
Abstract
Introduction
The importance of values in occupational therapy is generally agreed; however, there is no consensus about their nature or their influence on practice. It is widely assumed that occupational therapists hold and act on a body of shared values, yet there is a lack of evidence to support this.
Method
The research tested the hypothesis that occupational therapists’ responses to ethically challenging situations would reveal common values specific to the occupational therapy profession. A total of 156 occupational therapists were asked to decide what should be done in five common-place yet ethically complex situations, presented as scenarios for debate.
Results
The results show that while most occupational therapists share very general values, they frequently disagree about what to do in practice situations, often justifying their choices with different and sometimes conflicting specific values. In some cases, the same respondents espouse contradictory values in similar situations.
Conclusion
The extensive literature about decision-making – together with the study’s results – confirm that when occupational therapists make decisions, they draw on multiple factors, consciously and unconsciously. These factors vary between individuals. Value judgements are one part only of a complex process which includes personal experience, intuition, social influences, culture, psychological influences and relationships with both colleagues and clients.
Introduction
It is widely believed that professionals should practise according to ‘shared values’ such as the National Health Service (NHS) core values (NHS, 2015). ‘Values-based practice’, ‘values-based mission statements’ and ‘values-based recruitment’ are commonly considered basic requirements for ethical practice (Francis, 2013; HEE, 2014). Yet at the same time there is no consensus among theorists about what values are, and no empirical evidence that professionals actually hold, or act on, shared values (Seedhouse, 2005, 2009).
Some theorists equate values with ‘needs, wishes and preferences’ (Brecher, 2014; Fulford, 2011; Wright-St Clair and Newcombe, 2014), others see them as ‘commitments, goals, desires, interests and perspectives (including moral perspectives)’ (Loughlin, 2014: ix), while others characterise them as ‘enduring beliefs which a person holds about what is good or desirable in life’ (Rokeach, 1973). One occupational therapist asserts that a value is neither a belief, nor attitude, nor principle, for example, but ‘an abstract, evaluative concept that serves to determine the ethical validity of an attitude, action or situation’ (Drolet, 2014; 7). These and many other perspectives on values have been discussed, and challenged, by various theorists over the past 50 years with no clear consensus or definition (Allport, 1961; Fulford, 2008; Loughlin, 2002, 2014; Loughlin and Miles, 2015; Loughlin et al., 2018; Rokeach, 1973; Seedhouse, 2005; Veatch, 1995).
Values in occupational therapy literature
The Royal College of Occupational Therapists (RCOT) has attempted to identify the professional values and behaviours expected of its members in its professional standards and code of ethics and professional conduct (RCOT, 2015, 2017). These values include: occupational focus (‘promote participation’); service-user centred; work within professional competence, develop professional competence; team work; communicate respectfully; efficiency and sustainability; and manage risks. The RCOT believes ‘occupation and activity are fundamental to a person’s health and well-being’ (RCOT, 2017: 2) and prioritises respectful communication and professional competence (RCOT, 2017).
However, a recent review of values in the occupational therapy literature (Drolet, 2014) notes that most of the profession’s value statements lack an evidence base and are compiled only from professional association documents and/or the personal opinions of occupational therapy scholars. This being so, there are inevitable conflicts within the profession. For instance, the American Occupational Therapy Association (AOTA) identifies seven core values of occupational therapy practice – altruism, equality, freedom, justice, dignity, truth, and prudence (AOTA, 1993, 2015). These values have been challenged as culturally specific, denying alternative global contexts in which occupational therapy is practised (Hocking et al., 1995). The reaction of occupational therapy theorists to this sort of criticism has been to suggest yet further values, for example, courage, imagination, resilience, integrity and mindfulness (Peloquin, 2007). One study identified 61 values perceived to be ‘essential’ in occupational therapy (Aguilar et al., 2013). Clearly, opinions on occupational therapy values differ greatly (Drolet, 2014; Wright-St Clair and Newcombe, 2014).
Four recent studies on values in occupational therapy practice have used different methodologies including interviews (Aguilar et al., 2012; Drolet and Désormeaux-Moreau, 2016), Delphi technique (Aguilar et al., 2013) and an experimental mixed methods design using the Values Exchange (VX) (Wright-St Clair and Newcombe, 2014). Three of the studies relied on occupational therapists reporting the values they consider to be important, while the fourth used a case scenario for participants to judge, based on a common practice dilemma (Wright-St Clair and Newcombe, 2014). The findings of this latter study were that the occupational therapists involved disagreed about what to do in the scenario and used diverse values in their decision-making, suggesting both that there is no simple set of professional values in occupational therapy, and that occupational therapists’ personal values are integrated in their professional decision-making.
Method
An exploratory sequential mixed methods approach was taken. Ethical approval for the study was obtained through the University of Worcester. The study comprised three phases: phase 1 aimed to develop five practice-based scenarios which would comprise the data collection tool for phase 2; phase 2 aimed to elicit the values of practising occupational therapists through a dedicated online forum (VX); phase 3 aimed to identify strategies for translating the study findings for education and practice through a series of focus groups.
Phase 1: scenario development
Building on a previous study (Wright-St Clair and Newcombe, 2014) which focused on one practice scenario in a community setting, a series of scenarios reflecting the diversity of occupational therapy practice was required for this study. The initial phase of this study involved a purposive group of six practising (or recently retired) occupational therapists with experience in a range of practice settings, four service users and four researchers, to ensure the scenarios captured clients’ and occupational therapists’ perceptions. Invitations to a half-day workshop, together with information regarding the study aims, were sent directly to occupational therapist contacts known to the first author and chosen because of their specific knowledge and broad range of experience of occupational therapy. In addition requests were sent to three senior occupational therapists in local NHS trusts for nominations from specific areas of practice. Invitations to service users were sent through the University of Worcester IMPACT group. The ethics committee advised that phase one participants did not require consent forms, as this phase was considered preparatory to the main study.
The workshop began with an introduction to the concept of values in occupational therapy practice and a discussion about values in occupational therapy. Participants worked in small groups to discuss potential scenarios that would highlight a professional dilemma. The development of the scenarios was based on discussions of participants’ experiences and shared understandings of situations where client and therapist’ values can conflict.
Each scenario gave a clear description of a complex but recognisable practice dilemma, involving a specific client. The client’s and family’s opinions, and other considerations that might influence the occupational therapist’s course of action, were included. Figure 1 provides an example of one of the scenarios agreed by the team, as it appears on the website.
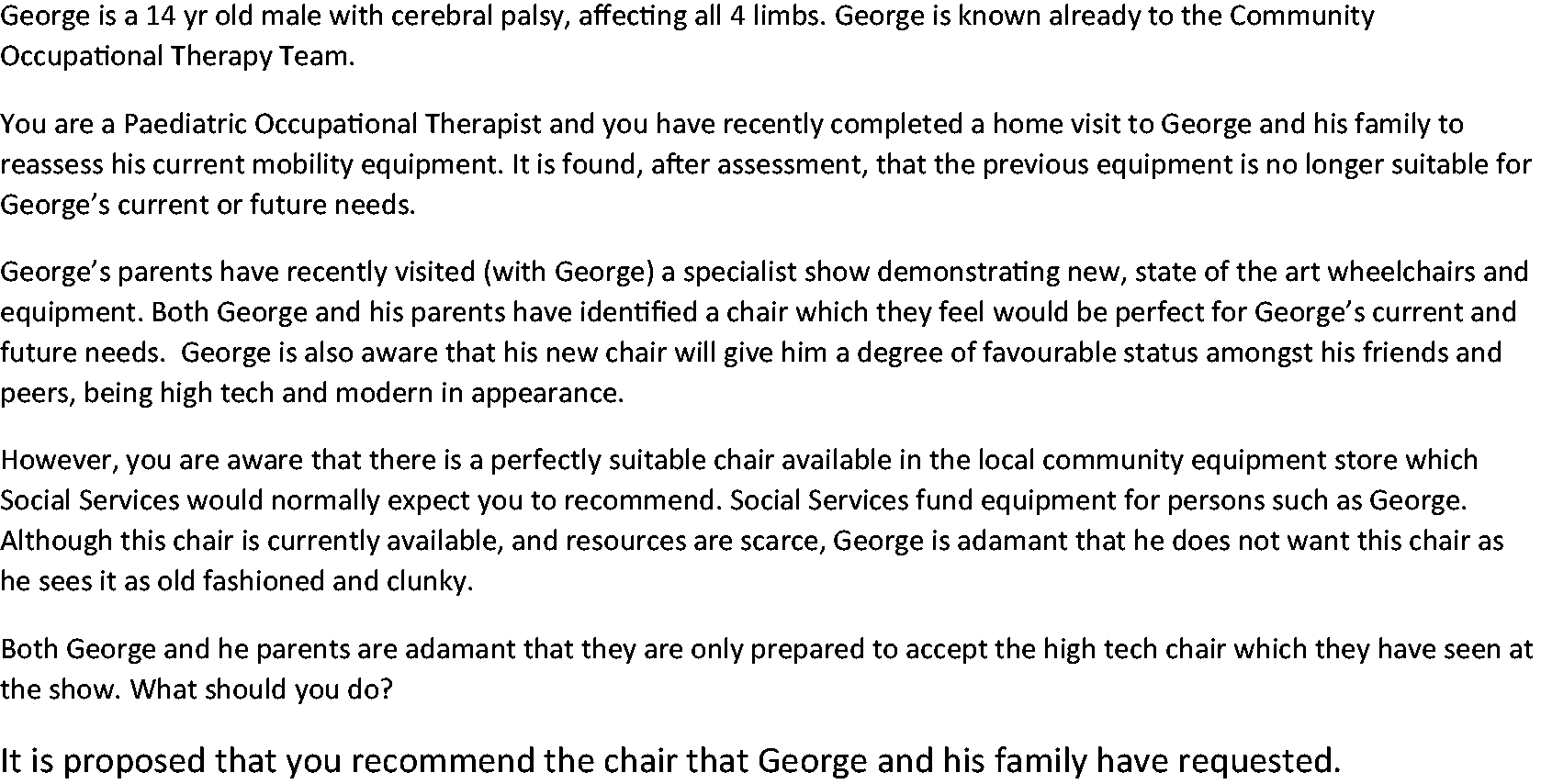
George.
It was assumed that the inclusion of practising occupational therapists and service users in the development of the scenarios would increase the validity of the data collection. Consequently, the researchers worked closely with participants to ensure that the scenarios were consistent with current health service provision and based on occupational therapists’ and service users’ experience. A proposal for action, to which respondents’ could agree or disagree, was made for each scenario.
Phase 2: online data collection
The scenarios formed the data collection tool for phase 2. Initially six scenarios were uploaded to a dedicated group page on the VX http://otresearch.vxcommunity.com/. The VX has been collecting data about healthcare decision-making for over 16 years and hosts over half a million unique responses to dilemmas, many of which are in the public domain. The VX has been used in education internationally for teaching and assessment of values-based decision-making (Godbold and Lees, 2013, 2016; McInerney and Lees, 2018) and for research (Wright-St Clair and Newcombe, 2014). It has proved to be a reliable and easily accessible on-line forum for ethical debate.
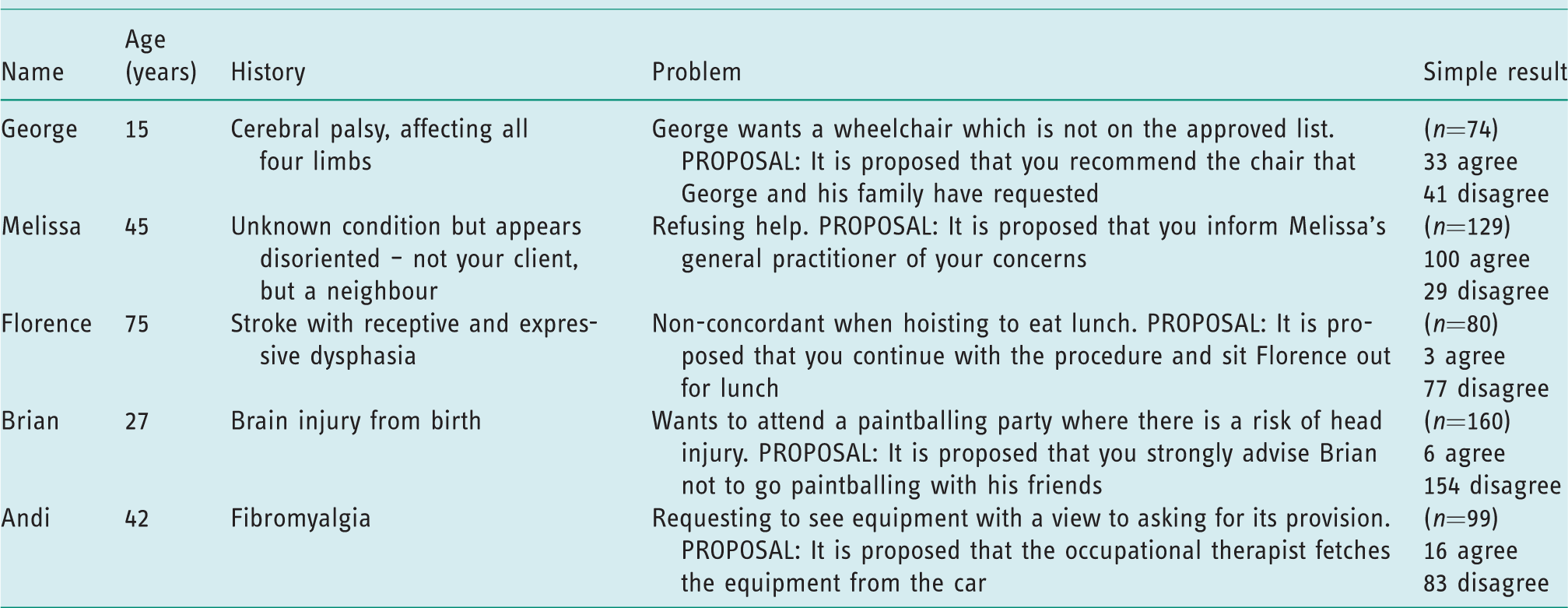
Both the use of the VX website and the six scenarios were piloted. Over a period of four weeks, the workshop participants were invited to log on to the VX website, pilot the process of polling, providing brief rationales to support their decisions, discussing the scenarios, and make suggestions for editing the wording and layout. A photograph for each scenario was downloaded from the internet and included in the scenario layout. The piloting process allowed each participant to make responses to the scenarios and to discuss their rationales online. During the piloting period the final five scenarios were selected for the study (see Table 1). One scenario did not generate a lot of discussion, the solution appeared simple and clear to all and it did not therefore elicit the data on values that underpinned the proposed action leading to the group deciding that this scenario should be removed.
Summary of five scenarios and polling results.
Following the pilot period, occupational therapists from across the UK and from a broad range of practice settings were recruited through social media to respond to the scenarios.
Phase 2 of the study required participants to register on the dedicated group page, where information on the study’s aims and a consent form were provided. Participants were asked to provide basic demographic data and choose a pseudonym with which to participate, if they wanted to maintain anonymity. Occupational therapists were recruited from a range of practice settings. Respondents were asked to consider the five scenarios and independently explain and justify what they would do.
Analysis of the findings occurred in two ways. Initially the results of the polls were considered, and where appropriate the demographic data of respondents who agreed and disagreed with each proposal were compared. It is important to note that agreement or disagreement with the proposal does not necessarily indicate the values that underpin individual respondents’ decisions. Instead inductive analysis of the qualitative data, provided in participants’ rationales and discussion threads explored the values (or preferences) behind the decision-making process. A process of thematic analysis was conducted by the first author, using a process of initial coding and categorisation, to elicit themes (Braun and Clarke, 2006).
Phase 3: knowledge translation
The results of phase 2 were used to generate strategies for knowledge translation through education of students and practising occupational therapists. The results of this final phase of the research are not included in this article and will be the basis of further publications. A series of focus groups including practising occupational therapists and service users were conducted in various locations across the UK. Invitations to participate in the focus groups were sent to all participants of phase 2 and via social media to occupational therapists across the UK. Participant information and consent forms were sent to all respondents prior to the focus group and consent confirmed before the group commenced. Focus groups included a brief summary of the findings and a semi-structured format to generate strategies for knowledge translation. The focus group discussions were digitally recorded, and key points were agreed and documented throughout the discussions. Transcriptions of the discussion, together with the written documents, were analysed thematically to identify strategies for pre and post-registration education.
This article presents the results of phase 1, together with the preliminary results from phase 2. Further analysis of the results of phase 2 and phase 3 will be published separately.
Results
A total of 160 occupational therapists registered in this phase of the study and completed the first scenario (Brian) as they appeared on the site. Participant numbers for the other scenarios varied; some participants did not complete all five scenarios. The response rate for each scenario and polling results are shown in Table 1.
Of the 160 participants; 150 were women and 10 were men, representing the gender imbalance within the occupational therapy profession. Participants had a wide range of practice experience, as indicated by the years since qualification, 70 participants had between 0 and 10 years since qualifying, while 15 had between 31 and 40 years since qualification (see Table 2). Participants also indicated their current practice areas, which were grouped together into hospital, community and non-clinical to allow for comparisons. The study involved participants from a wide range of practice areas; 54 respondents worked in hospital settings, 78 worked in the community, 13 worked in non-clinical settings and 15 indicated ‘other setting’ (see Table 3).
Respondents’ years since qualification.

Participants’ areas of practice.

For each scenario participants were presented with online polls using a Likert scale with ‘agree strongly’, ‘agree’, ‘disagree’ and ‘disagree strongly’ choices. The results of the polls are shown in Table 1. Participants provided their rationales and opinions as free text comments, which were visible to other respondents, which allowed for online discussion and debate. In addition two scenarios (Florence and George) were presented as VX ‘cases’, and offered respondents further opportunity to explore their ideas and values by responding to visual prompts (think screens) and clicking on a number of pre-set options. Think screen 1 asked ‘Who matters most?’ Think screen 2 provides six possible reactions to the scenario including dignity, your feelings, your role, law, risk, and rights. Participants are asked to pick any that apply (i.e. that help you say what you really want to) and there were additional prompts to identify what underlies the choice. Think screen 3 asked participants to identify reasons, and what alternatives might be pursued. Each screen included comment boxes for participants to add free text. The think screens aimed to promote further self-enquiry to identify individual views – they did not provide a pre-selected range of values. After submitting their views, respondents were able to comment on each other’s responses in unlimited conversation threads. A total of 553 unique responses were received for the five situations.
The results of the polling show high agreement among participants for two scenarios; Florence and Brian. In both scenarios most participants disagreed with the proposal to go against the client’s desires and perceived wishes, lending some credence to the view that occupational therapists are sensitive to clients’ values and work in creative ways to respect client autonomy.
However, this is not the same for the other three scenarios, George, Melissa and Andi. Further exploration of the responses to these demonstrates the complexity of occupational therapy decisions, revealing a range of values and influences.
Examples of occupational therapists using divergent values
Preliminary results provide clear evidence that participants in this study used divergent values to underpin decision-making. The following examples highlight the fact that, as professionals, occupational therapists differ in respecting client values.
The polling results for George’s request for a non-standard wheelchair demonstrate the lowest level of consensus, with a 45:55 split among 74 participants. Comparison of respondents based on years since qualification and area of practice demonstrate little difference between those that agreed and those who disagreed, although a higher proportion of participants with 21–30 years of experience, i.e. those with arguably most experience, were more likely to disagree, than those with less experience. Interestingly, participants working in the community were more likely to disagree than those working in hospitals. However, it is important to note that the low numbers of respondents in each group suggests caution in interpreting these trends.
Analysis of the qualitative data suggests that for those who disagreed with the proposal (to recommend the chair George and his family requested) sensitivity to and respect for the client’s values was overridden by a duty to administer interventions in adherence with organisational policy; for example: I could not justify recommending something just because it is what the client and his parents want. (OT A) The duty to the service and equity of treatment to all. I cannot recommend a more expensive item if it offers no other benefits than status for George. I would recommend the old-fashioned chair from the stores, with the proviso that George and family can purchase the modern chair if they so wish. (OT B) Both chairs are considered to meet George’s physical needs. The one they have chosen also helps George to maintain his confidence and access meaningful occupation as a teenager as he develops through this emotionally challenging period. Parents can be assured that this need is met and the chair is likely to last him longer than the aged chair in stock. (OT C)
For Andi and Melissa, the polls showed a higher level of consensus with an 80%:20% split, although interestingly most participants decided against the expressed wishes of the client, giving a variety of justifications for their decisions. In justifying the decision to go against the clients’ wishes, occupational therapists provided alternative ways of meeting clients’ assumed needs, based on the occupational therapy role and the client’s diagnosis.
For instance, for Andi, who had requested ADL equipment: I would explain that our ethos, in most circumstances, is to help people maintain as much independence as possible and in this instance, being functionally active without equipment may assist with pain/mood. Equipment provision may ultimately lower feelings of self-efficacy and foster an overreliance. I would explain that better long-term outcomes are more likely to be achieved through engagement with various treatments/therapies. (OT D) Although Andi has a choice, it is not our role as an OT to simply be dictated to. Equipment is prescribed for someone based on an assessment of need, so if she is not deemed at this moment in time to need such equipment then giving it to her will only lead her to conform/adapt to a disability role, which is the opposite of what our profession promotes. (OT E) A meaningful conversation about equipment would, in my view, be enhanced by having some equipment in the house to look at, talk about and try out. Otherwise it is all just a theoretical discussion with the OT holding the power over what an individual feels may help her. I would be extremely uncomfortable with this. (OT P) I have a duty to report my concerns, not as an OT but as a member of the public, and neighbour. There is no confidentiality being breached and even if there was, I would argue that information was passed on in the best interests of the person. (OT H) I feel I would have a duty of care as a neighbour regardless of my profession, but working as an OT I feel I would be negligent if I did not alert her GP/local authorities. (OT I) If I was the OT I feel that as her neighbour it’s really the only course of action available to me – in the circumstances I don’t feel I could go along with her request for me to do nothing. (OT J) She needs appropriate help. I couldn’t ignore the fact she is looking so unwell and at risk. (OT K) As far as we are aware the lady is able to make decisions about her own welfare. She has made it clear that she doesn’t want you involved. Although I would naturally feel concern for my neighbour I am not a family member and the GP may not be able to discuss his patient with me. (OT P) I think it is Melissa’s decision to contact her GP to seek advice and support. (OT M) I don’t have a professional relationship with Melissa, she is not and never has been my client, she is a neighbour…. I can’t imagine it being appropriate for me to contact her GP. (OT N) I would not feel comfortable making a referral to a healthcare practitioner without her consent. I also think that what the GP can do with this information is really limited, given that she is not consenting to see the Dr herself. (OT O)
Examples of the same participant using divergent values in similar situations
Across the five scenarios, analysis of the results indicate that respondents’ application of values is divergent not only between participants in the group, but also with the same participant across different scenarios. The following example shows how a respondent may in one case perceive a clear duty to meet a client’s expressed need but not in another similar case.
One participant (OT F) was clearly sympathetic with George and his family’s values and supported their choice because of the aesthetic properties of the chair, the psychological impact and valued a holistic approach: The other chair that is funded will meet George’s physical needs yes, but what about his other needs? His emotional developmental needs? His new and emerging identity and role as he emerges into a teenager? That is why he wants a ‘cool’ and high tech chair. Image is and will be important to him. We are holistic OT’s; that is what we need to think about. I believe that Andi wants equipment because it will ‘look’ like she has an illness and therefore feel more ‘validated/affirmed‘ by others as stated above. We are a very visual disability culture – if you don’t see aids/adaptations then ‘they don’t have a disability’…. I have a professional duty to meet needs in a manner that is acceptable to the client. I may offer to bring some equipment at the next appointment to try if these were standard items from the loan store, but would be cautious about arranging a demo with a non-standard item if I was not sure I could justify the need for a special purchase…
Discussion
The study aimed to explore the professional values that underpin decision-making in occupational therapy practice, though eliciting responses to five specifically designed scenarios. The collective responses of 160 occupational therapists were analysed, and show that occupational therapists’ decision-making is dependent on a range of factors, creating divergent responses in some situations. Further analysis of these differences demonstrates that, despite the profession having a shared knowledge base and a common culture of ‘enabling’, much is open to personal interpretation. Similar to Wright-St Clair and Newcombe (2014) this study demonstrates that occupational therapists make divergent decisions about practical situations, indicating variation in how our common professional knowledge and philosophy is applied. A lack of consensus between members of the same profession is not surprising, when considering the multitude of factors that frequently need to be considered in practice.
Further analysis demonstrated divergence in the rationales between occupational therapists and at times also the same occupational therapists demonstrated divergence across different scenarios. It is evident that occupational therapists do not consistently apply particular professional values in decision-making. One example of a specific professional value such as client-centred practice, as supported by codes of ethics and standards of practice (RCOT, 2015, 2017), was found to be a significant factor in decision-making for some and yet easily disregarded by others. More surprisingly client-centred practice may not be consistently upheld by the same therapist in different situations. The study further suggests that occupational therapists will apply the same value differently (for example, ‘respect’), according to the situation.
There is no consensus in the literature regarding professional values (Aguilar et al., 2012). The findings of this study add empirical evidence to this dissension and challenge the assumption that all occupational therapists share the same values – even the most obvious values of the profession may be applied differently in practice. While the occupational therapy profession values ‘enabling’ in general, what each occupational therapist thinks will ‘enable’ frequently differs.
To appreciate the preliminary results of the empirical study it is necessary to place them in the context of contemporary official literature, in which numerous assumptions are widely accepted, particularly in mission statements, codes and declarations. The most significant of these are (a) that people hold constant values that always affect their behaviour in the same way (it is assumed that we can be sure, for example, that professional X will always be truthful because she somehow possesses the value ‘truthfulness’); (b) that groups of people who make up a profession will hold the same values; (c) that individual members of ‘values-based professions’ will consistently apply their profession’s values across all their practice; and (d) that professionals can and should be retained and recruited (or not) according to which values they hold. Philosophical reflection, well-known decision-making theory, and the study’s empirical results show that these assumptions cannot be sustained.
While it is easy to agree in general about the desirability of values like ‘respecting’ and ‘enabling’ clients, such value-statements provide only limited guidance to practitioners when dealing with real-world situations (Drolet, 2014; Peile and Fulford, 2015). For example, two occupational therapists may be committed to valuing both ‘patient autonomy’ and ‘acting in the patient’s best interests’, but how they interpret these commitments may differ in individual cases. One might interpret ‘valuing patient autonomy’ as requiring compliance with the patient’s currently expressed wishes, whatever they are, while another might regard the wishes as ‘out of character’ and hence not ‘authentic’, and so conclude that compliance with them would not be compatible with truly respecting autonomy in this instance (Kane, 2017). Furthermore, when the values of ‘respecting autonomy’ and ‘acting in the patient’s best interests’ are perceived to conflict, as in Andi’s scenario, which value the professional prioritises may differ both between two practitioners, and for the same practitioner in different contexts (Peile, 2014).
To understand how it is possible for there to be so much enthusiasm for values in healthcare while there is, at the same time, so much uncertainty about what they are, it is helpful to distinguish between two different understandings of ‘values-based practice’. These understandings are:
Values-based practice understanding one: declaring, sharing and using ‘the right values’
This version of values-based practice assumes that it’s essential that professionals share and apply the ‘right values’, for example those expressed in ethical codes, professional mission statements, or those which form part of the NHS constitution (NHS, 2015).
Values-based practice understanding two: exploring values in context
This version of values-based practice emphasises the importance of professionals working to clarify their own and their clients’ values to include them sensitively in decision-making, and to try to achieve the most desirable outcomes (Fulford, 2008; Loughlin, 2014, 2018; Seedhouse, 2005, 2009).
According to the first approach, if professionals adhere to the approved set of organisational values then it is assumed that they will practise consistently, acting in the same way as their fellow professionals, on every specific occasion. According to the second understanding, the importance of recognising values is not to deliver the same service to all clients, but to deliver a service a particular client wants, and the professional is prepared and able to deliver.
Philosophical reflection, investigations into real-life decision-making (Ariely, 2009; Damasio, 1994) and evidence from this and the studies of Wright-St Clair and Newcombe (2014) show that the first understanding is naive and does not reflect how practical decisions are made. The second understanding is more realistic.
The results show that occupational therapists often try to balance client and family values with their professional obligations and their own values. However, this process is highly variable and depends on many factors, which result in diverse and complex decision- making in practice (Creek et al., 2005; Pentland et al., 2018). As a group, the respondents do not have a fixed and stable set of values, nor do they always apply their values in the same way: they respect some people’s choices some of the time but not all people’s choices all the time. Unlike ‘missions’ and ‘ethical codes’ – which are cast in black and white – individuals’ values fluctuate and vary according to many factors, including the situation they are in, how they feel emotionally at the time, peer pressures, their previous experiences, their perceptions of risk, their cultural background, and so on.
Conclusion, limitations and recommendations
We did not find a group of professionals applying a clear and shared set of values to solve problems, rather we found a group of human beings responding to situations in complex human ways.
There are limitations to what can be claimed from one empirical study. It is possible that, were the study repeated with a similar group of occupational therapists, there would be a different result. It is possible that were this study to be carried out with groups from other professions there would be a different result. And it is possible that randomly selected respondents from the general public would respond differently from the occupational therapy professionals we studied.
It is therefore recommended that a further research programme is implemented, using a similar methodology to the first study:
Research a similar cohort of occupational therapists, to gauge replicability. Research a cohort from another health profession. Research a service/commercial profession, for example middle managers in the banking industry. Research a randomly selected cohort from the general public.
It should also be acknowledged that decision-making in real life may be different from decision-making about scenarios sitting before a computer, deciding about hypothetical situations. Non-verbal and environmental cues were lacking, and it is possible that with time and further consultation with fellow occupational therapists, decisions would be different.
An immediate recommendation from the results of the present study is that the education of occupational therapy students and professionals should be enhanced. The results clearly show a wide range of reasoning and justifications about practical situations, many of which either contrast or directly conflict. It seems important, therefore, to build this reality into both undergraduate education and continuing professional development, by designing and implementing educational programmes that enable occupational therapists and occupational therapy students to recognise the complexity of everyday decision-making in depth, to become more aware of their own assumptions, reactions and value judgements in difficult cases, and to recognise and learn how to respond to fellow professionals – and clients – who may bring very different values and justifications to practice.
Key findings
Occupational therapists apply values in practical decision-making in complex and divergent ways. Values are one factor among others in practical decision-making. The complexity of occupational therapy decision-making should be included in student and professional education.
What the study has added
The study provides evidence about the role of values in occupational therapy decision-making, highlighting how important it is to be aware of personal, professional and clients’ realities in everyday practice.
Footnotes
Acknowledgements
Laura Torney (research assistant) contributed to the initial recruitment and administration of the study.
Research ethics
Ethical approval for this study was received in October 2016 from the University of Worcester ethics committee (approval number: PRLT080816). The ethics committee advised that ethical approval was not required for the scenario development phase of the study as it was believed this was a preparatory phase to the research.
Consent
Participants of the online data collection via VX were provided with information about the study and asked to tick a box to indicate consent to be included in the study.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to research, authorship and/or publication of this article: The research tool used in this study was developed and is owned by David Seedhouse.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research project was supported by UKOTRF grant from the Royal College of Occupational Therapists.
Contributorship
Yvonne Thomas as chief investigator for the study was responsible for the study design, ethical approval, review of the occupational therapy literature and produced the first draft of the article and contributed to each revision. David Seedhouse was coinvestigator and was involved in all aspects of the study design and made a major contribution to the results and discussion sections of the article. Vanessa Peutherer provided a major contribution to the development, writing and piloting of scenarios, and contributed to the writing of the methods section of the article. Michael Loughlin contributed to the literature review related to values and to the discussion section of the article.
Collectively, all authors contributed to the analysis of the results from the VX and participated in the development and subsequent revisions of the completed article.