal needs (Christiansen and Baum, 1997). This study demonstrated that the temporal activity patterns of individuals with stroke differed from those of healthy individuals in the control group; they developed different activity patterns compared with healthy individuals. The major change was a decrease in the number and variety of activities. Secondly, the time spent on certain activities, which were commonly performed by both the study and control groups, differed considerably; for example, stroke individuals spent either more or very little time than usual on some routine activities, and thus follow a different routine activity pattern. Stroke individuals did not spend time engaging in education and play activities but spent more time in rest/sleep and therapeutic exercise.
It is stated that adult individuals devote time to work, education, personal care (Gauthier and Smeeding, 2003; Pentland et al., 1999), social activities, their households (Cella et al., 2016), sleep (Cella et al., 2016; Garikapati et al., 2016) and IADL (Cella et al., 2016; Fricke and Unsworth, 2001; Gauthier and Smeeding, 2003) during the day. The study showed that individuals with stroke mostly use time for sleep, rest and watching TV, but not on other activities, and this was particularly evident on comparing our results with the control group. Similarly, people with schizophrenia (Cella et al., 2016) and chronic obstructive pulmonary disease (Hunt et al., 2014) spent less time in self-care, social and leisure activities and more time in sedentary behaviors compared to the general population.
Sedentary behavior is evident and has adverse effects for individuals with stroke (Alzahrani et al., 2011; Atler, 2016). More recently, the duration of time spent on sedentary behavior has been associated with cardiovascular disease risk, type 2 diabetes, breast and colon cancers, and cardiovascular and all-cause mortality (Tremblay et al., 2010). Studies also have confirmed that sedentary lives can replace meaningful activities of individuals with stroke (Alzahrani et al., 2011). Based on the shift in activity domains, we interpreted that the study group spent their time sleeping, resting and performing therapeutic exercises, which they would otherwise have spent on productive and leisure activities. It is very important to educate the person and the family about the risks of sedentary life. We may say that temporal activity pattern is valuable with regard to decreasing morbidity risks and increasing quality of life by achieving meaningful participation.
ADL is important for the continuity of life (Bonder and Dal Bello-Haas, 2017). Our results demonstrate that individuals with stroke perform ADL to go on with routine life; however, activity diversity and time allocation was not similar to the control group. In his work on ADL, Bejerholm et al. showed that individuals find ADL more meaningful when it is in balance with time use (Bejerholm et al., 2006). As meaningful participation was lacking according to our results, we think it is necessary to analyze the variety of, and time spent on, ADL activities as well as the intent and reason underlying these activities. A notable difference between groups was that stroke individuals did not perform self-care activities like shaving, applying make-up and grooming under this domain. Bonder et al. emphasized the need for individuals to care for their bodies (Bonder and Dal Bello-Haas, 2017). Higher self-efficacy of individuals with chronic stroke indicated more participation and independence in ADL (Frost et al., 2015). Therefore, it is very necessary to focus especially on self-care activities in this population. At the beginning, a plan to increase time use for self-care activities may have a positive effect on participation.
It is stated that ADL is negatively affected by many different factors such as cognitive impairment, depression, visual disturbances, fatigue and other physical problems after stroke (Anderson and Whitfield, 2013). Our results indicated that stroke individuals take more time to complete activities than healthy individuals. One of the reasons for this could be the impairments stroke survivors may have. However, devoting longer time to one activity may inhibit the person to do other activities, thereby affect temporal activity pattern. Kielhofner stated physical, mental or psychological pathologies prevent individuals from dedicating the adequate time to activities and finding new meaningful activities (Kielhofner, 1977). A broader understanding of impairments affecting time utilization for meaningful activities may help clinicians develop effective programs to overcome participation difficulties.
Another output of this study showed that one of the most time-consuming activities performed during an entire day for the study group was engagement in therapeutic exercises, which is listed under the IADL domain of AOTA. Fricke et al. found that more than 20 IADL activities were performed by healthy participants during a day, and transportation activities were the most important ones for participants (Fricke and Unsworth, 2001). IADL is found to be negatively affected as our study group did not value any activity different to therapeutic exercise and often repeated only this activity. This may be because individuals will to increase their wellbeing and believe they will get better with exercise. Physical activity is effective as a rehabilitation tool for improving functional recovery (Dunn et al., 2017) and wellbeing (Globas et al., 2012) after stroke. However, studies have shown a decline in doing physical activities and increase in sedentary life 2–4 years after stroke (Paul et al., 2016). For our study group, it may be beneficial to organize therapeutic exercise in temporal pattern. It is also important to encourage valued IADL and understand their effect on wellbeing and psychological status.
One study have shown that 5–10 years after stroke, at least 30% of survivors experience a reduced social everyday activities (Wolfe et al., 2011). The results of our study were also consistent with this finding: social interaction was disrupted as study groups’ temporal activity pattern did not cover any work, social participation, educational or leisure activities. Stroke survivors were less likely to engage in recreational activities or go out for visits with their families than healthy controls. One of the predictors for participation restrictions was depression and anxiety symptoms (Skolarus et al., 2014). Social participation is strongly related with mental health: better community participation indicates better mental health (Ding et al., 2015). Taking into consideration the fact that the individual gets used to doing nothing for social participation or work, friend-bonding activities can be planned to start interaction with individuals. It would also be useful to encourage stroke individuals to perform socially relevant activities in different physical environments, such as those performed by healthy individuals.
We found that unlike the control group, individuals with stroke assigned a very low value to the activities and did the tasks out of necessity and not interest. Hocking indicated that health and wellbeing can be created, experienced and restored by participation in the valued and meaningful occupations that enable people to participate in meaningful occupations (Hocking, 2013). Stewart et al. reported that more than 70 studies have shown that occupation influences health and wellbeing positively (Stewart et al., 2016). The temporal activity pattern of individuals with stroke lacked meaning. Stroke individuals can be encouraged to think of valued occupations and involve valued activities in their daily patterns. Thus, occupational wellbeing can be gained.
This study had several limitations. First, the selection of participants could not be randomized. However, to avoid any bias, the researcher who analyzed the assessment results was not involved in interviewing process. Second, there was a lack of knowledge of the physical environment. It would be beneficial to know where and in what conditions individuals spend their time. Third, it was not enough to understand the temporal activity pattern of individuals by investigating the activities performed by them only on a 1-day basis. Analyzing activities performed over at least a week would have provided more detailed information and would have enabled us to understand the differences between activities performed during weekdays and weekends. Fourth, the assessment tool that we used to address temporal activity patterns records one activity over each hour. However, there is a possibility that individuals performed more than one activity over an hour. Because we questioned the individuals regarding their most time-consuming and valued activity, there is also a possibility that valuable activities of a shorter duration were not considered. Finally, to obtain generalizable results and have normally distributed data, studies with larger sample size are warranted.
It is important to understand the complexity in temporal structures of occupations to enhance subjective health (Björklund et al., 2015). This study showed the temporal dysfunction in activity pattern of individuals with stroke and suggested the areas in which individuals with stroke need to be supported. Therapists may benefit from this knowledge when planning treatment during the chronic stage of stroke. Participation in valued activities may be the basic aim; however, self-care, IADL, social interaction and productive activities were the areas that need the attention of clinicians. The variety of activities may be increased; thus, a valued healthy pattern can be developed in individuals. Finally, evaluation of individuals in terms of his/her temporal pattern can add a different perspective to clinicians.
Key findings
The temporal activity pattern of stroke individuals significantly differed from that of healthy individuals. For people with stroke, therapeutic exercise and sleep have taken the place of meaningful activities. Participation in valued activities was lacking for people with stroke.
What the study has added
This study provided data that support the link between participation in meaningful activities and health for individuals with stroke. Analyzing the temporal aspect of activities outlined the need for encouraging activity balance and engagement in self-care, social participation, and productive and instrumental activities of daily living. This study can help clinicians to structure the lives of people with stroke and their families.
Footnotes
Research ethics
This study was approved by the Non-Interventional Clinical Trials Ethics Committee under the record number GO/941 in 2016.
Consent
The aim and procedures of the study were explained in detail verbally, and informed consent was obtained from the individuals who voluntarily agreed to participate in the study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of the article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Contributorship
İbrahim Yavuz Tatlı and Burcu Semin Akel researched literature, applied for ethical approval and contributed to the development of the data. All authors contributed to the methodology of the project and the statistical analysis plan. İbrahim Yavuz Tatlı gathered data and Burcu Semin Akel carried out the statistical analysis. İbrahim Yavuz Tatlı wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.