
Abstract
Introduction
Occupational therapists are increasingly referred children who experience difficulty with social interaction at school. Research indicates that social difficulties are impacted by inefficient use of cognitive strategies. The Perceive, Recall, Plan and Perform system of intervention targets underlying cognitive strategies during task performance. This study aimed to investigate the impact of a playground social skills programme based on the Perceive, Recall, Plan and Perform intervention.
Method
A quantitative, experimental, crossover design was used to evaluate the effectiveness of the Perceive, Recall, Plan and Perform intervention on developing social competence for a group of children in primary school (Kindergarten to Grade Three). Sixteen children participated in the study. Goal attainment scaling scores and Perceive, Recall, Plan and Perform assessment scores rated by teachers were used as outcome measures. Data were analysed using a series of two-way repeated-measures analysis of variance.
Results
Outcome measures taken at three time-points indicated that the children improved in social performance significantly more when receiving the Perceive, Recall, Plan and Perform intervention compared to opportunities for regular playground activities. This was apparent across both goal attainment scaling change scores and change in intervention total scores.
Conclusion
This strategy-focused approach appeared to be effective in developing the thinking strategies that facilitate children’s social participation at school.
Introduction
Social competence is a broad multidimensional term used to describe how well children are able to evaluate social situations, and to select and apply social behaviours that are most appropriate to a given social context (VandenBos, 2015). By interacting with others at school, children develop the social skills necessary to participate in a range of academic and social activities (Pascoe and Brennan, 2017). Occupational therapists are increasingly referred children who experience reduced social competence. Children’s ability to think in specific social contexts is influenced by cognitive strategies that determine how well they plan, carry out and regulate appropriate social behaviours (OECD, 2013). There is limited guidance for occupational therapists working in schools about how best to improve social participation through the use of cognitive strategies. This study aimed to investigate the outcomes of a social skills programme based on the Perceive, Recall, Plan and Perform (PRPP) system of intervention, an intervention targeting cognitive strategy use (Chapparo and Ranka, 2010).
Literature review
Social competence and school participation
Social and emotional learning has become an integral part of school participation, with children expected to fit the occupational role of a ‘social learner’ (OECD, 2013). It is through engagement with others that children acquire the knowledge and skills needed to work and achieve curriculum objectives (Pressley and Harris, 2006). Shared learning is an important part of classroom education, with children expected to know how to respond to their peers during group activities (NSW Education Standards Authority, 2017). On the playground, children apply a variety of social skills encompassing assertiveness, emotional coping, communication and problem-solving to initiate and maintain play with their peers (Skard and Bundy, 2008). Play provides opportunity for children to develop friendships and to learn strategies to manage emotions of frustration and anger provoked by different scenarios (Skard and Bundy, 2008). In the classroom, performance is mediated by how well children adapt social skills to the context of varied social learning activities (Lim and Rodger, 2008).
Educational research has demonstrated the negative impact of reduced emotional control on children’s alertness and state of readiness for learning (Weissberg et al., 2015). While positive emotional responses during playground interactions are associated with enhanced long-term recall, an inability to regulate emotions disrupts the thinking processes required for classroom learning (Durlak et al., 2011). Anecdotal reports of the rise in occupational therapy referrals to target social competence may be explained by increasing parent concerns. A joint study between Monash University and the Australian Scholarships Group found that 69% of parents across the public and independent education sector believed that schools should incorporate more social skill training, with a need to address difficulties with playground interactions (Australian Scholarships Group Friendly Society Limited, 2017).
Intervention for social participation
There has been a surge in research over the past few decades as children’s social and emotional learning (SEL) becomes more of a concern in education. Most studies describing occupational therapy interventions for social participation have focused on skill acquisition: teaching children steps for social interactions, including engaging appropriately with others; initiating conversation; and developing an awareness of social norms (Hilton, 2015). A comprehensive review was conducted by O’Conner and colleagues (2017) to review the literature on evidence-based SEL programmes that were associated with positive student behaviours. In their report they outlined four core practices that were effective in facilitating social and emotional learning. The acronym SAFE refers to programmes that are: sequenced (use a connected and sequenced set of activities to achieve skill development), active (dynamic forms of learning allowing children to practise skills in real life context), focused (at least one component is focused on developing personal or social skills) and specific (target specific SEL skills rather than a general approach). Lim and Rodger (2008) suggest that rather than targeting skills in isolation, occupation-based models of practice that consider social competencies needed by children in their specific contexts should be used.
Social cognition
While social competence is dependent upon many contextual factors, cognition is thought to be a primary determinant (OECD, 2013). Social cognition is the ability to attend to, encode, interpret, plan and execute appropriate social behaviours in a given interaction (Case-Smith, 2015). Social cognitive processes involve the operation of memory stores, decision processes and response mechanisms (VandenBos, 2015). Emphasis has been placed on children being able to monitor the emotional cues of their peers in order to plan and mediate appropriate behavioural responses (Dodge et al., 2013). Children taught higher level thinking strategies for understanding peer perspectives and for interpreting social meaning through concepts such as ‘theory of mind’ have better social outcomes then those that are taught skills in isolation (Case-Smith, 2015). Social interactions are not only mediated by the presence of a set of competent social skills, but also on how well children process and interpret social information in order to adapt and modify existing skills to suit the situation (Dodge et al., 2013).
Cognitive strategy use
Social competence can be enhanced by teaching children how to use cognitive strategies during everyday activities (Chapparo, 2017). Cognitive strategies are mental thinking tactics selected and applied to guide cognition and are influenced by information processing (Pressley and Harris, 2006). Information processing refers to the flow of information through the human nervous system, involving the operation of perceptual systems, memory stores, decision processes and response mechanisms (VandenBos, 2015). Effective cognitive strategy use implies salience or use of known cognitive strategies in the ‘here and now’ to match the context of task and the environment. Inefficient use of cognitive strategies occurs when children do not select and apply strategies that optimise task performance (Chapparo and Ranka, 2014). Application of this view of social competence suggests the need for an ecological approach to assessment and intervention that focuses on teaching cognitive strategies during social participation in real-world contexts.
There is limited information in the literature specifying cognitive strategy use and how it can be addressed during social aspects of occupational performance. There are two approaches that are described. The first of these, Cognitive Orientation for daily Occupational Performance (CO-OP) (Polatajko and Mandich, 2004), is a global problem-solving framework that focuses on establishing child-led goals and uses a ‘goal, plan, do, check’ framework to assist children with subsequent skill acquisition. To date, research on CO-OP has provided evidence of effectiveness with children with Developmental Coordination Disorder (Bernie and Rodger, 2004), attention deficit hyperactivity disorder (Hahn-Markowitz et al., 2011) and acquired brain injury (Missiuna et al., 2010) in attaining desired skills in daily activities. This approach focuses on giving children opportunities to learn new skills by finding their own way to solve problems (Polatajko and Mandich, 2004). While the goal is to support generalising and transferring learning to different contexts and skills, social competence is multi-contextual and requires an adaptation and child-specific cognitive strategies during social performance. The PRPP system is an approach that can be used to assess and support children of any age or social circumstance whose performance is compromised by difficulties processing the cognitive demands of everyday tasks (Chapparo and Ranka, 2014).
The PRPP system of task analysis is an occupational therapy assessment and intervention approach that is based on concepts of occupational performance and information processing. The focus of intervention is on how individuals apply cognitive strategies during occupational performance, and integrates aspects of systematic instruction and learning theory. Therapists plan interventions aimed at building strategy use across the four dimensions of information processing that underpin each part of the PRPP system (Chapparo and Ranka, 2010): perceive strategies (attention and sensory perception), recall strategies (learning and memory), plan strategies (goal-setting, problem-solving, evaluating) and perform strategies (initiating, continuing, controlling actions). The PRPP intervention purports to broaden the traditional focus of teaching children systematic steps for social skills by incorporating instruction in information processing strategies that focus on cognitive processes being employed during the performance of social tasks (Chapparo and Ranka, 2010).
To date, research on the use of the PRPP for improving everyday performance has focused on adults with brain injury (Nott et al., 2008). While studies have provided promising results that support the generalisation and efficacy of strategy use intervention for everyday activities, no information is available that evaluates the impact of PRPP intervention on social participation. Considering the primary place of cognitive processes for social competence, there is limited guidance on ways to specifically target cognitive strategy use to improve children’s social participation in occupational therapy. Therefore, this study was guided by the research question: ‘What is the impact of a playground social skills programme based on the PRPP system of intervention on children’s social competence?’
Method
Research design
A quantitative experimental design was used to evaluate the effectiveness of the PRPP intervention on improving social competence in a group of children in the first four years of formal schooling. Specifically, a crossover design was adopted in which two groups of children received the PRPP intervention at different times. Crossover design is defined as a basic experiment in which participants are randomly assigned to as many groups as there are conditions (Nelson et al., 2017). A group of eight children received the PRPP intervention while another eight children (control) took part in normal playground interaction. The groups then crossed over so that each group received the alternate form of intervention in the subsequent term. This study occurred on the playground of a school in Greater Western Sydney across two school terms (Term 2 and Term 3).
Participants
The data comprised information on social skills and patterns of cognitive strategy use for 16 children. All children were from mainstream classrooms. Teachers nominated children who had difficulty with playground interactions to participate in the programme. The children were aged between five and 10 years. In Term 2, there were four girls in Grade Three who participated in the programme and four boys in Grade One and Grade Two who formed another group. In Term 3, there were another four girls in Grade Three who participated and four boys in Kindergarten that formed another group. Two boys in the social group from Term 2 had a diagnosis of high functioning autism spectrum disorder (ASD), and one child in Grade Three that attended the social group in Term 3 had a mild intellectual disability.
Instrumentation
In this study, teacher perceptions of children’s change in social skills and cognitive strategy use were sought. Two outcome measures were used to assess children’s performance in social activities that were part of routine practice for developing and evaluating the intervention.
Goal attainment scaling scores
For the first outcome measure, SMART goals were set for each child prior to attending the programme. The SMART acronym was used to ensure that the goals were specific, measurable, achievable, realistic and timely (Bovend'Eerdt et al., 2009). Attainment of goals was measured using goal attainment scaling (GAS). GAS is a method of scoring (quantifying) the attainment of goals (Kiresuk and Sherman, 1968) and is based on predicting the expected goal to be achieved, accompanied by at least two states above the expected outcome and two states below, one of which is usually the current (or ‘baseline’) state (Bovend'Eerdt et al., 2009). This measure was chosen as it is well researched with empirical evidence (Hurn et al., 2006) and is more sensitive to individual change compared to other standardised measures of change.
Goals for each child were based on teacher concerns regarding playground participation. Teacher observations of the child’s social behaviour and its impact on social participation in the classroom and on the playground were used to formulate these goals. Goals also reflected discussion with children in the older groups about difficulties that they were having with interactions on the playground. Each child’s SMART goals were quantified on a –2 to +2 scale, with each level defined. For example, for one child the goal was to use a confident voice to ask to join in a game with his peers on the playground with no prompting. The –2 was defined as ‘the child requires frequent assistance to ask to join in a game and is observed playing on his own’, while +2 was defined as ‘almost always shows an ability to play with his peers’.
The PRPP system of task analysis
The second outcome measure used the assessment component of the PRPP system of task analysis (Chapparo and Ranka, 2014) to evaluate change in cognitive strategy use according to teacher perceptions. The PRPP assessment is an occupation-based, standardised, criterion-referenced assessment that measures the effectiveness of cognitive strategy use during task performance. It has been used successfully to measure change in cognitive strategy use during everyday occupational performance with adults (Nott et al., 2009) and children (Mills et al., 2016) who have difficulties with learning and behaviour, and has been used to analyse text-based data (Lewis et al., 2016). Research indicates good inter-rater and intra-rater reliability and excellent discriminant validity (Nott et al., 2009).
The PRPP assessment focuses on cognitive strategies that are theoretically aligned with four ‘quadrants’ of information processing: sensory perception and attention; recall; planning and performance monitoring (see inner layer of Figure 1). The data were collected from a teacher questionnaire based on the PRPP assessment. Teachers rated children’s social performance across 35 different cognitive strategy use items (see outer layer of Figure 1) on a 3-2-1 scale. This involved rating performance across the 35 items as (3) effective in task performance; (2) questionable/occasional difficulty or (1) not effective/difficult. Each question represented one cognitive strategy use item from the PRPP model. For example: ‘Does the child recognise facial expressions and feelings expressed by others?’ ‘Does the child choose the best strategy for solving a problem on the playground?’

The Perceive, Recall, Plan and Perform (PRPP) system of task analysis conceptual model (Chapparo and Ranka, 2014).
Intervention
The programme that was the focus of this study was based on the PRPP system of intervention. Children were invited to attend a ‘Mystery Club’ working as a team of social detectives to discover cognitive strategies every week in the context of regular playground activities. The programme occurred in a separate area on the playground of the school with a focus on transitioning social skills to the playground. There were four children to one therapist. Each session ran for the course of one lunch period per week across one term, which equated to 10 weeks of intervention. The occupational therapist also liaised with school staff to ensure that teachers understood the strategies to prompt the children when required.
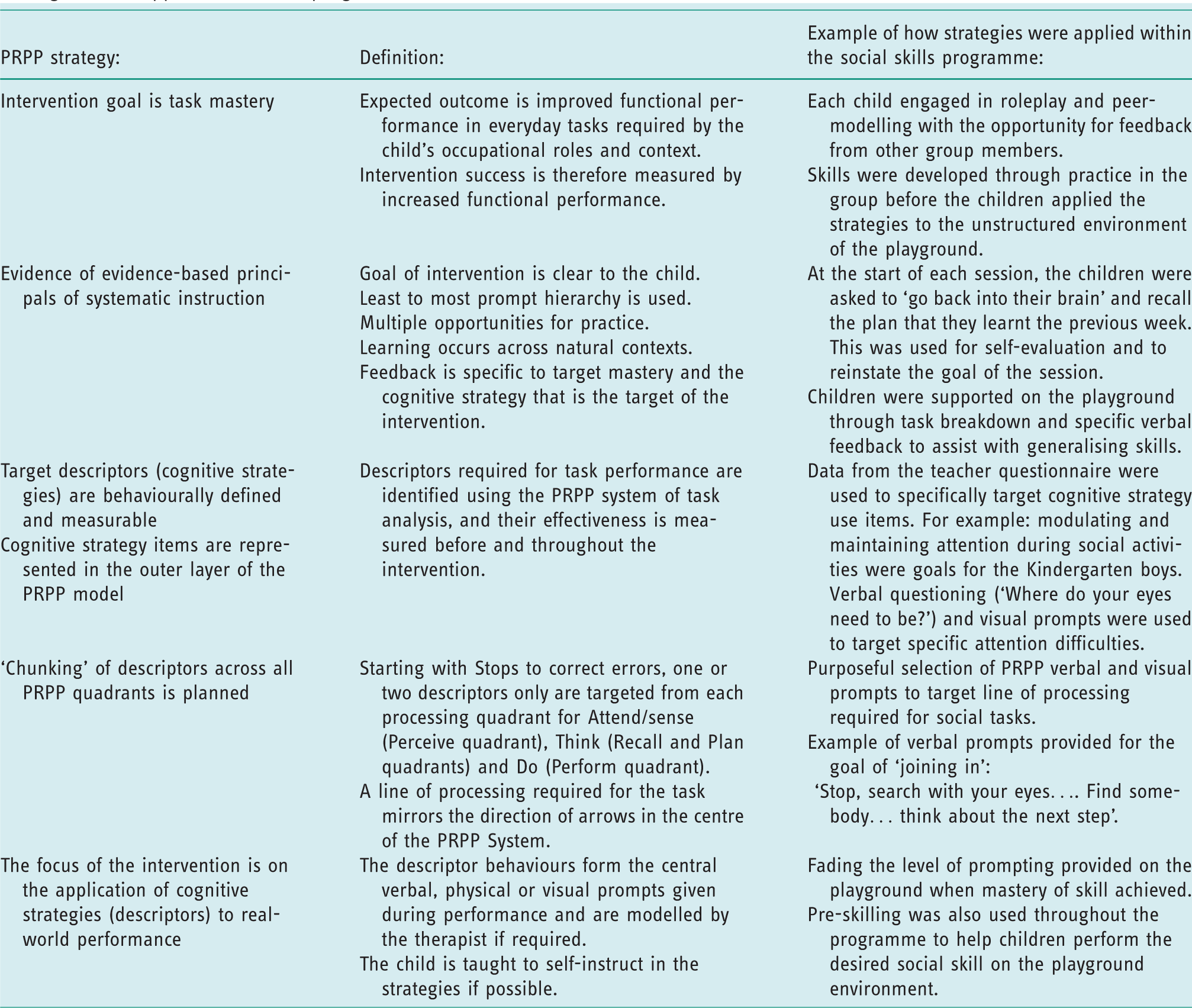
The PRPP intervention targets processes that support or inhibit the construction, processing and storage of information needed for everyday occupational performance (Chapparo and Ranka, 2010). Data from the teacher questionnaires were used to target specific cognitive strategy use items represented in the PRPP conceptual model (see outer layer of Figure 1). For example, modulating and maintaining attention during social activities were goals for the Kindergarten boys’ group, and specific PRPP verbal and visual prompts were used to target attention difficulties during play activities. These play activities were tailored to the ages of the children and their interests. For example, the boys in the Kindergarten group were facilitated in knowing how to ‘join in’ and engage in imaginative unstructured play. The girls in Grade Three were taught strategies for negotiating and problem-solving used in the context of structured playground activities such as playing a game of ‘handball’. One core principal of PRPP intervention is evidence-based principals of systematic instruction. At the earlier stages of the programme, children were supported with a high level of prompting during social activities and were then assisted on the playground through task breakdown and specific verbal feedback to assist with generalising skills. Social skills were modelled in the small groups before the children then applied the strategies to the unstructured environment of the playground. Table 1 defines the core intervention principals in the PRPP system of intervention and provides examples of how these were embedded within the programme.
Core principals of intervention of the Perceive, Recall, Plan and Perform (PRPP) system of intervention and examples of how strategies were applied within the programme.
Data collection procedures
Ethical approval was obtained from The University of Sydney Human Research Ethics Committee Project No: 2016/219. Parents provided written consent to the school for their children to be part of the programme. The programme occurred as part of routine occupational therapy practice requested by the school. The children were invited to attend the programme and verbal consent was assumed if they agreed to be part of ‘Mystery Club’. The children were informed of the purpose of the programme and were keenly motivated to learn new strategies to support playground interactions. A goal-setting meeting occurred at the start of the year with the teachers and the occupational therapist to formulate individualised goals. In Term 2, two groups of children participated in the programme (a group of four girls in Grade Three and a group of four boys in Grades One and Two). Crossover occurred in Term 3, with those that were the control crossing over and becoming the intervention group (another group of four girls in Grade Three and a group of four boys in Kindergarten).
All teachers were asked to complete the outcome measures at three time-points throughout the year. The teachers observed the children’s social interactions and cognitive strategy use in the natural context of the playground and classroom environments. The teachers were given a week to make their observations and measure the children’s performance at the three time-points. The first data collection time was prior to Term 2, before any of the children received the intervention. This was used to establish a baseline. The second data collection time was at the end of Term 2, prior to crossover. The third time was after Term 3, after all four groups of children had received the programme. Statistical analysis was then used to measure the effect of the intervention on children’s social participation across these time periods.
Data analysis
Data were analysed using a series of two-way, repeated-measures analyses of variance (ANOVAs), one for GAS scores described below, and one each for the four PRPP quadrant scores, described further below (Pallant, 2013). The intervention variable had two levels: Group A included all the children who participated in the social skill program in Term 2; Group B included all children who participated in the program in Term 3. It was appropriate to have them all grouped together due to the small numbers of participants in the study. GAS scores and PRPP quadrant total scores were the outcome measures used at the three time-points. The factor of time had three levels: baseline prior to any intervention; post-intervention after the initial 10 week intervention period; post-crossover after the 10 week crossover intervention period. The Statistical Package for the Social Science Statistics (IBM SPSS©) Version 24 was used for analysis.
GAS scores
GAS scores were used as primary outcome measures for this study, as they allowed for a measure of child-relevant occupational performance outcomes. The alpha level for statistically significant differences was set at p<0.05. Assumptions were tested using Mauchly’s test of sphericity (assumptions were met if sphericity was considered non-significant, p>.05). Data were then analysed using a two-way, between-group, repeated-measures ANOVA that measures the differences in mean scores between two groups. All ANOVAs tested the main effect for group (did one group of children overall average higher scores that the other group?), the main effect for time (did both groups change their average social performance over the course of the study?), and the interaction between group and time (did both groups follow the same pattern of change in performance over time?). For both the main effect for time, and the group by time interaction, quadratic contrasts were used to clarify the pattern of change in children’s GAS scores. The first (linear) contrast tested if average social performance at the end of data collection was higher or lower than at the start. The second (quadratic) contrast tested if any change in average social performance was more rapid at different times of the study. The primary prediction was that there would be a significant quadratic interaction between group and time, with Group A improving most in Term 2 first, when they received the PRPP system of intervention, and Group B improving most rapidly in Term 3, when they then crossed over and received the PRPP intervention.
The PRPP system of task analysis
PRPP quadrant scores were then analysed as secondary outcome measures to determine the effect of the intervention on children’s cognitive strategy use. Each of the four quadrants were individually analysed to determine the change in children’s cognitive strategy use across the perceive, recall, plan and perform quadrants. This involved a process of converting raw PRPP scores (as tallied on the questionnaire) into percentage scores. There are 35 cognitive strategy use items (outer layer of Figure 1) that are rated on a 3-2-1 scale. The total quadrant score that a child can get for perceive, recall and plan is 27 for each quadrant (9 items by the highest score of 3) and 24 for perform (8 items in this quadrant). Each child’s total score for each quadrant was converted into a percentage score. Percentage scores were calculated across the three time-points and entered into SPSS. The process used for GAS score analysis was also used for PRPP analysis. The primary prediction was that there would be similar changes in PRPP quadrant scores to the changes in GAS scores.
Results
Change in GAS scores
A two-way, repeated-measures ANOVA was conducted to explore the impact of the social skills programme on children’s social performance, as measured by GAS scores. Mauchly’s test indicated that assumption of sphericity had not been violated (x2 (2) = .926, p >.05).
As can be seen from Figure 2, predictions were confirmed for the GAS scores. Both groups had improved their average GAS score by the end of the study (F(1,14) = 50.806, p<0.001), and there was no evidence either had improved more than the other (main effect for group F(1,14) =2.871, p =0.112). Most importantly, both groups showed the greatest improvement in the term when they received the PRPP system of intervention (parallel non-parametric analysis using Mann–Whitney U tests produced similar results to parametric analysis) (quadratic interaction: F(1,14) = 18.053, p = 0.001).
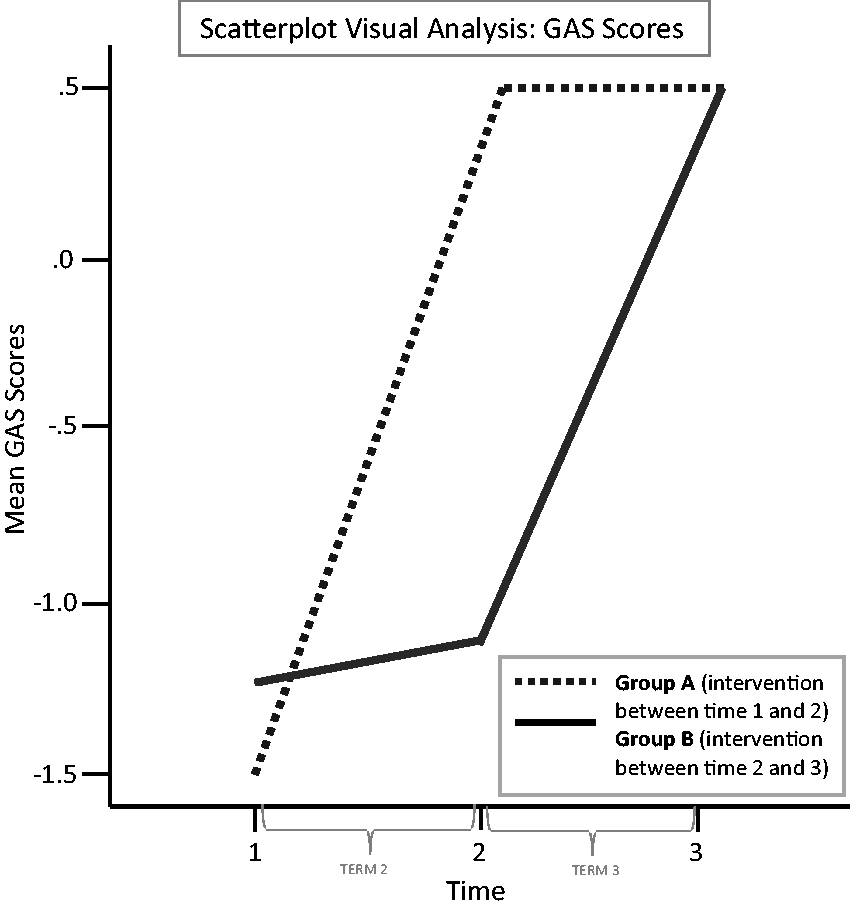
Scatterplot showing linear progression of goal attainment scaling (GAS) scores after children received the intervention.
Change in PRPP quadrant percentage scores
Two-way, repeated-measures ANOVAs were also conducted to explore the impact of the social skills programme on children’s cognitive strategy use, as measured by the four PRPP quadrants. Mauchly’s test indicated that assumption of sphericity had not been violated for all four PRPP quadrants (perceive: x2 (2) = 0.495, p >0.05; recall: x2 (2) = 0.158, p >0.05; plan: x2 (2) = 0.243, p >0.05; perform: x2 (2) = 0.185, p >0.05).
As can be seen from Figure 3, most improvement in cognitive strategy use coincided with children receiving the PRPP intervention. Both groups had improved their average PRPP quadrant scores by the end of the study and there was no evidence that one group had improved more than the other. Most importantly, coinciding with improved GAS scores, both groups showed the greatest improvement in cognitive strategy use when they received the intervention (quadratic interaction: perceive: F(1,14) =14.351, p = 0.002; recall: F(1,14) =8.057, p = 0.013; plan: F(1,14) = 7.852, p = 0.014; perform: F(1,14) = 11.834, p = 0.004).
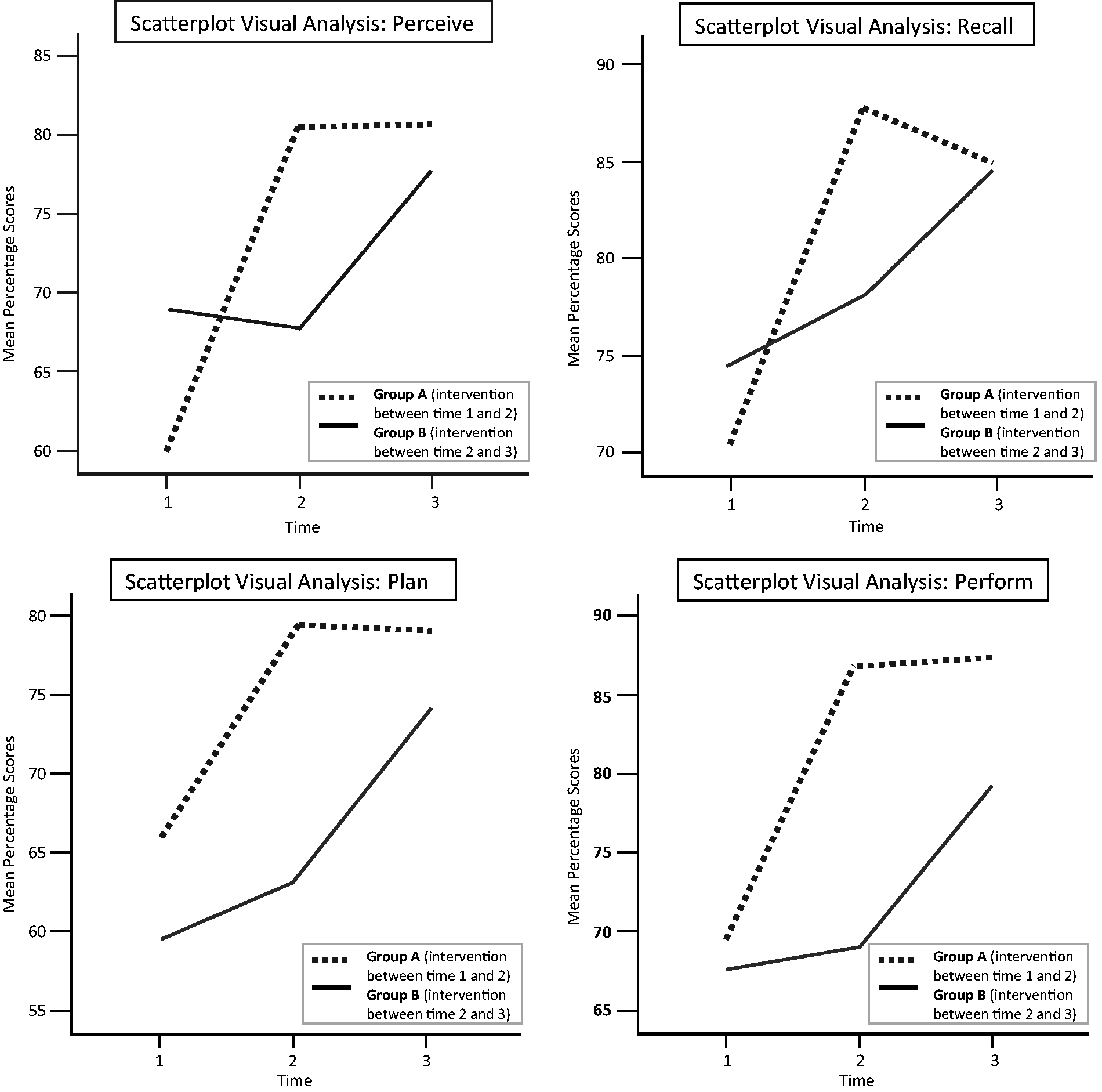
Scatterplot showing linear progression of PRPP quadrant scores (Perceive, Recall, Plan and Perform) after receiving the intervention.
Discussion and implications
The purpose of this study was to evaluate the effectiveness of a social skills programme developed to teach children how to use cognitive (thinking) strategies during playground activities. For 16 children, cognitive strategies deemed essential for daily occupational performance were measured using the PRPP system of task analysis. Assessment findings gathered at baseline were used to construct an intervention programme that taught children to direct their thinking strategically across a variety of social activities. This strategy-focused approach appeared to be effective in developing improved capacity to participate in playground social activities in children with reduced social competence. Outcome measures taken at three time-points for two groups of children suggest that children improved in social performance when receiving the PRPP intervention in comparison to current instructional methods used during playground interactions. Visual analysis also indicated that the children in Group B made some small improvement when not receiving the intervention which could be explained by natural learning during social interactions.
The results of this study provide initial evidence about the effectiveness of teaching children how to apply cognitive strategies as a basis for developing social skills. In this study, children’s social performance as measured by an improvement in GAS scores modelled a similar pattern of improvement in cognitive strategy use, as measured by the PRPP system. Children were taught a repertoire of strategies for attending, analysing information, selecting important details, relating new information to prior knowledge and organising knowledge for effective task performance. This aligns with a growing body of literature into the importance of using multiple information-gathering strategies to support generalisation of social skills (McKown et al., 2009; Siegler, 2007). The capacity to generate thinking strategies plays an important role in children’s joint attention and cooperation within social interactions (Chapparo and Ranka, 2010). With increased opportunity to use thinking strategies, children became more adaptive during social interactions by learning to gather and manipulate the information most appropriate to the salient social interaction.
Few published studies have attempted to evaluate the impact of occupational therapy interventions that address cognitive strategy use in children with reduced social competence. In this study, children’s cognitive strategy use during playground interactions was targeted. Information collected at baseline indicated that children had the most difficulty with perceive and planning processes. Perceive items including strategies for attending and analysing social information were simultaneously targeted with strategies teaching children how to think and choose the best strategy ‘fit’ relative to a social situation. Studies of children who exhibit difficulties with social competence have demonstrated successful outcomes when the intervention is based on principals of systematic instruction (Bauminger et al., 2005; Case-Smith, 2015). Methods of therapy instruction used in these studies have included task analysis, prompting, modelling and peer/self-evaluation (Case-Smith, 2015). Additionally, research shows that children who are able to attend to the social environment are more responsive to change and are more likely to generate relevant thinking strategies when a social problem is presented (Dodge et al., 2013).
The results of this study indicate that transfer of social skills is influenced by children’s capacity to develop and use thinking strategies within the context of the playground. In this study, children in Group A demonstrated improved strategy use both during and following the period of intervention. Clinicians often report feeling challenged as a result of not being able to teach children how to generalise social skills to the context of varied social interactions (Lim and Rodger, 2008). Studies reported in the literature have focused on teaching specific social skills within small groups, but there is limited focus on thinking abilities to help children make predictions and change their behaviour according to past knowledge and experiences (Hilton, 2015; O’Conner et al., 2017). Children in this study were able to generate numerous thinking strategies in response to a problem through not only active social engagement, but also through use of guided instruction about self-evaluation and reflection. This finding adds to the body of evidence that supports social learning through peer engagement and application to a real-world context (Pascoe and Brennan, 2017).
A common difficulty experienced by children with reduced social competence is the inability to recall plans for effective social interaction. As found in previous studies, it is children with higher cognitive flexibility that are the most cooperative and responsive in social activities with their peers (Dodge et al., 2013; O’Conner et al., 2017). Cognitive flexibility during social activities is partly dependent on how well children are able to adapt known strategies based on past experiences (Chapparo and Ranka, 2010). In this study, children in Group A demonstrated improved memory for social ‘rules’ of engagement immediately after the course of intervention but were then unable to maintain the same level of performance when crossover occurred. This is demonstrated by the results of the recall quadrant analysis, which modelled a decline in children’s cognitive strategy use in the second time frame. This finding reinforces the importance of helping children recall past schemas so that they are able contextualise social skills to the time and place of an interaction. The intervention provided for these children lasted for less than one school term. It is possible that intervention for a longer period of time may further strengthen the capacity to transfer strategies to the context of the playground (O’Conner et al., 2017). With increasing experience and exposure to practising both the skills needed as well how to use cognitive strategies across different situations, it is likely that children will learn to internalise and apply strategies independently.
Limitations
There were several limitations to this study. The data used in the study were from a small group of children from one area of Greater Western Sydney. Data from a more diverse population of children may present different results. The school setting of the study allowed for only a 10-week programme to be implemented. Further studies that involve longer periods of intervention and an evaluation into the long-term impact of cognitive strategy use would provide more detail to guide therapists in assessment and planning follow-up. Outcome measures that evaluated performance from the children’s perspective would have strengthened findings from this study. Replicating the study across subjects and settings would further strengthen findings.
Conclusion
This study evaluated the effectiveness of the PRPP intervention with children who were experiencing difficulty with social participation. Using a crossover study design, children in a social skills programme targeting cognitive strategy use improved in participation in social activities at school. The results of this study can be used to guide future assessment and planning in the area of social cognition for occupational therapists. Further studies using the PRPP system are required to build on these findings to further target children’s social competence.
Key findings
Occupational therapy directed by the Perceive, Recall, Plan and Perform (PRPP) intervention was associated with improvement in children’s performance during social activities. Children’s social competence at school is influenced by the ability to generate cognitive thinking strategies during social performance.
What the study has added
The PRPP system of task analysis can be used to guide the practice of occupational therapists working with children who have difficulties with social competence at school.
Footnotes
Research ethics
Ethical approval was obtained from The University of Sydney Human Research Ethics Committee Project No: 2016/219.
Consent
Parents provided written consent to the school for their children to be part of the programme.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Contributorship
All authors contributed to the methodology of the project, and the statistical analysis. Julianne Challita co-led the design of the study, the collection and analysis of the data, and the writing of the manuscript. Christine Chapparo assisted with the design of the study, appraisal of data, and writing and revision of the manuscript. Joanne Hinitt assisted with data appraisal and writing the manuscript. Robert Heard also assisted with data analysis and interpretation, and writing the manuscript.