
Abstract
Introduction
Over 400 million people worldwide are living with diabetes. Research suggests that people struggle to manage their diabetes and an in-depth understanding of the lived experience of diabetes is required to inform and promote occupational therapy practice. This article reports on one part of a PhD study into the role of occupational therapy in diabetes self-management.
Method
Semi-structured interviews using an intuitive inquiry methodology were conducted with 22 people with diabetes in three separate studies. Analysis of the lived experience of all participants was drawn together to explore the understanding of diabetes self-management from an occupational perspective using the Model of Human Occupation.
Findings
The occupation of diabetes self-management was conceptualised with seven inter-related occupational forms. Challenges were related to occupational identity, volition, habituation, performance capacity and the context in which these took place.
Conclusion
This study, embedded in the experiences of those with diabetes, suggests that occupational therapy has a distinct role in diabetes self-management, through seeing this self-management as an occupation. The use of the Model of Human Occupation enables a focus on the characteristics of the occupational forms and how these might be adapted for successful occupational engagement.
Introduction
The rising number of cases of all types of diabetes worldwide is a concern for public health policy (World Health Organization (WHO), 2016) and the personal impact on the individual with diabetes is considerable. Approaches to diabetes self-management (DSM) that can help people to manage this condition and prevent further complications in terms of the context of their own lives appear to be the way forward (Nagelkerk et al., 2006).
This research article focuses on one aspect of a PhD study into the role of occupational therapy in DSM. The three aims of the PhD study were to explore the lived experience of diabetes, explore the use of metaphor to understand that experience and explore the role of occupational therapy in relation to DSM. A previous article described the lived experience of diabetes (Youngson et al., 2015) and the focus of this article is a consideration of the use of the Model of Human Occupation (MOHO) (Kielhofner, 2008) to conceptualise DSM as a distinct occupation. Within this, the occupational forms and the impact of volition, habituation, performance capacity and the environment will be considered.
Diabetes
Over 400 million people worldwide are living with diabetes but it can also result in premature death and disability (WHO, 2016). There are three main types of diabetes: type 1, type 2 and gestational diabetes (WHO, 2016). Prediabetes is a borderline condition, where blood glucose levels are higher than normal and where it is considered that people are at risk of developing type 2 diabetes (Mainous III et al., 2014). Type 1 is characterised by the body’s inability to produce insulin, while in type 2, either not enough insulin is produced or the insulin does not work properly (WHO, 2016). Gestational diabetes is a temporary condition that develops in pregnancy where the mother develops resistance to insulin (WHO, 2016). Insulin is required to help glucose enter the cells from the blood stream, where it is used as fuel. Lack of, or resistance to, insulin results in high blood glucose levels, which can lead to macrovascular complications such as cardiovascular events and stroke (particularly when combined with high blood pressure and cholesterol levels), and/or microvascular conditions such as kidney, eye and nerve damage (WHO, 2016). Poorly controlled diabetes is also linked to depression, anxiety, phobias and eating disorders (Diabetes UK, 2016). Type 1 diabetes is not preventable and is treated with insulin therapy. Type 2 is the most common form of diabetes and may need medication to lower blood sugar levels. In the long term, insulin therapy may be required. It is overall recommended that lifestyle changes are made to diet and exercise to control blood sugar levels to manage and prevent type 2 diabetes (WHO, 2016).
DSM
Traditionally DSM is viewed from the medical perspective of monitoring of blood glucose levels (HbA1c), blood pressure and cholesterol, collectively known as metabolic control (NICE, 2015). Additionally, people with diabetes are encouraged to make lifestyle changes to pursue a healthy diet, take more exercise and comply with medical recommendations (WHO, 2016). However, this tends to simplify exactly what is involved in the complexity of DSM. This includes managing medication and testing (Montez and Karner, 2005), engaging in healthcare appointments (Thorne and Paterson, 2001; Watts et al., 2010) incorporating diabetes education (Lutfey, 2005), plus lifestyle changes such as alterations to diet (Brackenridge and Swenson, 2004), and incorporating exercise (Nagelkerk et al., 2006). Evidence suggests that, despite educational programmes and healthcare guidance, many people with diabetes struggle to adhere to advice on self-management and experience barriers to successfully incorporating this into individual lifestyles (Mulvaney, 2009; Nagelkerk et al., 2006). Indeed, Ingadottir and Halldorsdottir (2008) conclude that managing diabetes is a constant balance between trying to follow recommendations and the wellbeing of living a normal life.
Occupational therapy
Although it would appear that lifestyle change might be a key skill of occupational therapy, a review of the literature reveals that research into occupational therapy in diabetes care is sparse, particularly in relation to managing diabetes in the context of everyday life (Pyatak, 2011). It is only recently that occupational therapists have started to consider an occupational perspective. Fritz (2014) examined the influence of daily routines on DSM, while Thompson (2014) considered the need to develop appropriate habits and routines to support self-management. Similarly Pyatak et al. (2015) emphasise the need to integrate self-management behaviours into everyday occupations and routines. Interestingly, it is research in the nursing profession where examples can be found of where participants have discussed how certain occupations are affected by sugar levels or how medication affects routines and habits (Thorne and Paterson, 2001). The use of occupational therapy models could allow an occupational perspective in contrast to a medically based ‘impairment’ focus (Scott et al., 2017).
MOHO
One of the most commonly used models in practice and in research is the MOHO (Lee et al., 2012). The MOHO enables us to understand people as occupational beings and to view them as being situated within dynamic complex systems. The MOHO concepts to explain this complexity include motivation for occupation (volition), routine patterning of occupational behaviour (habituation), nature of skilled performance (performance capacity) and the dynamic influence of the physical and social context (environment) (Kielhofner, 2008). Use of MOHO enables occupational therapists to have a conceptual framework that focuses on understanding occupation (Kielhofner, 2008).
Volition involves a person’s values, their interests and their beliefs in how effective they perceive they are at doing (Kielhofner, 2008). Habituation relates to how a person organises their patterns of behaviour, which are guided by their roles, habits and routines (Kielhofner, 2008). The environment includes immediate, local and global influences as well as corresponding social and cultural effects (Kielhofner, 2008).
The theoretical perspective of MOHO and its application to DSM is the focus of this research article.
Method
The Ethics Committee of the University of Cumbria consented to ethical approval for this study. A qualitative methodology and intuitive inquiry (Anderson, 2004) research design were chosen in order to enable a reflexive and considered exploration of the issues. Intuitive inquiry is described as a qualitative hermeneutical approach, which combines intuition with ‘intellectual precision’ and includes creativity and deep reflection (Anderson, 2004, pp.307). It provides a cohesive structure for the methodological aspects of heuristic phenomenology, interpretative phenomenological analysis, metaphor analysis, discourse analysis, creativity and mixed media artwork.
There were three studies:
Diabetes lived experience (see Youngson et al., 2015), Occupational therapists with diabetes, and Diabetes in relation to the potential occupational therapy role.
For each study a purposive convenience sample of people was sought. This ensured that participants had the particular characteristics required, of living with diabetes, to enable exploration of the themes (Ritchie et al., 2003). The convenience sample was chosen for ease of access. In order to reduce potential bias (Ritchie et al., 2003), a range of ages, types of diabetes and time with the condition were selected. All participants were over the age of 18. Study 1 and study 3 participants were recruited from the general population while study 2 participants were recruited from the occupational therapy profession in the UK (and one from the USA). Participants were provided with an information sheet and written consent was sought prior to participation in the study. Data was collected in all 3 studies using digitally recorded individual, semi-structured interviews of 60–90 minutes duration by the first author. In study 1, participants were asked to describe what it was like to live with diabetes with subsequent questions for further exploration or explanation (Legard et al., 2003). Fuller details of the method from study 1 are reported in Youngson et al. (2015). Study 2 participants were invited to use their own metaphors (Gauntlett, 2007) to describe their experiences of diabetes. This gave an opportunity to further understand the realities of living with diabetes and explore the use of metaphor. Participants were also invited to discuss how they might have used occupational therapy concepts in their own self-management and how it might be applied to others with diabetes, thus enabling an exploration of an occupational therapy perspective. Study 3 participants were also invited to describe what it was like to live with diabetes through creation of their own metaphors, and to consider what kind of diabetes service would help with self-management. Although these studies each had a different focus, the overall findings gave a comprehensive perspective on living with diabetes and thus the data from the three studies was pooled for the purpose of considering the occupation of DSM.
Interviews were transcribed in full and sent to participants for checking. Thematic analysis of the data began with an initial immersion of reading and re-reading the transcripts. Initial codes were applied to each line of transcript in keeping with phenomenological priceiples, from which broad categories were developed (Finlay, 2011). As in the perspective of intuitive inquiry, a number of different strategies including the use of a fieldwork diary, reflection through creative mixed-media artwork and moments of intuition were used alongside the coding to ensure a comprehensive representation of the perspectives of the participants. In each study an analysis of the findings were sent in a report to participants for review and comment. Participants who responded confirmed their agreement and some provided extra feedback in response to the reports. This included further detailed description of their diabetes experiences, which was incorporated into the findings. A further deductive analysis of the data from all three studies was conducted using the concepts and definitions from the MOHO (Kielhofner, 2008) to focus on this theoretical perspective.
Results
Study participants.
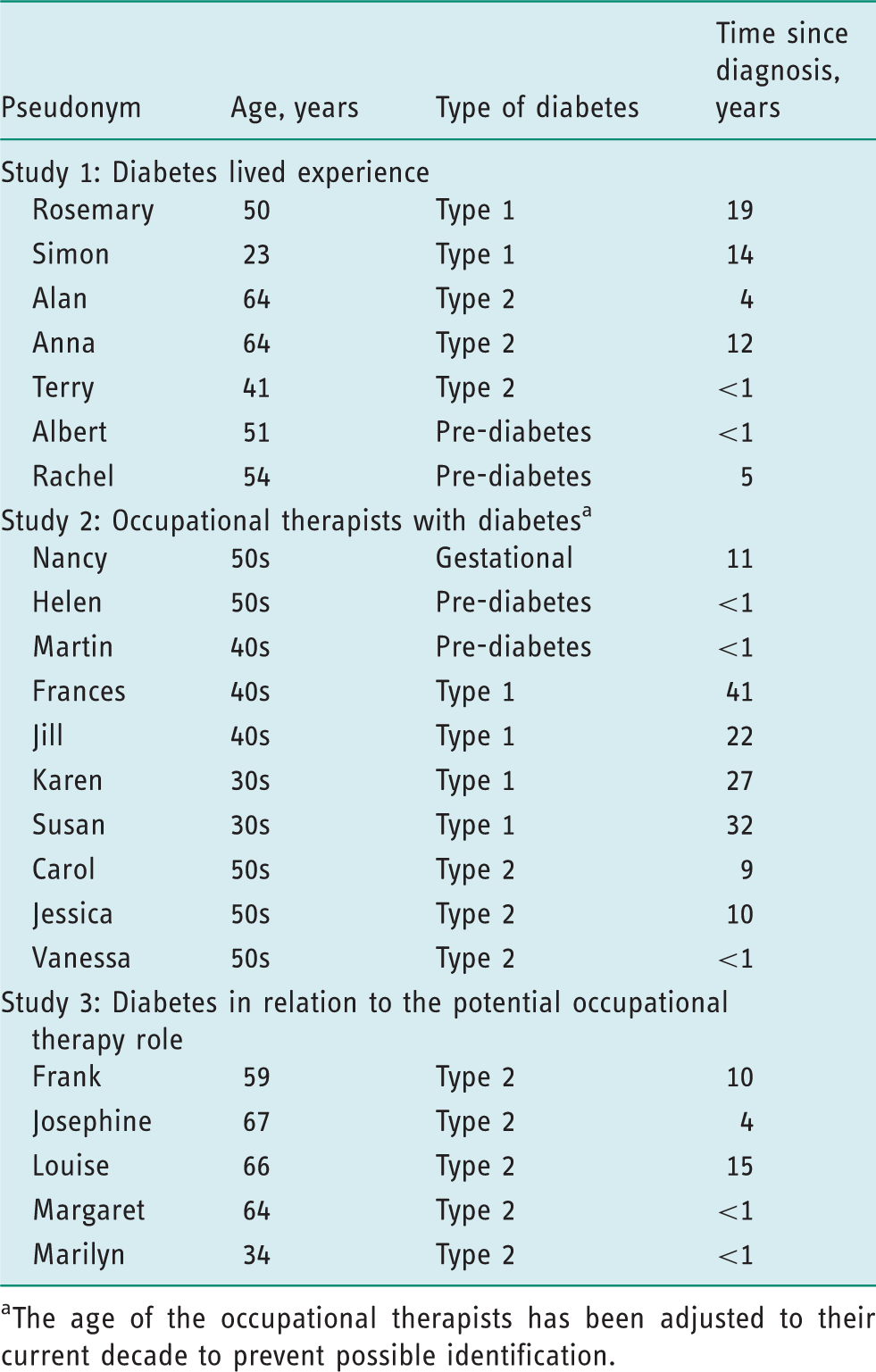
The age of the occupational therapists has been adjusted to their current decade to prevent possible identification.
Studies 1, 2 and 3 all revealed aspects of living with diabetes where participants described the realities of fitting the condition into their daily lives. As shown in Figure 1, the findings are conceptualised, across all participants, into the occupation of DSM aspects of management from type 1, type 2, gestational and pre-diabetes are described and collectively they summarise the experience of the participants into seven inter-related occupational forms. The thinking bubble in the middle indicates the self and the decisions all participants have to make about how, what, why and when they will organise self-management. Starting from top right of Figure 1, and in the direction of the arrows, these seven occupational forms of DSM are summarised alphabetically as follows: managing appointments, managing diet, exercise, information and education, managing other illness, managing medication and testing blood sugar.
The occupational forms of the occupation of diabetes self-management.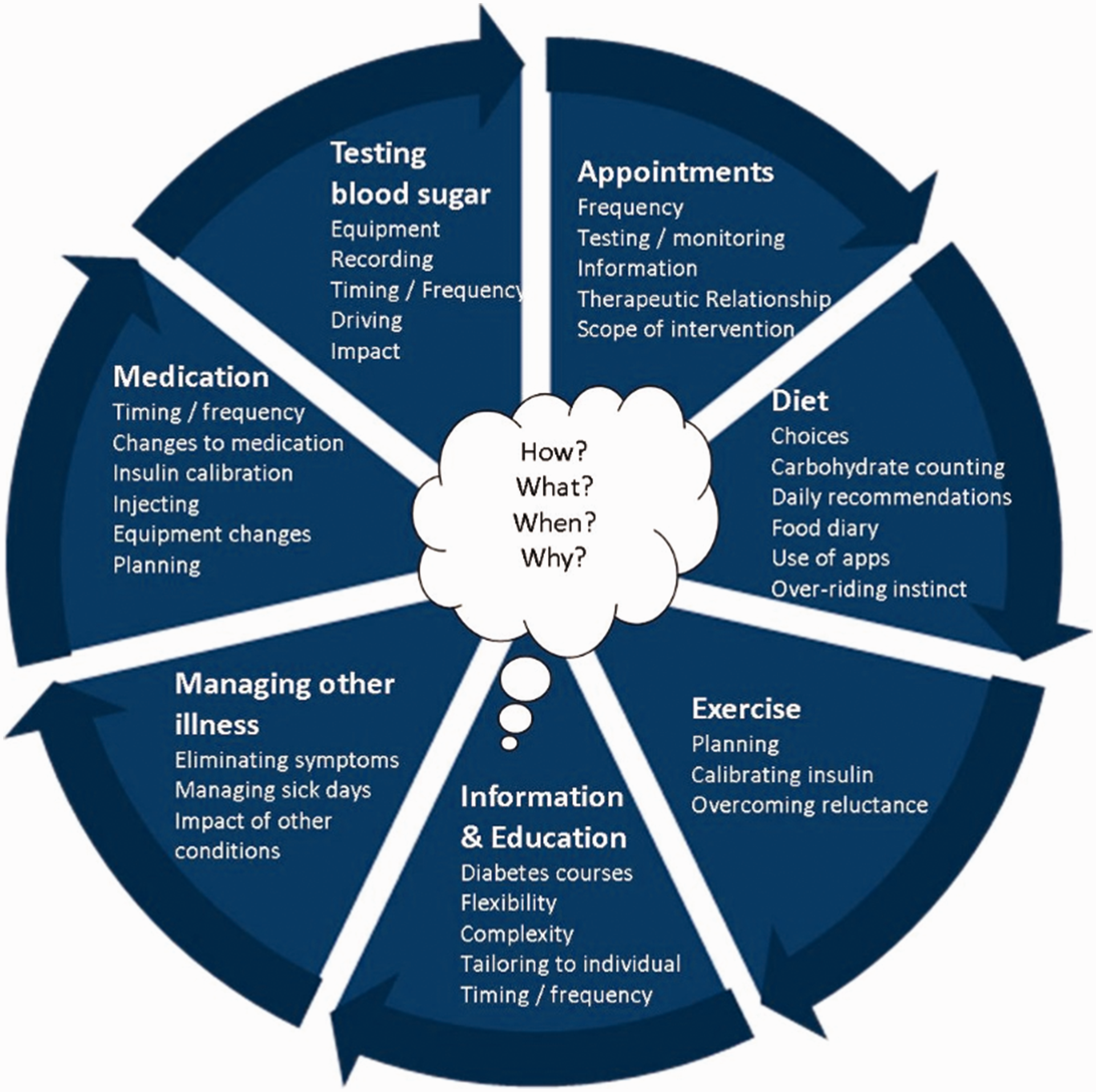
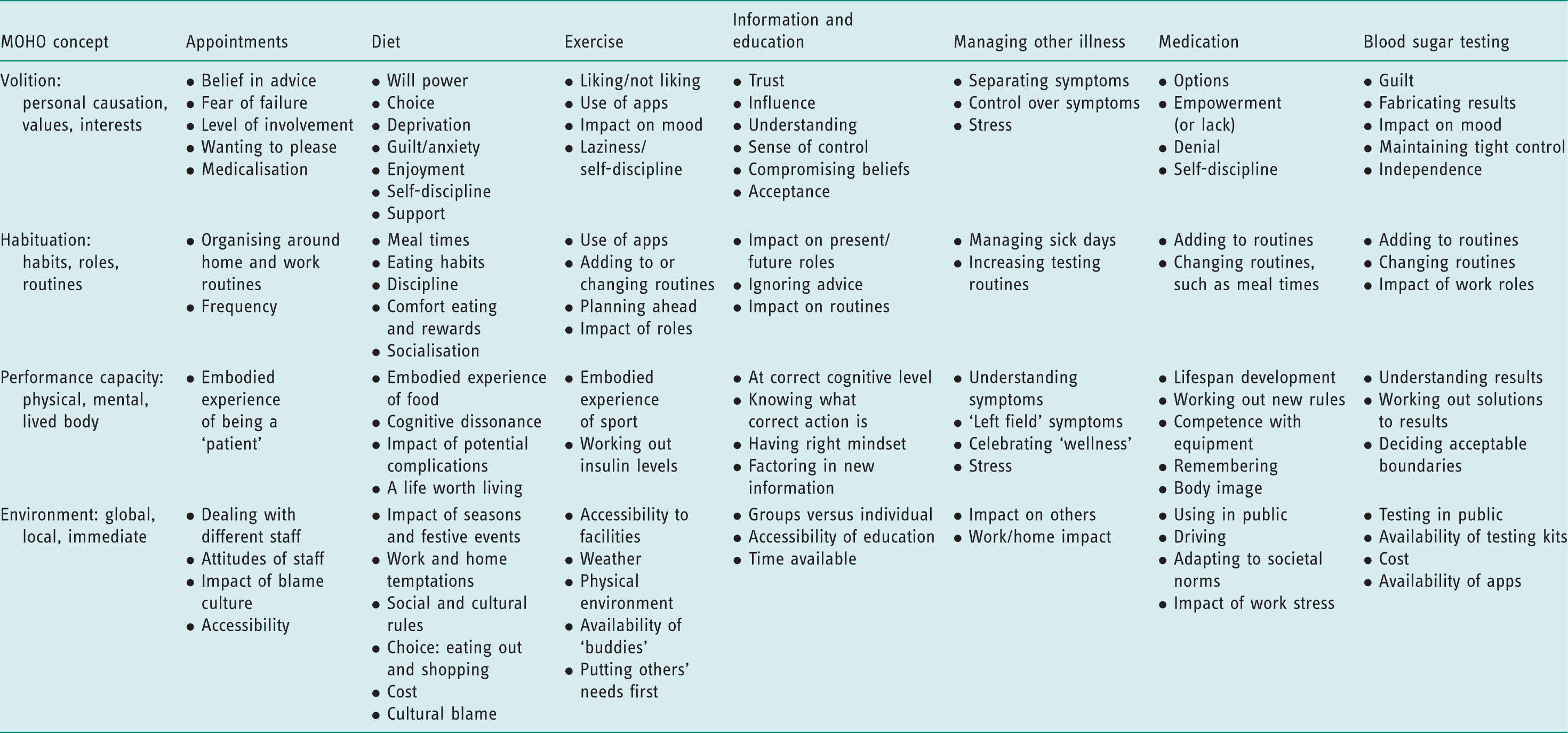
The complexity of this occupation is further broken down into the components of MOHO as summarised in Figure 2 and Table 2. Figure 2 takes one aspect of DSM, blood sugar testing, showing the impact of volition, performance capacity, habituation and environment, using the words of the participants from all three studies.
Using the Model of Human Occupation to illustrate blood sugar testing. Occupation of diabetes self-management in relation to the Model of Human Occupation (MOHO).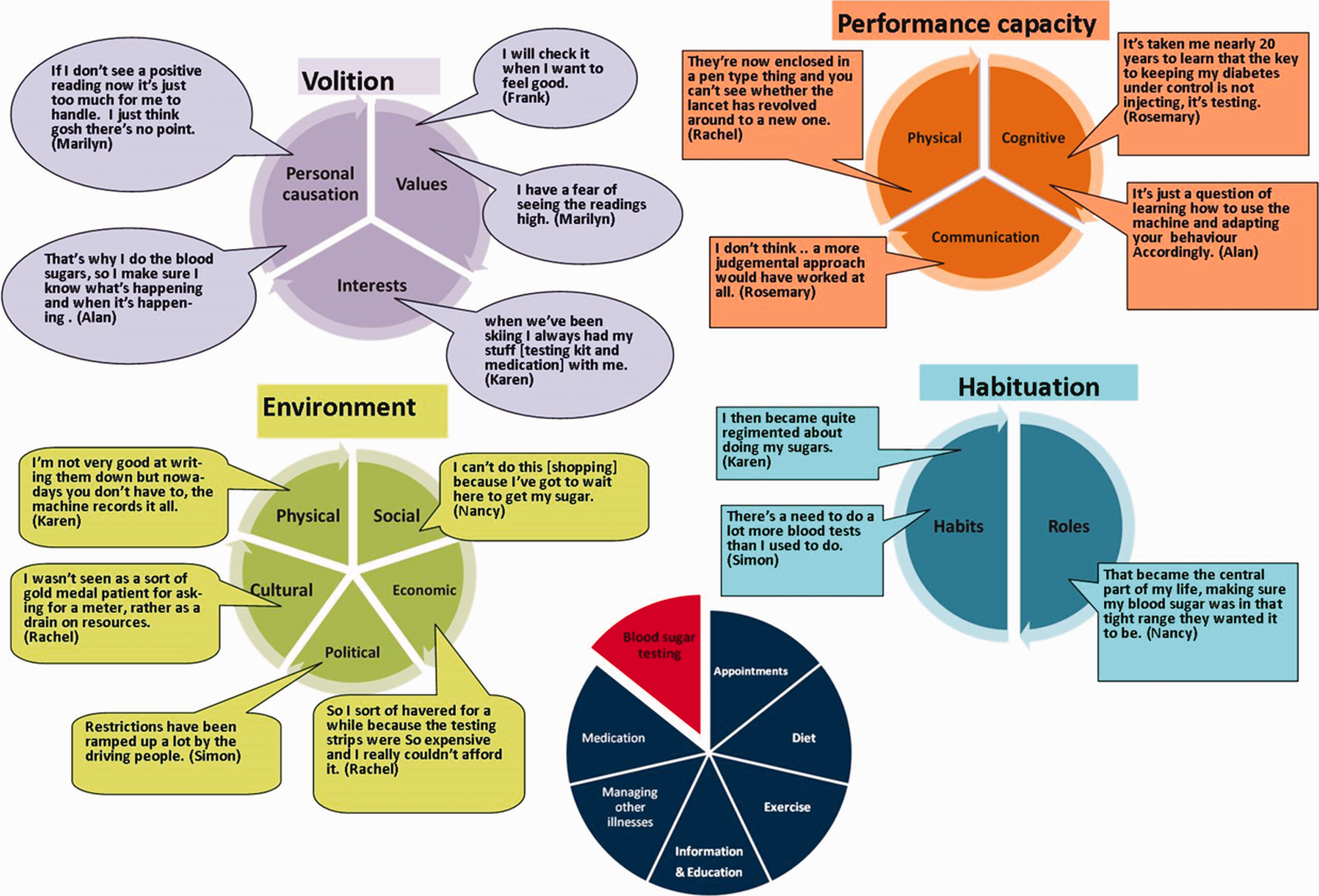
As can be seen from the blood sugar testing example above, this is not merely a physical task, as might be understood from a medical perspective. The formation of new habits is required, it is impacted by job roles (such as the need to test before driving), requires learning, is value laden and is influenced by experience and beliefs.
Table 2 takes a wider perspective on DSM, summarising the MOHO components across the seven occupational forms. MOHO was applied to the findings to further describe the particular aspects of these occupational forms to aid understanding of what motivated participants, how the challenges might be explained in terms of performance capacity, changes to routine or the impact of the wider environment. These are explained in further detail below.
Applying the MOHO to the occcupation of DSM
Volition
The components of volition (personal causation, values and interests) are interwoven and it is the relationship between these components which influences how people assess and manage themselves. For participants their ability to engage with the occupational forms of DSM was bound up with their beliefs about themselves and their trust in professionals. Managing the therapeutic relationship, especially where different professionals were encountered on each appointment, led some to insisting on seeing the same person as ‘I was being given different advice by different people everytime I went’ (Frances). For Frances, dealing with this conflicting information not only impacted on her sense of capacity to manage but was also at odds with her conviction that health professionals should provide clear information to work with.
Appointments involved engaging with the scope of the intervention and managing the required ‘checks and balances’ (Carol) of eyes, feet, blood pressure, blood sugar levels and impact of medication; dealing with information exchange; and managing the frequency of appointments eg too often or not soon enough. Some participants felt that the frequency of appointments did not suit them and the impact of their personal causation was explained in terms of wanting reassurance that they were doing the right thing. Margaret, for example, reported that ‘they leave you, they let you flounder’. Issues of trust, power and communication characterised the therapeutic relationship, with some participants describing that ‘it always felt like going to see the headmistress’ (Jill) and only being ‘given preconceived options’ (Frances). Some participants approached appointments with trepidation, concerned about being judged by professionals or wanting to please by adhering to advice as far as possible. To meet this desire to please, Susan discussed making up blood sugar test results stating that the healthcare staff ‘would look at the book that was completely fabricated’, but that would indicate that she was within the expected range. For all of these participants, the content of appointments or attitudes of professionals had a direct influence on feelings of personal capacity and self-efficacy, and challenged their values about what they considered to be the right course of action.
Correspondingly, changing behaviour as a result of education and information exchange appeared to rely on whether participants trusted the information or whether it actually compromised their beliefs. Information and advice was often seen as negative, ‘it’s very much about you can’t have, you can’t be having this’ (Carol). Others found that courses, such as Dose Adjusted for Normal Eating for type 1 diabetes, had a very positive impact, allowing for more adaptability in diet, which meant that for Jill, ‘I’m now a bit more flexible as to how I can control the diabetes’. Marilyn reported that she wanted to manage her diabetes her way rather than follow the recommended advice. However, she concluded that ‘it was upsetting to see that there wasn’t anything natural I could do and that I had to compromise my own kind of spiritual beliefs really to then treat this condition’. Here, the challenge related to a sense of obligation to acting on the advice. Where this matched the participant’s beliefs and values, there was the possibility for positive change, but where the advice was at odds with these, there was a likelihood of ignoring the information.
Making changes to diet and exercise was particularly bound up with values and interests: many participants felt that they did not have the self-discipline required to make changes, and described their interests around socialising and food. Managing diet, for some, resulted in reduced food choices and feelings of exclusion while shopping for food, and having to make efforts not to give in to temptation. Participants discussed how their diabetes impacted on socialising with friends in terms of trying to make healthy food choices while not inconveniencing dinner party hosts, negotiating the refusal of food gifts, and of feeling a nuisance by spoiling others’ pleasure.
Personal causation was bound up with testing in terms of the emotional (either positive or negative) impact of results. Carol reported her fear of becoming obsessed with testing and Louise stated that she got ‘discouraged’ by the results. Likewise, Marilyn stopped herself testing because ‘if I know the readings are going to be higher I don’t want to confirm it because I know that by confirming it my morale drops’.
Overall, getting into the right ‘headspace’, or positive personal causation, was seen as key. As Terry reported ‘I’ve got to be in the right frame of mind…because no amount of just telling me “if you don’t do this your leg’s going to drop off” is going to work.’ While Anna similarly stated that ‘I think you’ve got to be at a place where you think “I really do have to do something”’.
Habituation
The summary in Table 2 indicates the effects of habits, routines and roles across all the occupational forms and highlights that some participants prioritised work and family life ahead of their own self-management. Some participants discussed the difficulty of fitting appointments around home and work routines as well as the need to change routines around food, exercise and testing. Participants had to learn to override the habit to eat when stressed, change meal routines in relation to medication. Helen described changing habitual meal time routines with her family to ensure smaller portion sizes ‘And the only way I could control them…was to give them a smaller plate and then they got it better’. Martin reported his habit of eating to control stress and to reward himself but stated that food had become his ‘downfall’.
Simon explained how his routines developed into a non-testing habit, ‘I should worry more, I should do more blood tests and get everything under control more but I guess you know, having been for so long, maybe not getting there quite as quickly as I should have, maybe I’ve kind of got into that habit’.
Routines required changing and sometimes careful planning. Jill described having to plan medication and sugar supplies to cover possibilities of hypoglycaemia, as ‘it’s quite hard to get things like blood sugars right on long [bicycle] rides’.
Some found exercise had a very positive impact on their diabetes, such as Susan, who found sport to be ‘my medicine’ but others found routines hard to sustain. Participants had to over-come exercise reluctance, such as Louise, who stated ‘I know I ought to do more exercise, I hate exercise’ and Margaret, who said that it had been recommended to her that she join a fitness class but that this had not been part of her usual routine as ‘I’ve never fancied gyms, I don’t like them’.
Performance capacity
Performance capacity relates to the physical and cognitive components that enable people to perform occupations, as well as the subjective ‘lived body’ experience. As summarised in Table 2, participants talked about the understanding of physical symptoms, the physical difficulties of using some testing equipment and the cognitive ability required to work out medical equipment and understand results. Medication management formed a major part of DSM for the participants. In terms of performance capacity this involved working out timing of medication, dealing with changes to medication and possible risk factors, incorporating new equipment, calibrating insulin amounts in relation to diet and exercise, making choices about where and when to inject. Jill struggled with ‘phases where I just forget to take my insulin’. This required participants to be aware of their safety limits and planning beforehand to ensure adequate supplies of medication or emergency glucose.
Performance capacity was of concern not just in the present, but also when considering the future. Carol and Terry reported that they did not think they could cope with the possibility of having to physically inject insulin in the future, while Frances reported ‘I know I can never do an insulin pump’.
Although diabetes education is seen as the cornerstone of prevention and treatment, participants described difficulties with courses being tailored to their own cognitive levels. Some, like Frank, found education patronising ‘I found the level of information was quite low’, while others found it too complex.
Several participants discussed the difficulty of distinguishing between diabetes symptoms and the symptoms of other illnesses and how this affected medication or making adjustments to DSM. As Alan explained, ‘I only really check my blood glucose if I’m feeling unwell and I want to, by a process of elimination, work out that it’s not my diabetes’. Karen similarly stated that ‘if I feel funny I will do more tests’ even when she attributed this to tiredness. Frances commented that hypos might well be due to ‘a period or 90 million reasons and you can’t control every one of them’. Additionally, participants felt the need to check out symptoms to ensure that complications of diabetes were not developing.
The embodied experience of being a ‘patient’ was particularly pertinent here. As Frank stated, ‘I don’t want to be good at being a patient’, explaining that ‘whilst I might be a patient…. outside this office…. I’m not your patient, I’m my life’.
Environment
The environment includes the physical, social, cultural, economic and political contexts that affect occupation. Figure 2 and Table 2 give examples of the impact of positive and negative aspects of the environment on DSM. One notable example of this was the impact of blame culture. Frank reported that ‘I think people blame…. you’re a burden on the NHS’, while Jill commented that ‘to attach value judgements to food is a really dangerous place to be’. Louise discussed the difficulty of ‘constantly struggling with weight’ and how it was ‘a curse especially in the age in which we live where physical appearance is so criticised’.
The lack of available facilities in the physical environment constrained how well DSM was managed. Jill commented that she did not always have access to somewhere to inject and that it had taken her a long time to feel able to do this in public, being sensitive to the needs of others, ‘I used to think you couldn’t inject in public because it might upset someone’. In the same way, the local environment in terms of the availability of leisure facilities, access to footpaths or difficulty of managing hillly terrain all affected DSM.
Discussion
DSM needs to be accomplished in the context of the person’s lifestyle, it being only one aspect of the complexity of managing daily lives (Fritz, 2014; Gillibrand and Flynn, 2001). Conceptualising DSM as an occupation with seven occupational forms allows further understanding of the many aspects that require successful management. The occupational forms of the occupation of DSM change with time, experience and other life events of the people concerned (Pyatak et al., 2015). Considering diabetes from an occupational perspective differs from the traditional medical view of self-management tasks by taking into consideration the individual in the context of their own daily life. Using MOHO further explains how the occupational identity of the person; their choices, beliefs, values and interests; their habits, roles and performance capacities; and the opportunities or demands of the environment impact on that self-management. This supports the findings of Thompson (2014), who considered the need to develop appropriate habits and routines to support self-management. Pyatak et al. (2015) similarly emphasised the need to integrate self-management into everyday occupations and routines.
Although the diabetes literature highlights managing the therapeutic relationship (Thorne and Paterson, 2001), the importance of testing and recording (Ingadottir and Halldorsdottir, 2008), information exchange (Watts et al., 2010), diet (Brackenridge and Swenson, 2004), exercise (Nagelkerk et al., 2006) and medication (WHO, 2016), it was clear from the participants that how successful they were with these occupational forms was bound up in values and interests. Managing diet, for some, resulted in reduced food choices and feelings of exclusion while shopping for food and having to make efforts not to give in to temptation, as found by Wellard et al. (2008). Amorim et al. (2014) describe the emotional impact of diabetes on identity and the participants here discussed how their diabetes impacted on socialising with friends in terms of trying to make healthy food choices while not inconveniencing dinner party hosts, negotiating the refusal of food gifts and of feeling a nuisance or spoiling others’ pleasure.
As stated in the findings, participants talked about the physical understanding of symptoms and the cognitive ability required to work out medical equipment and understand results, highlighted by Montez and Karner (2005), requiring participants to be aware of their safety limits and planning beforehand to ensure adequate supplies of medication or emergency glucose. This was clearly associated with roles and routines as well as personal causation.
Overall, dealing with the culture of blame across these occupational forms added another layer of difficulty for the participants. Browne et al. (2013) discuss the negative impact of stigma and how negative or oversimplified views of diabetes can be experienced from friends, society in general, the media and healthcare professionals. Participants described how unhelpful and demotivating this culture of blame could be. Being censured by healthcare professionals for apparent lack of control of blood sugars (Ingadottir and Halldorsdottir, 2008) was not only seen as frustrating and disempowering but also counterproductive.
As Gardener et al. (2017) argue, successful DSM requires a complex skill set. They suggest that occupational therapists have a role to play in enabling people to achieve mastery of DSM by understanding the occupational performance elements. Conceptualising DSM as an occupation and understanding the complex dynamic between the person, occupation and environment, using the MOHO, could be one way of highlighting the unique occupational therapy perspective.
Limitations
The sample size of 22 participants means that the findings cannot be generalised to the diabetes population as a whole. However, the study does give some insight into the complexity of managing DSM and provides an occupational perspective that could complement existing services. Further research will be required to investigate whether this theoretical perspective would work in practice and how this might be used to design effective occupational therapy interventions.
The research is also limited in terms of its focus on the individual with diabetes. It is clear that DSM also relies on effective policy in terms of access to healthcare, education and guidance in many aspects of the occupational forms described, such as education and information, diet and physical activity. Further research is required into the impact of public health and health promotion opportunities on these occupational forms.
Conclusion
People can live long and healthy lives if diabetes is well managed and type 2 diabetes can be prevented with lifestyle changes to diet and exercise to control blood sugar levels (WHO, 2016). Within healthcare, this is currently managed through medication, health education and follow-up, with a focus on the biomedical approach.
The purpose of this study was to understand the experience of DSM and to explore the potential role for occupational therapy. Within this the MOHO was considered as a way of conceptualising and understanding the complexity of the occupation of DSM with its seven inter-related occupational forms. This has highlighted the complexity of an individual managing DSM in the context of their own lives and the multiple and complex systems that this entails, which goes beyond the biomedical approach. This increases the knowledge base with specific reference to DSM and occupation. This approach could strengthen an occupation-based occupational therapy intervention, which is different to, yet complements current medical practice in DSM.
This study, embedded in the experiences of those with diabetes, suggests that there is a role for occupational therapy in DSM, and that occupational therapy has a distinct role through seeing this self-management as an occupation.
WHO (2016: pp.53) concludes in its Global Report on Diabetes that ‘a range of health professionals is required for the care and treatment of diabetes, including physicians, nurses, dieticians and specialists such as obstetricians, ophthalmologists, vascular surgeons and physiotherapists’. It is time that occupational therapists were added to this list.
Key findings
Diabetes self-management can be conceptualised as an occupation. Occupational therapy has a distinct role through seeing self-management as an occupation. The Model of Human Occupation enables understanding of the occupational forms of diabetes self-management.
What the study has added
Conceptualising diabetes self-management as an occupation may enable occupational therapists to facilitate successful engagement in this occupation.
Footnotes
Acknowledgements
I would like to thank all the participants for their time and enthusiasm in sharing their experiences of diabetes. I would also like to thank my supervision team, Diane Cox, Helen Wilby and Fiona Cole, for all their support. Finally, I would like to thank the reviewers for the extremely helpful detailed and considered responses in their feedback to help shape this article.
Research ethics
Ethical approval was obtained from the University of Cumbria, approval numbers 12/13 (2013), 12/49 (2013) and 13/11 (2014).
Consent
All participants provided written informed consent to be interviewed for this study.
Declaration of conflicting interests
None declared.
Funding
The author received no financial support for the research, authorship and/or publication of this article.