
Abstract
Introduction
This study aimed to understand existing vocational rehabilitation service provision in one locality in London (population 3.74 million), identify any gaps and explore reasons for this, to support service development.
Method
Using soft systems methodology to guide the research process, semi-structured interviews were completed with nine participants, who were clinicians and managers providing vocational rehabilitation within a National Health Service context. Data were analysed thematically to build a ‘rich picture’ and develop a conceptual model of vocational rehabilitation service delivery. Findings were then ratified with participants at an engagement event.
Results
The findings indicate a spectrum of vocational rehabilitation service provision for long-term neurological conditions with differing levels of funding in place. Vocational rehabilitation often takes place ‘under the radar’ and therefore the true vocational rehabilitation needs of this population, and the extent of service provision, is not known. There is inconsistency of understanding across the services as to what constitutes vocational rehabilitation and outcomes are not routinely measured.
Conclusion
For vocational rehabilitation services to develop they require appropriate funding, driven by government policy to commissioners. Clear definitions of vocational rehabilitation, collecting and sharing outcome data and effective communication across services are needed at a local level. This is expressed in a conceptual model of vocational rehabilitation service delivery.
Keywords
Introduction
Long-term neurological conditions (LTNCs) result from damage to the body’s nervous system (the brain, spinal cord and/or peripheral nerves), caused by disease or injury. LTNCs include sudden onset conditions (such as stroke, traumatic brain injury (TBI) and spinal cord injury (SCI)), intermittent or unpredictable conditions (such as epilepsy and migraine), progressive conditions (such as multiple sclerosis (MS) and muscular dystrophy) and stable neurological conditions (such as post-polio syndrome) (Department of Health, 2005). There are approximately 12.5 million people with LTNCs in England, equating to 59,000 per clinical commissioning group (Neurological Alliance, 2014). The nature, causes and impact of these LTNCs varies greatly between individuals, but for many people injury or diagnosis occurs at working age.
For most adults work is integral to daily life, providing financial support, emotional and psychological wellbeing, security and independence (Baldwin and Brusco, 2011). Unemployment can negatively affect these factors, impacting on engagement in activities and putting psychological and physical health at risk (Blank et al., 2015; Dorstyn et al., 2019). Research indicates that high levels of sickness absence and health-related unemployment lead to poor health outcomes and increased reliance on the state (Black and Frost, 2011; Department for Work and Pensions (DWP) and Department of Health, 2008). Maintaining working roles is therefore important at a societal level, as well as for individuals (Waddell and Burton, 2006), including those with LTNCs (Playford et al., 2011; Radford et al., 2018; Sinclair et al., 2014).
After minor ailments (such as coughs and colds), musculoskeletal conditions (such as back pain) and mental health issues (for example anxiety and depression) are the most common causes of sickness absence in England (Public Health England, 2018). Government initiatives aimed at providing vocational support for people with health conditions or disability have therefore been designed with this client group in mind. However, the complex and often hidden needs of people with LTNCs are often difficult to support within generic programmes (Radford et al., 2013; Sweetland et al., 2007; Tyerman, 2012) and a need for specialist vocational rehabilitation (VR), tailored to the needs of this group, has been identified (Hilton et al., 2018; Libeson et al., 2018; Playford et al., 2011; Radford et al., 2013; Sinclair et al., 2014; Tyerman, 2012).
VR can be described as ‘whatever helps someone with a health problem to stay at, return to and remain in work’ (Waddell et al., 2008: 8). Health professionals are integral to managing health conditions and people with LTNCs consistently outline the benefit of support from people who understand the impact of their condition on maintaining employment (Sweetland et al., 2012). In the United Kingdom, occupational therapists are often the clinician leading this work, using key skills to help people overcome barriers to continuing with the valued occupation of employment (COT, 2016). The timing of VR interventions is key, with evidence suggesting that early intervention to support people to manage their LTNC in the workplace leads to them staying in work for longer (Doogan and Playford, 2014; Kirk-Brown et al., 2014; Radford et al., 2013, 2018; Rusbridge et al., 2013; Sweetland et al., 2012; Tyerman, 2012). However, in practice the provision of specialist VR remains sporadic, with poor inter-agency collaboration between health and employment services, meaning that people with LTNCs are at higher risk of being unemployed (All-Party Parliamentary Group for MS, 2016; Playford et al., 2011; Sinclair et al., 2014).
Sinclair et al. (2014) used soft systems methodology (SSM) to explore stroke-specific VR in Derbyshire (one English county, population 791,966 (Office for National Statistics, 2017)) with the aim of clarifying existing service provision to support future service development. They identified that a lack of a sanctioned VR pathway led to ad hoc support, along with an unmet need for milder stroke survivors. Specific VR training was often lacking and cross-agency working ineffective. Timing of VR was highlighted as a complex issue with not only early, but also late intervention required depending on the stroke survivor’s needs and rehabilitation journey. Due to competing priorities, commissioners deemed VR as non-essential (over services such as acute stroke units and early supported discharge teams), which made VR service development challenging and inconsistent.
Sinclair et al. (2014) noted that their study focused on one geographical area and one LTNC (stroke), and that the results may not generalise to other regions and conditions. However, the methodology was robust and the results give a basis to review and compare current service provision in other localities, across all LTNCs. In line with this, the aim of this study was to conduct an analysis of VR services in North Central and North East London (NC&NEL) (an area incorporating 13 London boroughs, population 3,473,707 (Office for National Statistics, 2017)), focused by the following aims:
To investigate VR service provision in NC&NEL, exploring facilitators and barriers to supporting people with LTNCs to maintain employment. To identify gaps in VR service provision in NC&NEL, the reasons for these and explore stakeholders’ perspectives of how this could be addressed. To develop a conceptual model of VR service delivery for NC&NEL to aid future development of a VR pathway for LTNC in this locality.
Methods
Research design
Identifying barriers and facilitators to vocational rehabilitation service provision requires an in-depth understanding of the current situation. Therefore, this study used a qualitative methodology. This included semi-structured interviews, thematic analysis of data and an engagement event with participants.
We followed Sinclair et al. (2014) in using SSM (Checkland and Scholes, 1999) to guide this study. SSM is a systematic research approach, which can be used to evaluate interventions rooted in complex management, organisational and policy contexts, where no easy solution is identifiable (Checkland and Scholes, 1999; Sinclair et al., 2014). SSM uses systems rules and principles, following seven stages to support thinking about the real world and the human relationships between structure, process and outcome:
Identifying the problematic situation. Researching the situation and building a ‘rich picture’ (a diagrammatic representation of the current or real-world situation). Selecting perspectives and building ‘root definitions’ (key processes that should take place within the desired system). Developing a conceptual model of the change system. Comparing the model with the real-world situation. Defining the changes to be implemented. Taking action.
This study focused on stages one to six of SSM, using semi-structured interviews with VR service providers to gain qualitative data. These data were used to build a ‘rich picture’ of the topic, which was then ratified at an engagement event. SSM uses a structured framework ‘CATWOE’ (customers, actors, transformation process, worldview, owners and environmental constraints) to explore the perspectives of participants in relation to the research aim (Table 1). This was therefore used to both develop the research questions and structure the data analysis.
The soft systems methodology CATWOE approach.
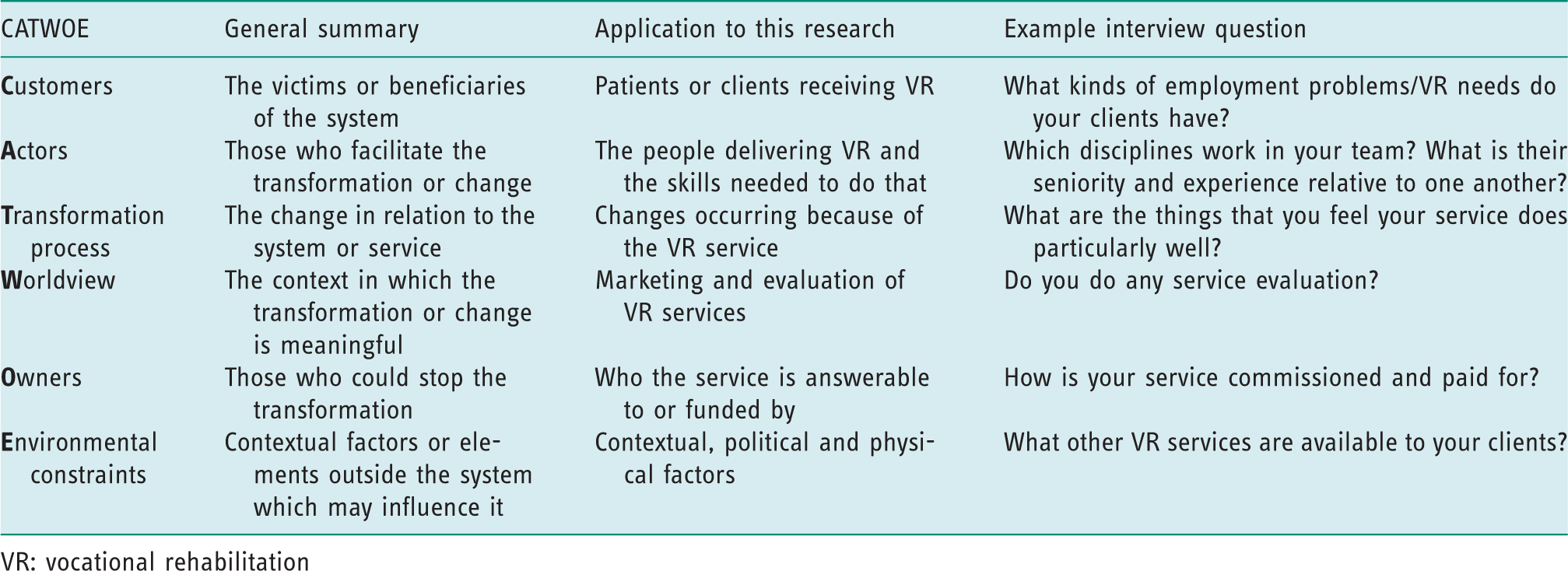
VR: vocational rehabilitation
Ethical approval
Ethical approval was obtained from Brunel University London's Department of Clinical Sciences, Research Ethics Committee. Ref: 14/10/MOT/18. Written informed consent was gained from all participants. To ensure confidentiality for participants, people and sites, data have been anonymised.
Participants
Participants for the study were recruited using convenience sampling via the University College London Partners (UCLP), Centre for Neuro Rehabilitation, VR special interest group and wider stakeholders identified by group members (for example known providers of VR services who are not active group members). UCLP is an organisation that aims to bring together health professionals and researchers to aid service development. The VR special interest group meets monthly and is open to anyone with an interest in VR. Members work across a variety of National Health Service (NHS), academic and third sector services.
Both managers and clinicians from NHS services within NC&NEL were invited to participate in semi-structured face-to-face interviews to identify the problematic situation and build a ‘rich picture’ of current VR service provision (SSM stages 1 and 2). Participants were limited to NHS providers due to resource constraints of the study and the implications of this are discussed in the limitations section of this paper.
Data collection and analysis
Questions for the semi-structured interviews were developed using CATWOE (see Table 1 for examples) and piloted with members of the VR special interest group to ensure they were understandable to the professionals being interviewed. The interviews were audio recorded and transcribed verbatim. SSM does not provide a method for data analysis. Data were analysed thematically following Braun and Clarke’s (2006) approach, with CATWOE (as outlined in Table 1) as a guide.
The transcripts were analysed independently by two authors (KH and GE) and compared and discussed to ensure consistency. Using the CATWOE framework, barriers and facilitators of VR service provision were identified (SSM stage 3). A diagrammatic ‘rich picture’ was formulated together with a root definition; this conceptual model of VR in NC&NEL was compared to existing service provision (SSM stages 4 and 5) and shared with participants at the engagement event. At this event, the research findings were further developed and ratified (SSM stage 6).
Findings
Nine participants from six different services (one inpatient rehabilitation, three community neurological rehabilitation teams (CNRT), and two specialist VR services) volunteered to participate. A semi-structured interview was completed with each of them individually. Seven of the participants were occupational therapists (two of whom were managers), one was a physician (and a service lead) and one was a clinical psychologist. All of the participants were female. Data on age and years of practice were not collected.
All participants attended the engagement event, apart from those from service 6 who did not respond to their invitation. In addition to those interviewed, managers from services 4 and 5 and authors KH and GE were also in attendance at the engagement event.
Findings from the semi-structured interview data analysis are presented below using each of the CATWOE categories.
Customers
All but one of the services accepted referrals for adults with any neurological condition. Community team referrals were mainly received from GPs, health professionals in acute hospital services and occasionally social services. In general, the community team referrals were not specifically for VR; however, VR was often highlighted as an issue within the client’s initial assessment. A specialist outpatient VR service received internal referrals from their hospital colleagues and external referrals from GPs, other hospitals and community teams who did not provide VR. In terms of the patients we work with […] the biggest groups are probably stroke, multiple sclerosis, brain tumour and head injury, but all other neurological diagnoses as well. (P6) It’s [employment need] normally either someone who’s in work… they’re in employment they've had an injury or an accident, or they've got a progressive condition and there needs to be either thought made about adjustments or it’s about a return to work plan … it might be about disclosing. (P4)
Actors
Both specialist and generalist clinicians provided VR interventions. The majority of VR interventions were led by occupational therapists with access to other disciplines where required. The permutations of core and extended teams varied, but a core team tended to include occupational therapy and psychology, with physiotherapy and speech and language therapy available through defined pathways. Linking with disciplines outside of the core multi-disciplinary team (MDT) was seen as beneficial, including disability employment advisors and job coaches. The voc rehab service is […] led by a specialist occupational therapist […] but also they regularly access neuropsychologists and […] if a patient required it in relation to their return to work issues, they could also access speech and language and physio. (P2) I personally think that vocational rehab is a speciality service in its own right. And I don’t think that it’s something that should fall to OTs to dabble in […] I don’t have the capacity or the support to go away and learn all the latest employment law and benefits and what help you can get, so I don’t consider myself to be a vocational rehab expert in any way shape or form, I am more of a sign-poster or if you’ve got a job we can go back to then that’s fine. (P1)
Transformation process
Changes and developments in services were shaped by the content of VR interventions, communication with other services/commissioners, and review of outcome data. The scope of VR interventions varied across the services. Specialist services were able to provide input across the breadth of VR. However, they identified that job-seeking requires skills that are often not available within their current service provision. The generalist services provided VR interventions on a more ad hoc basis and often with limitations, for example only providing support with return to work. If we got a referral for vocational rehab, we’d struggle because we’re not funded to do specifically vocational rehab. […] if it comes up within their general assessment and treatment that they’re having […] we can do that […] but it needs to be part of their overall treatment, rather than specific. (P8) We don’t tend to pull that … information out […] it’s time to be able to do that and to make the information useful […] we’ve not been asked for it […] at the moment it would be quite tricky to pull that data, we would have to probably keep it separately. (P4) The Job Centre, also our local disability employment advisors, will contact me if they have people with neurological conditions […] we’ve kind of set up quite a nice sort of channel so […] they’ll check in with me just to see if I know them and if […] they are suitable to come through to us as well. (P2)
Worldview
Funding for VR varied considerably across the services. The specific VR services received allocated VR funding, which was managed flexibly at an NHS Trust level with overall sign-off from commissioners. Within the generalist services there was variability of VR funding, complicated by different funding streams for stroke and other neurological conditions. We’re not a voc rehab specific service and in fact we’re not even commissioned to do voc rehab full stop. […] But we would, if you think about the sort of pre-voc rehab pathway, we stretch that to as far as we possibly can without going into someone’s work place. (P5) We had to do a lot of marketing at the beginning and what we tried to do was to base the service on what was already happening in London, so we looked at other service models and we tried to … sort of develop what we did in the community alongside other community […] examples. (P2)
Ownership
Across the services, the core ‘owners’ were NHS trusts and commissioners. Agreement that VR is a health outcome and therefore a local commissioning responsibility, rather than falling to national employment support services, was identified as beneficial in obtaining commissioner-led funding. We have ample evidence that a lot of commissioners still think that work is not health, despite the fact that it is … embraced in quality outcome two of the NHS quality outcomes framework […] it was in the National Service Framework for long-term conditions as quality requirement six and […] there is a national rehabilitation delivery board, where vocational rehabilitation […] is about their third objective with the view that if you commission for vocational rehabilitation you are commissioning for excellence. (P6)
Environment
All participants identified that service location and geographical environment impacted on service provision. The services embedded in the community had more established links with local services and were able to provide interventions in a variety of locations. What’s important is to embed people in their own community […] most people want to volunteer locally to their home or get work more locally to their home and also […] the social isolation […] barriers to integration of these patients […] being embedded in a system that’s within their community … that seems really valuable. (P9) The drivers were that the research showed that this intervention works, that this population is hugely … under serviced and […] the current political climate of getting people back to work and keeping people in work […] I think this joined up service was born out of clinical need but also […] socio-political drivers as well. (P6) Actual or perceived funding to provide VR services is in place. Clinicians have direct formal contact with commissioners to support funding of service. Services explicitly acknowledge/state that they provide VR (it is not under the radar). Services have a clear concept of what VR is and how they provide it. Expertise exists within a core MDT to meet the needs that patients identify are their vocational problems (from a neuro-rehabilitation point of view). An effective triage process is in place: patients are quickly assessed and prioritised. Services are well integrated within the community they serve: support services are known about and liaised with and the service is delivered in the geographical area/space most appropriate for the patient. The needs of people who are self-employed/unemployed are understood and met. There are identified, proactive ways for people to link back into the service as needed. Desirable work outcomes are identified and measured. Patients’ needs are not always identified and therefore met, as the service perceives they do not have the skills to provide VR. The prevalence of work problems in the service’s population of people with neurological problems is not known.
Rich picture
In line with SSM, the CATWOE data analysis was used to develop a ‘rich picture’ or real-world situation of current VR service delivery in NC&NEL (Figure 1). This demonstrates a spectrum of service provision, ranging from specialist VR services where funding is agreed to generalist rehabilitation services that provide VR on an ad hoc basis, without specific funding identified.

‘Rich picture’ demonstrating the complexity and variability of vocational rehabilitation provision for long-term neurological conditions in North Central and North East London.
Specialist services are collecting VR outcomes data, which they outline is essential for service development, but there is a lack of consistency of measures used and no formal way of sharing this information. In contrast, the generalist services are not collating any work-related data and therefore do not have a full understanding of the VR needs of their population.
At the centre of the ‘rich picture’ are other services that provide work support and the ways that the VR services communicate with them. Depending on geographical location and service focus, communication could be consistent through personal contact (which was reported as beneficial) or on an ad hoc basis. Job-seeking support was seen as outside the scope of most of the VR services with their current resources and skills. It is therefore pictured as part of ‘other services’.
Conceptual model and engagement event
At the engagement event we reviewed and expanded the initial findings through collaborative discussion with participants, leading to an agreement of the most important factors required for effective VR, as follows:
Actual or perceived funding to provide VR services is in place. The government leads funding via commissioners. Expertise to provide VR exists within an extended MDT, including the DWP. Services have a clear concept of what VR is and how they provide it. There are identified, proactive ways for people to link back into VR services as needed.
We then refined the ‘rich picture’ shown in Figure 1 to present a conceptual model of VR service delivery for NC&NEL (Figure 2). The importance of communication links between specialist, generalist and other VR services is shown in Figure 2 by the lines linking the services. Specialist and generalist VR services need to agree definitions of VR and identify ways that services can share data to improve commissioning pathways and service delivery. A top-down commissioning approach via the government and NHS England was seen as an essential driver for service development. Job-seeking is kept as a separate pathway (as shown by the dashed arrow in Figure 2) as participants report the need for further exploration of appropriate models of service delivery, including the possibility of shared group programmes.

Conceptual model of vocational rehabilitation service delivery for North Central and North East London.
Discussion
The main findings of this study relate to the need for nationally agreed funding, an extended VR MDT, a job-seeking pathway, shared understanding of VR interventions, shared standards for data collection and outcome measurement, the provision of timely VR services, and the integration of VR services within the local community.
Funding was seen as the most important factor in providing effective VR services. When specific VR funding was in place, services were able to focus on delivering effective VR through continued service development. Without specific funding, services were required to manage VR within the competing demands of their general caseloads. Therefore, VR tended to be provided ‘under the radar’, limiting both the range of VR interventions provided and the development of needed services. Playford et al. (2011) and Sinclair et al. (2014) highlight that commissioners do not view VR as a legitimate health concern, despite the fact that people who are unemployed are more frequent users of health services (Black and Frost, 2011).
Our study supports findings from previous research showing that expertise to deliver work retention interventions for people with LTNCs resides with the common disciplines found in a neurology MDT (for example, occupational therapists, clinical psychologists, physicians, speech and language therapists) (Rumrill and Roessler, 2015; Sweetland et al., 2012). However, we identify that additional team members including Job Centre Plus, careers counsellors and job coaches are required to deliver effective VR to job seekers, in line with Tyerman (2012) and Sweetland et al. (2012), who note that different kinds of support are required for people who are employed or returning to employment, compared to those who need to find new employment.
Interestingly, there is no consensus in the literature on what VR consists of or how best to deliver it. As a consequence, provision of VR varies from service to service, with some services performing elements of VR within a general rehabilitation programme. This has resulted in a lack of clarity regarding the extent of met and unmet VR needs within the population, and many commissioners and referrers not being aware of the extent of VR service provision currently occurring. In addition, we found that there is no routine or consistent collection of VR outcomes within NC&NEL. As acknowledged in the recent government paper Improving Lives: The Work, Health and Disability Green Paper (Department for Work and Pensions and Department of Health, 2016), work should be embedded as a health outcome and therefore the routine collection of work-related outcomes related to people with LTNCs is needed to inform business case development and local commissioning (Department for Work and Pensions and Department of Health, 2016; Sinclair et al., 2014).
The participants in this study agreed that defining VR interventions for job maintenance, return to work, work exit and job-seeking is essential. A lack of taxonomy or classifications of VR interventions is highlighted as a challenge throughout the VR literature, with authors struggling to establish which service type produces the best work outcomes (Baldwin and Brusco, 2011; Ottomanelli and Lind, 2009; Tyerman, 2012).
By definition, LTNCs fluctuate and change. Participants in this study recognised that having standardised, proactive ways for people to link back into VR services when needed was essential. This is well documented within the literature, with early and on-going intervention resulting in people staying in work for longer, thereby reducing the burden on society (Doogan and Playford, 2014; Kirk-Brown et al., 2014; Middleton et al., 2015; Radford et al., 2013, 2018; Rusbridge et al., 2013; Sweetland et al., 2012; Tyerman, 2012).
There was consensus among participants that for effective VR to occur, services should be well integrated within the community they serve, enabling awareness of and personal liaison within the extended MDT. Local provision gives flexibility to provide VR in the geographical area or space most appropriate for service users (for example practising computer-based tasks in a local library rather than in a hospital clinic room).
Implications for service provision
Using SSM, this research study has identified barriers and facilitators of VR service provision in NC&NEL, gaps in service delivery and the reasons for this. It has explored how stakeholders think the issues identified could be addressed, and developed a conceptual model of VR service delivery for the locality. This was fed back to the local VR special interest group, which helped develop project work. The results suggest a need for integrated commissioning between health, the DWP and voluntary sectors, based on an accurate assessment of met and unmet VR needs. This would ensure VR services are appropriately established and can meet the needs of people with LTNCs to both retain their current jobs and re-enter the workplace should they become unemployed. This needs to be facilitated by the collection of work status as a health outcome, along with agreed standard VR outcome measures. The findings demonstrate that there has been little change in NHS VR provision in recent years despite recommendations in the National Service Framework for Long Term Conditions in 2005 (Department of Health, 2005) and the government’s agenda to reduce the number of people claiming ill health benefits.
Limitations
The results of this study are local to the six services that participated. To the best of our knowledge, we captured all of the services who identified themselves as providing NHS funded VR in NC&NEL. However, it is possible that other services are providing VR although they may not identify themselves as doing so.
The primary researcher (KH) is a colleague of many of the participants, which could have led to interview bias. Efforts were made to minimise this by asking the participants the same questions during the semi-structured interviews and using CATWOE to analyse the data. The engagement event also helped to limit bias as participants were given the opportunity to discuss, debate and develop the research themes outside of direct researcher facilitation.
It was important to gain the perspectives of both clinicians and managers as they could have differing viewpoints regarding VR service delivery, and these views are represented in the study. However, the study was limited to NHS service providers and it would be valuable to explore the perspectives of commissioners and other VR providers, including the DWP and charity-led services.
The study focused on a specific geographical area, with implications for generalisability. However, like Sinclair et al. (2014), we have found SSM to be both feasible and valuable for this kind of evaluation, and our results are congruent with theirs. This provides a potential framework for other services to follow suit, contributing to the wider picture of VR service provision.
Future research
The evidence regarding the provision VR for LTNCs is currently limited. Following on from this study, further research, which examines the perspectives of people with LTNCs of their work support needs, and the adequacy of services to meet these, would be valuable. From a service-delivery point of view it is important to test the feasibility of collecting a common core set of VR outcomes data across different service providers.
Conclusion
The research model employed in this study is effective in identifying local systems currently in place to provide VR. It could be used more widely to identify inequalities in LTNC VR service provision. As a priority, commissioners need to clearly understand met and unmet LTNC VR needs. This would be facilitated by development of a VR taxonomy, and the collation of agreed work data and outcomes.
Key findings
Vocational rehabilitation (VR) provision for long-term neurological conditions (LTNCs) is variable and often happens ‘under the radar’. To improve service delivery, commissioners need to understand the met and unmet VR needs of people with LTNCs.
What the study has added
This study has highlighted systemic issues regarding funding and service provision of VR for people with LTNCs in one locality, adding to the small evidence base in this clinical area.
Footnotes
Acknowledgements
The authors wish to thank the participants for their involvement in this study.
Research ethics
Ethical approval was obtained from Brunel University London's Department of Clinical Sciences Research Ethics Committee. Ref: 14/10/MOT/18, November 2014.
Consent
All participants provided written informed consent to be interviewed for the study.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article. Author EDP was supported by the National Institute for Health Research, University College London Hospitals, Biomedical Research Centre.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article. Author KH was supported by the Therapy and Rehabilitation Services Department at the National Hospital for Neurology and Neurosurgery, the Trustees of University College London Hospitals NHS Foundation Trust, The Constance Owens Trust and the Elizabeth Casson Trust in funding her MSc in Occupational Therapy, which this research formed part of.
Contributorship
Kate Hayward researched literature and applied for ethical approval. All authors contributed to the methodology of the project. Kate Hayward and Gail Eva developed and interpreted the data. Kate Hayward wrote the first draft of the paper. All authors reviewed and edited the manuscript and approved the final version.